
Abstract
Background
Understanding the physical qualities of male, adolescent rugby league players across age groups is essential for practitioners to manage long-term player development. However, there are many testing options available to assess these qualities, and differences in tests and testing protocols can profoundly influence the data obtained.
Objectives
The aims of this systematic review were to: (1) identify the most frequently used tests to assess key physical qualities in male, adolescent rugby league players (12–19 years of age); (2) examine the testing protocols adopted in studies using these tests; and (3) synthesise the available data from studies using the most frequently used tests according to age group.
Methods
A systematic search of five databases was conducted. For inclusion, studies were required to: (1) be original research that contained original data published in a peer-reviewed journal; (2) report data specifically for male, adolescent rugby league players; (3) report the age for the recruited participants to be between 12 and 19 years; (4) report data for any anthropometric quality and one other physical quality and identify the test(s) used to assess these qualities; and (5) be published in English with full-text availability. Weighted means and standard deviations were calculated for each physical quality for each age group arranged in 1-year intervals (i.e., 12, 13, 14, 15, 16, 17 and 18 years) across studies.
Results
37 studies were included in this systematic review. The most frequently used tests to assess anthropometric qualities were body mass, standing height, and sum of four skinfold sites. The most frequently used tests to assess other physical qualities were the 10-m sprint (linear speed), 505 Agility Test (change-of-direction speed), Multistage Fitness Test (aerobic capacity), bench press and back squat one-repetition maximum tests (muscular strength), and medicine ball throw (muscular power). Weighted means calculated across studies generally demonstrated improvements in player qualities across subsequent age groups, except for skinfold thickness and aerobic capacity. However, weighted means could not be calculated for the countermovement jump.
Conclusion
Our review identifies the most frequently used tests, but highlights variability in the testing protocols adopted. If these tests are used in future practice, we provide recommended protocols in accordance with industry standards for most tests. Finally, we provide age-specific references for frequently used tests that were implemented with consistent protocols.
Clinical Trial Registration This study was conducted in accordance with the Preferred Reporting Items of Systematic Review and Meta-analysis guidelines and was registered with PROSPERO (ID: CRD42021267795).
Similar content being viewed by others


Background
Rugby league is an intermittent, field-based team sport, requiring players to repeatedly complete high-intensity bouts, interspersed with activity performed at lower intensities [1]. Rugby league is played from amateur to professional levels worldwide [2] with the largest professional leagues hosted in Australia [3] and England [4]. In many countries, rugby league is also played competitively among male, adolescent players aged between 12 and 19 years [5]. Indeed, professional rugby league clubs and national governing bodies invest in youth academies and talent identification programmes [6] to identify and develop adolescent players with favourable physical qualities that may increase their likelihood of success in rugby league. In this regard, a review by Till and colleagues [4] showed that male, adolescent rugby league players possessing superior physical qualities (height, body mass, and sum of skinfolds, speed, change-of-direction [COD] speed, muscular strength, and muscular power) were more likely to progress from amateur to professional playing standards (whereby players are contracted to play). Given the importance of physical qualities in determining career outcomes of male, adolescent rugby league players, a comprehensive synthesis of data representing key qualities across different ages and playing levels (i.e., amateur, academy, and elite) is essential. These data may be used as benchmark standards, allowing rugby league coaching staff to best prepare their adolescent players for successful transition to higher playing levels. Unfortunately, despite the welcomed increase in participation and professionalisation among female rugby league players across all age groups, limited research has reported the physical qualities of female, adolescent rugby league players [7]. Therefore, this review will focus on male, adolescent rugby league players, but systematic synthesis of the literature on this topic is encouraged in female, adolescent rugby league players as the evidence base grows.
