
Abstract
Background
There is a need to provide highly repetitive and intensive therapy programs for patients after stroke to improve sensorimotor impairment. The employment of technology-assisted training may facilitate access to individualized rehabilitation of high intensity. The purpose of this study was to evaluate the safety and acceptance of a high-intensity technology-assisted training for patients after stroke in the subacute or chronic phase and to establish its feasibility for a subsequent randomized controlled trial.
Methods
A longitudinal, multi-center, single-group study was conducted in four rehabilitation clinics. Patients participated in a high-intensity 4-week technology-assisted trainings consisting of 3 to 5 training days per week and at least 5 training sessions per day with a duration of 45 min each. Feasibility was evaluated by examining recruitment, intervention-related outcomes (adherence, subjectively perceived effort and effectiveness, adverse events), patient-related outcomes, and efficiency gains. Secondary outcomes focused on all three domains of the International Classification of Functioning Disability and Health. Data were analyzed and presented in a descriptive manner.
Results
In total, 14 patients after stroke were included. Participants exercised between 12 and 21 days and received between 28 and 82 (mean 46 ± 15) technology-assisted trainings during the study period, which corresponded to 2 to 7 daily interventions. Treatment was safe. No serious adverse events were reported. Minor adverse events were related to tiredness and exertion. From baseline to the end of the intervention, patients improved in several functional performance assessments of the upper and lower extremities. The efficiency gains of the trainings amounted to 10% to 58%, in particular for training of the whole body and for walking training in severely impaired patients.
Conclusions
Highly intensive technology-assisted training appears to be feasible for in- and outpatients in the subacute or chronic phase after stroke. Further clinical trials are warranted in order to define the most comprehensive approach to highly intensive technology-assisted training and to investigate its efficacy in patients with neurological disorders.
Trial registration
ClinicalTrials.gov Identifier: NCT03641651 at August 31st 2018
Similar content being viewed by others

Key messages regarding feasibility
-
What uncertainties existed regarding the feasibility? Do patients after stroke tolerate highly intensive trainings and how can such extraordinary long trainings be implemented?
-
What are the key feasibility findings? Highly intensive technology-supported training in general is feasible. However, it seems to be feasible only for a subset of patients after stroke with residual functional limitations, only minor cognitive impairment, and a health status allowing to tolerate the training load.
-
What are the implications of the feasibility findings for the design of the main study? Inclusion and exclusion criteria might be less restrictive. The logistics around the training must be taken into account, e.g., how do patients come to the training facility.
Background
Stroke is the second leading cause of death worldwide with 5.5 million deaths in 2016. With more than 80 million stroke survivors worldwide, stroke is a major cause of disability. In spite of declining incidence, improved survival, population growth, and aging may lead to an increase of people living with a stroke [1]. Of all stroke survivors, 20% remain dependent in their mobility [2]. In Europe, the total costs resulting from strokes were 37.4 billion in 2010 [1]. In Switzerland, in 2019, 19.2% of healthcare costs were spent on acute inpatient treatment, while only 2.2% were spent on inpatient rehabilitation and 2.5% for outpatient rehabilitation including physical and occupational therapy [3].
Highly intensive exercise-based rehabilitation improves patient outcomes. There is strong evidence that more intensive training leads to better rehabilitation outcomes in individuals with stroke [4,5,6,7,8] and reduces hospital readmission rates [9]. However, highly intensive exercise-based rehabilitation reported in studies is not generally available. During rehabilitation, individuals post-stroke make significantly less use of their more affected (− 60%) and less affected arm (− 30%) compared with healthy persons [10]. This non-use leads to further impairment [11]. In addition, therapy time during a regular day at a rehabilitation hospital is generally limited, mostly due to management decisions, lack of structured organization, and inefficient use of resources [12]. In four European rehabilitation centers, the amount of therapy offered to individuals with stroke varied considerably from 1 to 3 h per day. Here, less therapy time per day was associated with lower functional recovery [13]. Other research showed that only 4 min of patient activity and as little as 23–32 repetitions were observed during an activity-related arm therapy session [14, 15] and 357 repetitions during a lower extremity therapy session. The awareness that rehabilitation outcome improves with increasing therapy dose has influenced health insurance reimbursement in Switzerland. From January 2022 on, inpatient rehabilitation will only be reimbursed, if patients attend a minimum of 450 min of therapy per week [16]. The increased use of rehabilitation technologies allows one therapist to supervise several patients, thereby offering higher treatment intensity without increasing staff costs.
Discharge from inpatient rehabilitation is usually planned as soon as no inpatient care is needed, on average within the first 6 weeks after stroke which is long before patients reach full recovery. Compared with inpatient rehabilitation, the intensity of outpatient rehabilitation intensity is considerably lower. Reaching the full recovery potential is further threatened by the reduction of the length of stay for inpatient rehabilitation in Switzerland, which has decreased by 12% from 27.1 days in 2002 to 23.8 days in 2019 [17]. As a consequence, many individuals are discharged from rehabilitation considerably short of attaining their optimal potential. In conclusion, more training is required during and after inpatient rehabilitation to exploit the full potential of recovery.
