
Abstract
Background
The growing obesity epidemic in Malaysia presents a public health challenge that requires innovative intervention strategies. In an effort to address this problem, an Interactive Malaysian Childhood Healthy Lifestyle (i-MaCHeL) programme, which is a web-based initiative designed for preschool child–parent dyads offers a novel approach. Nevertheless, the success of such a web-based intervention depends on several interrelated factors. This research aims to examine the feasibility of i-MaCHeL in the Malaysian context, its usability for preschool child–parent dyads, and the acceptability of the programme among these user groups.
Methods
This was a single-arm pilot study involving 46 child–parent dyads recruited from six government preschools in Terengganu, Malaysia. The preschools were selected using a cluster random sampling technique at the preschool level. The intervention feasibility was determined based on the retention rate of participants in the pilot study. The System Usability Scale (SUS) and intervention process evaluation were used to assess the usability and acceptability of the web-based i-MaCHeL programme.
Results
The retention data demonstrated that 42 out of 46 participants completed the 13-week intervention programme, which showed that the overall retention rate was 91.3%. A mean (SD) SUS score of 84.70 (13.82) was obtained from parents, indicating that the web-based i-MaCHeL had an acceptable usability level. The mean scores of the process evaluation items ranged from 4.52 (0.63) to 4.83 (0.38), demonstrating that the web-based i-MaCHeL was highly accepted by the parents. The acceptability data also indicated that at least 92.9% (39/42) of the parents agreed/strongly agreed that the web content, programme duration, intervention dose, WhatsApp group, and delivery mode were appropriate.
Conclusions
According to these findings, the i-MaCHeL intervention using a web-based approach was feasible, usable, and acceptable as part of a weight-related behaviour change intervention for preschool child–parent dyads. This pilot study demonstrated that the web-based i-MaCHeL was feasible and promising for delivering weight-related behavioural intervention to child–parent dyads.
Trial registration
ClinicalTrials.gov, NCT04711525. Registered on January 15, 2021.
Similar content being viewed by others


Key messages regarding feasibility
-
A web-based health-related programme could be an effective strategy for making health-related programmes more accessible to families, particularly those with socioeconomic disadvantages. Although these programmes show promise, little is known about the feasibility, usability, and acceptability of these intervention programmes within the preschool child–parent dyads population in Malaysia.
-
The 13-week web-based i-MaCHeL programme delivered to preschool child–parent dyads was feasible, usable, and acceptable. The intervention process evaluation data indicated that at least 92.9% (39/42) of the parents agreed/strongly agreed that the web content, programme duration, intervention dose, WhatsApp group, and delivery mode were appropriate. This pilot study demonstrated that the web-based approach was an effective delivery mode for preschool child–parent dyads.
-
The study findings suggest that the i-MaCHeL intervention was highly scalable and warrants further investigation using a fully powered definitive cluster-RCT design to evaluate the effectiveness of the programme in improving child weight-related and dietary outcomes.
Background
Poor nutritional status, especially childhood obesity, is considered one of the most significant public health issues worldwide. Childhood obesity is associated with type 2 diabetes and heart disease in adult life and middle-age mortality [1]. In Malaysia, overweight and obesity coexist with being underweight among children and adolescents. In 2019, the National Health and Morbidity Surveys (NHMS) reported that 29.8% of children and adolescents aged 5 to 17 years were overweight or obese, and another 10% were underweight [2]. During early childhood, lifestyle behaviours that promote obesity are just being learned, and it is easier to establish new behaviours than to change the existing ones [3]. Moreover, health behaviours become more difficult to change with age and tend to track into adulthood but are quite malleable in the early years [4].
The features of preschool such as policies and practices regarding dietary intake and physical activity pose a realistic setting for delivering health-related behaviour change programmes at an early age [5, 6]. Furthermore, preschools represent an ideal setting to address social inequalities because they provide access to the community and generally have the necessary facilities, curriculum, environment, and personnel to promote a healthy lifestyle [7]. These include the organisational structure and the high level of trust that children and parents attach to preschool staff [8]. Considering the severe consequences of childhood obesity and the high likelihood of becoming obese in adulthood [9], there is a strong rationale to develop a comprehensive and effective weight-related behavioural intervention for preschool children.
Parents play a significant role in shaping the home food environment and influencing the child’s dietary behaviours [10]. Therefore, partnerships with parents to promote healthy lifestyle changes might have a lifelong impact on child weight-related outcomes. It is well established that targeting both children and parents in health-related behavioural intervention produces more significant impacts [11]. Therefore, obesity prevention is likely to have optimal effects if started in early childhood with parental involvement, as young children are generally guided by parents in their dietary intake and physical activity levels [12]. Notably, most web- and digital-based weight-related behavioural interventions in preschool-aged children were conducted in high-income developed countries; few were done in upper-middle-income developing countries [1, 11, 13]. To date, however, limited web-based intervention programmes targeting multifactorial weight-related behaviours (healthy eating, active physical activity, and sedentary behaviour) for preschool children that include parents are conducted in developing countries [1], especially in Malaysia.
The use of Information and Communication Technology (ICT) in adolescent and adult age groups has increased in recent years. A report by the Department of Statistics Malaysia on ICT use and access by individuals and households survey indicated that the percentage of individuals aged ≥15 years that used the internet was 83.5% in 2021, which increased by 2.3% as compared to 81.2% in 2018 [14, 15]. The data also indicated that the percentage of households’ access to the internet increased by 12.5 to 95.5% in 2021 as compared to 87.0% in 2018. Meanwhile, the percentage of households that have access to mobile phones also increased by 1.4 to 99.6% in 2021 as compared to 98.2% in 2018 [14, 15]. The high internet and mobile phone access highlighted the importance of the web-based approach for effective home-based intervention programmes, especially in Malaysia. It is well-documented that sustaining the engagement of both children and parents in long-term weight-related interventions is a significant challenge [10]. With the increasing number of households having access to mobile phones, tablets, and personal computers [16, 17], the web-based approach using these technologies could be used to improve adherence to the intervention programme. Furthermore, the speed at which individuals communicate and respond through mobile phones is advantageous for online intervention programmes [18]. It is well understood that distributing information and materials online increases the availability of the intervention, making it easy for parents to find and use health-related information at their convenience [6].
