
Abstract
Background
Adoption of contraceptive implants and intrauterine devices has been less than might be expected given their superior efficacy and convenience. The purpose of this study was to assess knowledge and beliefs held by women, which may influence their contraceptive choices and theirongoing utilization of contraceptive methods.
Methods
English speaking, nonpregnant, reproductive-age women, who were not surgically sterilized, were individually interviewed to obtain limited demographic characteristics and to assess their knowledge about the efficacy of various contraceptive methods in typical use and about the relative safety of oral contraceptives.
Results
A convenience sample of 500 women aged 18–45 years, with education levels that ranged from middle school to postdoctoral level was interviewed. The efficacy in typical use of both combined oral contraceptives and male condoms was correctly estimated by 2.2%; over two-thirds of women significantly overestimated the efficacy of each of those methods in typical use. Oral contraceptives were thought to be at least as hazardous to a woman’s health as pregnancy by 56% of women.
Conclusions
The majority of reproductive aged women surveyed substantially overestimated the efficacy of the two most popular contraceptive methods, often saying that they were 99% effective. Women with higher education levels were most likely to overestimate efficacy of oral contraceptives. Women of all ages and education levels significantly overestimated the health hazards of oral contraceptives compared to pregnancy. Overestimation of effectiveness of these methods of contraception, may contribute to lower adoption of implants and intrauterine devices. When individualizing patient counselling, misperceptions must be identified and addressed with women of all educational backgrounds.
Trial registration
Not applicable.
Similar content being viewed by others

Background
Contraceptive implants and intrauterine devices (IUDs) provide pregnancy protection on par with permanent contraception. Increased use of these methods has been associated temporally with decreases in unintended pregnancy rates in the United States (US) [1, 2]. Since there appears to be a link between inconsistent contraceptive use and perception of low personal risk for pregnancy, it is interesting to consider that a perception of low pregnancy risk might influence choice of contraceptive method [3]. While combined hormonal contraceptives and progestin-only pills, contraceptive patches, vaginal contraceptive rings and injections offer significant noncontraceptive benefits that are important to many women, inconsistent use of those methods results in first year typical failure rates that are at least 20 times higher than failure rates of IUDs and implants [4]. Male condoms in typical use have been reported to have even higher first year failure rates of 12% [5]. The superior efficacy and convenience of implants and IUDs should appeal to couples, but these top tier methods were still utilized by only 7.3% of US women in the 2011–13 National Survey of Family Growth (NSFG) [6].
Previous surveys and focus groups have tried to determine what various groups (contracepting women, at-risk women and the general public) believe to be the efficacy and safety of various methods of contraception [7,8,9]. Investigators have also attempted to understand why men and women discontinue contraceptive methods or use them inconsistently [9,10,11,12,13,14,15,16].
There are many factors that enter into a woman’s decision to choose a specific method of birth control, including health restrictions, cost, availability and partner preference. However, surveys consistently report that the most important feature that women want from their contraceptive method is efficacy [17,18,19]. Given that high priority, we sought to determine if women were aware of the superior pregnancy protection offered by IUDs and implants or if they thought older methods were as effective. We also asked how women rated the health risks of pregnancy compared to the health risks associated with combined oral contraceptives. Finally, we sought to determine if age, education or parity influenced any of the findings.
Methods
This project was approved by both the John F. Wolf Human Subjects Committee and the Research Committee at the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center (LA BioMed) (Project number 30329-01). Requirement for informed consent was waived because the study presented no more than minimal risk to the subjects and no personal identifying information would to be collected.
