
Abstract
Background
Several reviews have examined the health benefits of participation in specific sports, such as baseball, cricket, cross-country skiing, cycling, downhill skiing, football, golf, judo, rugby, running and swimming. However, new primary studies on the topic have recently been published, and the respective meta-analytic evidence needs to be updated.
Objectives
To systematically review, summarise and appraise evidence on physical health benefits of participation in different recreational sports.
Methods
Searches for journal articles were conducted in PubMed/MEDLINE, Scopus, SpoLit, SPORTDiscus, Sports Medicine & Education Index and Web of Science. We included longitudinal and intervention studies investigating physical health outcomes associated with participation in a given sport among generally healthy adults without disability.
Results
A total of 136 papers from 76 studies conducted among 2.6 million participants were included in the review. Our meta-analyses of available evidence found that: (1) cycling reduces the risk of coronary heart disease by 16% (pooled hazard ratio [HR] = 0.84; 95% confidence interval [CI]: 0.80, 0.89), all-cause mortality by 21% (HR = 0.79; 95% CI: 0.73, 0.84), cancer mortality by 10% (HR = 0.90; 95% CI: 0.85, 0.96) and cardiovascular mortality by 20% (HR = 0.80; 95% CI: 0.74, 0.86); (2) football has favourable effects on body composition, blood lipids, fasting blood glucose, blood pressure, cardiovascular function at rest, cardiorespiratory fitness and bone strength (p < 0.050); (3) handball has favourable effects on body composition and cardiorespiratory fitness (p < 0.050); (4) running reduces the risk of all-cause mortality by 23% (HR = 0.77; 95% CI: 0.70, 0.85), cancer mortality by 20% (HR = 0.80; 95% CI: 0.72, 0.89) and cardiovascular mortality by 27% (HR = 0.73; 95% CI: 0.57, 0.94) and improves body composition, cardiovascular function at rest and cardiorespiratory fitness (p < 0.010); and (5) swimming reduces the risk of all-cause mortality by 24% (HR = 0.76; 95% CI: 0.63, 0.92) and improves body composition and blood lipids (p < 0.010).
Conclusions
A range of physical health benefits are associated with participation in recreational cycling, football, handball, running and swimming. More studies are needed to enable meta-analyses of health benefits of participation in other sports.
PROSPERO registration number CRD42021234839.
Key Points
-
We found a reduced risk of all-cause mortality associated with cycling (–21%), running (–23%) and swimming (–24%).
-
Running also improves body composition, cardiovascular function at rest and cardiorespiratory fitness, while swimming also improves body composition and blood lipids.
-
Football improves body composition, blood lipids, fasting blood glucose, blood pressure, cardiovascular function at rest, cardiorespiratory fitness and bone strength, while handball improves body composition and cardiorespiratory fitness.
Similar content being viewed by others


Introduction
According to the latest Eurobarometer survey, 55% of European Union citizens participate in sports, usually with the aim to improve health and/or fitness [1]. A large majority of them do not do it regularly [1]. Studies have shown that, by participating in sports, adults can reap a range of health benefits, such as reduced risk of premature mortality, type 2 diabetes and cardiovascular disease and improved lipid profile, body composition, muscle strength and functional capacity [2,3,4,5]. Therefore, recreational sports participation has a large potential to improve the health of the population.
Specific types of sport (e.g. endurance sports and strength sports) may have distinct health benefits owing to their differences in biomechanical characteristics and physiological demands [6, 7]. For example, while endurance sports are more likely to improve cardiovascular function and aerobic fitness, strength sports are generally more likely to improve muscle function and bone health [8, 9]. There may also be differences in health benefits between specific sports disciplines (e.g. tennis and basketball) because each sport entails a unique set of movements that are performed in specific physical, psychological, social and environmental contexts. Therefore, from a public health perspective, it is important to determine health outcomes associated with participation in specific sports. Experts argue that creating ‘health profiles’ of different sports would also facilitate the implementation of health-enhancing programmes in sports clubs [8, 9]. Such evidence may also motivate individuals to increase their participation in sports [1].
Previously, we conducted a systematic review and meta-analysis of health benefits associated with different sports [6]. The review included 47 cross-sectional, 9 longitudinal and 13 intervention studies covering 26 sports and various health outcomes. However, sufficient data were available only for meta-analyses of the associations of football participation with maximal oxygen uptake (VO2max), resting heart rate and fat mass, while evidence for other sports and health outcomes needed to be summarised narratively. The meta-analyses found that football is associated with increased VO2max and resting heart rate, while its association with fat mass was not found to be significant. More recently, several reviews examined health benefits of sports participation. They have covered a range of sports, such as baseball [10], cricket [11], cross-country skiing [12], cycling [13], downhill skiing [5], football [14, 15], golf [3], judo [16], rugby [17], running [18] and swimming [19], generally suggesting favourable health outcomes associated with recreational sports participation. For example, a narrative review suggested that playing football is associated with improved cardiovascular, metabolic and musculoskeletal fitness [14], while a systematic review showed that running is associated with 27% lower risk of all-cause mortality [18].
However, large differences in the methods (e.g. study design, inclusion criteria and data synthesis) used in these reviews make the comparison of their findings challenging. Also, given that most of them were focused on a single sport and that some of them examined only specific outcomes, they could not assess the totality of evidence on health benefits of sports and comprehensively identify research gaps in this area. Importantly, literature searches in most of these reviews were completed several years ago and new primary studies on the health benefits of these sports have since been published. Therefore, the aim of this paper was to systematically review, summarise and appraise the evidence on physical health benefits of participation in different recreational sports.
Methods
Search Strategy
The protocol for this systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database (registration number: CRD42021234839). The review was written according to the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist [20].
The search for relevant studies was performed in the following databases: PubMed/MEDLINE, Scopus, SpoLit, SPORTDiscus, Sports Medicine & Education Index and Web of Science. The keyword ‘sport’ was combined with the keywords for ‘health’ and ‘fitness’ and with a range of keywords describing the study design (Additional file 1). The initial search was performed on 31 May 2020 and covered peer-reviewed articles published after 2012. The search was updated on 30 May 2022. For studies published before 2013, we referred to our earlier systematic review [6]. Two authors independently conducted the study selection from the references obtained in the initial (PO and SE) and updated (ARM and STC) searches. We also performed secondary searches by screening the reference lists of all included papers, lists of papers that cited the included papers, relevant review papers on the associations between sport and health and the authors’ personal database. Two authors independently conducted the initial secondary searches (NS and TM) and updated secondary searches (ARM and STC). Any potential disagreements in study selection were resolved by a third author (DJ).
Inclusion Criteria
Studies were considered for inclusion against the following criteria: (i) the study participants were generally healthy adults without disability (18 + years old); (ii) the study design was either longitudinal (cohort and case–control studies) or interventional (randomised controlled trials and quasi-experimental studies); (iii) the study included a group or groups of people participating in a specific sport (or in multiple sports of which each was represented by a separate group of participants in the analysis) and a comparison group of people who did not participate in the given sport; (iv) the study outcomes were related to physical health; and (v) the study was published in English, German or Finnish. We excluded studies in which the participants were top-level/elite/professional athletes and individuals with disability, frailty or chronic illness. We also excluded studies in which the participation in another sport was the only comparison group, and studies in which the outcome variables were injuries or other acute health problems.
Data Extraction
The following data were extracted from the included intervention studies: (1) the type of study design; (2) the number, sex and age of the participants in each comparison group; (3) the type, length, intensity and frequency of all interventions; and (4) the mean and standard deviation of each outcome variable before and after the intervention in the intervention and control groups. The data extraction was performed by one author (PO) and checked for accuracy by another author (ST).
The following data were extracted from the included longitudinal studies: (1) the type of study design; (2) the number, sex and age of the participants; (3) the duration of the follow-up; (4) the type of sports discipline(s) included in the analyses and the definition of the comparison group; (5) the name and measurement units of each outcome variable; (6) the data analysis method(s) and adjustments for confounding; and (7) the effect size (and its statistical significance and/or confidence interval [CI]) of the association between the participation in a specific sport and the outcome variable. The data extraction was performed by one author (ARM) and checked for accuracy by another author (ZP).
Risk of Bias and Certainty of Evidence
The quality of intervention studies was assessed using the Effective Public Health Practice Project Quality Assessment Tool [21]. The tool assesses six components of a study: (1) selection bias, (2) study design, (3) confounders, (4) blinding, (5) data collection methods and (6) withdrawals and drop-outs. Two authors (PO and AH) performed this evaluation. Any disagreements were resolved by a third author (SK).
The risk of bias in longitudinal studies was assessed using the Newcastle–Ottawa Quality Assessment Scale (NOS) for cohort studies [22]. This scale rates the risk of bias across three domains: (1) selection, (2) comparability and (3) outcome. The evaluation was performed by one author (ARM).
The certainty of evidence was assessed according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) criteria [23]. The evaluation was performed by two authors (NS and ZP) and checked by one author (HP). Given the large number of exposure and outcome variables covered in the meta-analyses, the assessment of certainty of evidence was performed only for cycling, running and swimming participation in relation to all-cause mortality, as a key health indicator.
Statistical Analysis
Random-effects meta-analyses with restricted maximum likelihood estimation were conducted to summarise the effects of participating in a specific sport (compared with no exercise) on a health outcome reported in intervention studies. The effect sizes were presented as the mean difference between the intervention and control group in changes from baseline to follow-up. For studies that did not report Pearson’s correlation between baseline and follow-up scores in the outcome variable, we used a weighted pooled correlation calculated from other studies on the given outcome. In the meta-analyses for which less than two correlation coefficients were reported across studies (i.e. in the analyses with mean arterial pressure, maximal heart rate, VO2max in L/min and peak ventilation as outcome variables), we replaced the missing correlations with 0.50. We did the same in sensitivity meta-analyses for all the remaining outcomes.