Considering that most face-to-face parent interventions have low retention and high dropouts [19], the web-based approach has the potential to increase participants’ adherence to the intervention programme [20]. Previous studies demonstrated that web-based intervention delivery methods were feasible, cost-effective, and acceptable in improving the weight-related behaviours of children [20,21,22]. Moreover, a web-based health-related programme could also be an effective strategy for making health-related programmes more accessible to families, particularly those with socioeconomic disadvantages [23, 24]. Although these studies show promise, little is known about the feasibility of these intervention programmes within the preschool child–parent dyads population in Malaysia. There has been considerable emphasis on the importance of usability testing for improving web-based interventions [25,26,27]. However, few studies have assessed the usability and acceptability of the web-based programme designed for child–parent dyads. Usability testing is a crucial step in the development of web-based and mobile-friendly programmes to ensure the programmes are accessible, effective, satisfying, and culturally competent [10, 28].
In Malaysia, the escalating rates of childhood obesity present a public health challenge that demands innovative intervention strategies. The Interactive Malaysian Childhood Healthy Lifestyle (i-MaCHeL) programme, a web-based initiative designed for preschool child–parent dyads, offers a novel approach to addressing this issue. Nevertheless, the success of such a web-based intervention depends on several interrelated factors. This research aims to investigate the viability of i-MaCHeL programme, focusing on its feasibility in the Malaysian context, the usability of its web-based platform for preschool child–parent dyads, and the acceptability of the programme among these user groups. This study was undertaken to provide quantitative data in designing a definitive cluster randomised controlled trial (RCT), allowing refinement of the study components, including the protocol, processes, and outcomes.
Objectives
In general, this study aims to provide quantitative data on feasibility, usability, and acceptability of i-MaCHeL programme for tailoring a large-scale definitive cluster-RCT. The specific objectives of this study are (1) to determine the intervention feasibility of the web-based i-MaCHeL programme among preschool child–parent dyads, (2) to assess the usability of the web-based i-MaCHeL programme among parents of preschool children, and (3) to assess the acceptability of the intervention process of the web-based i-MaCHeL programme among parents of preschool children.
Materials and methods
Research design
The trial design elements of this study are described in accordance with the Consolidated Standard of Reporting Trials (CONSORT) guidelines for pilot and feasibility studies (see Additional file 1) [29] and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (see Additional file 2) [30]. A total of 46 child–parent dyads from six government preschools in Terengganu, Malaysia, were recruited. As this was a pilot study and not hypothesis testing, no formal sample size calculation was conducted [31, 32]. It was also of note that the sample size of this pilot study (\(n\) = 46) was 20% from the intended population of the experimental group arm (\(n\) = 230) in our main cluster-RCT [33]. In addition, this pilot study was in accordance with recommendations by Ullman et al. (2016) [34] to minimise unnecessary costs, time, and recruitment of the definitive study participants. The quantitative data on the usability and acceptability of the web-based i-MaCHeL was gathered through self-administered web-based surveys. Besides that, the feasibility data was obtained from the number of participants who completed the study (retention rate) and the attendance percentage of participants in the intervention sessions (attendance rate). Comments and recommendations for improvement were also collected to supplement quantitative data.
Participants and setting
The web-based i-MaCHeL was pilot-tested among preschool child–parent dyads for 3 months with a focus on feasibility, usability, and acceptability outcomes. For this purpose, a total of 46 child–parent dyads that had similar characteristics to our study population were recruited to confirm the feasibility, usability, and acceptability of the newly developed web-based intervention programme.
Using the cluster random sampling technique at the preschool level, six preschools in Terengganu, Malaysia, were randomly selected to participate in this study. All preschools within Kuala Terengganu and Kuala Nerus districts were eligible for inclusion. There were 71 preschools in both districts. Because of varying cluster sizes, the preschools with insufficient children (fewer than 26 children) were excluded from the study [35]. After screening for inclusion, 37 preschools were eligible to participate in the present study. All 37 eligible preschools were assigned a unique identification number and randomly ordered by an independent researcher using a random number generator software (Research Randomizer version 4.0) [36] to generate a list of random numbers. The eligible preschools were then sequentially invited by email and a phone call to achieve the target number of six preschools. Within participating preschools, the child–parent dyads that did not meet eligibility criteria, were no longer interested, or unwilling to complete the baseline surveys were excluded from the study. In total, 46 child–parent dyads that fulfilled the eligibility criteria, consented, and completed the baseline assessment were included in the study. Participant recruitment and data collection for the pilot study were conducted between June and December 2021.
Eligibility criteria for preschool child–parent dyads
The eligibility criteria for the single-arm pilot study were in accordance with our main cluster-RCT study [33]. All preschool children aged 6 years and their parents were eligible for inclusion in the recruitment phase. The parent/guardian of the children was eligible for the study if they (1) could read and understand either English or Malay; (2) were aged between 25 and 49 years; (3) had regular internet access via a tablet device, mobile phone, or computer/laptop; (4) had regular access to a phone with texting capability; (5) had WhatsApp accounts or agreed to create the accounts, and (6) were comfortable to read/view materials on electronic devices. Child–parent dyads were excluded if (1) the children were taking medications or had a medical condition with the potential to affect their weight or restrict age-appropriate play; (2) the children had conditions that require the restriction of certain foods (e.g. celiac disease or food allergies), and; (3) the parents suffer from a severe physical or psychological illness, making the study too demanding for the family.