Technology enables robot-assisted and electromechanical gait and arm training, here referred to as technology-assisted-training (TAT). The devices reduce therapists’ physical burden thereby allowing longer training. Exhaustion of the therapist does not limit training duration. After the implementation of such devices, participants performed on average 569 functional arm movements more per session [18] and allowed walking distances of up to 2000 m or 3300 steps within a session [19].
Systematic reviews report positive effects of TAT for gait [20] and upper extremity function [21, 22]. One out of eight gait dependencies could be prevented if patients received TAT for improving walking function in addition to their regular therapy program [20]. More intensive gait TAT programs lead to better outcomes (gait: [20]; arm: [23]). Arm TAT improves activities of daily living and arm function in individuals post-stroke [24, 25].
Even though reviews report comparable effects of arm TAT if compared with conventional therapy [24, 25], TAT is more cost-efficient if one therapist supervises several patients in parallel.
Availability of TAT is still very sparse in outpatient rehabilitation settings though it would support patients exploiting their full potential of recovery. Improving the availability needs overcoming the barriers related to restrictions in healthcare insurance reimbursement.
Randomized controlled trials in outpatient settings are needed to evaluate the cost-effectiveness of highly intensive TAT to improve arm function and gait in patients after a stroke (PaS).
The Swiss RehabTech Initiative (SRTI) is an interest group with the aim to foster the meaningful implementation of technologies into the rehabilitation path, to promote the creation of appropriate reimbursement schemes and to facilitate the inclusion of rehabilitation technologies into the curricula of therapeutic professions.
Since highly intensive TAT is a complex intervention with a number of unknown elements, the present study focuses on the feasibility of a future full-scale randomized controlled trial (RCT) [26]. Such an explanatory trial would be based on multiple centers; therefore, we also planned this feasibility study in four centers. Our objectives were to evaluate (a) recruitment rate, reasons for exclusion, and possibilities to improve recruitment rate; (b) feasibility for centers to follow the standardized treatment protocol for the complex highly intensive technology-assisted rehabilitation intervention; (c) patients’ and therapists’ acceptance of the intervention; and (d) adverse effects of highly intensive TAT. In our study, we focused on highly intensive TAT. Consequently, estimating the effect of highly intensive TAT compared with usual low-dose outpatient treatment was not expected to be conclusive.
Methods
Study design, setting, and ethical approval
A multicenter single-arm feasibility trial was initiated by the SRTI in preparation for a RCT. For that purpose, a longitudinal single-group design was chosen. The study was implemented at four neurological rehabilitation centers across the German-speaking part of Switzerland, Reha Rheinfelden, Kliniken Valens, Klinik Lengg, and Rehaklinik Zihlschlacht, and conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the lead ethical committee of Canton Zurich (BASEC-nr: 2018-01214) with the involvement of the ethical committees of Eastern Switzerland and Northwest and Central Switzerland. The study was registered with clinicalTrials.gov (NCT 03641651).
Our reporting follows the CONSORT 2010 extension guideline on randomized pilot and feasibility trials [27].
Patients and recruitment
Patients were eligible when they fulfilled the following inclusion criteria:
-
Patients with residual hemiparesis after cerebrovascular accident
-
Up to 12 months after the event
-
Primary rehabilitation terminated
-
Able to cognitively comprehend the aim of the project corresponding to equal or more than 22 out of 30 points of the Montreal Cognitive Assessment (MoCA) [28]
-
General health condition allows for intensive rehabilitative training with limited supervision, i.e., clearance of responsible physician
-
Understand written and spoken German language
Patients presenting with any contraindication for the training with the respective devices were not considered for participation.
After study start, all sites recognized recruitment difficulties. Therefore, we amended the protocol and changed the inclusion criteria to include PaS without a restriction on the time after the stroke.
For this feasibility trial, it was planned to recruit five patients at each trial site. Recruitment strategies differed across the study sites: in-house patient database screening, flyer distribution, and direct contact by clinical staff. After a screening visit, written informed consent was obtained before data collection. After consultation of the responsible disciplines (e.g., therapists), the clearance for intensive training of the respective physician was obtained to confirm eligibility of the participant.
Intervention
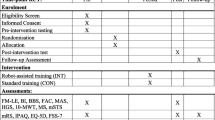
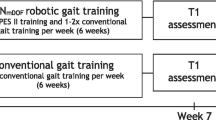
The intervention consisted of a highly intensive four-week TAT in addition to usual care. TAT took place in an outpatient or inpatient setting. Table 1 provides an overview on the interventions based on the Template for Intervention Description and Replication (TIDieR, Table 2 [29];.
Outcomes
For this study, a scoring manual was developed to ensure comparable procedures in each of the participating centers. Characteristics of the included patients (age, sex, BMI, diagnosis, time since stroke, paretic side and cognitive function) were collected at baseline (based on medical records) as recommended by the consensus-based core recommendations from the stroke recovery and rehabilitation roundtable [30]. All co-interventions such as medication or other therapies (e.g., physiotherapy, occupational therapy, psychological counseling, music therapy, water therapy, etc.) during the trial were recorded.