To summarise the adjusted hazard ratios (HRs) from longitudinal studies, we conducted random-effects meta-analyses with restricted maximum likelihood estimation. For longitudinal studies that conducted dose–response analyses (e.g. HRs for specific durations of activity) and did not report HRs for comparisons of ‘any’ versus ‘no’ participation in a given sport, in the meta-analysis we included the HR for the lowest dose of activity. We also conducted sensitivity meta-analyses in which we included HRs for the highest dose of activity.
We used the I2, τ2, Cochran’s Q test and prediction intervals to assess the heterogeneity of effect sizes. Low, moderate, substantial and high degree of heterogeneity was indicated by I2 values of 0–40%, 30–60%, 50–90% and 75–100%, respectively [24]. For the meta-analyses that included 10 or more effect sizes, we assessed the publication bias using the contour-enhanced funnel plot and the Egger’s asymmetry test [25]. We also calculated the pooled mean differences using the ‘trim and fill’ method and fail-safe N using the ‘general method’ [26].
The meta-analyses were conducted in R (R Foundation for Statistical Computing, Vienna, Austria), using the ‘metafor’ package [26].
Results
Search Results
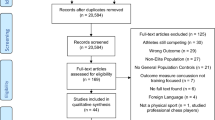
The database search yielded 27,429 papers and an additional 32,250 papers were identified through secondary searches. Following removal of duplicates, and title and abstract screening, 199 papers were left for full-text screening. A total of 80 papers [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106] from 46 intervention studies and 56 papers [7, 107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161] from 30 longitudinal studies were included in the analysis (Fig. 1).

Flowchart of the search and study selection process
Study Characteristics
The intervention studies included ~ 2400 participants and covered the following 19 different sport disciplines: football/soccer (hereafter referred to as ‘football’), running, swimming, alpine skiing, handball, cycling, climbing, volleyball, karate, rugby, basketball, floorball, badminton, tennis, table tennis, judo, golf, equestrian sports and taekwondo. In total, 29 papers from intervention studies included men only, 27 included women only and 24 included both men and women. The health outcomes covered in the intervention studies were: (1) cardiovascular function at rest; (2) cardiorespiratory fitness; (3) body composition; (4) metabolic fitness; (5) muscular fitness; (6) bone strength; and (7) physical performance. A descriptive summary of the intervention studies is presented in Additional file 2.
The longitudinal studies included ~ 2.64 million participants and covered 18 different sport disciplines, including: badminton, basketball, cycling, boxing/karate, football, golf, hockey, ice skating, racquetball, rowing, running, baseball, skiing, swimming, table tennis, tennis and volleyball. In total, 9 papers from the longitudinal studies referred to men only, 5 referred to women only and 42 referred to both men and women. One of the included longitudinal studies was international, with participants from Austria, Belgium, England, Italy, Spain, Sweden and Switzerland. Overall, 2 included papers from longitudinal studies were from Australia, 1 from Canada, 4 from China, 13 from Denmark, 6 from Finland, 1 from France, 5 from the Netherlands, 1 from Russia, 5 from Sweden, 6 from the UK and 11 from the USA. The following health outcomes were covered in the included longitudinal studies: (1) all-cause mortality, (2) cardiovascular mortality, (3) respiratory mortality, (4) diabetes mortality, (5) cancer mortality, (6) mortality from other causes, (7) cancer, (8) colon cancer, (9) breast cancer, (10) venous thromboembolism, (11) atrial fibrillation, (12) aortic stiffness, (13) cardiovascular disease, (14) coronary heart disease, (15) ischemic heart disease, (16) myocardial infarction, (17) stroke, (18) hypertension, (19) obesity or change in body composition, (20) hypertriglyceridemia, (21) impaired glucose tolerance, (22) diabetes, (23) respiratory diseases, (24) chronic obstructive pulmonary disease, (25) asthma, (26) joint diseases, (27) eye diseases, (28) chronic kidney disease, (29) allergies, (30) varicose veins and (31) diseases of the urogenital system. A descriptive summary of longitudinal studies is presented in Additional file 3.
Risk of Bias
The overall methodological quality was rated as moderate for 8 and weak for 72 papers from intervention studies (Additional file 4). The overall methodological quality was rated as fair for 15 and good for 41 papers from longitudinal studies (Additional file 5).
Meta-Analyses of Intervention Studies
Effects of Cycling on Health
We did not find significant effects of cycling on body mass, body mass index (BMI), systolic blood pressure and diastolic blood pressure (p > 0.05 for all; Table 1 and Additional file 6). There was high heterogeneity between the studies on body mass. We did not find significant heterogeneity among the studies on the remaining health outcomes (p > 0.05). The sensitivity analyses confirmed the findings (Additional file 7).
Effects of Football on Health
We found favourable effects of football on body mass, BMI, body fat mass, body fat percentage, total and low-density lipoprotein (LDL) cholesterol, fasting blood glucose, systolic and diastolic blood pressure, mean arterial pressure, resting heart rate, VO2max, peak ventilation, absolute measures of bone mineral content (total and in legs) and osteocalcin (p < 0.050 for all; Table 2). The sensitivity analyses confirmed the findings for all outcomes except for total cholesterol and LDL cholesterol (Additional file 8). In the main meta-analyses, we did not find significant effects of football on the remaining seven health outcomes (p > 0.05 for all). However, in the sensitivity analysis, we found a favourable effect of football on performance in the countermovement jump test (p = 0.031). There was high heterogeneity between the studies on all measures of body composition except for lean mass of legs. High heterogeneity was also found between the studies on high-density lipoprotein (HDL) cholesterol, VO2max (ml/kg/min) and countermovement jump. For most of the remaining health outcomes, heterogeneity between the studies was not found to be significant (p < 0.05). However, in most of the meta-analyses, prediction intervals were relatively wide.
Effects of Handball on Health
We found favourable effects of handball on body fat mass, body fat percentage and VO2max (p < 0.050 for all; Table 3). The sensitivity analyses did not confirm the findings for body fat mass and body fat percentage (Additional file 9). We did not find significant effects of handball on the remaining nine health outcomes (p > 0.05 for all). There was substantial heterogeneity between the studies on HDL cholesterol and VO2max and high heterogeneity between the studies on resting heart rate. For the remaining health outcomes, heterogeneity between the studies was not found to be significant (p < 0.05).
Effects of Running on Health
We found favourable effects of running on body fat mass, body fat percentage, resting heart rate, VO2max and peak ventilation (p < 0.010 for all; Table 4). In the main meta-analyses, we did not find significant effects of running on the remaining nine health outcomes (p > 0.05 for all). However, in the sensitivity analysis, we found a favourable effect of running on BMI (p = 0.003; Additional file 10). There was high heterogeneity between the studies on body mass, BMI, body fat mass, lean body mass and VO2max. For the remaining health outcomes, heterogeneity between the studies was not found to be significant (p < 0.05). However, in most of the meta-analyses, prediction intervals were relatively wide.
Effects of Swimming on Health
We found favourable effects of swimming on body fat percentage, total cholesterol and HDL cholesterol (p < 0.010 for all; Table 5). The sensitivity analysis did not confirm the findings for body fat mass and total cholesterol (Additional file 11). In the main meta-analyses, we did not find significant effects of swimming on LDL cholesterol (p = 0.120) and triglycerides (p = 0.007). However, in the sensitivity analysis, we found a favourable effect of swimming on LDL cholesterol (p = 0.002). There was substantial heterogeneity between the studies on body fat percentage. For the remaining health outcomes, heterogeneity between the studies was not found to be significant (p < 0.050).
Meta-Analyses of Longitudinal Studies
Health Outcomes Associated with Cycling
Cycling was associated with 21%, 10% and 20% lower risk of all-cause, cancer and cardiovascular mortality, respectively, over the follow-up periods (p ≤ 0.001 for all; Table 6). Cycling was also associated with 16% lower risk of coronary heart disease over the follow-up periods (p < 0.001). We did not find a significant association between cycling and the risk of cardiovascular disease (p = 0.230). Sensitivity analyses confirmed all the findings (Additional file 12). There was substantial heterogeneity between the studies on the risk of all-cause mortality and cardiovascular disease. For the remaining health outcomes, heterogeneity between the studies was not found to be significant (p < 0.05).
Health Outcomes Associated with Running
Running was associated with 23%, 20% and 27% lower risk of all-cause, cancer and cardiovascular mortality, respectively, over the follow-up periods (p < 0.05 for all; Table 6). There was substantial heterogeneity between the studies on the risk of all-cause mortality and high heterogeneity between the studies on the risk of cardiovascular mortality. Heterogeneity between the studies on cancer mortality was not found to be significant (p = 0.218). However, prediction intervals were relatively wide in all three meta-analyses.
Health Outcomes Associated with Swimming
Swimming was associated with 24% lower risk of all-cause mortality over the follow-up periods (p = 0.005; Table 6). There was substantial heterogeneity between the studies included in the meta-analysis.
Publication Bias
The Egger’s asymmetry test (Additional files 13, 14, 15 and 16) did not show significant publication bias for the studies included in the meta-analyses of the effects of football on body mass (p = 0.579), body fat percentage (p = 0.796), systolic blood pressure (p = 0.940) and diastolic blood pressure (p = 0.460). In the meta-analyses for body mass and diastolic blood pressure, the pooled mean differences estimated using the ‘trim and fill’ method were the same as the pooled mean differences calculated from the studies included in the original meta-analyses. For body fat percentage and systolic blood pressure, similar results were obtained using the ‘trim and fill’ method when compared with the original meta-analyses (pooled mean difference calculated using the ‘trim and fill’ method [dtf] = –1.69; 95% CI: –2.42, –0.97; p < 0.001 versus pooled mean difference [d] = –1.98; 95% CI: –2.68, –1.28; p < 0.001 for body fat percentage and dtf = –3.75; 95% CI: –6.29, –1.21; p = 0.004 versus d = –4.44; 95% CI: –6.78, –2.09; p < 0.001 for systolic blood pressure). The fail-safe Ns indicated that the number of potential unpublished studies averaging null results needed to increase the p-value for the pooled effect size to 0.05 (i.e. above the statistical significance threshold) would be 16 for body mass, 37 for body fat percentage, 17 for systolic blood pressure and 10 for diastolic blood pressure. The tests were not performed for other meta-analyses owing to the small number of included studies (n < 10).