Web-based i-MaCHeL intervention process
In the present study, the web-based i-MaCHeL was designed with an innovative approach to deliver a health-related behaviour change programme for preschool child–parent dyads. The web-based i-MaCHeL was developed to be accessible on both desktop and mobile phone platforms. The i-MaCHeL consists of 13 web-based modules related to healthy eating, active physical activity, and sedentary behaviour of preschool-aged children. Distinctive features of web-based i-MaCHeL intervention include access to various health-related educational information such as infographics, reading materials, informative videos, relevant pictures, and interactive parent–child activities designed to increase child–parent engagement in health-related behaviour change programmes. The compilation of helpful guides and tips related to children’s healthy lifestyles, healthy recipes for kids, and a BMI calculator were also provided on the web-based i-MaCHeL. Besides that, the WhatsApp group was incorporated as a natural extension for the web-based i-MaCHeL programme to encourage participation and adherence to the intervention programme. The WhatsApp group was utilised to provide notification functions for newly available modules, weekly reminders to complete the modules, and motivational text messages to participants [23, 37]. The preschool child–parent dyads were asked to complete 13 modules over a 3-month period (one module per week). In order to ensure the web-based programme is functional at all times, the digital media content, online activities, and web interfaces were regularly improved and monitored to address technical issues in a timely manner, including accommodating any operating system updates [38].
Data collection and instruments
Demographic characteristics
Demographic information was collected from parents at the baseline data collection point. Parents were asked to proxy-report general information about their family unit. Sociodemographic information of children and their families, which include a child’s sex, ethnicity, date of birth, the number of children under 18 years old living in the household, household income, parents’ age, education level, current working status, and current marital status, were collected. Household incomes were categorised into three groups (low, middle, and high incomes) based on the standard income classification of Malaysia [39].
Intervention feasibility
The intervention feasibility was determined based on the percentage of participants in the study who completed the intervention programme (retention rate) and the attendance percentage of participants in the intervention sessions (attendance rate). The attendance of the participants for every session was monitored using online completion forms. The completion forms were completed by parents upon the completion of every module throughout the 13-week intervention programme.
Usability testing
The System Usability Scale (SUS) adapted from Brooke (1986) [40] was used to assess the usability of the web-based i-MaCHeL. The SUS measures usability from the perspectives of effectiveness, efficiency, and satisfaction of the i-MaCHeL website platform. The SUS comprises a simple 10-item instrument using a 5-point Likert scale ranging from ‘strongly disagree’ to ‘strongly agree’ (see Table 2). The word ‘system’ in the SUS questionnaire was replaced with the term ‘website’ to make the questions more appropriate for the web-based programme [25, 41]. Total SUS scores range from 0 to 100; a higher score indicates a better usability test [42]. The total SUS score was calculated by summing up the score contributions from each item. The score contribution for each item ranges from 0 to 4. For items 1, 3, 5, 7, and 9, the score contribution was the scale position minus 1. For items 2, 4, 6, 8, and 10, the score contribution was 5 minus the scale position. Then, multiply the sum of the scores by 2.5 to obtain the total SUS score [40].
User acceptability
The process evaluation questionnaire adapted from Hammersley et al. (2019) [4] was used to assess the acceptability of the 13-week web-based i-MaCHeL intervention programme. The questionnaire was designed to evaluate user acceptability with the web content, programme duration, intervention dose, WhatsApp group, and mode of delivery. A 5-point Likert scale with the response ranging from ‘strongly disagree’ to ‘strongly agree’ was used in the process evaluation questionnaires.
The usability testing and user acceptability of the web-based i-MaCHeL programme were assessed immediately following the completion of the 13-week web-based intervention programme. The parents were asked to independently complete self-administered web-based surveys at the end of the programme. The force step completion function was used in the web-based surveys to prevent missing data, so informants could only continue with the questionnaire when all items were completed. Feedback and comments to improve the web-based i-MaCHeL were also obtained from the parents through the surveys. The data and feedback obtained from this pilot study were analysed to further improve the development process and ensuing hypothesis testing of the definitive cluster-RCT.
Statistical analysis
Participant sociodemographics, System Usability Scale (SUS), and intervention process evaluation data were analysed using descriptive statistical analysis. The data were provided as mean (SD) or number (percent). The SUS instrument yields a single number representing a composite measure of the overall usability score of the web-based i-MaCHeL. Analyses were performed using Statistical Product and Service Solutions (SPSS; version 25.0; IBM, Armonk, NY, USA).
Ethical considerations
This study was approved by the Universiti Sultan Zainal Abidin Human Research Ethics Committee, Malaysia, on August 24, 2020, with reference No. UniSZA/UHREC/2020/184. The ethics committees approved the consent form, information letter, and study consent procedure. The study protocol was registered with ClinicalTrials.gov on January 15, 2021 (Identifier No: NCT04711525). Written informed consent was obtained from all parents/caregivers prior to the commencement of the pilot study. The consent to participate was obtained from the parents of preschool children. Once consent forms were collected and eligible child–parent dyads were determined, the child–parent dyads were enrolled in the single-arm pilot study. The participants were given the right to refuse or not to participate in the study. No financial compensation was provided for all participants. Participants were entitled to withdraw from the study at any point and do so with no disadvantage. Participation in the study could be discontinued at all times with no obligation to provide a reason.