Feasibility-related outcomes: The primary goal of this study was to investigate the feasibility of the intensive TAT, which were evaluated by:
-
The recruitment process (providing recruitment rate, reasons for exclusion and possibilities to improve this process)
-
The feasibility for centers to follow the standardized treatment protocol for the complex highly intensive technology-assisted rehabilitation intervention, and
-
Patients’ and therapists’ acceptance of the intervention incorporated, specifically how well the intensive TAT was tolerated.
Intervention-related outcomes were assessed at every training day in terms of devices used and primarily addressed impairment (lower extremity and gait, upper extremity, other) and duration of training. The following outcomes were evaluated:
-
Patients’ adherence to the prescribed training was evaluated in terms of scheduled vs. actually performed trainings.
-
Subjectively perceived effort of every training was measured with the modified Borg (CR-10 Borg) scale [31].
-
The subjectively perceived effectiveness of training series was evaluated with the Patient’s Global Impression of Change Scale (PGICS) [32]. The PGICS consists of two questions, (1) the amount of change on a seven-point scale which reveals the patient’s overall improvement and (2) the degree of change since the beginning of the study on a 11-point scale (0 = much better, 5 = no change and 10 = much worse). A 2-point change on the 11-point scale was considered clinically meaningful [33]. The PGICS was assessed once at the end of the whole intervention.
-
Adverse events (AE) were recorded to evaluate safety of the assessments and intervention. An AE was defined as any unintended sign, symptom, or disease in a participant, temporally associated with the intervention. A serious adverse event (SAE) was defined as any event which required a hospital stay and/or resulted in permanent or significant incapacity or disability or an event that was life-threatening. Unrelated AEs (event started in no relationship to intervention) were distinguished from related AEs (event started in relationship to the intervention.
Further outcomes can be categorized into patient-related outcomes and efficiency gains.
For patient-related outcomes an assessment battery was set up, consisting of assessments of all components of the International Classification of Functioning Disability and Health [34], as recommended for robot-assisted exercise trials [30]. Participants were assessed at baseline and at the end of the intervention by self-report or by an assessor according to the type of test.
-
Generic functional performance of patients was assessed by the Functional Independence Measure (FIM). The interview-based assessment consists of 18 items, 13 physical domain items and 5 items related to cognition [35]. Based on the level of dependence, each item can be scored from one to seven, with seven indicating complete independence and one indicating complete dependence.
-
For assessing upper extremity motor function, the Fugl-Meyer Assessment - Upper Extremity (FMA - UE) published by See et al. [36] was used. The 33-item assessment evaluates the motor function of the arm and the wrist/hand. The FMA-UE has shown good and well-documented psychometric properties, especially validity, and is recommended for assessing motor function in intervention trials [37]. A FMA-UE score below 25 corresponds to severe impairment, indicating that a person is unable to actively move a robot arm without assistance [38].
-
Gross manual dexterity was evaluated with the Box&Block Test (BBT) [39]. The test was performed in a sitting position. Patients were instructed to transfer a maximum number of wooden blocks from one compartment to another in 60 s. Both the affected and the unaffected side were assessed and compared with age-related norm scores [40].
-
Walking capacity was evaluated with the Walking Index of the Chedoke-McMaster Stroke Assessment (CSMA-WI). The WI is part of the 10-items activity inventory of the CSMA and consists of five items: Walking indoors, walking outdoors (e.g., over rough ground), walking outdoors several blocks, stairs, and the 2-min walk test [41]. All items except for walking distance were rated on a 7-point ordinal scale, where a score of seven indicates complete independence and a score of 1 that full assistance was necessary [42]. Participants’ mobility status was evaluated by using the Functional Ambulation Categories (FAC) assessment developed by Holden et al. (41). Six different categories determine a person’s mobility status and the support needed. A person scoring zero is not able to walk and a person scoring five is fully independent. Usual and maximum gait speed was assessed by the 10- Meter Walking Test (10MWT). Participants had to walk twice the distance of 10 m, first in their usual pace and then in a fast pace (“as fast but as safe as possible”). They were instructed to start two meters in front of the starting line to make sure that gait speed was measured after acceleration.
-
Balance abilities were quantified by the performance-based Berg Balance Scale (BBS) [43]. The BBS consists of 14 tasks with a maximum score of 56. A higher scoring indicates better balance. For all tasks, the patient’s best performance was recorded, independently of the hemiparetic leg.
-
Participation was assessed using following questionnaires:
-
To assess stroke-specific disabilities and quality of life, the German validated version of the Stroke Impact Scale (SIS, 59 items) was used [44, 45]. The SIS assesses function in eight domains (strength, hand function, (instrumental) ADLs, mobility, memory, communication, emotion, social participation, stroke recovery) and the extent of recovery since stroke onset was quantified on a visual analogue scale [45]. Domain scores were scored on a 5-point Likert scale and domain scores calculated ranging from zero to 100.
-
Health-related quality of life was determined by the five-dimension version of the EQ-5D [46]. The manual published by the EuroQol Group was followed [47]. Patients rated each item on a 5-point level. The results were combined to a health state profile (e.g., 15321) as well as transformed into an index value. For that purpose, the Crosswalk Index Value Calculator was downloaded from the online platform of the EuroQoL Group, and the German value set was used [48]. In addition, the self-related health status was rated on a visual analogue scale (EQ VAS).