The demands of male, adolescent rugby league match-play necessitate players have well-developed physical qualities including high body mass and low sum of skinfolds [8], as well as high linear speed [9], COD speed [10], aerobic capacity [11], muscular strength [12], and muscular power [13], relative to their age. Accordingly, the physical qualities of male, adolescent rugby league players reported in the literature have been compiled in previous reviews [1, 4, 14]. For example, Till and colleagues [4] conducted the most comprehensive review to date, synthesising the reported values for selected physical qualities (i.e., height, body mass, and sum of skinfolds from 12 studies, muscular strength from 4 studies, and muscular power, linear speed, COD speed, and aerobic capacity from 11 studies) in elite male, adolescent rugby league players (13–20 years of age). While this previous review [4] offers useful insight, there is a need for an updated review for several reasons. Firstly, the previous review [4] only included studies examining “elite”, adolescent, male rugby league players, defined as those “who were selected for a national governing body talent identification and development programme or were members of a professional rugby league club academy programme”. Consequently, the physical qualities of male, adolescent rugby league players at non-elite playing levels, including those playing at amateur and school levels, remains to be synthesised. Secondly, the data representing physical qualities reported in the previous review [4] were not differentiated according to the test protocols implemented across studies [15], with detailed accounts of the testing protocols used to assess each quality being omitted. In this regard, identifying the most frequently used tests and testing protocols in the literature may assist in establishing future testing recommendations for male, adolescent rugby league players.
Recognising the value of identifying frequently used tests in the literature, Chiwaridzo and colleagues [16] conducted a systematic review on this topic in 2017, but several of the inclusion criteria used limit the specificity of the findings to male, adolescent rugby league players. For example, the previous review [16] encompassed both rugby league (71% of studies) and rugby union (26% of studies) players, with some studies combining players from both sports (3% of studies). Secondly, male, adult players were included in the previous review [16], who possess varied physical qualities compared to male, adolescent rugby league players [17] and may have access to varied facilities and equipment; thus older rugby league players may require, or have used different, testing protocols compared to younger players. Thirdly, a thorough evaluation of the testing protocols adopted when implementing each test was not provided in the previous review [16], which is important given testing protocol variations can impact the data obtained [15]. Therefore, identifying the most frequently used tests and testing protocols to measure physical qualities in male, adolescent rugby league players will enable future synthesis of similar data for comparison according to age group and playing level. Furthermore, identifying protocol discrepancies among the literature for specific tests may assist in recommending how they should be implemented in the future.
Therefore, the aims of this systematic review are to: (1) identify the most frequently used tests to assess key physical qualities in male, adolescent rugby league players (12–19 years of age); (2) examine the testing protocols adopted in studies using these tests; and (3) synthesise the available data from studies using the most frequently used tests according to age group.
Methods
Design and Search Strategy
This systematic review was conducted in accordance with the Preferred Reporting Items of Systematic Reviews and Meta-analyses (PRISMA) guidelines and was registered with PROSPERO (ID: CRD42021267795). Five databases were searched (PubMed, MEDLINE, Web of Science, Scopus, and SPORTDiscus) on 1 July 2022. A search strategy containing 33 keywords was employed with keywords divided into three levels, each linked by the Boolean operator ‘AND’. Keywords within each level were linked by the Boolean operator ‘OR’ (Additional file 1: Table A). All search results were exported from each database and imported into reference management software (EndNote, version X9.3.3; Clarivate Analytics, Microsoft Corp, Redmond, MA).
Study Selection and Inclusion Criteria
Duplicate studies retrieved across multiple databases were removed within the reference management software. To be included in this systematic review, studies were required to: (1) be original research that contained original data (i.e., not previously reported in another study) published in a peer-reviewed journal; (2) report data specifically for male, adolescent rugby league players; (3) report the mean age for the recruited participants to be between 12 and 19 years; (4) report data for any anthropometric quality and one other physical quality and identify the test(s) used to assess these qualities; and (5) be published in English with full-text availability.
Studies were excluded if they: (1) reported previously published data, or were a narrative review, systematic review, or meta-analysis; (2) reported the age of the player sample outside of the range of 12–19 years; (3) included only female players or did not differentiate data according to sex if examining female and male players together; (4) did not report data for at least one anthropometric quality and at least one other physical quality concurrently, or provide these data on request via email communication if data were not clearly reported in the published version; (5) did not identify the test(s) used to assess the included physical qualities; or (6) adopted a longitudinal observational or experimental study design and did not report baseline data.