Certainty of Evidence
The certainty of evidence on the associations of cycling and running with the risk of all-cause mortality was assessed as ‘moderate’, because of substantial heterogeneity between studies (Additional file 17). The certainty of evidence on the association between swimming and the risk of all-cause mortality was assessed as ‘low’, because of high heterogeneity between studies.
Discussion
Key Findings
The key findings of this review are that: (1) cycling is associated with a reduced risk of coronary heart disease and all-cause, cancer and cardiovascular mortality; (2) football has favourable effects on body composition, blood lipids, fasting blood glucose, blood pressure, cardiovascular function at rest, cardiorespiratory fitness and bone strength; (3) handball has favourable effects on body composition and cardiorespiratory fitness; (4) running is associated with a reduced risk of all-cause, cancer and cardiovascular mortality and has favourable effects on body composition, cardiovascular function at rest and cardiorespiratory fitness; and (5) swimming is associated with a reduced risk of all-cause mortality and has favourable effects on body composition and blood lipids.
Comparison with Previous Studies
A previous systematic review [162] showed a 16% lower risk of cardiovascular disease and a 17% lower risk of cardiovascular mortality associated with cycling. We found a somewhat weaker association between cycling and cardiovascular disease and a somewhat stronger association between cycling and a cardiovascular mortality, probably because of additional studies included in the data synthesis. Another systematic review [163] indicated a 23% lower all-cause mortality risk and a 24% lower cardiovascular mortality risk associated with cycling. These results are closely comparable with our findings. Unlike in our review, a previous systematic review [164] found that cycling is associated with lower BMI. This discrepancy between findings may be owing to the fact that our meta-analysis was peformed exclusively on intervention studies in adults, while the previous review also included observational studies and studies conducted among adolescents.
Meta-analyses in our earlier systematic review have shown that football is associated with increased VO2max and lower resting heart rate [6]. Previous reviews also found favourable associations of football with physical and cardiorespiratory fitness, body fat mass, blood pressure, LDL cholesterol and indices of bone health [165, 166]. In the current review, we confirmed these results and additionally found favourable associations between football and body mass, BMI and fasting blood glucose. Unlike a previous review [165], we did not find a significant association between football and performance in the countermovement jump test, possibly because the meta-analysis in the previous review included studies conducted among children and prostate cancer patients in addition to studies conducted among healthy adults.
We did not find any previous review on health benefits of handball that could be used for comparative purposes. We expanded the body of evidence on this topic by conducing meta-analyses on the association between handball and 12 health outcomes and finding favourable associations with body fat and VO2max.
In our previous review [6], we did not find enough studies to conduct meta-analyses on the health benefits of running. Meta-analyses conducted as part of a more recent systematic review [18] found that running is associated with 27%, 30% and 23% lower risk of all-cause, cardiovascular and cancer mortality, respectively. In the current review, we conducted the meta-analyses with larger pooled samples and found very similar effect sizes, which confirmed previous results. Additional studies published since our previous review [6] also enabled us to conduct meta-analyses of the associations of running with 14 other health outcomes and to find that running is beneficial for body composition and cardiorespiratory fitness.
A recent systematic review [167] found favourable associations of swimming with cardiorespiratory fitness and body composition. Our meta-analyses confirmed the finding for body composition and provided additional evidence on the benefits of swimming for blood lipid profile and all-cause mortality risk.
Implications for Clinicians and Policy Makers
Our findings suggest that sports participation can be promoted as part of ‘lifestyle medicine’, to help prevent a range of chronic diseases. This should be facilitated by policy makers through the development and implementation of adequate sports policies with a focus on ‘sport for all’ [8, 9], and by clinicians through direct promotion of sports among their clients.
Previous studies found that the rates of sport related injuries are relatively low but certainly not negligible [6, 168]. The benefits of sports found in the current review likely outweigh the risks; however, a formal evaluation of the health benefits/risks would need to be conducted for different sport disciplines to confirm this. Evidence on health risks associated with sports highlights the need for effective injury prevention measures. A summary of preventive solutions is provided in a recent review [169].
The potential of sports to promote public health remains under-utilised [170]. A recent paper found that medical representatives of international Olympic sport federations rated the importance of preventing chronic diseases in the general population relatively low compared with other health themes/programmes within their federations [171]. Evidence presented in the current review suggests that chronic disease prevention through sports participation should receive greater priority on the agenda of sports organisations.
Strengths and Limitations of the Review and Included Studies
The strengths of the current review include: (1) an extensive literature search that included both backward and forward citation tracking, (2) a large number of included studies that covered various sports and health outcomes and (3) a large number of meta-analyses that were conducted.
The current review also has several limitations. First, in the literature search, we did not use keywords for specific sports and health outcomes, as this would have made it unfeasible. Although this was compensated for by comprehensive secondary searches, it is possible that we missed some relevant studies. Second, while the methodological quality of included longitudinal studies was generally good, most of the included intervention studies rated poorly in terms of blinding and selection bias. The selection bias is very common in intervention trials on the effects of sports participation, because participants are often recruited from those who expressed their interest to participate in a given sport. The blinding of participants is highly impractical or impossible in such intervention trials. Hence, the low scores in these two aspects of study quality were expected. Third, we did not perform dose–response analyses. Given that we conducted 68 meta-analyses of overall effects of sports participation, further dose–response analyses were beyond the scope of this review. Dose–response analyses of the associations between sports participation and health outcomes can be found in previous reviews that were focused on a single sport [18, 163, 172]. Fourth, we considered only physical health outcomes of sports participation. Specific sports may also have distinct associations with various economic, environmental, psychological and social outcomes. Finally, the certainty of evidence was assessed only for the associations of cycling, running and swimming participation with the risk of all-cause mortality. However, this is in accordance with the recommendation that in comprehensive systematic reviews that include many outcome variables, certainty of evidence should be assessed for selected outcomes only [24].
Conclusions
On the basis of the pooled findings from 136 papers, the following can be concluded for recreational sports: (1) cycling reduces the risk of coronary heart disease and all-cause, cancer and cardiovascular mortality; (2) football may help in reducing weight and improving blood lipids, fasting blood glucose, blood pressure, cardiovascular function at rest, cardiorespiratory fitness and bone strength; (3) handball may help in reducing weight and improving cardiorespiratory fitness; (4) running reduces the risk of all-cause, cancer and cardiovascular mortality and may help in reducing weight and improving cardiovascular function at rest and cardiorespiratory fitness; and (5) swimming reduces the risk of risk of all-cause mortality and may help in reducing weight and improving blood lipids.
More studies are needed to enable meta-analyses of physical health benefits of other sports. The quality of future intervention studies in this area could be improved by blinding the assessors, making more appropriate adjustments for confounding, and reducing the drop-out rates.
Availability of Data and Materials
All data relevant to the study are included in the article or uploaded as supplementary information. Further information is available upon reasonable request.
Abbreviations
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
- HDL:
-
High-density lipoprotein
- HR :
-
Hazard ratio
- LDL:
-
Low-density lipoprotein
- NOS:
-
Newcastle–Ottawa Quality Assessment Scale
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- VO2max :
-
Maximal oxygen uptake
References
TNS Opinion & Social. Special Eurobarometer 525: Sport and physical activity: Brussels, Belgium: European Commission;2022.
Luo H, Newton RU, Ma’ayah F, Galvão DA, Taaffe DR. Recreational soccer as sport medicine for middle-aged and older adults: a systematic review. BMJ Open Sport Exerc Med. 2018;4(1):e000336. https://doi.org/10.1136/bmjsem-2017-000336.
Murray AD, Daines L, Archibald D, Hawkes RA, Schiphorst C, Kelly P, et al. The relationships between golf and health: a scoping review. Br J Sports Med. 2017;51(1):12–9. https://doi.org/10.1136/bjsports-2016-096625.
Bangsbo J, Hansen PR, Dvorak J, Krustrup P. Recreational football for disease prevention and treatment in untrained men: a narrative review examining cardiovascular health, lipid profile, body composition, muscle strength and functional capacity. Br J Sports Med. 2015;49(9):568–76. https://doi.org/10.1136/bjsports-2015-094781.
Burtscher M, Federolf PA, Nachbauer W, Kopp M. Potential health benefits from downhill skiing. Front Physiol. 2018;9:1924. https://doi.org/10.3389/fphys.2018.01924.
Oja P, Titze S, Kokko S, Kujala UM, Heinonen A, Kelly P, et al. Health benefits of different sport disciplines for adults: systematic review of observational and intervention studies with meta-analysis. Br J Sports Med. 2015;49(7):434–40. https://doi.org/10.1136/bjsports-2014-093885.
Oja P, Kelly P, Pedisic Z, Titze S, Bauman A, Foster C, et al. Associations of specific types of sports and exercise with all-cause and cardiovascular-disease mortality: a cohort study of 80 306 British adults. Br J Sports Med. 2017;51(10):812–7. https://doi.org/10.1136/bjsports-2016-096822.
Kokko S, Oja P, Foster C, Koski P, Laalo-Häikiö E, Savola J. Sports Club for Health—Guidelines for health-oriented sports activities in a club setting. Helsinki, Finland: Finnish Sport for All Association; 2011.
Koski P, Matarma T, Pedišić Ž, Kokko S, Aoife L, Hartmann H, et al. Sports Club for Health (SCforH)—updated guidelines for health-enhancing sports activities in a club setting. Helsinki, Finland: Finnish Olympic Committee; 2017.
Bullock GS, Uhan J, Harriss EK, Arden NK, Filbay SR. The relationship between baseball participation and health: a systematic scoping review. J Orthop Sports Phys Ther. 2020;50(2):55–66. https://doi.org/10.2519/jospt.2020.9281.