The study survey first obtained limited demographic information and then asked specific questions about knowledge and beliefs about method efficacy. The survey instrument was beta-tested to determine if the questions were understandable to the population to be studied and to ensure consistency in the way that the two surveyors (RK and LLL) administered the survey. Women were interviewed within the family planning clinic and the gynecology clinic at Harbor-UCLA Medical Center and in the open areas of Los Angeles BioMedical Research Institute campus. In both the gynecology and the family planning clinics, all uninsured women living in the State of California with family incomes below 200% of the Federal poverty levels qualify for enrollment into the state Medicaid program, (Family PACT) which provides all forms of contraception without any charge. Women interviewed at other locations on campus may have had private insurance coverage; at the time of this survey most California insurance companies were providing without charging any co-payments under the provision of the Affordable Care Act. Exclusion criteria for study participation included all of the following: age under 18 or over 45 years, use of permanent contraception (tubal ligation, tubal occlusion, or hysterectomy) pregnancy, and an inability to speak English. Responses gathered about efficacy from these subjects were compared to the estimates derived from the National Survey of Family Growth and published in most standard texts of the time [20]. Specifically, correct estimates of first year failure rates in typical use were assumed to be 9% for oral contraceptives and 18% for male condoms. For purposes of this survey, the term “efficacy” was used because it was more familiar to the women. It is the term used in product labeling and in advertisements for methods. “Efficacy” was calculated as the difference between 100 and the method’s first year failure rate in typical use. Women were offered efficacy choices of 99, 95, 91, 83 and 70% for each of the methods (oral contraceptives, male condoms, IUD, implant). At the conclusion of the survey, women were asked which they thought was more hazardous to a woman’s health—oral contraceptives or pregnancy. The results were compiled into an Excel document; standard statistical programs were used for calculations. Specifically, p values were calculated using Graph Pad Quick Calcs with Fisher’s exact test and two tail tests. Chi square tests were applied to percentages of women overall and in each subgroup with answers that were correct vs. incorrect, or correct vs. overestimates or correct vs underestimates. The threshold for statistical significant analyses was set at p < 0.05.
Results
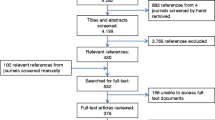
In total, 781 women were individually invited by one of the female researchers (RK, LL) to participate in the survey. Of the 781 women approached, 215 women declined, and 66 women met exclusionary criteria, leaving a study population of 500 women. Virtually all the women who declined to be interviewed expressed an interest in participating, but said that they did not have time available to do so.
The demographic characteristics of the reproductive-aged women in this convenience sample are displayed in Table 1. Their mean age was 25.1 years, ranging from 18 to 45 years slightly over one fifth (20.2%) had only attended high school. One woman’s highest education was middle school. However, over half of the participants had graduated from a 4-year college and another 17% had done graduate work. Parity ranged from 0 to 6; 51.6% of the study population was nulliparous. Given the public setting in which questions were being asked, women were not directly asked about their current sexual activity or contraceptive method use.
Table 2 displays the study participants’ estimates of efficacy in typical use of COCs and male condoms. When offered five different estimates of first year efficacy (99, 95, 91, 83, and 70%), 2.2% of the study population correctly identified the first-year efficacies in typical use of both COCs and male condoms. Regardless of age, education or parity, study subjects overwhelmingly overestimated the pregnancy protection provided in typical use of each of these methods. Compared to women with no college experience, those with at least a 4-year college degree were more likely to overestimate the efficacy of COCs (71.1% vs. 55.4% p = 0.0028), but not the efficacy of condoms (74.3% vs. 68% p = 0.1385). While far fewer women underestimated the efficacy of COCs, the less educated women were more likely than women with more education to do so; high school graduates were more likely to underestimate the efficacy of COCs compared to those with college degrees (29.7% vs. 15.2% p = .0071). Educational attainment did not affect the proportion of women who underestimated the efficacy of condoms.
Table 3 shows that 56.2% of all women surveyed believed that oral contraceptives were at least as hazardous to a woman’s health as pregnancy. Almost half (47.7%) of women with at least a 4-year college education said that birth control pills pose at least as great of a risk to a woman’s health as pregnancy, compared to 68.4% of women who had no more than a high school education (p = .0001). Parity made no difference; 60% of multiparous women believed that combined hormonal contraceptive pills are at least as risky as pregnancy compared to 52.7% of nulliparous women (p = 0.1158).