Observational and experimental studies were included in this systematic review, but baseline data (i.e., prior to the longitudinal monitoring period or implementation of any intervention) for the reported physical qualities were extracted to avoid any confounding influence of time or intervention. Two reviewers (MC and CP) independently screened titles and abstracts of all studies retrieved from the initial search, with all conflicts discussed. If conflicts could not be resolved through discussion, a third reviewer (AS) was consulted to provide a consensus decision (n = 1). Two reviewers (MC and CP) subsequently examined all full-text versions for final eligibility with all conflicts resolved via discussion.
Assessment of Reporting Quality
An assessment of study quality was completed on each included study using a modified Downs and Black checklist [18]. The modified Downs and Black checklist has been implemented in systematic reviews quantifying demands and match metrics of rugby league players [19, 20], and is a valid risk-of-bias tool for observational studies [21]. In the modified Downs and Black checklist, a score of 11 is the highest quality score achievable (Additional file 2: Table B); however, one question (question 9) was not applicable to this review and therefore a score of 10 was the highest quality score achievable. Two reviewers (MC and CP) independently conducted the risk of bias and quality assessment, with three discrepancies arising between reviewers and resolved via discussion.
Data Extraction
Data from all included studies were extracted into a customised spreadsheet (Microsoft Excel, version 16.54; Microsoft Corp, Redmond, MA). Data were extracted from each study by the lead author (MC) and verified by another author for accuracy (CP). Extracted data included author names, year of publication, sample size, mean age of player sample, any sub-group reported (i.e., playing level categorised into amateur, academy, and elite levels, and positional groups as stipulated in the study), tests conducted to assess any physical quality, the data (i.e., mean ± standard deviation) reported for each test, and protocols specific to each test. Where confidence intervals were reported (n = 4) [1, 22,23,24], standard deviations were calculated using these data according to the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0) for consistency in reporting.
Categorisation and Presentation of Findings
Data extracted from each included study were first categorised as physical qualities including anthropometric (height, body mass, and sum of skinfolds), linear speed, COD speed, aerobic capacity, muscular strength, and muscular power. Further, the total number of studies using each test and the total cumulative sample size of players assessed using each test were reported.
For data to be reported in this review and to consolidate our reporting of the most frequently used tests in the literature, permitting reasonable comparison of physical qualities, a test must have: (1) been used in a minimum of three studies; and (2) assessed at least 5% of the total cumulative sample reported in the literature for that quality. For example, if 6000 players were assessed for linear speed across all included studies, a test must have been used in at least three studies, and cumulatively assessed at least 300 players to be reported. While all tests identified from all included studies are reported in Table 1, only data from frequently used tests are reported in this review.
Data included in this review were then organised by physical quality. All physical qualities were reported in separate tables. Within these tables, studies are ordered based on the mean chronological age of the player sample reported and assigned to the appropriate age group spanning 12–19 years in 1-year intervals. In studies reporting data for multiple age categories (i.e., 14, 15, and 16 years), data for those respective groups were extracted, and reported independently in our review. Data and sample size are reported according to the positional subgroups reported in each study. Furthermore, we categorised the playing levels of study participants as: (1) amateur (a voluntary non-contractual player, competing for a school or club); (2) academy (contracted to participate as part of an institution/club); and (3) elite (contracted to a professional club and/or selected to play at a regional or higher representative level). These definitions were developed in accordance with a recent framework [25] given the literature included in this review reported playing levels using several different terms such as “sub-elite” and “academy”.