Bullock GS, Perera N, Murray A, Orchard J, Arden NA, Filbay SR. The relationship between cricket participation, health, and wellbeing: a systematic scoping review. Int J Sports Med. 2022;43(5):401–10. https://doi.org/10.1055/a-1686-6632.
Laukkanen JA, Kunutsor SK, Ozemek C, Mäkikallio T, Lee DC, Wisloff U, et al. Cross-country skiing and running’s association with cardiovascular events and all-cause mortality: a review of the evidence. Prog Cardiovasc Dis. 2019;62(6):505–14. https://doi.org/10.1016/j.pcad.2019.09.001.
Grøntved A, Rasmussen MG, Blond K, Østergaard L, Andersen ZJ, Møller NC. Bicycling for transportation and recreation in cardiovascular disease prevention. Curr Cardiovasc Risk Rep. 2019;13:1–8. https://doi.org/10.1007/s12170-019-0623-z.
Krustrup P, Krustrup BR. Football is medicine: it is time for patients to play! Br J Sports Med. 2018;52(22):1412–4. https://doi.org/10.1136/bjsports-2018-099377.
Castillo-Bellot I, Mora-Gonzalez J, Fradua L, Ortega FB, Gracia-Marco L. Effects of recreational soccer on health outcomes: a narrative review. J Sci Sport Exer. 2019;1(2):142–50. https://doi.org/10.1007/s42978-019-0012-9.
Ciaccioni S, Condello G, Guidotti F, Capranica L. Effects of judo training on bones: a systematic literature review. J Strength Cond Res. 2019;33(10):2882–96. https://doi.org/10.1519/jsc.0000000000002340.
Griffin SA, Panagodage Perera NK, Murray A, Hartley C, Fawkner SG, S PTK, et al. The relationships between rugby union, and health and well-being: a scoping review. Br J Sports Med. 2021;55(6):319–26. https://doi.org/10.1136/bjsports-2020-102085.
Pedisic Z, Shrestha N, Kovalchik S, Stamatakis E, Liangruenrom N, Grgic J, et al. Is running associated with a lower risk of all-cause, cardiovascular and cancer mortality, and is the more the better? A systematic review and meta-analysis. Br J Sports Med. 2020;54(15):898–905. https://doi.org/10.1136/bjsports-2018-100493.
Gates A, Cumming I. The health & wellbeing benefits of swimming: individually, societally, economically, nationally. Swim England’s Swimming and Health Commission; 2017.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. 2021;372: n71. https://doi.org/10.1136/bmj.n71.
Effective Public Healthcare Panacea Project. Quality Assessment Tool for Quantitative Studies. 2023 [cited; Available from: http://www.ephpp.ca/tools.html
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute; 2019.
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. Br Med J. 2008;336(7650):924–6. https://doi.org/10.1136/bmj.39489.470347.AD.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions: John Wiley & Sons; 2019.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. Br Med J. 1997;315(7109):629–34. https://doi.org/10.1136/bmj.315.7109.629.
Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1–48. https://doi.org/10.18637/jss.v036.i03.
Andersen LJ, Hansen PR, Søgaard P, Madsen J, Bech J, Krustrup P. Improvement of systolic and diastolic heart function after physical training in sedentary women. Scand J Med Sci Sports. 2010;20(S1):50–7. https://doi.org/10.1111/j.1600-0838.2009.01088.x.
Andersen TR, Schmidt J, Nielsen J, Randers M, Sundstrup E, Jakobsen M, et al. Effect of football or strength training on functional ability and physical performance in untrained old men. Scand J Med Sci Sports. 2014;24(S1):76–85. https://doi.org/10.1111/sms.12245.
Andersen TR, Schmidt JF, Pedersen MT, Krustrup P, Bangsbo J. The effects of 52 weeks of soccer or resistance training on body composition and muscle function in+ 65-year-old healthy males–a randomized controlled trial. PLoS ONE. 2016;11(2): e0148236. https://doi.org/10.1371/journal.pone.0148236.
Aras D, Akalan C. Sport climbing as a means to improve health-related physical fitness parameters. J Sports Med Phys Fitness. 2015;56(11):1304–10.
Aras D, Ewert AW. The effects of eight weeks sport rock climbing training on anxiety. Acta Medica Mediterr. 2016;32(223):223–30. https://doi.org/10.19193/.393-6384_2016_1_35.
Aslan A, Salci Y, Guvenc A. The effects of weekly recreational soccer intervention on the physical fitness level of sedentary young men. Montenegrin J Sports Sci Med. 2019;8(1):51–9. https://doi.org/10.26773/mjssm.190308.
Bangsbo J, Nielsen JJ, Mohr M, Randers M, Krustrup BR, Brito J, et al. Performance enhancements and muscular adaptations of a 16-week recreational football intervention for untrained women. Scand J Med Sci Sports. 2010;20(S1):24–30. https://doi.org/10.1111/j.1600-0838.2009.01050.
Barene S, Holtermann A, Oseland H, Brekke O-L, Krustrup P. Effects on muscle strength, maximal jump height, flexibility and postural sway after soccer and Zumba exercise among female hospital employees: a 9-month randomised controlled trial. J Sports Sci. 2016;34(19):1849–58. https://doi.org/10.1080/02640414.2016.1140906.
Barene S, Krustrup P, Brekke OL, Holtermann A. Soccer and Zumba as health-promoting activities among female hospital employees: a 40-weeks cluster randomised intervention study. J Sports Sci. 2014;32(16):1539–49. https://doi.org/10.1080/02640414.2014.906043.
Barene S, Krustrup P, Jackman S, Brekke O, Holtermann A. Do soccer and Zumba exercise improve fitness and indicators of health among female hospital employees? A 12-week RCT. Scand J Med Sci Sports. 2014;24(6):990–9. https://doi.org/10.1111/sms.12138.
Beato M, Coratella G, Schena F, Impellizzeri FM. Effects of recreational football performed once a week (1 h per 12 weeks) on cardiovascular risk factors in middle-aged sedentary men. Sci Med Footb. 2017;1(2):171–7. https://doi.org/10.1080/24733938.2017.1325966.
Blond MB, Rosenkilde M, Gram AS, Tindborg M, Christensen AN, Quist JS, et al. How does 6 months of active bike commuting or leisure-time exercise affect insulin sensitivity, cardiorespiratory fitness and intra-abdominal fat? A randomised controlled trial in individuals with overweight and obesity. Br J Sports Med. 2019;53(18):1183–92. https://doi.org/10.1136/bjsports-2018-100036.
Carrasco M, Vaquero M. Water training in postmenopausal women: effect on muscular strength. Eur J Sport Sci. 2012;12(2):193–200. https://doi.org/10.1080/17461391.2010.551414.
Celik O, Salci Y, Ak E, Kalaci A, Korkusuz F. Serum cartilage oligomeric matrix protein accumulation decreases significantly after 12 weeks of running but not swimming and cycling training—a randomised controlled trial. Knee. 2013;20(1):19–25. https://doi.org/10.1016/j.knee.2012.06.001.
Cho S-Y, Roh H-T. Taekwondo enhances cognitive function as a result of increased neurotrophic growth factors in elderly women. Int J Environ Res Public Health. 2019;16(6):962. https://doi.org/10.3390/ijerph16060962.
Ciaccioni S, Capranica L, Forte R, Chaabene H, Pesce C, Condello G. Effects of a judo training on functional fitness, anthropometric, and psychological variables in old novice practitioners. J Aging Phys Act. 2019;27(6):831–42. https://doi.org/10.1123/japa.2018-0341.
Connolly LJ, Nordsborg NB, Nyberg M, Weihe P, Krustrup P, Mohr M. Low-volume high-intensity swim training is superior to high-volume low-intensity training in relation to insulin sensitivity and glucose control in inactive middle-aged women. Eur J Appl Physiol. 2016;116(10):1889–97. https://doi.org/10.1007/s00421-016-3441-8.
Connolly LJ, Scott S, Mohr M, Ermidis G, Julian R, Bangsbo J, et al. Effects of small-volume soccer and vibration training on body composition, aerobic fitness, and muscular PCr kinetics for inactive women aged 20–45. J Sport Health Sci. 2014;3(4):284–92. https://doi.org/10.1016/j.jshs.2014.07.003.
de Geus B, Joncheere J, Meeusen R. Commuter cycling: effect on physical performance in untrained men and women in Flanders: minimum dose to improve indexes of fitness. Scand J Med Sci Sports. 2009;19(2):179–87. https://doi.org/10.1111/j.1600-0838.2008.00776.x.
de Geus B, Van Hoof E, Aerts I, Meeusen R. Cycling to work: influence on indexes of health in untrained men and women in Flanders. Coronary heart disease and quality of life. Scand J Med Sci Sports. 2008;18(4):498–510. https://doi.org/10.1111/j.1600-0838.2007.00729.x.
Dela F, Niederseer D, Patsch W, Pirich C, Müller E, Niebauer J. Glucose homeostasis and cardiovascular disease biomarkers in older alpine skiers. Scand J Med Sci Sports. 2011;21(S1):56–61. https://doi.org/10.1111/j.1600-0838.2011.01342.x.
Fristrup B, Krustrup P, Andersen JL, Hornstrup T, Løwenstein FT, Larsen MA, et al. Effects of small-sided recreational team handball training on mechanical muscle function, body composition and bone mineralization in untrained young adults—a randomized controlled trial. PLoS ONE. 2020;15(11): e0241359. https://doi.org/10.1371/journal.pone.0241359.
Helge E, Andersen TR, Schmidt JF, Jørgensen N, Hornstrup T, Krustrup P, et al. Recreational football improves bone mineral density and bone turnover marker profile in elderly men. Scand J Med Sci Sports. 2014;24(S1):98–104. https://doi.org/10.1111/sms.12239.