Discussion
A woman’s perception of the efficacy and safety of a contraceptive method may strongly influence both her selection of the method and her decision to continue to use it over time [3, 17]. These perceptions are often derived from, or at least perpetuated by, the media and distributed via peer networks, educational facilities, and popular culture, including magazines, television shows, movies, online blogs and other social media [21]. New tools piloted to assess women’s contraceptive knowledge have concluded that contraceptive knowledge may be lower than previous studies have suggested [22].
Despite the importance that women claim they attach to the efficacy of different methods in selecting methods to use, our study found that the vast majority of women was misinformed about the pregnancy protection offered by the most popular methods. Only 2.2% of our study population was able to correctly identify the first-year failure rates in typical use of COCs and the male condoms and most erred on the side of overestimating the efficacy of those methods. These findings may help explain why there has not been a more enthusiastic and widespread adoption of contraceptive implants and intrauterine devices, despite their proven superiority in pregnancy protection [4]. The National Campaign to Prevent Teen and Unintended Pregnancy also showed that most adolescent women believe all contraception is equally effective so that emphasizing the effectiveness of IUDs and implants is not likely to impress young women. They conclude that it is more important to discuss the other attributes and benefits of IUDs and implants than efficacy [23]. A recent national telephone survey of 2302 women veterans, aged 18–44, found that only 50% knew that the male condom was less effective at preventing pregnancy compared to sterilization, IUDs and implants and hormonal contraception [24].
The percent of women who underestimated COC efficacy in our study is comparable to findings of the ACOG surveys done in the 1985 and 1993, which found that nearly 4 in 10 women of childbearing age thought that the failure rate of the pill was at least 10% [25]. Surveys of 900 women in Jamaica and India found that only 46% of women knew that COCs are more effective than condoms and only 50% knew that IUDs are more effective than condoms [19]. It is possible that this misinformation contributes to understanding why so many women use methods that are inconsistent with their stated reproductive life plans [26, 27].
Contraceptive users themselves are not alone in these misbeliefs. In a study of parents of 13–17 year olds, Eisenberg et al reported that many parents (especially conservatives) underestimated the perfect use effectiveness of condoms for reducing both pregnancy and STD risks [28]. Parisi et al found that 81% of primary care physicians surveyed underestimated the risk of pregnancy with unprotected intercourse; but 85% overestimated the efficacy of COCs, and 62% overestimated the efficacy of male condoms for pregnancy protection [29].
In the combined 2002 and 2006–2010 National Surveys of Family Growth, 16.5% of sexually active women reported they did not use contraception [30]. Thomas et al have demonstrated that the single most effective step to reduce unintended pregnancy rates in the US would be to increase the proportion of sexually active women not seeking pregnancy who use any method at all [31]. However, it may be easier to persuade women who have decided to contracept to adopt methods that may be more effective. Both approaches are important. Both may benefit from educating women about their risks of pregnancy if they continue their current actions. Since great disparities continue to exist among different racial and ethnic groups independent of access to healthcare, different counselling approaches may be needed [32].
In the televised Nelson congressional hearings in 1970 about oral contraceptive safety, millions of Americans tuned in to hear experts testify that “estrogen is to cancer as fertilizer is to wheat” [33]. Concerns about the safety of contraception are prevalent and long standing. ACOG/Gallop polls conducted in 1985 and 1993 reported that over half of pill users believed they were accepting a significant health risk by taking an oral contraceptive, and over 60% thought that COCs were riskier than childbirth [25]. Recent press coverage of breast cancer and depression risk for a variety of hormonal methods has fueled this underlying mistrust as have ongoing disputes about the clinical significance of potential differences seen in risk of thrombosis [34,35,36,37,38]. National surveys in Ireland in 2010 found that 37% of Irish women agreed with the statement “the OCP has dangerous side effects” and that such agreement was the strongest predictor variable of non-use of OCPs [39]. Excessive fears about the safety of oral contraceptive were also revealed in an earlier survey done by our group and others [39,40,41].
The clear consensus from all experts is that all of the methods are safer to the health of the women who are candidates than pregnancy [42,43,44,45]. This study demonstrates that this last reassuring message has not reached most women. Over half of women interviewed in this study believed that oral contraceptives were at least as hazardous to a woman’s health as pregnancy.