For the most frequently used tests, the procedural description was checked against test-specific criteria the authors deemed essential for test replication in practice that may also impact the data obtained. Specifically, criterion protocols crosschecked in every study using the 10-m sprint were: (1) starting distance behind the line; (2) number of trials conducted and whether the mean time (s) or best time (s) across trials was reported; and (3) equipment used to assess sprint time. Criterion protocols crosschecked in every study using the 505 Agility Test were: (1) number of trials and whether the mean time (s) or best time (s) across trials was reported; and (2) equipment used to measure COD performance time. There were no specific criterion protocols crosschecked for studies using the Multistage Fitness Test (MSFT), as studies consistently reported protocols stipulated by Ramsbottom [26]. Criterion protocols crosschecked in every study using the one-repetition maximum (1RM) (for squat and bench press) were: (1) number of attempts; (2) rest duration between each attempt; and (3) equipment used to measure 1RM. Criterion protocols crosschecked in every study using the countermovement jump (CMJ) were: (1) whether an arm swing was permitted; (2) number of trials and whether the mean jump height (cm) or best jump height (cm) across trials was reported; and (3) equipment used to measure jump height. Criterion protocols crosschecked in every study using the medicine ball throw (MBT) were: (1) the position in which the player performed the throw; (2) mass of the medicine ball; and (3) number of trials and whether the mean throw distance (m) or best throw distance (m) across trials was reported.
Finally, to understand the progression of player qualities across age groups, data for each included test were combined to provide a mean value for each frequently used test in each age group. Importantly, only studies that used the most frequently adopted protocols for the given test were included in this calculation; for example, where a study used a 10-m sprint test, the reported data would be used to calculate the weighted mean and standard deviation if implemented using electronic light gates to record the best time across three trials, with players starting 0.5 m from the first light gate. To provide mean values, all data for a given test within an age group were weighted according to sample size (e.g., [mean height (A) × sample (A)] + [mean height (B) × sample (B)]/[total sample (A + B)]). This method was also applied to standard deviation values. Given the low number of studies examining amateur and elite players, and inconsistencies in reporting playing positions across studies, normative mean values were not able to be calculated according to playing level or positional groups. Furthermore, due to a lack of methodological consistency in protocols of the CMJ across the studies included in this review, the calculation of a weighted mean for the CMJ test was precluded.
Results
Identification and Selection of Articles
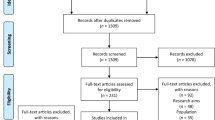
Searches across databases identified a total of 267 relevant studies, and a further seven studies were identified via manual searches of reference lists and deemed eligible for inclusion (n = 274). Ninety-five duplicate studies were removed, and the title and abstract of the remaining 179 studies were screened by two independent reviewers (MC and CP). A total of 131 studies did not meet the inclusion criteria and the remaining 48 studies were eligible for full-text review. The full-text version of one study could not be retrieved, and 10 studies [27,28,29,30,31,32,33,34,35,36] were excluded in the full-text screening process. As such, 37 studies were included in this systematic review (Fig. 1).

Selection process of eligible studies for synthesis in this review. Notes: aReports excluded according to exclusion criteria: (1) reported previously published data or were a narrative review, systematic review, or meta-analysis; (2) reported mean age of the sample outside the specified age range of 12–19 years; (3) included only female players or did not differentiate data according to sex if examining female and male players together; (4) did not report data for at least one physical characteristic and at least one physiological characteristic concurrently, or did not provide these data on request via email communication if data were not clearly reported in the published study; (5) did not identify the test(s) used to assess the included physical; (6) adopted a longitudinal observational or experimental design and did not report baseline data
Assessment of Reporting Quality
Study quality scores ranged from 6 to 10 for the 10 items assessed in the modified Downs and Black checklist. No studies were excluded based on risk of bias and methodological quality, with the mean score across included studies being 7.7 ± 1.2 out of 10 (Additional file 3: Table C).
Frequency of Test Use
Table 1 shows the frequency of use for each individual test to assess physical qualities in male, adolescent rugby league players. A total of 37 studies examined the physical qualities of male, adolescent rugby league players, employing 35 different tests (Table 1).