Helge EW, Aagaard P, Jakobsen MD, Sundstrup E, Randers MB, Karlsson MK, et al. Recreational football training decreases risk factors for bone fractures in untrained premenopausal women. Scand J Med Sci Sports. 2010;20(S1):31–9. https://doi.org/10.1111/j.1600-0838.2010.01107.x.
Hornstrup T, Løwenstein FT, Larsen MA, Helge EW, Póvoas S, Helge J, et al. Cardiovascular, muscular, and skeletal adaptations to recreational team handball training: a randomized controlled trial with young adult untrained men. Eur J Appl Physiol. 2019;119(2):561–73. https://doi.org/10.1007/s00421-018-4034-5.
Hornstrup T, Póvoas S, Helge JW, Melcher PS, Fristrup B, Andersen JL, et al. Cardiovascular and metabolic health effects of team handball training in overweight women: impact of prior experience. Scand J Med Sci Sports. 2020;30(2):281–94. https://doi.org/10.1111/sms.13563.
Hornstrup T, Wikman JM, Fristrup B, Póvoas S, Helge EW, Nielsen SH, et al. Fitness and health benefits of team handball training for young untrained women—a cross-disciplinary RCT on physiological adaptations and motivational aspects. J Sport Health Sci. 2018;7(2):139–48. https://doi.org/10.1016/j.jshs.2017.09.007.
Jakobsen MD, Sundstrup E, Krustrup P, Aagaard P. The effect of recreational soccer training and running on postural balance in untrained men. Eur J Appl Physiol. 2011;111(3):521–30. https://doi.org/10.1007/s00421-010-1669-2.
Jakobsen MD, Sundstrup E, Randers MB, Kjær M, Andersen LL, Krustrup P, et al. The effect of strength training, recreational soccer and running exercise on stretch–shortening cycle muscle performance during countermovement jumping. Hum Mov Sci. 2012;31(4):970–86. https://doi.org/10.1016/j.humov.2011.10.001.
Khadije P, Saeed S, Abdolhamid H. The effect of 6–week recreational futsal training on body composition of non–athletic obese girls. Adv Obes Weight Manag Control. 2018;8(4):220–2. https://doi.org/10.15406/aowmc.2018.08.00247.
Knoepfli-Lenzin C, Sennhauser C, Toigo M, Boutellier U, Bangsbo J, Krustrup P, et al. Effects of a 12-week intervention period with football and running for habitually active men with mild hypertension. Scand J Med Sci Sports. 2010;20(S1):72–9. https://doi.org/10.1111/j.1600-0838.2009.01089.x.
Krustrup P, Christensen JF, Randers MB, Pedersen H, Sundstrup E, Jakobsen MD, et al. Muscle adaptations and performance enhancements of soccer training for untrained men. Eur J Appl Physiol. 2010;108(6):1247–58. https://doi.org/10.1007/s00421-009-1319-8.
Krustrup P, Hansen PR, Andersen LJ, Jakobsen MD, Sundstrup E, Randers MB, et al. Long-term musculoskeletal and cardiac health effects of recreational football and running for premenopausal women. Scand J Med Sci Sports. 2010;20(S1):58–71. https://doi.org/10.1111/j.1600-0838.2010.01111.x.
Krustrup P, Hansen PR, Randers M, Nybo L, Martone D, Andersen LJ, et al. Beneficial effects of recreational football on the cardiovascular risk profile in untrained premenopausal women. Scand J Med Sci Sports. 2010;20(S1):40–9. https://doi.org/10.1111/j.1600-0838.2010.01110.x.
Krustrup P, Nielsen JJ, Krustrup BR, Christensen JF, Pedersen H, Randers MB, et al. Recreational soccer is an effective health-promoting activity for untrained men. Br J Sports Med. 2009;43(11):825–31. https://doi.org/10.1136/bjsm.2008.053124.
Krustrup P, Skoradal MB, Randers M, Weihe P, Uth J, Mortensen J, et al. Broad-spectrum health improvements with one year of soccer training in inactive mildly hypertensive middle-aged women. Scand J Med Sci Sports. 2017;27(12):1893–901. https://doi.org/10.1007/s00421-009-1319-8.
Lauber B, Keller M, Gollhofer A, Müller E, Taube W. Spinal reflex plasticity in response to alpine skiing in the elderly. Scand J Med Sci Sports. 2011;21(S1):62–8. https://doi.org/10.1111/j.1600-0838.2011.01343.x.
Lee B-A, Oh D-J. Effect of regular swimming exercise on the physical composition, strength, and blood lipid of middle-aged women. J Exerc Rehabil. 2015;11(5):266. https://doi.org/10.12965/jer.150242.
Leung K-M, Chung P-K, Hagger MS. The effects of light volleyball intervention programme in improving selected physical and psychological attributes of older adults in Hong Kong. Int J Sport Exerc Psychol. 2020;18(1):1–12. https://doi.org/10.1080/1612197X.2018.1462231.
Liu L, Liu L. The key research of sports in maintaining human health. Rev Bras Med Esporte. 2021;27:335–7. https://doi.org/10.1590/1517-8692202127032021_0088.
Mendham AE, Duffield R, Coutts AJ, Marino F, Boyko A, Bishop DJ. Rugby-specific small-sided games training is an effective alternative to stationary cycling at reducing clinical risk factors associated with the development of type 2 diabetes: a randomized, controlled trial. PLoS ONE. 2015;10(6): e0127548. https://doi.org/10.1371/journal.pone.0127548.
Mendham AE, Duffield R, Marino F, Coutts AJ. Small-sided games training reduces CRP, IL-6 and leptin in sedentary, middle-aged men. Eur J Appl Physiol. 2014;114(11):2289–97. https://doi.org/10.1007/s00421-014-2953-3.
Meyers MC. Effect of equitation training on health and physical fitness of college females. Eur J Appl Physiol. 2006;98(2):177–84. https://doi.org/10.1007/s00421-006-0258-x.
Milanović Z, Pantelić S, Kostić R, Trajković N, Sporiš G. Soccer vs. running training effects in young adult men: which programme is more effective in improvement of body composition? Randomized controlled trial. Biol Sport. 2015;32(4):301–5. https://doi.org/10.5604/20831862.1163693.
Milanović Z, Pantelić S, Sporiš G, Mohr M, Krustrup P. Health-related physical fitness in healthy untrained men: effects on VO2max, jump performance and flexibility of soccer and moderate-intensity continuous running. PLoS ONE. 2015;10(8): e0135319. https://doi.org/10.1371/journal.pone.0135319.
Mohr M, Helge EW, Petersen LF, Lindenskov A, Weihe P, Mortensen J, et al. Effects of soccer vs swim training on bone formation in sedentary middle-aged women. Eur J Appl Physiol. 2015;115(12):2671–9. https://doi.org/10.1007/s00421-015-3231-8.
Mohr M, Lindenskov A, Holm P, Nielsen H, Mortensen J, Weihe P, et al. Football training improves cardiovascular health profile in sedentary, premenopausal hypertensive women. Scand J Med Sci Sports. 2014;24(S1):36–42. https://doi.org/10.1111/sms.12278.
Mohr M, Nordsborg NB, Lindenskov A, Steinholm H, Nielsen HP, Mortensen J, et al. High-intensity intermittent swimming improves cardiovascular health status for women with mild hypertension. BioMed Res Int. 2014;2014. https://doi.org/10.1155/2014/728289.
Møller NC, Østergaard L, Gade JR, Nielsen JL, Andersen LB. The effect on cardiorespiratory fitness after an 8-week period of commuter cycling—a randomized controlled study in adults. Prev Med. 2011;53(3):172–7. https://doi.org/10.1016/j.ypmed.2011.06.007.
Mühlbauer T, Stuerchler M, Granacher U. Effects of climbing on core strength and mobility in adults. Int J Sports Med. 2012;33(06):445–51. https://doi.org/10.1055/s-0031-1301312.
Müller E, Gimpl M, Kirchner S, Kröll J, Jahnel R, Niebauer J, et al. Salzburg Skiing for the Elderly Study: influence of alpine skiing on aerobic capacity, strength, power, and balance. Scand J Med Sci Sports. 2011;21(S1):9–22. https://doi.org/10.1111/j.1600-0838.2011.01337.x.
Naderi A, Goli S, Shephard R, Degens H. Six-month table tennis training improves body composition, bone health and physical performance in untrained older men; a randomized controlled trial. Sci Sports. 2021;36(1):72. e1–e9. https://doi.org/10.1016/j.scispo.2020.02.008.
Narici M, Flueck M, Koesters A, Gimpl M, Reifberger A, Seynnes O, et al. Skeletal muscle remodeling in response to alpine skiing training in older individuals. Scand J Med Sci Sports. 2011;21(S1):23–8. https://doi.org/10.1111/j.1600-0838.2011.01338.x.
Niederseer D, Ledl-Kurkowski E, Kvita K, Patsch W, Dela F, Mueller E, et al. Salzburg Skiing for the Elderly Study: changes in cardiovascular risk factors through skiing in the elderly. Scand J Med Sci Sports. 2011;21(S1):47–55. https://doi.org/10.1111/j.1600-0838.2011.01341.x.
Niederseer D, Steidle-Kloc E, Mayr M, Müller EE, Cadamuro J, Patsch W, et al. Effects of a 12-week alpine skiing intervention on endothelial progenitor cells, peripheral arterial tone and endothelial biomarkers in the elderly. Int J Cardiol. 2016;214:343–7. https://doi.org/10.1016/j.ijcard.2016.03.229.
Nordsborg NB, Connolly L, Weihe P, Iuliano E, Krustrup P, Saltin B, et al. Oxidative capacity and glycogen content increase more in arm than leg muscle in sedentary women after intense training. J Appl Physiol. 2015;119(2):116–23. https://doi.org/10.1152/japplphysiol.00101.2015.
Nybo L, Sundstrup E, Jakobsen MD, Mohr M, Hornstrup T, Simonsen L, et al. High-intensity training versus traditional exercise interventions for promoting health. Med Sci Sports Exerc. 2010;42(10):1951–8. https://doi.org/10.1249/MSS.0b013e3181d99203.