-
-
Efficiency gains achieved with the application of technological devices were calculated at the end of the study. Here, trainings with devices were compared to trainings without devices regarding required staff for preparation, training, and wrap-up (Table 2).
Due to the study design, there was no control intervention and therefore no randomization and/or blinding procedures were applied. Centers undertook measures to minimize assessor bias. During final assessment, assessors were kept blind to the baseline values.
Data analysis
Patient characteristics, training-related data, and feasibility outcomes were analyzed descriptively. Absolute and relative frequency together with parameters of central tendency and distribution were presented.
Due to the small sample size, pre-post analyses of patient-related outcomes were performed by non-parametrical tests. Wilcoxon Signed-rank test was used to examine differences in pretest and posttest scores. Effect size r was calculated as z statistic divided by square root of the sample size. Additionally, change scores and 95% confidence intervals (CI) were calculated. A 2-sided p value of < 0.05 was considered statistically significant. All analyses were performed using the R language for statistical computing (R Foundation for Statistical Computing; Vienne, Austria).
It should be noted that the inferential statistics reported alongside the estimation of intervention effects should be considered exploratory. The findings are not meant to represent the results of a definite trial nor will they serve as a basis for sample size calculations for a main trial [49].
For the efficiency gain analysis, staff time was presented relative to regular therapy without the respective device.
Results
Enrolment and patient characteristics
Patients were screened and recruited between November 2018 and November 2019 at the four participating centers (Fig. 1 screening and enrolment). Participating patients were diagnosed with stroke between 2 months to 9 years prior to recruitment for the study. Due to a reorganization, one clinic was no longer able to participate.

Screening and enrolment of study participants
Fourteen patients were included in the study and received the intervention at the end of their first inpatient rehabilitation period or in an outpatient setting. Due to the COVID-19 pandemic, one patient in one clinic could not complete all training sessions. Patients’ characteristics are provided in Table 3.
Intervention-related data
Devices used and duration of training
All 14 patients exercised between twelve and 21 days with technological devices. They received between 28 and 82 (mean 46 ± 15) TATs during the study period, which corresponded to two to seven daily interventions. In total, 652 interventions with 20 different devices were undertaken (Table 4). Most trainings were scheduled to either up to 30 min (n = 382) or 31–45 min (n = 210, Table 4).
Patients’ adherence
In general, patients showed a high adherence to their scheduled TAT (Table 5). The number of scheduled and performed trainings correlated with r = 0.56, 95% CI: 0.50–0.61. Adherence rates for different impairments are shown in Fig. 2.

Trainings with technological devices (n = 646) in minutes scheduled vs. actually performed
Perceived exertion (modified Borg scale)
The median perceived exertion on the CR-10 Borg scale during all trainings amounted to 4 (IQR: 3–6). Patients with different impairments reported only small differences of their perceived exertion (Fig. 3).

Perceived exertion during trainings
Adverse events
No serious adverse event was observed. However, 33 adverse events (AE) were reported during or after 652 trainings (5.1%). The AEs were equally distributed over device categories or impairments with 14 occurring during lower extremity and gait trainings (in 4.7% of the trainings), 11 during upper extremity trainings (in 5.5% of the trainings), and 8 during other trainings (in 5.3% of trainings) according to the number of trainings (Table 4).
The most frequent symptoms were tiredness and exertion (n = 17) or pain (n = 14). Two AEs were unrelated to the intervention but were allocated by therapists to lower extremity and gait trainings.
Subjectively perceived effectiveness of training
Meaningful improvement («much improved» or «very much improved») regarding the perceived effectiveness of training series, measured by the PGICS, was reported by 50% of the PaS. A clinically meaningful change was indicated by 35.7% of the PaS.
Patient-related outcomes
Table 6 presents the data on patient-related outcomes for pre- and post-intervention assessment values.
Effect of technology-assisted training on lower extremity and gait
After receiving TAT, participants improved their mean time for the 10MWT from 25.2 s (SD 23.8) during pre-assessment to 21.2 s (SD 15.7) during post-assessment at maximum speed (p = 0.016, r = 0.68). Although statistical analysis was based on the variability of ranks, interpretation of mobility status measured by the FAC should be based on the raw scores. Pre- and post-training median FAC scores improved from 2 to 3.5. A FAC score of two means that participants required assistance from another person in the form of continuous or intermittent manual contact for walking, a FAC score of 3.5 indicates unrestricted walking with only verbal supervision. Walking capacity, monitored by the CSMA-WI, did not show statistically significant improvements.
Effect of technology-assisted training on upper extremity
The participants’ median scores of FMA-UE increased from 16 (IQR 12.5) at baseline to 27.5 (IQR 23.8) after TAT. Statistical analyses indicate significant improvements of both measurements for upper extremity performance (FMA-UE p = 0.002, r = 0.87; BBT p = 0.014, r = 0.74).
Effect of technology-assisted training on generic functional performance and quality of life
Regarding generic functional performance, participants achieved a median 5-point change on the FIM. Improvements relating to QoL were visible in the SIS (p = 0.003, r = 0.78) but not in the EQ-5D Index and the corresponding SIS stroke recovery item.