Results
Intervention feasibility
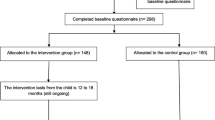
All 13 modules of the web-based i-MaCHeL were successfully delivered to the child–parent dyads within 13 weeks of the intervention programme (one module per week). A total of 46 child–parent dyads were enrolled in the intervention programme at the baseline. However, only 42 participants with an attendance rate of > 75% (completed at least 10 out of 13 modules) had successfully completed the intervention programme and post-test assessments. The other 4 participants who discontinued participation with an attendance rate of < 50% (completed less than seven modules) and refused to respond to communication attempts (calls, emails, and texts) were designated as lost to follow-up. Overall, this study demonstrated that the retention rate of the intervention programme was 91.3% (42/46) (Fig. 1).

Flow chart of the i-MaCHeL programme trial
At baseline, all recruited parents were Malays. Almost all parents were female (42/46, 91.3%) and married (41/46, 97.8%). More than three-quarters of them (32/46, 69.6%) had an age range between 30 and 39 years old. This study managed to recruit preschool children with just over half of their fathers (24/46, 52.2%) and 41.3% (19/46) of their mothers without college or university education. It was also noted that more than half of their mothers (27/46, 58.7%) were not working (housewives). This study also indicated that 43.4% (20/46) of their fathers worked in the private sector. The data demonstrated that nearly two-thirds (30/46, 65.3%) of the parents came from low-income households. In addition, most (43/46, 93.5%) participating parents indicated that they had less than five children aged under 18 years. Details of the demographic characteristics of study participants were provided in Table 1.
Usability testing
The mean and standard deviation (SD) for the raw scores for each statement in the SUS instrument by parents were presented in Table 2. The statements for the positive responses (items 1, 3, 5, 7, and 9) of the SUS subscale showed that the mean (SD) score of the parents ranged from 4.45 (0.71) to 4.69 (0.52). The statements for the negative responses (items 2, 4, 6, 8, and 10) of the SUS subscale reported that the mean (SD) score of the parents ranged from 1.69 (0.92) to 2.10 (1.41). The internal consistency of the parents’ responses was also assessed to determine the reliability of the 10-item SUS instrument. Cronbach’s alpha coefficient analysis was performed, and Cronbach’s alpha obtained was 0.84, indicating that the SUS instrument had good reliability (Cronbach’s alpha of at least 0.80) [43].
This study categorised the SUS cumulative scores into 7-scale adjective ratings. The corresponding 7-scale adjective ratings and SUS cumulative scores of the parents on a scale of 0–100 were presented in Table 3. The data showed that 38.2% (16/42) of the parents rated the website as ‘best imaginable’, followed by 23.8% (10/42) who rated the website as ‘excellent’. Another 19.0% (8/42) of parents rated the website as ‘good’. The exact value of another 19.0% (8/42) rated the website as ‘OK’. In addition, analysis of the SUS score yielded an overall mean (SD) value of 84.70 (13.82) among parents (see Table 3). The overall mean SUS score of ≥ 70 points was considered acceptable for usability measures [42]. Therefore, the data indicated that the parents agreed that the web-based i-MaCHeL had acceptable usability. The high usability scores point to the potential of the web-based approach in providing weight-related behavioural intervention for preschool child–parent dyads.
User acceptability
The process evaluation questionnaires were used to assess the user acceptability of the 13-week web-based i-MaCHeL intervention programme. Table 4 shows the intervention process evaluation of the i-MaCHeL programme among parents. The mean (SD) score for every item of the questionnaires ranged from 4.52 (0.63) to 4.83 (0.38). The findings showed that all parents agreed/strongly agreed that the content of the web-based i-MaCHeL programme was interesting, relevant, and easy to understand; the activities in the web-based i-MaCHeL programme were interesting; the information about healthy eating and physical activity in the web-based i-MaCHeL module was adequate, and the information about physical activity and sedentary activity in the web-based i-MaCHeL module was helpful. The data also indicated that 97.6% (41/42) of parents agreed/strongly agreed that one module per week was appropriate; the information about sedentary activity in the web-based i-MaCHeL module was adequate, and the information about healthy eating in the web-based i-MaCHeL module was helpful. Apart from that, 95.2% (40/42) of parents agreed/strongly agreed that the 13-week programme’s duration was appropriate. Besides that, 92.9% (29/42) of parents agreed/strongly agreed that the online delivery mode was suitable. The data demonstrated that the web-based i-MaCHeL was widely accepted by the intended target population.
Discussion
The web-based i-MaCHeL programme was pilot-tested among preschool child–parent dyads to evaluate the feasibility, usability, and user acceptability of the intervention programme. The web-based i-MaCHeL targeted parents as agents of change in promoting the healthy lifestyle of their children [22]. The parents were required to complete all web-based activities in the modules with their children throughout the 3-month intervention program. Given that this was a small pilot study, the study was unable to demonstrate any intervention effect because the sample size was not powered to detect changes in outcomes [38, 44]. Therefore, the proposed study outcome measures of the definitive cluster-RCT were not assessed in this study. Nevertheless, it is important to acknowledge that the web-based i-MaCHeL had a high retention level and was potentially efficacious. The high retention rates might reflect, in part, the web-based delivery mode offered in the present study. In addition, the overall retention rate for the current study was aligned with existing weight-related behaviour studies, which reported retention rates ranging from 78 to 93% [20, 45, 46]. The study findings support the utilisation of the web-based delivery mode as an acceptable mode of delivery for weight-related behavioural intervention among child–parent dyads. The recruitment effort of child–parent dyads through the government preschool was substantial [8]. Engagement with preschool teachers to facilitate recruitment was crucial, as they had established a good rapport with the parents [47]. This study suggested that it was important to build a good relationship with parents and preschool teachers to ensure the response and high adherence to the intervention programme. Considering the high retention rate (91.3%) of the present study at three months post-intervention completion and the lengthening of the proposed follow-up period in the main trial, an a priori goal for the definitive cluster RCT (\(n\) = 460 child–parent dyads) is to retain 75% of participants at the 9-month follow-up [33].