Patterson S, Pattison J, Legg H, Gibson A-M, Brown N. The impact of badminton on health markers in untrained females. J Sports Sci. 2017;35(11):1098–106. https://doi.org/10.1080/02640414.2016.1210819.
Pedersen MT, Vorup J, Bangsbo J. Effect of a 26-month floorball training on male elderly’s cardiovascular fitness, glucose control, body composition, and functional capacity. J Sport Health Sci. 2018;7(2):149–58. https://doi.org/10.1016/j.jshs.2017.12.002.
Pereira R, Krustrup P, Castagna C, Coelho E, Santos R, Helge EW, et al. Effects of recreational team handball on bone health, postural balance and body composition in inactive postmenopausal women—a randomised controlled trial. Bone. 2021;145: 115847. https://doi.org/10.1016/j.bone.2021.115847.
Pereira R, Krustrup P, Castagna C, Coelho E, Santos R, Martins S, et al. Effects of a 16-week recreational team handball intervention on aerobic performance and cardiometabolic fitness markers in postmenopausal women: a randomized controlled trial. Prog Cardiovasc Dis. 2020;63(6):800–6. https://doi.org/10.1016/j.pcad.2020.10.005.
Póvoas SC, Castagna C, Resende C, Coelho EF, Silva P, Santos R, et al. Effects of a short-term recreational team handball-based programme on physical fitness and cardiovascular and metabolic health of 33–55-year-old men: a pilot study. BioMed Res Int. 2018:4109796. https://doi.org/10.1155/2018/4109796.
Quist JS, Rosenkilde M, Petersen M, Gram A, Sjödin A, Stallknecht B. Effects of active commuting and leisure-time exercise on fat loss in women and men with overweight and obesity: a randomized controlled trial. Int J Obes. 2018;42(3):469–78. https://doi.org/10.1038/ijo.2017.253.
Rajarajan S, Anandhan P. Effect of walking cycling and swimming on physiological changes among overweight men. Int J Yogic Hum Mov Sports Sci. 2018;3(2):798–800.
Randers MB, Hagman M, Brix J, Christensen JF, Pedersen MT, Nielsen JJ, et al. Effects of 3 months of full-court and half-court street basketball training on health profile in untrained men. J Sport Health Sci. 2018;7(2):132–8. https://doi.org/10.1016/j.jshs.2017.09.004.
Randers MB, Nielsen JJ, Krustrup BR, Sundstrup E, Jakobsen MD, Nybo L, et al. Positive performance and health effects of a football training program over 12 weeks can be maintained over a 1-year period with reduced training frequency. Scand J Med Sci Sports. 2010;20(S1):80–9. https://doi.org/10.1111/j.1600-0838.2010.01091.x.
Sareban M, Fernandez La Puente de Battre MD, Reich B, Schmied C, Loidl M, Niederseer D, et al. Effects of active commuting to work for 12 months on cardiovascular risk factors and body composition. Scand J Med Sci Sports. 2020;30(S1):24–30. https://doi.org/10.1111/sms.13695.
Schmidt JF, Hansen PR, Andersen TR, Andersen L, Hornstrup T, Krustrup P, et al. Cardiovascular adaptations to 4 and 12 months of football or strength training in 65-to 75-year-old untrained men. Scand J Med Sci Sports. 2014;24(S1):86–97. https://doi.org/10.1111/sms.12217.
Seynnes O, Koesters A, Gimpl M, Reifberger A, Niederseer D, Niebauer J, et al. Effect of alpine skiing training on tendon mechanical properties in older men and women. Scand J Med Sci Sports. 2011;21:39–46. https://doi.org/10.1111/j.1600-0838.2011.01340.x.
Shimada H, Lee S, Akishita M, Kozaki K, Iijima K, Nagai K, et al. Effects of golf training on cognition in older adults: a randomised controlled trial. J Epidemiol Community Health. 2018;72(10):944–50. https://doi.org/10.1136/jech-2017-210052.
Skoradal MB, Helge EW, Jørgensen NR, Mortensen J, Weihe P, Krustrup P, et al. Osteogenic impact of football training in 55-to 70-year-old women and men with prediabetes. Scand J Med Sci Sports. 2018;28:52–60. https://doi.org/10.1111/sms.13252.
Sundstrup E, Jakobsen MD, Andersen LL, Andersen TR, Randers MB, Helge JW, et al. Positive effects of 1-year football and strength training on mechanical muscle function and functional capacity in elderly men. Eur J Appl Physiol. 2016;116(6):1127–38. https://doi.org/10.1007/s00421-016-3368-0.
Tiberiu ȘR, Iacob H. Tennis as a recreational physical activity for adults: the effect on physical fitness. Studia Universitatis Babes-Bolyai, Educatio Artis Gymnasticae. 2019;64(2):47–56. https://doi.org/10.24193/subbeag.64(2).14.
Tomar R, Allen JA. Physical and physiological benefits of small sided recreational handball in untrained males: relationship of body fat with aerobic capacity. Phys Educ Stud. 2021;25(6):339–44. https://doi.org/10.15561/20755279.2021.0601.
Tomar R, Antony VC. Effect of small-sided recreational soccer on metabolic controls, lipid profile and physical characteristics in untrained males. Med Sci. 2019;23(100):835–42.
Tomar R, Antony VC. Linkage of aerobic capacity and body fat percent: effects of recreational activity on aerobic capacity, body composition, blood pressure and resting heart rate in University students. Med Sci. 2019;23(98):557–64.
Trajković N, Sporiš G, Krističević T, Bogataj Š. Effects of small-sided recreational volleyball on health markers and physical fitness in middle-aged men. Int J Environ Res Public Health. 2020;17(9):3021. https://doi.org/10.3390/ijerph17093021.
van Ginkel S, Amami M, Dela F, Niederseer D, Narici M, Niebauer J, et al. Adjustments of muscle capillarity but not mitochondrial protein with skiing in the elderly. Scand J Med Sci Sports. 2015;25(4):e360–7. https://doi.org/10.1111/sms.12324.
Witte K, Emmermacher P, Pliske G. Improvement of balance and general physical fitness in older adults by karate: a randomized controlled trial. Complement Med Res. 2017;24(6):390–3. https://doi.org/10.1159/000479151.
Yoshimura Y, Imamura H. Effects of basic karate exercises on maximal oxygen uptake in sedentary collegiate women. J Health Sci. 2010;56(6):721–6. https://doi.org/10.1248/jhs.56.721.
Ahmadi-Abhari S, Sabia S, Shipley MJ, Kivimäki M, Singh-Manoux A, Tabak A, et al. Physical activity, sedentary behavior, and long-term changes in aortic stiffness: the Whitehall II study. J Am Heart Assoc. 2017;6(8): e005974. https://doi.org/10.1161/jaha.117.005974.
Albrecht M, Koolhaas CM, Schoufour JD, van Rooij FJ, Kavousi M, Ikram MA, et al. Physical activity types and atrial fibrillation risk in the middle-aged and elderly: the Rotterdam Study. Eur J Prev Cardiol. 2018;25(12):1316–23. https://doi.org/10.1177/2047487318780031.
Andersen K, Hållmarker U, James S, Sundström J. Long-distance skiing and incidence of hypertension: a cohort study of 206 889 participants in a long-distance cross-country skiing event. Circulation. 2020;141(9):743–50. https://doi.org/10.1161/CIRCULATIONAHA.119.042208.
Andersen ZJ, De Nazelle A, Mendez MA, Garcia-Aymerich J, Hertel O, Tjønneland A, et al. A study of the combined effects of physical activity and air pollution on mortality in elderly urban residents: the Danish Diet, Cancer, and Health Cohort. Environ Health Perspect. 2015;123(6):557–63. https://doi.org/10.1289/ehp.1408698.
Armstrong ME, Green J, Reeves GK, Beral V, Cairns BJ. Frequent physical activity may not reduce vascular disease risk as much as moderate activity: large prospective study of women in the United Kingdom. Circulation. 2015;131(8):721–9. https://doi.org/10.1161/CIRCULATIONAHA.114.010296.
Berentzen T, Petersen L, Schnohr P, Sørensen T. Physical activity in leisure-time is not associated with 10-year changes in waist circumference. Scand J Med Sci Sports. 2008;18(6):719–27. https://doi.org/10.1111/j.1600-0838.2007.00761.x.
Besson H, Ekelund U, Brage S, Luben R, Bingham S, Khaw K-T, et al. Relationship between subdomains of total physical activity and mortality. Med Sci Sports Exerc. 2008;40(11):1909–15. https://doi.org/10.1249/MSS.0b013e318180bcad.
Blond K, Jensen MK, Rasmussen MG, Overvad K, Tjønneland A, Østergaard L, et al. Prospective study of bicycling and risk of coronary heart disease in Danish men and women. Circulation. 2016;134(18):1409–11. https://doi.org/10.1161/CIRCULATIONAHA.116.024651.
Chakravarty EF, Hubert HB, Lingala VB, Fries JF. Reduced disability and mortality among aging runners: a 21-year longitudinal study. Arch Intern Med. 2008;168(15):1638–46. https://doi.org/10.1001/archinte.168.15.1638.
Chase NL, Sui X, Blair SN. Swimming and all-cause mortality risk compared with running, walking, and sedentary habits in men. Int J Aquat Res Educ. 2008;2(3):213–23. https://doi.org/10.25035/ijare.02.03.03.
Chomistek AK, Cook NR, Flint AJ, Rimm EB. Vigorous-intensity leisure-time physical activity and risk of major chronic disease in men. Med Sci Sports Exerc. 2012;44(10):1898–905. https://doi.org/10.1249/MSS.0b013e31825a68f3.
Dhana K, Koolhaas CM, Berghout MA, Peeters A, Ikram MA, Tiemeier H, et al. Physical activity types and life expectancy with and without cardiovascular disease: the Rotterdam Study. J Public Health (Oxf). 2017;39(4):e209–18. https://doi.org/10.1093/pubmed/fdw110.