Cost-specific outcomes
Pertaining to staff-time, TATs were more efficient. Depending on the training goal, the efficiency gains amounted between 10% and 58% (Fig. 4).

Efficiency gain in % staff time. The reference relates to the same trainings without devices
Discussion
In this study, the feasibility of a highly intensive TAT was evaluated in a longitudinal single-group design to evaluate the safety and acceptance of the intervention and to establish its feasibility for a subsequent RCT. Fourteen patients in the subacute and chronic phase after stroke received four weeks of TAT with three to five training days per week in addition to conventional treatment in four neurological rehabilitation centers.
Technology-assisted motor training was implemented in neurological rehabilitation based on theoretical rationale and fundamental research [50]. An important element of the technological assistance is the possibility to train at high intensities, i.e., number of repetitions. Evidence about the effectiveness of TAT for motor rehabilitation becomes established only gradually in an ongoing process. The present study presents a first attempt to address the feasibility of TAT in PaS, who had completed their primary rehabilitation using extraordinarily high intensities as defined by three to five weekly training days each comprising at least five trainings with a duration of 45 min. The duration of this TAT was set at 4 weeks. This duration was considered by consensus to be adequate to evaluate the feasibility of the program. In addition, it was a reasonable time for participating centers to provide equipment and staff. According to the literature, a training duration of at least 2 weeks might be adequate to elicit functional responses. The duration of most repetitive task trainings (84%) included in the Cochrane Review by French et al. [51] was up to 12 weeks. However, 19 of 33 studies (58%) reported a training duration equal to our study, i.e., 4 weeks. The study revealed that only a small fraction of screened patients met the inclusion criteria and consented for participation. The results of the PaS, who participated, suggest that highly intensive TAT is feasible in an inpatient as well as an outpatient setting. Participants attended most scheduled trainings and reported only a low number of undesired events. Besides, the study results indicate improvements in multiple measures of functional performance after highly intensive TAT.
Technology-assisted training
There is a substantial amount of literature concerning the efficacy of TAT and the importance of the therapy dosage in the rehabilitation of stroke patients [23, 52, 53]. Our data confirm these previous results. High-intensity TAT led to clinically meaningful improvements in functional scores as well as in the self-perceived effectiveness, captured by the PGICS. Due to the uncontrolled design of this feasibility study, only an intra-group comparison before and after the 4 weeks of highly intensive TAT was possible. Therefore, we cannot exclude that patients would have equally improved if they had received the same dosage of conventional therapies. Nonetheless, the results are encouraging and should be studied in an adequately powered RCT using rater-blinded assessments.
Feasibility
In the present study, less than 4% of the screened patients finally participated. This is at least partially due to the rigorous inclusion and exclusion criteria. Many patients were excluded because of recurrent stroke, but also because of the absence of residual hemiparesis. A relatively high proportion of patients could not participate due to cardiovascular, respiratory, or orthopedic disease or cognitive impairment. In addition, specifically for outpatients, logistical challenges represented a barrier. The slow recruitment rate persisted even after adapting the inclusion criteria. Given the selected sample, we cannot exclude that highly intensive TAT may be applicable only in a subset of patients without clinically relevant comorbidities or cognitive dysfunction. It appears likely that highly intensive TAT is rather feasible in PaS with an otherwise good general health and preserved cognitive function. Additional studies should investigate to what degree high-intensity TAT is feasible in medically more compromised patients. It can also be hypothesized that highly intensive TAT may be useful in patients with recurrent stroke. Low drop-out rates during the intervention phase however support the assumption that high-intensity TAT is acceptable to PaS and in about the range of comparable studies [54].
Recommendations for further studies
Highly intensive TAT in the present study included a variety of different devices in four different clinics suggesting that this therapy approach could be feasible for a wide range of health care providers. However, the specialized equipment also requires adequately trained personnel in order to set up therapy plans fulfilling the criteria for highly intensive TAT as used in this trial. Current rehabilitation devices unfold their therapeutic potential only if they are used in conjunction with skilled therapeutic staff [50, 55]. Interestingly, the study could be successfully performed under in- and outpatient conditions. This might be attributable to the relatively good health condition of the sample, which was also considered essential for other outpatient rehabilitation programs [56]. The experimental training of this study involved several hours of practicing with the help of technological devices. To keep up motivation has been considered challenging [57]. Participants of the present study attended between 5 and 87.5% of the planned sessions. Lower adherence rates were observed with trainings with a longer duration than 45 min. It is therefore recommended for future trials involving high-intensity TAT to consider the length of training sessions.
The core of this study was intensive motor training in order to maximize functional improvements. The optimal intensity however depends on the actual condition of the participants and needs to be adapted on a regular basis [58]. Here, the degree of exertion was measured by the modified Borg scale, which was acceptable to participants. However, the results revealed a broad ranging from 1 to 10, indicating that not all trainings have been performed at a challenging intensity. Possible explanations may be that participants did not train at their limit during the first sessions, when they still familiarized with the devices, or that they rated later training sessions less strenuous once used to the devices and training. The safety profile with a relatively low proportion of adverse events in relation to the total number of sessions was to be expected and is in line with other reports [59, 60]. No serious adverse events did occur. Adverse events mostly referred to exertion and tiredness or pain and were always transitory. The relative high proportion of tiredness/exertion among the adverse events raises the question whether the modified Borg scale alone can adequately capture cognitive fatigue besides physical exertion. The use of an additional instrument may be warranted. Overall, the study provides evidence that highly intensive TAT is safe in patients in the subacute or chronic phase after a stroke.