Educational status and household income were commonly used as a proxy for socioeconomic disparities [38]. The government-funded Ministry of Education Malaysia (MOE) preschools were selective in offering the programme to children from socioeconomically disadvantaged families. Therefore, partnership with MOE preschools enables the present study to reach and recruit less vulnerable parents. The flexibility of the web-based approach allows the i-MaCHeL programme to be available for all user demographics and diverse groups of participants. In the present study, the parents, mostly from low-income households, found the web-based i-MaCHeL was usable and acceptable. Furthermore, the findings of this study might be influenced by the ubiquity of the households’ access to the internet and mobile phones, which creates the potential to make web-based i-MaCHeL widely available to parents, including those from low-income families. In addition, electronic technologies have become more available, affordable, and widely adopted across all socioeconomic status and age groups [16]. Therefore, the adherence rates to the web-based programme could be maintained even for families with low socioeconomic status. Given the greater need in socioeconomically disadvantaged families [38], the web-based i-MaCHeL provides a useful delivery mode to engage child–parent dyads in weight-related behavioural intervention.
The advantage of using a web-based delivery mode was demonstrated by the flexibility for participants to join the programme from home or anywhere with an internet connection [48]. The web-based approach had the potential to increase intervention accessibility as the participants could complete the modules of the i-MaCHeL programme remotely at any time without the child–parent having to travel or schedule appointments to attend the intervention programme in a specific setting. The web-based approach of the i-MaCHeL programme was consistent with user preferences and the widespread use of the internet and mobile phones in Malaysia [14]. Previous studies identified that the participants accessed the online intervention via several modalities, including a desktop, smartphone, and tablet [17, 48, 49]. The current web-based programme was designed to be a mobile-friendly interface and optimised for viewing on a mobile phone to improve accessibility and efficiency. The feature offers flexibility as it is not limited to any specific device, permitting participants to use the web-based programme at no additional cost.
This study also incorporated multiple strategies to minimise attrition, which include partnering with preschool teachers and holding a few contests with prizes during the 13-week intervention period. Previously conducted studies reported that parents would like to see some social support components in an online intervention where they could interact with other participants [48]. Therefore, the WhatsApp group (social media platform) was also included as a natural extension of the web-based interventions to increase engagement and prompt participants to visit the web-based i-MaCHeL more frequently. WhatsApp apps provide prompt text delivery, which may influence the participants' responses and adherence to the intervention programme. WhatsApp group is an accessible and convenient platform where the participants have the opportunity to communicate with other members and give prompt responses [37, 50]. In addition, the WhatsApp group served to notify parents when new topics became available on the i-MaCHeL website, a reminder to complete the topics and to spark discussions between parents during the intervention period. These findings supported the utilisation of WhatsApp groups as a push notification function to help increase participants’ engagement with an online intervention. Evidence has shown that additional social media components in combination with health-related behavioural intervention could enhance intervention efficacy [45]. These strategies have been shown to be effective in promoting participants’ involvement and adherence to the intervention programme. The current study was in accordance with previous works that successfully incorporated the social media platform to address health-related behavioural intervention [28, 37, 50].
Prior works that used the System Usability Scale (SUS) demonstrated that the web- and digital-based health-related programmes had acceptable usability among the targeted population [17, 51, 52]. In the present study, the usability data demonstrated that the web-based i-MaCHeL had a positive user experience and was highly usable. No difficulty with site navigation, web interface, or gaining access to the web-based programme was reported by the parents. The study also found that the parents need minimal technical support to navigate the web-based programme. Participants were able to initiate and complete the modules on the web-based i-MaCHeL independently based on written instructions provided on the website, indicating that web-based i-MaCHeL was practical and convenient to use [45]. Based on the feedback provided by the participants, the problem arises due to poor mobile coverage in their residence. However, it did not prevent participants from successfully completing the module on the web-based i-MaCHeL. Although the web-based i-MaCHeL was well received by participants, a few minor improvements, as suggested by participants, such as fixing malfunctioning activities, were applied to the web-based programme.
Intervention process evaluation provides useful data to assess user acceptability with the web-based i-MaCHeL programme. The web-based i-MaCHeL demonstrated high acceptability, as most parents ranked the process evaluation items as ‘agree’ or ‘strongly agree’. The study finding was consistent with previous trials reporting that web-based delivery mode was highly accepted among parents in managing the weight-related behaviour of their children [4, 48]. Parents reported that the web content was informative, helpful, relevant, and easy to understand. Most participants were satisfied with the parent-child online activities and WhatsApp group component. In addition, participants also expressed a strong desire for an online delivery mode, intervention dose (1 module per week), and programme duration (13 weeks). Participants’ high ratings of acceptability and retention levels to the web-based programme suggested that the web-based i-MaCHeL was feasible as a mode of delivery among preschool child–parent dyads. Besides that, the web-based i-MaCHeL provides useful and relevant information about healthy lifestyle resources related to preschool-aged children. The parent–child online activities offered in the programme were designed to reinforce the knowledge learned effectively [38, 44]. The difficulty level of the online activities was tailored for preschool children to motivate them to use the website. Overall, at the end of the programme, the web-based i-MaCHeL received positive comments from parents, indicating that web-based i-MaCHeL was widely accepted by the targeted population. Based on the feedback received, participants were particularly satisfied with the overall web content, web interface, and the information conveyed. This pilot study suggested that it was feasible and deemed acceptable to apply the web-based i-MaCHeL programme among preschool child–parent dyads in the main trial.