There are important limitations to the generalizability of our results. Very recent calculations of typical use failure rates all lower than the estimates we used in this study. Pill failure rates, in typical use, are now quoted as 6% (down from 9%) and for the male condom, 13% is now quoted [5]. Although the corresponding efficacy rates for those exact estimates (94 and 91%) were not offered as options in this study, it is clear that the findings of overestimation of efficacy still are correct, since so many women estimated 99 and 95% efficacy rates for all methods. The study population represented a diverse sample of English speaking women and included uninsured, indigent women as well as a highly educated medical and research professional staff. However, the study population was geographically isolated. No information was collected about race or ethnicity, so we are not able to assess the impacts of those variables. Rosenfield et al have demonstrated higher rates of contraceptive misinformation among non-Hispanic black women [24]. Direct questions about the subject’s current sexual activity and contraceptive use were not included in the survey as it was administered in a potentially public setting. This may possibly have limited our ability to interpret the differences seen between contraceptive users and nonusers. However, the significant prevalence of misinformation revealed by this study in all women overshadows any of the differences that may have been observed between groups.
Understanding the prevalence of misperceptions about method failures and contraceptive safety can help clinicians provide targeted counselling to enable each woman to make a more informed contraceptive choice.
Conclusions
This survey of 500 English-speaking reproductive aged, nonpregnant women found that two thirds of women surveyed markedly over-estimated the efficacy of more traditional methods of contraceptive, such as condoms and oral contraceptives. Women with higher education levels were not immune to misinformation; they understated the failure rates at higher rates than women with high school educations only. At the same time, the majority of women overstated the health risks of pill use, reporting that oral contraceptives are at least as hazardous to a woman’s health as pregnancy. Promoting the unparalleled pregnancy protection offered by implants and intrauterine contraceptives may not resonate with potential users because they do not see any room for improvement in efficacy. On the other hand, the increased safety of progestin-only or nonhormonal methods may interest more of them who are apparently quite concerned about the health risks of estrogen-containing pills. Additionally, results demonstrate that women are ill-informed about the potential health risks of pregnancy.
Abbreviations
- ACOG:
-
American Congress of Obstetricians and Gynecologists
- COCs:
-
Combined oral contraceptives
- IUD:
-
Intrauterine device
- OCP:
-
Oral contraceptive pill
References
Kavanaugh ML, Jerman J, Finer LB. Changes in use of long-acting reversible contraceptive methods among U.S. women, 2009–2012. Obstet Gynecol. 2015;126(5):917–27.
Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374(9):843–52.
Moreau C, Bohet A. Frequency and correlates of unintended pregnancy risk perceptions. Contraception. 2016;94(2):152–9.
Birgisson NE, Zhao Q, Secura GM, Madden T, Peipert JF. Preventing unintended pregnancy: The Contraceptive CHOICE Project in Review. J Womens Health (Larchmt). 2015;24(5):349–53.
Sundaram A, Vaughan B, Kost K, et al. Contraceptive failure in the United States: estimates from the 2006–2010 National Survey of Family Growth. Perspect Sex Reprod Health. 2017;49(1):7–16.
Daniels K, Daugherty J, Jones J. Current contraceptive status among women aged 15–44: United States, 2011–2013. NCHS Data Brief. 2014;173:1–8.
Unintended Pregnancy in the United States. (2013 December). Guttmacher Insitute. Last accessed 15 Jan 2016. from http://www.guttmacher.org/pubs/FB-Unintended-Pregnancy-US.html. Accessed 16 June 2017.
Edwards JE, Oldman A, Smith L, McQuay HJ, Moore RA. Women’s knowledge of, and attitudes to, contraceptive effectiveness and adverse health effects. Br J Fam Plann. 2000;26(2):73–80.
Lundsberg LS, Pal L, Gariepy AM, Xu X, Chu MC, Illuzzi JL. Knowledge, attitudes, and practices regarding conception and fertility: a population-based survey among reproductive-age United States women. Fertil Steril. 2014;101(3):767–74.