Study strengths and limitations
The present study opens new avenues for a more effective rehabilitation of PaS even in outpatient settings. Considering the importance of highly repetitive and intensive therapy programs for the improvement of sensorimotor impairment after stroke, the employment of TAT may facilitate the access of PaS to individualized rehabilitation at adequate intensities.
TAT is associated with a slightly increased preparation time for each session as compared with conventional therapies. However, overall TAT was associated with significant efficiency gains, which resulted in the benefit that higher training intensities could be provided with about the same number of personnel. This means that TAT can be performed with a lower therapist-to-patient ratio than conventional therapies. This preliminary result needs to be confirmed with a sound cost-effectiveness study, since TAT is usually not adequately reimbursed by health insurances and other cost bearers.
There are limitations to this study. Apart from the single-group design and the low ratio of recruited-to-screened patients, one main limitation of the present study was the small sample size. Unfortunately, the envisaged number of 20 patients could not be reached because of the aforementioned recruitment issues, organizational restructuring in one clinic, and the beginning of the COVID-19 pandemic towards the end of the trial. We can therefore not exclude that the low number of participants may have biased the results of the present study.
The calculation of efficiency gains was based on reference values estimated by expert clinicians rather than empirical data. Therefore, efficiency gains observed in this study might be slightly be under- or overestimated. Additionally, not at all study centers assessors were blinded pertaining to the aims of the study aims, which may have led to biased estimates of patient-related outcomes.
Conclusions
This study proposes that highly intensive TAT is feasible for in- and outpatients with subacute or chronic stroke. Highly intensive TAT seems to be effective but may be applicable only in a subset of PaS and presenting with only minor cognitive impairment and in a condition of good general health. Further clinical trials are warranted in order to define the most comprehensive approach to highly intensive TAT and to investigate its efficacy in patients with chronic neurological disorders.
Availability of data and materials
The datasets used/analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- 10mWT:
-
10-meter walk test
- BBS:
-
Berg Balance Scale
- BBT:
-
Box and Block Test
- CMSA:
-
Chedoke-McMaster Stroke Assessment Measure
- EQ-5D:
-
EuroQol-5D
- FAC:
-
Functional Ambulation Categories
- FIM:
-
Functional Independence Measurement
- SIS:
-
Stroke Impact Scale
- TAT:
-
Technology-assisted training
- PGIC:
-
Patient Global Impression of Change
References
Gorelick PB. The global burden of stroke: persistent and disabling. Lancet Neurol. 2019;18:417–8.
Gresham GE, Fitzpatrick TE, Wolf PA, McNamara PM, Kannel WB, Dawber TR. Residual disability in survivors of stroke — the Framingham study. N Engl J Med. 1975;293:954–6.
Bundesamt für Statistik. (2021). Kosten des Gesundheitswesens nach Leistungen - 1995-2019 | Tabelle. In: Bundesamt Für Stat. https://www.bfs.admin.ch/bfs/de/home/statistiken/kataloge-datenbanken/tabellen.assetdetail.16944799.html. Accessed 25 Jun 2021.
Pollock A, Baer G, Campbell P, Choo PL, Forster A, Morris J, et al. Physical rehabilitation approaches for the recovery of function and mobility following stroke. Cochrane Database Syst Rev. 2014;2014(4):CD001920.
Saunders DH, Sanderson M, Hayes S, Kilrane M, Greig CA, Brazzelli M, et al. Physical fitness training for stroke patients. Cochrane Database Syst Rev. 2016;3:CD003316.
van Duijnhoven HJR, Heeren A, Peters MAM, Veerbeek JM, Kwakkel G, Geurts ACH, et al. Effects of exercise therapy on balance capacity in chronic stroke: systematic review and meta-analysis. Stroke. 2016;47:2603–10.
Veerbeek JM, van Wegen E, van Peppen R, van der Wees PJ, Hendriks E, Rietberg M, et al. What is the evidence for physical therapy poststroke? A systematic review and meta-analysis. PLoS One. 2014;9:e87987.
Wist S, Clivaz J, Sattelmayer M. Muscle strengthening for hemiparesis after stroke: a meta-analysis. Ann Phys Rehabil Med. 2016;59:114–24.
Andrews AW, Li D, Freburger JK. Association of rehabilitation intensity for stroke and risk of hospital readmission. Phys Ther. 2015;95:1660–7.
Lang CE, Wagner JM, Edwards DF, Dromerick AW. Upper extremity use in people with hemiparesis in the first few weeks after stroke. J Neurol Phys Ther. 2007;31:56–63.
Taub E, Miller NE, Novack TA, Cook EW, Fleming WC, Nepomuceno CS, et al. Technique to improve chronic motor deficit after stroke. Arch Phys Med Rehabil. 1993;74:347–54.