Strengths and limitations of the study
The i-MaCHeL programme has several strengths. The i-MaCHeL programme is a web-based and self-paced learning programme designed with an innovative approach in delivering comprehensive information to prevent malnutrition risk among the children population. The application of the web-based approach in delivering health-related behaviour change programmes for preschool child–parent dyads was the first (to our knowledge) in Malaysia to be clearly annotated. In addition, this study contributes to the growing body of evidence supporting the feasibility, usability, and acceptability of using the web-based approach to address child weight-related behaviours. Besides that, the i-MaCHeL employed the multi-component approach by targeting several weight-related behaviour components such as healthy eating, active physical activity, and sedentary behaviour related to preschool-aged children. Addressing multiple behavioural targets is essential to maximise the impact of the weight-related behavioural intervention [11, 13, 28]. Given the greater need in socioeconomically disadvantaged families for health-related behavioural intervention [38], the programme successfully addresses preschool child–parent dyads with low-income households. Prior research demonstrates that the internet was used as a preferred channel for retrieving information about healthy eating, particularly among families with low socioeconomic status [24]. Furthermore, the i-MaCHeL programme provides information and resources to support parents in improving child weight-related behaviours, intending to achieve the optimal nutritional status of preschool-aged children. The programme focuses on early childhood intervention in encouraging children to practice a healthy lifestyle and educating parents to shape home lifestyles for optimal child growth and development. Typically, parents have more influence on the behavioural choices of preschool children than later in childhood [28]. Little research was available targeting child–parent dyads to improve the weight-related behaviours of preschoolers [11].
While promising, several potential limitations in this pilot study need to be addressed in future research. The limitations of this pilot study include its relatively small sample size, primary focus on descriptive data, the absence of a control group for comparison, and short time frame with no follow-up period, which may have contributed to the insufficient power to detect meaningful significance changes in child weight-related outcomes [45]. Although the present study was not powered to detect meaningful differences in child weight-related outcomes, the sample size was sufficient for this preliminary pilot work to provide new insights into the development, usability, acceptability, and feasibility of the web-based i-MaCHeL programme. This pilot study supports future research in investigating the potential effectiveness of the i-MaCHeL intervention with a more representative sample size of preschool child–parent dyads.
Conclusion
The 13-week web-based i-MaCHeL programme delivered to preschool child–parent dyads, mostly from low-income families, was feasible, usable, and acceptable. This single-arm pilot study demonstrated that the web-based approach was an effective delivery mode for preschool child–parent dyads and likely to improve child weight-related and dietary outcomes. Mobile-friendly web-based programmes like i-MaCHeL could be cost-effective and promising for weight-related behavioural intervention. The study supports the development of web-based intervention research focusing on programme effectiveness and translation into primary healthcare services. The study findings suggest that the i-MaCHeL intervention was highly scalable and warrants further investigation using a fully powered definitive cluster-RCT design to statistically evaluate the effectiveness of the programme in improving child weight-related and dietary outcomes. In the definitive cluster-RCT study, we hypothesised that trends in improvements in children’s BMI z-score, dietary intake, physical activity, screen time duration, health-related quality of life, parental self-efficacy, parental role modelling, and parental policies at 3- and 9-month follow-up would be observed [33].
Availability of data and materials
All relevant data from this study were made available.
Abbreviations
- ICT:
-
Information and Communication Technology
- i-MaCHeL :
-
Interactive Malaysian Childhood Healthy Lifestyle
- RCT:
-
Randomised controlled trial
References
Brown T, Moore TH, Hooper L, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev. 2019;7(7):CD001871.
Institute for Public Health, Ministry of Health Malaysia. National Health and Morbidity Survey (NHMS), Vol. I: non-communicable diseases, risk factors and other health problems. 2019. Available from: https://iku.moh.gov.my/images/IKU/Document/REPORT/NHMS2019/Report_NHMS2019-NCD_v2.pdf. Accessed 2 Sept 2023.
Natale RA, Lopez-Mitnik G, Uhlhorn SB, Asfour L, Messiah SE. Effect of a child care center-based obesity prevention program on body mass index and nutrition practices among preschool-aged children. Health Promot Pract. 2014;15(5):695–705.
Hammersley ML, Okely AD, Batterham MJ, Jones RA. An Internet-Based Childhood Obesity Prevention Program (Time2bHealthy) for Parents of Preschool-Aged Children: Randomized Controlled Trial. J Med Internet Res. 2019;21(2):e11964.
Kennedy AB, Schenkelberg M, Moyer C, Pate R, Saunders RP. Process evaluation of a preschool physical activity intervention using web-based delivery. Eval Program Plann. 2017;60:24–36.
Blomkvist EAM, Helland SH, Hillesund ER, Overby NC. A cluster randomized web-based intervention trial to reduce food neophobia and promote healthy diets among one-year-old children in kindergarten: study protocol. BMC Pediatr 2018;18(1):232.
Lubans DR, Smith JJ, Plotnikoff RC, et al. Assessing the sustained impact of a school-based obesity prevention program for adolescent boys: the ATLAS cluster randomized controlled trial. Int J Behav Nutr Phys Act. 2016;13:92.
Li B, Liu WJ, Adab P, et al. Cluster-randomised controlled trial to assess the effectiveness and cost-effectiveness of an obesity prevention programme for Chinese primary school-aged children: the CHIRPY DRAGON study protocol. BMJ Open. 2017;7(11):e018415.
Ang YN, Wee BS, Poh BK, Ismail MN. Multifactorial influences of childhood obesity. Curr Obes Rep. 2013;2(1):10–22.