Dons E, Rojas-Rueda D, Anaya-Boig E, Avila-Palencia I, Brand C, Cole-Hunter T, et al. Transport mode choice and body mass index: cross-sectional and longitudinal evidence from a European-wide study. Environ Int. 2018;119:109–16. https://doi.org/10.1016/j.envint.2018.06.023.
Fan M, Lv J, Yu C, Guo Y, Bian Z, Yang S, et al. Association between active commuting and incident cardiovascular diseases in Chinese: a prospective cohort study. J Am Heart Assoc. 2019;8(20): e012556. https://doi.org/10.1161/JAHA.119.012556.
Farahmand B, Broman G, De Faire U, Vågerö D, Ahlbom A. Golf: a game of life and death–reduced mortality in Swedish golf players. Scand J Med Sci Sports. 2009;19(3):419–24. https://doi.org/10.1111/j.1600-0838.2008.00814.x.
Fisher JE, Loft S, Ulrik CS, Raaschou-Nielsen O, Hertel O, Tjønneland A, et al. Physical activity, air pollution, and the risk of asthma and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2016;194(7):855–65. https://doi.org/10.1164/rccm.201510-2036OC.
Fuller D, Pabayo R. The relationship between utilitarian walking, utilitarian cycling, and body mass index in a population based cohort study of adults: comparing random intercepts and fixed effects models. Prev Med. 2014;69:261–6. https://doi.org/10.1016/j.ypmed.2014.10.022.
Grøntved A, Koivula RW, Johansson I, Wennberg P, Østergaard L, Hallmans G, et al. Bicycling to work and primordial prevention of cardiovascular risk: a cohort study among Swedish men and women. J Am Heart Assoc. 2016;5(11): e004413. https://doi.org/10.1161/JAHA.116.004413.
Hållmarker U, Lindbäck J, Michaelsson K, Ärnlöv J, Åsberg S, Wester P, et al. Survival and incidence of cardiovascular diseases in participants in a long-distance ski race (Vasaloppet, Sweden) compared with the background population. Eur Heart J Qual Care Clin Outcomes. 2018;4(2):91–7. https://doi.org/10.1093/ehjqcco/qcy005.
Hoevenaar-Blom MP, Wendel-Vos GW, Spijkerman AM, Kromhout D, Verschuren WM. Cycling and sports, but not walking, are associated with 10-year cardiovascular disease incidence: the MORGEN study. Eur J Prev Cardiol. 2011;18(1):41–7. https://doi.org/10.1097/HJR.0b013e32833bfc87.
Johnsen NF, Christensen J, Thomsen BL, Olsen A, Loft S, Overvad K, et al. Physical activity and risk of colon cancer in a cohort of Danish middle-aged men and women. Eur J Epidemiol. 2006;21(12):877–84. https://doi.org/10.1007/s10654-006-9076-z.
Johnsen NF, Ekblond A, Thomsen BL, Overvad K, Tjønneland A. Leisure time physical activity and mortality. Epidemiology. 2013;24(5):717–25. https://doi.org/10.1097/EDE.0b013e31829e3dda.
Koolhaas CM, Dhana K, Golubic R, Schoufour JD, Hofman A, van Rooij FJ, et al. Physical activity types and coronary heart disease risk in middle-aged and elderly persons: the Rotterdam study. Am J Epidemiol. 2016;183(8):729–38. https://doi.org/10.1093/aje/kwv244.
Koolhaas CM, Dhana K, Schoufour JD, Lahousse L, van Rooij FJ, Ikram MA, et al. Physical activity and cause-specific mortality: the Rotterdam study. Int J Epidemiol. 2018;47(5):1705–13. https://doi.org/10.1093/ije/dyy058.
Kubesch NJ, Therming Jørgensen J, Hoffmann B, Loft S, Nieuwenhuijsen MJ, Raaschou-Nielsen O, et al. Effects of leisure-time and transport-related physical activities on the risk of incident and recurrent myocardial infarction and interaction with traffic-related air pollution: a cohort study. J Am Heart Assoc. 2018;7(15): e009554. https://doi.org/10.1161/JAHA.118.009554.
Kunutsor SK, Lakka TA, Kurl S, Mäkikallio TH, Jae SY, Laukkanen JA. Leisure-time cross-country skiing and the risk of venous thromboembolism: a prospective cohort study. Eur J Prev Cardiol. 2021;28(10):1138–41. https://doi.org/10.1177/2047487320908978.
Kunutsor SK, Laukkanen JA, Kurl S, Mäkikallio TH, Khan H. Leisure-time cross-country skiing and risk of atrial fibrillation and stroke: a prospective cohort study. Eur J Prev Cardiol. 2020;27(19):2354–7. https://doi.org/10.1177/2047487319901040.
Kunutsor SK, Mäkikallio TH, Kauhanen J, Voutilainen A, Jae SY, Dey RS, et al. Leisure-time cross-country skiing is associated with lower incidence of type 2 diabetes: a prospective cohort study. Diabetes Metab Res Rev. 2020;36(1): e3216. https://doi.org/10.1002/dmrr.3216.
Kunutsor SK, Mäkikallio TH, Kauhanen J, Voutilainen A, Jae SY, Kurl S, et al. Leisure-time cross-country skiing is associated with lower incidence of hypertension: a prospective cohort study. J Hypertens. 2019;37(8):1624–32. https://doi.org/10.1097/hjh.0000000000002110.
Laukkanen JA, Lakka TA, Ogunjesa BA, Kurl S, Kunutsor SK. Cross-country skiing and the risk of acute myocardial infarction: a prospective cohort study. Eur J Prev Cardiol. 2020;27(10):1108–11. https://doi.org/10.1177/2047487319869696.
Laukkanen JA, Laukkanen T, Kunutsor SK. Cross-country skiing is associated with lower all-cause mortality: a population-based follow-up study. Scand J Med Sci Sports. 2018;28(3):1064–72. https://doi.org/10.1111/sms.12980.
Lee D-C, Pate RR, Lavie CJ, Sui X, Church TS, Blair SN. Leisure-time running reduces all-cause and cardiovascular mortality risk. J Am Coll Cardiol. 2014;64(5):472–81. https://doi.org/10.1016/j.jacc.2014.04.058.
Littman A, Kristal A, White E. Effects of physical activity intensity, frequency, and activity type on 10-y weight change in middle-aged men and women. Int J Obes. 2005;29(5):524–33. https://doi.org/10.1038/sj.ijo.0802886.
MacDonald CJ, Madika AL, Lajous M, Laouali N, Artaud F, Bonnet F, et al. Associations between physical activity and incident hypertension across strata of body mass index: a prospective investigation in a large cohort of French women. J Am Heart Assoc. 2020;9(23): e015121. https://doi.org/10.1161/JAHA.119.015121.
Matthews CE, Jurj AL, Shu X-O, Li H-L, Yang G, Li Q, et al. Influence of exercise, walking, cycling, and overall nonexercise physical activity on mortality in Chinese women. Am J Epidemiol. 2007;165(12):1343–50. https://doi.org/10.1093/aje/kwm088.
Mekary RA, Feskanich D, Malspeis S, Hu FB, Willett WC, Field AE. Physical activity patterns and prevention of weight gain in premenopausal women. Int J Obes. 2009;33(9):1039–47. https://doi.org/10.1038/ijo.2009.127.
Mielke GI, Bailey TG, Burton NW, Brown WJ. Participation in sports/recreational activities and incidence of hypertension, diabetes, and obesity in adults. Scand J Med Sci Sports. 2020;30(12):2390–8. https://doi.org/10.1111/SMS.13795.
Østergaard L, Jensen MK, Overvad K, Tjønneland A, Grøntved A. Associations between changes in cycling and all-cause mortality risk. Am J Prev Med. 2018;55(5):615–23. https://doi.org/10.1016/j.amepre.2018.06.009.
Patterson R, Panter J, Vamos EP, Cummins S, Millett C, Laverty AA. Associations between commute mode and cardiovascular disease, cancer, and all-cause mortality, and cancer incidence, using linked Census data over 25 years in England and Wales: a cohort study. Lancet Planet Health. 2020;4(5):e186–94. https://doi.org/10.1016/S2542-5196(20)30079-6.
Porter AK, Cuthbertson CC, Evenson KR. Participation in specific leisure-time activities and mortality risk among US adults. Ann Epidemiol. 2020;50:27–34. https://doi.org/10.1016/j.annepidem.2020.06.006.
Porter AK, Schilsky S, Evenson KR, Florido R, Palta P, Holliday KM, et al. The association of sport and exercise activities with cardiovascular disease risk: the Atherosclerosis Risk in Communities (ARIC) study. J Phys Act Health. 2019;16(9):698–705. https://doi.org/10.1123/jpah.2018-0671.
Pronk A, Ji B, Shu X, Chow W, Xue S, Yang G, et al. Physical activity and breast cancer risk in Chinese women. Br J Cancer. 2011;105(9):1443–50. https://doi.org/10.1038/bjc.2011.370.
Rasmussen MG, Grøntved A, Blond K, Overvad K, Tjønneland A, Jensen MK, et al. Associations between recreational and commuter cycling, changes in cycling, and type 2 diabetes risk: a cohort study of Danish men and women. PLoS Med. 2016;13(7): e1002076. https://doi.org/10.1371/journal.pmed.1002076.
Rasmussen MG, Overvad K, Tjønneland A, Jensen MK, Østergaard L, Grøntved A. Changes in cycling and incidence of overweight and obesity among Danish men and women. Med Sci Sports Exerc. 2018;50(7):1413–21. https://doi.org/10.1249/MSS.0000000000001577.
Sahlqvist S, Goodman A, Simmons RK, Khaw K-T, Cavill N, Foster C, et al. The association of cycling with all-cause, cardiovascular and cancer mortality: findings from the population-based EPIC-Norfolk cohort. BMJ Open. 2013;3(11): e003797. https://doi.org/10.1136/bmjopen.2013.003797.