De Wit L, Putman K, Schuback B, et al. Motor and functional recovery after stroke: a comparison of 4 European rehabilitation centers. Stroke. 2007;38:2101–7.
Putman K, de Wit L, Schupp W, et al. Use of time by physiotherapists and occupational therapists in a stroke rehabilitation unit: a comparison between four European rehabilitation centres. Disabil Rehabil. 2006;28:1417–24.
Hayward KS, Brauer SG. Dose of arm activity training during acute and subacute rehabilitation post stroke: a systematic review of the literature. Clin Rehabil. 2015;29:1234–43.
Lang CE, Macdonald JR, Reisman DS, Boyd L, Jacobson Kimberley T, Schindler-Ivens SM, et al. Observation of amounts of movement practice provided during stroke rehabilitation. Arch Phys Med Rehabil. 2009;90:1692–8.
DefReha_3.0__d.pdf.
Aufenthaltsdauer in Rehabilitationseinrichtungen | OBSAN. https://www.obsan.admin.ch/de/indikatoren/aufenthaltsdauer-rehabilitationseinrichtungen. Accessed 25 Jun 2021.
Flynn N, Froude E, Cooke D, Kuys S. Repetitions, duration and intensity of upper limb practice following the implementation of robot assisted therapy with sub-acute stroke survivors: an observational study. Disabil Rehabil Assist Technol. 2020:1–6.https://doi.org/10.1080/17483107.2020.1807621.
Spiess MR, Jaramillo JP, Behrman AL, Teraoka JK, Patten C. Unexpected recovery after robotic locomotor training at physiologic stepping speed: a single-case design. Arch Phys Med Rehabil. 2012;93:1476–84.
Mehrholz J, Thomas S, Werner C, Kugler J, Pohl M, Elsner B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev. 2017. https://doi.org/10.1002/14651858.CD006185.pub4.
Mehrholz J. Is electromechanical and robot-assisted arm training effective for improving arm function in people who have had a stroke?: a cochrane review summary with commentary. Am J Phys Med Rehabil. 2019;98(4):339–40.
Wu J, Cheng H, Zhang J, Yang S, Cai S. Robot-assisted therapy for upper extremity motor impairment after stroke: a systematic review and meta-analysis. Phys Ther. 2021;101:pzab010.
Mehrholz J, Pohl M, Platz T, Kugler J, Elsner B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst Rev. 2018;9:CD006876.
Chien W-T, Chong Y-Y, Tse M-K, Chien C-W, Cheng H-Y. Robot-assisted therapy for upper-limb rehabilitation in subacute stroke patients: a systematic review and meta-analysis. Brain Behav. 2020;10:e01742.
Mehrholz J, Pollock A, Pohl M, Kugler J, Elsner B. Systematic review with network meta-analysis of randomized controlled trials of robotic-assisted arm training for improving activities of daily living and upper limb function after stroke. J Neuroeng Rehabil. 2020;17:83.
Arain M, Campbell MJ, Cooper CL, Lancaster GA. What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med Res Methodol. 2010;10:67.
Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355:i5239.
Hachinski V, Iadecola C, Petersen RC, et al. National Institute of neurological disorders and stroke-Canadian stroke network vascular cognitive impairment harmonization standards. Stroke. 2006;37:2220–41.
Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687–7.
Kwakkel G, Lannin NA, Borschmann K, et al. Standardized measurement of sensorimotor recovery in stroke trials: consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int J Stroke. 2017;12:451–61.
Williams N. The Borg rating of perceived exertion (RPE) scale. Occup Med. 2017;67:404–5.
Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113:9–19.
Kamper SJ, Maher CG, Mackay G. Global rating of change scales: a review of strengths and weaknesses and considerations for design. J Man Manip Ther. 2009;17:163–70.
(2001) International classification of functioning, disability, and health: ICF. Version 1.0. Geneva; World Health Organization: 2001. ©2001.
Hamilton BB, Laughlin JA, Fiedler RC, Granger CV. Interrater reliability of the 7-level functional independence measure (FIM). Scand J Rehabil Med. 1994;26:115–9.
See J, Dodakian L, Chou C, Chan V, McKenzie A, Reinkensmeyer DJ, et al. A standardized approach to the Fugl-Meyer assessment and its implications for clinical trials. Neurorehabil Neural Repair. 2013;27:732–41.
Bushnell C, Bettger JP, Cockroft KM, et al. Chronic stroke outcome measures for motor function intervention trials: expert panel recommendations. Circ Cardiovasc Qual Outcomes. 2015;8:S163–9.
Sivan M, O’Connor R, Makower S, Levesley M, Bhakta B. Systematic review of outcome measures used in the evaluation of robot-assisted upper limb exercise in stroke. J Rehabil Med. 2011;43:181–9.
Platz T, Pinkowski C, van Wijck F, Kim I-H, di Bella P, Johnson G. Reliability and validity of arm function assessment with standardized guidelines for the Fugl-Meyer test, action research arm test and box and block test: a multicentre study. Clin Rehabil. 2005;19:404–11.
Mathiowetz V, Volland G, Kashman N, Weber K. Adult norms for the box and block test of manual dexterity. Am J Occup Ther. 1985;39:386–91.