Leung MM, Mateo KF, Verdaguer S, Wyka K. Testing a Web-Based Interactive Comic Tool to Decrease Obesity Risk Among Minority Preadolescents: Protocol for a Pilot Randomized Control Trial. JMIR Res Protoc. 2018;7(11):e10682.
Bleich SN, Vercammen KA, Zatz LY, Frelier JM, Ebbeling CB, Peeters A. Interventions to prevent global childhood overweight and obesity: a systematic review. Lancet Diabetes Endocrinol. 2018;6(4):332–46.
Nixon CA, Moore HJ, Douthwaite W, Gibson EL, Vogele C, Kreichauf S, et al. Identifying effective behavioural models and behaviour change strategies underpinning preschool- and school-based obesity prevention interventions aimed at 4-6-year-olds: a systematic review. Obes Rev. 2012;13(SUPPL. 1):106–17.
Zarnowiecki D, Mauch CE, Middleton G, et al. A systematic evaluation of digital nutrition promotion websites and apps for supporting parents to influence children's nutrition. Int J Behav Nutr Phys Act. 2020;17(1):17.
Department of Statistics Malaysia. ICT use and access by individuals and households survey report. 2021. Available from: https://www.dosm.gov.my/portal-main/release-content/ict-use-and-access-by-individuals-and-households-survey-report-malaysia-2021. Accessed 2 Sept 2023.
Department of Statistics Malaysia. ICT use and access by individuals and households survey report. 2018. Available from: https://www.dosm.gov.my/portal-main/release-content/ict-use-and-access-by-individuals-and-households-survey-report-malaysia-2018#:~:text=Overview&text=In%202018%2C%20percentage%20of%20individuals,70.5%20per%20cent%20in%202018. Accessed 2 Sept 2023.
Sze YY, Daniel TO, Kilanowski CK, Collins RL, Epstein LH. Web-based and mobile delivery of an episodic future thinking intervention for overweight and obese families: a feasibility study. JMIR mHealth uHealth. 2015;3(4):e4603.
Browne S, Kechadi MT, O'Donnell S, et al. Mobile Health Apps in Pediatric Obesity Treatment: Process Outcomes From a Feasibility Study of a Multicomponent Intervention. JMIR Mhealth Uhealth. 2020;8(7):e16925.
McManama O’Brien KH, LeCloux M, Ross A, Gironda C, Wharff EA. A pilot study of the acceptability and usability of a smartphone application intervention for suicidal adolescents and their parents. Arch Suicide Res. 2017;21(2):254–64.
Gomes AI, Pereira AI, Roberto MS, Boraska K, Barros L. Changing parental feeding practices through web-based interventions: A systematic review and meta-analysis. PLoS One. 2021;16(4):e0250231.
Thorén A, Janson A, Englund E, Silfverdal SA. Development, implementation and early results of a 12-week web-based intervention targeting 51 children age 5–13 years and their families. Obes Sci Pract. 2020;6(5):516–23.
Barnes C, Grady A, Nathan N, et al. A pilot randomised controlled trial of a web-based implementation intervention to increase child intake of fruit and vegetables within childcare centres. Pilot Feasibility Stud. 2020;6(1):163.
Wald ER, Ewing LJ, Moyer SCL, Eickhoff JC. An interactive web-based intervention to achieve healthy weight in young children. Clin Pediatr. 2018;57(5):547–57.
Johnson PR, Bushar J, Dunkle M, Leyden S, Jordan ET. Usability and Acceptability of a Text Message-Based Developmental Screening Tool for Young Children: Pilot Study. JMIR Pediatr Parent. 2019;2(1):e10814.
Tobey LN, Koenig HF, Brown NA, Manore MM. Reaching low-income mothers to improve family fruit and vegetable intake: food hero social marketing campaign—research steps, development and testing. Nutrients. 2016;8(9):562.
Verdaguer S, Mateo KF, Wyka K, Dennis-Tiwary TA, Leung MM. A Web-Based Interactive Tool to Reduce Childhood Obesity Risk in Urban Minority Youth: Usability Testing Study. JMIR Form Res. 2018;2(2):e21.
Chia A, Chew MNJS, Tan SYX, et al. A Web-Based Time-Use Application to Assess Diet and Movement Behavior in Asian Schoolchildren: Development and Usability Study of My E-Diary for Activities and Lifestyle (MEDAL). J Med Internet Res. 2021;23(6):e25794.
Campbell A, Hartling L, Plourde V, Scott SD. Parental Knowledge, Self-confidence, and Usability Evaluation of a Web-Based Infographic for Pediatric Concussion: Multimethod Study. JMIR Pediatr Parent. 2022;5(2):e36317.
Ullmann G, Kedia SK, Homayouni R, et al. Memphis FitKids: implementing a mobile-friendly web-based application to enhance parents' participation in improving child health. BMC Public Health. 2018;18(1):1068.
Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355:i5239.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–7.
Hawkins KR, Apolzan JW, Staiano AE, Shanley JR, Martin CK. Efficacy of a home-based parent training-focused weight management intervention for preschool children: the DRIVE randomized controlled pilot trial. J Nutr Educ Behav. 2019;51(6):740–8.
Malden S, Hughes AR, Gibson AM, et al. Adapting the ToyBox obesity prevention intervention for use in Scottish preschools: protocol for a feasibility cluster randomised controlled trial [published correction appears in BMJ Open. 2019 Jan 24;9(1):e023707corr1]. BMJ Open. 2018;8(10):e023707.
Rashid AF, Wafa SW, Abd Talib R, Abu Bakar NM. An interactive Malaysian Childhood Healthy Lifestyle (i-MaCHeL) intervention programme to change weight-related behaviour in preschool child-parent dyads: study protocol of a cluster randomised controlled trial. PLoS ONE. 2022;17(10):e0276843.