Rosenberg MJ, Waugh MS, Long S. Unintended pregnancies and use, misuse and discontinuation of oral contraceptives. J Reprod Med. 1995;40(5):355–60.
Rosenberg MJ, Waugh MS. Oral contraceptive discontinuation: a prospective evaluation of frequency and reasons. Am J Obstet Gynecol. 1998;179(3 Pt 1):577–82.
Moreau C, Cleland K, Trussell J. Contraceptive discontinuation attributed to method dissatisfaction in the United States. Contraception. 2007;76(4):267–72.
Peipert JF, Zhao Q, Allsworth JE, et al. Continuation and satisfaction of reversible contraception. Obstet Gynecol. 2011;117(5):1105–13.
Beksinska ME, Rees HV, Smit J. Temporary discontinuation: a compliance issue in injectable users. Contraception. 2001;64(5):309–13.
Potter L, Oakley D, de Leon-Wong E, Cañamar R. Measuring compliance among oral contraceptive users. Fam Plan Perspect. 1996;28(4):154–8.
Westhoff CL, Heartwell S, Edwards S, et al. Oral contraceptive discontinuation: do side effects matter? Am J Obstet Gynecol. 2007;196(4):412.e1–6.
Grady WR, Klepinger DH, Nelson-Wally A. Contraceptive characteristics: the perceptions and priorities of men and women. Fam Plan Perspect. 1999;31(4):168–75.
Madden T, Secura GM, Nease RF, et al. The role of contraceptive attributes in women’s contraceptive decision making. Am J Obstet Gynecol. 2015;213(1):46.e1–6.
Steiner MJ, Trussell J, Mehta N, et al. Communicating contraceptive effectiveness: A randomized controlled trial to inform a World Health Organization family planning handbook. Am J Obstet Gynecol. 2006;195(1):85–91.
Trussell J, et al. Contraceptive Technology. 20th ed. New York: Ardent Media; 2011. p. 50.
Goldzieher JW. Bust without boom. Contraception. 2000;61(1):27–8.
Haynes MC, Ryan N, Saleh M, Winkel AF, Ades V. Contraceptive Knowledge Assessment: validity and reliability of a novel contraceptive research tool. Contraception. 2016;95(2):190–7.
The National Campaign to Prevent Teen and Unplanned Pregnancy. Last accessed 15 Jan 2016. https://thenationalcampaign.org/. Accessed 16 June 2017.
Rosenfeld E, Callegari LS, Sileanu FE, et al. Racial and ethnic disparities in contraceptive knowledge among women veterans in the ECUUN study. Contraception. 2017. Epub ahead of print.
Gallop Organization. Attitudes toward contraception, ACOG news release. 1985.
Nelson AL, Shabaik S, Xandre P, Awaida JY. Reproductive life planning and preconception care 2015: Attitudes of English-speaking family planning patients. J Womens Health (Larchmt). 2016;25(8):832–9.
Foster DG, Biggs MA, Ralph LJ, et al. Family planning and life planning reproductive intentions among individuals seeking reproductive health care. Womens Health Issues. 2008;18(5):351–9.
Eisenberg ME, Bearinger LH, Sieving RE, Swain C, Resnick MD. Parents’ beliefs about condoms and oral contraceptives: are they medically accurate? Perspect Sex Reprod Health. 2004;36(2):50–7.
Parisi SM, Zikovich S, Chuang CH, Sobota M, Nothnagle M, Schwarz EB. Primarycare physicians’ perceptions of rates of unintended pregnancy. Contraception. 2012;86(1):48–54.
Mosher W, Jones J, Abma J. Nonuse of contraception among women at risk of unintended pregnancy in the United States. Contraception. 2015;92(2):170–6.
Thomas A, Karpilow Q. The intensive and extensive margins of contraceptive use: comparing the effects of method choice and method initiation. Contraception. 2016;94(2):160–7.