Schnohr P, Marott JL, Lange P, Jensen GB. Longevity in male and female joggers: the Copenhagen City Heart Study. Am J Epidemiol. 2013;177(7):683–9. https://doi.org/10.1093/aje/kws301.
Schnohr P, O’Keefe JH, Holtermann A, Lavie CJ, Lange P, Jensen GB, et al. Various leisure-time physical activities associated with widely divergent life expectancies: the Copenhagen City Heart Study. Mayo Clin Proc. 2018;93(12):1775–85. https://doi.org/10.1016/j.mayocp.2018.06.025.
Schnohr P, O’Keefe JH, Marott JL, Lange P, Jensen GB. Dose of jogging and long-term mortality: the Copenhagen City Heart Study. J Am Coll Cardiol. 2015;65(5):411–9. https://doi.org/10.1016/j.jacc.2014.11.023.
Sheehan CM, Li L. Associations of exercise types with all-cause mortality among US adults. Med Sci Sports Exerc. 2020;52(12):2554–62. https://doi.org/10.1249/MSS.0000000000002406.
Svedberg N, Sundström J, James S, Hållmarker U, Hambraeus K, Andersen K. Long-term incidence of atrial fibrillation and stroke among cross-country skiers: cohort study of endurance-trained male and female athletes. Circulation. 2019;140(11):910–20. https://doi.org/10.1161/CIRCULATIONAHA.118.039461.
Tovar-García ED. The associations of different types of sports and exercise with health status and diseases: evidence from Russian longitudinal data. Sports Sci Health. 2021;17(3):687–97. https://doi.org/10.1007/s11332-021-00734-x.
Turrell G, Hewitt BA, Rachele JN, Giles-Corti B, Busija L, Brown WJ. Do active modes of transport cause lower body mass index? Findings from the HABITAT longitudinal study. J Epidemiol Community Health. 2018;72(4):294–301. https://doi.org/10.1136/jech-2017-209957.
Wang N, Zhang X, Xiang Y-B, Li H, Yang G, Gao J, et al. Associations of Tai Chi, walking, and jogging with mortality in Chinese men. Am J Epidemiol. 2013;178(5):791–6. https://doi.org/10.1093/aje/kwt050.
Wang Y, Lee D-C, Brellenthin AG, Eijsvogels TM, Sui X, Church TS, et al. Leisure-time running reduces the risk of incident type 2 diabetes. Am J Med. 2019;132(10):1225–32. https://doi.org/10.1016/j.amjmed.2019.04.035.
Watts EL, Matthews CE, Freeman JR, Gorzelitz JS, Hong HG, Liao LM, et al. Association of leisure time physical activity types and risks of all-cause, cardiovascular, and cancer mortality among older adults. JAMA Netw Open. 2022;5(8): e2228510. https://doi.org/10.1001/jamanetworkopen.2022.28510.
Nordengen S, Andersen LB, Solbraa AK, Riiser A. Cycling is associated with a lower incidence of cardiovascular diseases and death: part 1—systematic review of cohort studies with meta-analysis. Br J Sports Med. 2019;53(14):870–8. https://doi.org/10.1136/bjsports-2018-099099.
Zhao Y, Hu F, Feng Y, Yang X, Li Y, Guo C, et al. Association of cycling with risk of all-cause and cardiovascular disease mortality: a systematic review and dose-response meta-analysis of prospective cohort studies. Sports Med. 2021;51(7):1439–48. https://doi.org/10.1007/s40279-021-01452-7.
Nordengen S, Andersen LB, Solbraa AK, Riiser A. Cycling and cardiovascular disease risk factors including body composition, blood lipids and cardiorespiratory fitness analysed as continuous variables: part 2-systematic review with meta-analysis. Br J Sports Med. 2019;53(14):879–85. https://doi.org/10.1136/bjsports-2018-099778.
Milanović Z, Pantelić S, Čović N, Sporiš G, Mohr M, Krustrup P. Broad-spectrum physical fitness benefits of recreational football: a systematic review and meta-analysis. Br J Sports Med. 2019;53(15):926–39. https://doi.org/10.1136/bjsports-2017-097885.
Zouhal H, Hammami A, Tijani JM, Jayavel A, de Sousa M, Krustrup P, et al. Effects of small-sided soccer games on physical fitness, physiological responses, and health indices in untrained individuals and clinical populations: a systematic review. Sports Med. 2020;50(5):987–1007. https://doi.org/10.1007/s40279-019-01256-w.
Lahart IM, Metsios GS. Chronic physiological effects of swim training interventions in non-elite swimmers: a systematic review and meta-analysis. Sports Med. 2018;48(2):337–59. https://doi.org/10.1007/s40279-017-0805-0.
Chia L, De Oliveira SD, Whalan M, McKay MJ, Sullivan J, Fuller CW, et al. Non-contact anterior cruciate ligament injury epidemiology in team-ball sports: a systematic review with meta-analysis by sex, age, sport, participation level, and exposure type. Sports Med. 2022;52(10):2447–67. https://doi.org/10.1007/s40279-022-01697-w.
Leppänen M, Aaltonen S, Parkkari J, Heinonen A, Kujala UM. Interventions to prevent sports related injuries: a systematic review and meta-analysis of randomised controlled trials. Sports Med. 2014;44(4):473–86. https://doi.org/10.1007/s40279-013-0136-8.
Khan KM, Thompson AM, Blair SN, Sallis JF, Powell KE, Bull FC, et al. Sport and exercise as contributors to the health of nations. Lancet. 2012;380(9836):59–64. https://doi.org/10.1016/s0140-6736(12)60865-4.
Mountjoy M, Junge A, Budgett R, Doerr D, Leglise M, Miller S, et al. Health promotion by International Olympic Sport Federations: priorities and barriers. Br J Sports Med. 2019;53(17):1117–25. https://doi.org/10.1136/bjsports-2018-100202.
Kelly P, Kahlmeier S, Götschi T, Orsini N, Richards J, Roberts N, et al. Systematic review and meta-analysis of reduction in all-cause mortality from walking and cycling and shape of dose response relationship. Int J Behav Nutr Phys Act. 2014;11:132. https://doi.org/10.1186/s12966-014-0132-x.
Acknowledgements
The European Commission support for the production of this publication does not constitute endorsement of the contents which reflects the views only of the authors, and the Commission cannot be held responsible for any use which may be made of the information contained therein.
Funding
This manuscript was prepared as part of the “Creating Mechanisms for Continuous Implementation of the Sports Club for Health Guidelines in the European Union” project, funded by the Erasmus + Collaborative Partnerships grant (reference number: 613434-EPP-1-2019-1-HR-SPO-SCP).
Author information
Authors and Affiliations
Contributions
P.O. contributed to study conceptualisation, study selection, data extraction, quality assessment, interpretation of results and write-up of the introduction, results and discussion sections; A.R.M. contributed to study selection, data extraction, quality assessment, interpretation of results and write-up of the introduction and results section; S.T. contributed to study selection, data extraction, quality assessment and write-up of the results section; D.J. contributed to study conceptualisation and study selection; S-T.C. contributed to study selection; N.S. contributed to study selection and certainty of evidence assessment; S.E. contributed to study selection; T.M. contributed to study selection; T.V. contributed to study selection; A.H. contributed to quality assessment; J.G. contributed to the write-up of the methods section; S.K. contributed to quality assessment; P.Ko. contributed to study selection; P.Ke. contributed to literature search and conceptualisation of data analysis; C.F. contributed to conceptualisation of data analysis; H.P. contributed to certainty of evidence assessment; Z.P. conducted data analyses, contributed to study conceptualisation, literature search, data extraction, interpretation of results and write-up of the introduction, methods, results and discussion sections, and led the correspondence with editors and reviewers. All authors contributed to revising the manuscript and read and approved its final version.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Competing interests
The authors have no competing interests relevant to this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Search syntax.
Additional file 2:
Summary of intervention trials on health effects of participation in specific sports.
Additional file 3:
Summary of longitudinal studies on the association between participation in specific sports and health.
Additional file 4:
Methodological quality appraisal of intervention studies using the Effective Public Health Practice Project Quality Assessment Tool.
Additional file 5:
Methodological quality appraisal of longitudinal studies using the Newcastle-Ottawa Quality Assessment Scale.
Additional file 6:
Forest plots from main meta-analyses.
Additional file 7:
The effects of cycling on health outcomes: results of four sensitivity meta-analyses in which missing correlations were replaced with 0.50.
Additional file 8:
The effects of football on health outcomes: results of 20 sensitivity meta-analyses in which missing correlations were replaced with 0.50
Additional file 9:
The effects of handball on health outcomes: results of 12 sensitivity meta-analyses in which missing correlations were replaced with 0.50.
Additional file 10:
The effects of running on health outcomes: results of 13 sensitivity meta-analyses in which missing correlations were replaced with 0.50.
Additional file 11:
The effects of swimming on health outcomes: results of five sensitivity meta-analyses in which missing correlations were replaced with 0.50.
Additional file 12:
The longitudinal associations between cycling and the risk of mortality and morbidity: results of 5 sensitivity meta-analyses of hazard ratios for any participation or the highest reported dose of activity.
Additional file 13:
Funnel plot for the meta-analysis on the effects of football on body mass.
Additional file 14:
Funnel plot for the meta-analysis on the effects of football on body fat percentage.
Additional file 15:
Funnel plot for the meta-analysis on the effects of football on systolic blood pressure.
Additional file 16:
Funnel plot for the meta-analysis on the effects of football on diastolic blood pressure.
Additional file 17:
Certainty of evidence on the associations of cycling, running, and swimming participation with the risk of all-cause mortality.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Oja, P., Memon, A.R., Titze, S. et al. Health Benefits of Different Sports: a Systematic Review and Meta-Analysis of Longitudinal and Intervention Studies Including 2.6 Million Adult Participants. Sports Med - Open 10, 46 (2024). https://doi.org/10.1186/s40798-024-00692-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-024-00692-x