Gowland C, Stratford P, Ward M, Moreland J, Torresin W, Van Hullenaar S, et al. Measuring physical impairment and disability with the Chedoke-McMaster stroke assessment. Stroke. 1993;24:58–63.
CMSA Manual and Score Form.pdf.
Berg KO, Wood-Dauphinee SL, Williams JI, Maki B. Measuring balance in the elderly: validation of an instrument. Can J Public Health. 1992;83(Suppl 2):S7–11.
Petersen C, Morfeld M, Bullinger M. Fragebogen über die Folgen eines Schlaganfalls. Fortschr Neurol Psychiatr. 2001;69:284–90.
Duncan PW, Bode RK, Min Lai S, Perera S. Rasch analysis of a new stroke-specific outcome scale: the stroke impact scale11No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the author(s) or upon any organization with which the author(s) is/are associated. Arch Phys Med Rehabil. 2003;84:950–63.
Herdman M, Gudex C, Lloyd A, Mf J, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20:1727–36.
EuroQol Research Foundation EQ-5D-5L User Guide, 2019.
van Hout B, Janssen MF, Feng Y-S, Kohlmann T, Busschbach J, Golicki D, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15:708–15.
Sim J. Should treatment effects be estimated in pilot and feasibility studies? Pilot Feasibility Stud. 2019;5:107.
Gassert R, Dietz V. Rehabilitation robots for the treatment of sensorimotor deficits: a neurophysiological perspective. J Neuroeng Rehabil. 2018;15:46.
French B, Thomas LH, Coupe J, McMahon NE, Connell L, Harrison J, et al. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst Rev. 2016. https://doi.org/10.1002/14651858.CD006073.pub3.
Mehrholz J, Thomas S, Kugler J, Pohl M, Elsner B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev. 2020. https://doi.org/10.1002/14651858.CD006185.pub5.
Straudi S, Severini G, Da Roit M, Pizzongolo LDM, Martinuzzi C, Basaglia N. The dose of robot-assisted gait therapy may influence functional recovery in a multidisciplinary rehabilitation program: an exploratory retrospective study. Int J Rehabil Res. 2020;43:175–82.
Bosomworth H, Rodgers H, Shaw L, et al. Evaluation of the enhanced upper limb therapy programme within the Robot-Assisted Training for the Upper Limb after Stroke trial: descriptive analysis of intervention fidelity, goal selection and goal achievement. Clin Rehabil. 2021;35:119–34.
Budhota A, Chua KSG, Hussain A, et al. Robotic assisted upper limb training post stroke: a randomized control trial using combinatory approach toward reducing workforce demands. Front Neurol. 2021;12:622014.
Langhorne P, Holmqvist L. Early supported discharge after stroke. J Rehabil Med. 2007;39:103–8.
Colombo R, Pisano F, Mazzone A, Delconte C, Micera S, Carrozza MC, et al. Design strategies to improve patient motivation during robot-aided rehabilitation. J NeuroEngineering Rehabil. 2007;4:3.
Guadagnoli MA, Lee TD. Challenge point: a framework for conceptualizing the effects of various practice conditions in motor learning. J Mot Behav. 2004;36:212–24.
Rodgers H, Bosomworth H, Krebs HI, et al. Robot assisted training for the upper limb after stroke (RATULS): a multicentre randomised controlled trial. Lancet. 2019;394:51–62.
Keeling AB, Piitz M, Semrau JA, Hill MD, Scott SH, Dukelow SP. Robot enhanced stroke therapy optimizes rehabilitation (RESTORE): a pilot study. J Neuroeng Rehabil. 2021;18:10.
Acknowledgements
All authors are members of the SRTI study group. Additional members are as follows: Alexandra Menig, Center for Neurological Rehabilitation, Zihlschlacht, Switzerland; Liliana P Paredes, Center for Neurological Rehabilitation, Zihlschlacht, Switzerland; Heike Rosemeier, Rehabilitation Centre Valens, Taminaplatz 1, 7317 Valens, Switzerland.
Funding
This study was funded by a foundation which expressed the wish to keep its name confident.
Author information
Authors and Affiliations
Consortia
Contributions
CSA, JK, JCM, MS, and MW were involved in the development of the study protocol. MS and MW acquired project funding. CSA, JK, and MW were leading in the manuscript development and contributed most of the text. RS and CZ contributed with the clinical aspects. MJE, LR, and CZ were involved in the analyses and production of tables and figures. SW did the economic analysis. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the lead ethical committee of Canton Zurich (BASEC-nr: 2018-01214) with the involvement of the ethical committees of St. Gallen and Northwest and Central Switzerland. The study was registered with clinicalTrials.gov (NCT03641651). Participants gave written informed consent prior to data collection.
Consent for publication
All authors consented for this publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schuster-Amft, C., Kool, J., Möller, J.C. et al. Feasibility and cost description of highly intensive rehabilitation involving new technologies in patients with post-acute stroke—a trial of the Swiss RehabTech Initiative. Pilot Feasibility Stud 8, 139 (2022). https://doi.org/10.1186/s40814-022-01086-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40814-022-01086-0