Grady CD, Dehlendorf C, Cohen ED, Schwarz EB, Borrero S. Racial and ethnic differences in contraceptive use among women who desire no future children, 2006–2010 National Survey of Family Growth. Contraception. 2015;92(1):62–70.
The Pill. www.pbs.org/ugbh/amex/pill/peopleevents/html. Accessed 16 June 2017.
Lidegaard Ø, Milsom I, Geirsson RT, Skjeldestad FE. Hormonal contraception and venous thromboembolism. Acta Obstet Gynecol Scand. 2012;91(7):769–78.
Lidegaard Ø, Nielsen LH, Skovlund CW, Skjeldestad FE, Løkkegaard E. Risk of venous thromboembolism from use of oral contraceptives containing different progestogens and oestrogen doses: Danish cohort study, 2001–9. BMJ. 2011;343:d6423.
Lete I, Chabbert-Buffet N, Jamin C, et al. Haemostatic and metabolic impact of estradiol pills and drospirenone-containing ethinylestradiol pills vs. levonorgestrel-containing ethinylestradiol pills: A literature review. Eur J Contracept Reprod Health Care. 2015;20(5):329–43.
Hugon-Rodin J, Gompel A, Plu-Bureau G. Epidemiology of hormonal contraceptives-related venous thromboembolism. Eur J Endocrinol. 2014;171(6):R221–30.
Skovlund CW, Mørch LS, Kessing LV, Lidegaard Ø. Association of Hormonal Contraception With Depression. JAMA Psychiat. 2016;73(11):1154–62.
Molloy GJ, Sweeney LA, Byrne M, et al. Prescription contraception use: a cross-sectional population study of psychosocial determinants. BMJ Open. 2015;5(8):e007794.
Nelson AL, Rezvan A. A pilot study of women’s knowledge of pregnancy health risks: implications for contraception. Contraception. 2012;85(1):78–82.
Gueren C. (2013, July 23). 10 birth Control Myths-Debunked!. Womenshealthmag.com. Last accessed 15 Jan 2016. http://www.womenshealthmag.com/health/birth-control-myths. Accessed 16 June 2017.
Sitruk-Ware R. Hormonal contraception and thrombosis. Fertil Steril. 2016;106(6):1289–94.
Heinemann LA, Dinger JC, Assmann A, Minh TD. Use of oral contraceptives containing gestodene and risk of venous thromboembolism: outlook 10 years after the third-generation “pill scare”. Contraception. 2010;81(5):401–7.
Han L, Jensen JT. Does the Progestogen Used in Combined Hormonal Contraception Affect Venous Thrombosis Risk? Obstet Gynecol Clin North Am. 2015;42(4):683–98.
Heit JA, Spencer FA, White RH. The epidemiology of venous thromboembolism. J Thromb Thrombolysis. 2016;41(1):3–14.
Acknowledgements
Not applicable.
Funding
No external funding was utilized. The authors donated their time and supplies.
Availability of data and materials
The data set generated during the current study is available from the corresponding author on reasonable request.
Authors’ contributions
Each author met criteria for authorship. All three helped design the study and test the survey tool. RK and LLL interviewed all the subjects. ALN drafted the manuscript and RK and LLL helped edit it. All authors agree to its contents.
Competing interests
Roshni Kakaiya and Lia Lopez declare they have no competing interests.
Anita L Nelson declares that she has received payments for research from Agile, Bayer, ContraMed and Merck, and honoraria for participation on advisory boards or speaker bureaus for Allergan, Agile, Aspen Pharmaceutical, Bayer, ContraMed, The Female Health Company, Merck, MicroCHIPS Biotech, and PharmaNest.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This project was approved by both the John F. Wolf Human Subjects Committee and the Research Committee at the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center (LA BioMed). Requirement for informed consent was waived because the study presented no more than minimal risk to the subjects and no personal identifying information was to be collected (Project number 30329-01).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kakaiya, R., Lopez, L.L. & Nelson, A.L. Women’s perceptions of contraceptive efficacy and safety. Contracept Reprod Med 2, 19 (2017). https://doi.org/10.1186/s40834-017-0046-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40834-017-0046-5