Ullman AJ, Kleidon T, Gibson V, et al. Central venous Access device SeCurement And Dressing Effectiveness (CASCADE) in paediatrics: protocol for pilot randomised controlled trials. BMJ Open. 2016;6(6):e011197.
Adab P, Pallan MJ, Lancashire ER, et al. Effectiveness of a childhood obesity prevention programme delivered through schools, targeting 6 and 7 year olds: cluster randomised controlled trial (WAVES study) [published correction appears in BMJ. 2018 May 2;361:k1954]. BMJ. 2018;360:k211.
Urbaniak GC, Plous S. Research randomizer (version 4.0) [computer software]. 2013. Available from: https://www.randomizer.org/. Accessed 2 Sept 2023.
Esentürk OK, Yarımkaya E. Whatsapp-based physical activity intervention for children with autism spectrum disorder during the novel coronavirus (Covid-19) pandemic: a feasibility trial. Adapt Phys Act Q. 2021;38(4):569–84.
Laws RA, Denney-Wilson EA, Taki S, Russell CG, Zheng M, Litterbach E-K, et al. Key lessons and impact of the growing healthy mHealth program on milk feeding, timing of introduction of solids, and infant growth: quasi-experimental study. JMIR mHealth uHealth. 2018;6(4):e9040.
Department of Statistics Malaysia. Report of household income and basic amenities survey. 2016. Available from https://www.dosm.gov.my/portal-main/release-content/report-of-household-income-and-basic-amenities-survey-2016. Accessed 2 Sept 2023.
Brooke J. SUS-A quick and dirty usability scale. Usability Eval Ind. 1996;189(194):4–7.
Teo CH, Ng CJ, Lo SK, Lim CD, White A. A Mobile Web App to Improve Health Screening Uptake in Men (ScreenMen): Utility and Usability Evaluation Study. JMIR Mhealth Uhealth. 2019;7(4):e10216.
Bangor A, Kortum P, Miller J. Determining what individual SUS scores mean: adding an adjective rating scale. J Usability Stud. 2009;4(3):114–23.
Taber KS. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. 2018;48(6):1273–96.
Otis M, Zhu J, Mustafa-Kutana SN, et al. Testing Usability and Feasibility of a Mobile Educator Tool for Pediatric Diabetes Self-Management: Mixed Methods Pilot Study. JMIR Form Res. 2020;4(5):e16262.
Chai LK, Collins CE, May C, et al. Feasibility and efficacy of a web-based family telehealth nutrition intervention to improve child weight status and dietary intake: A pilot randomised controlled trial. J Telemed Telecare. 2021;27(3):146–58.
Morgan PJ, Grounds JA, Ashton LM, et al. Impact of the 'Healthy Youngsters, Healthy Dads' program on physical activity and other health behaviours: a randomised controlled trial involving fathers and their preschool-aged children. BMC Public Health. 2022;22(1):1166.
Hammersley ML, Wyse RJ, Jones RA, et al. Telephone and Web-Based Delivery of Healthy Eating and Active Living Interventions for Parents of Children Aged 2 to 6 Years: Mixed Methods Process Evaluation of the Time for Healthy Habits Translation Trial. J Med Internet Res. 2022;24(5):e35771.
Chai LK, Collins CE, May C, Brown LJ, Ashman A, Burrows TL. Fidelity and acceptability of a family-focused technology-based telehealth nutrition intervention for child weight management. J Telemed Telecare. 2021;27(2):98–109.
Kang NG, You MA. The effects of a smartphone-based education program designed to help mothers safely administer medication to their children. CIN Comput Informatics Nurs. 2023;41(2):77–85.
Ikezawa N, Yoshihara R, Kitamura M, et al. Web-Based Exercise Interventions for Children with Neurodevelopmental Disorders. Pediatr Rep. 2023;15(1):119–28.
Pagoto S, Tulu B, Waring ME, et al. Slip Buddy App for Weight Management: Randomized Feasibility Trial of a Dietary Lapse Tracking App. JMIR Mhealth Uhealth. 2021;9(4):e24249.
Nitsch M, Adamcik T, Kuso S, Zeiler M, Waldherr K. Usability and engagement evaluation of an unguided online program for promoting a healthy lifestyle and reducing the risk for eating disorders and obesity in the school setting. Nutrients. 2019;11(4).
Acknowledgements
The authors wish to sincerely thank the local authorities, preschool teachers, parents, and children in Terengganu, Malaysia, who participated in or supported this study.
Funding
The authors received funding from Universiti Sultan Zainal Abidin (ref no: UniSZA/2021/DPU2.0/14).
Author information
Authors and Affiliations
Contributions
AFA managed data collection, data entering, and analysis, contributed to the study design and website development, and drafted the manuscript. SWW and RAT contributed to the study design, data interpretation, and edited the manuscript. NMA contributed to the website development and reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the Universiti Sultan Zainal Abidin Human Research Ethics Committee, Malaysia, on August 24, 2020, with reference no. UniSZA/UHREC/2020/184. Written informed consent was obtained from all parents/caregivers prior to the commencement of the study. The ethics committees approved the consent form, information letter, and study consent procedure. The study protocol was registered with ClinicalTrials.gov on January 15, 2021 (Identifier No: NCT04711525; https://classic.clinicaltrials.gov/ct2/show/NCT04711525).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rashid, A.F.A., Syed Saadun Tarek Wafa, S.W.W., Talib, R.A. et al. Interactive Malaysian Childhood Healthy Lifestyle (i-MaCHeL) programme: a single-arm pilot study. Pilot Feasibility Stud 10, 80 (2024). https://doi.org/10.1186/s40814-024-01483-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40814-024-01483-7