A total of 37 studies examined anthropometric qualities using 10 different tests to assess standing height, body mass and skinfold thickness, but five tests were not reported in our dataset due to limited use and inadequate sample size; therefore, five frequently used tests examining anthropometric qualities are reported in this review from 37 studies. Furthermore, 33 studies examined linear speed using nine different tests, but four tests were not reported in our dataset due to limited use and inadequate sample size; therefore, five frequently used tests examining linear speed are reported in this review from 33 studies. Nineteen studies examined COD speed using five different tests, but three tests were not reported in our dataset due to limited use; therefore, two frequently used tests examining COD speed are reported in this review from 16 studies. Twenty-eight studies assessed aerobic capacity using three different tests, but one test was not reported in our dataset due to limited use and inadequate sample size; therefore, two frequently used tests examining aerobic capacity are reported in this review from 28 studies. Nine studies assessed muscular strength using three different tests, and therefore, all three tests examining muscular strength are reported in this review from all nine studies. Thirty-one studies assessed muscular power using five different tests, but three tests were not reported in our dataset due to limited use and inadequate sample size; therefore, two frequently used tests examining muscular power are reported in this review from 31 studies.
Anthropometric Qualities
All 37 studies examined anthropometric qualities (Table 2), with measures of standing height assessed via stadiometer, body mass assessed via electronic scales, and skinfold thickness assessed via Σ4 skinfold thickness using Harpenden callipers the most frequently assessed qualities and tests. Most studies examined 17-year-old players (21 studies, 57%) with the least frequently studied age group being 12-year-old players (one study, 3%). A total sample of 6083 players were included across all studies examining anthropometric qualities. Across all ages, studies most frequently assessed academy players (35 studies, 95%), followed by elite (six studies, 16%), and amateur players (four studies, 11%). Seven studies (19%) reported data for players competing at multiple playing levels. Most studies (31 studies, 84%) did not report data according to playing position and grouped data for all players collectively.
When examining the protocols used to assess anthropometric qualities, 33 studies (89%) reported standing height, of which 25 studies (76%) reported using a stadiometer (cm) and six studies (16%) did not report the equipment used. Thirty-seven studies (100%) reported body mass (kg), of which most studies (31 studies, 86%) reported using electronic scales, and six studies (16%) did not report the equipment used. Fourteen studies (39%) reported measuring body composition via skinfold thickness using Σ4 sites, of which all studies (14 studies, 100%) reported using Harpenden callipers.
Linear Speed
Table 3 shows data for the included tests examining linear speed, measuring performance time (s) most frequently using the 10-m sprint test. A total of 37 studies examined linear speed in male, adolescent rugby league players aged between 12 and 19 years. Most studies examined 17-year-old players (18 studies, 55%) with the least frequently studied age group being 12-year-old players (one study, 3%). A total sample of 5789 players were included across all studies examining linear speed. Across all ages, studies most frequently assessed academy players (31 studies, 94%), followed by elite (11 studies, 33%), and amateur players (three studies, 9%). Nine studies (27%) reported data for players competing at multiple playing levels. Most studies (24 studies, 73%) did not report data according to playing position and grouped data for all players collectively.
When examining the protocols used to assess linear speed, 18 studies (55%) reported the starting distance of players behind the starting gate (0.3 m, n = 6, 33%; 0.5 m, n = 11, 61%; 0 m, n = 1, 6%) and 15 studies (45%) did not report where players started. Thirty-two studies (97%) reported linear sprint time in seconds (s) using electronic light gates, while one study (3%) reported sprint time in seconds (s) using a radar gun. Seventeen studies (52%) reported the best sprint time across three trials and 13 studies (39%) reported the best sprint time across two trials. One study (3%) reported that two trials were used in their analysis but did not indicate whether the best or average time was reported, and two studies (6%) did not report the number of trials completed, or how performance time was determined.
Change of Direction Speed
Table 4 shows data for the included tests examining COD speed, measuring performance time (s) most frequently using the 505 Agility Test. A total of 16 studies examined COD speed in male, adolescent rugby league players aged between 13 and 18 years. Most studies examined 15-year-old players (10 studies, 63%), with the least frequently studied age group being 18-year-old players (one study, 6%). No included studies examined 12-year-old players. A total sample of 3765 players were included across all studies examining COD speed. Across all ages, studies most frequently assessed academy players (11 studies, 69%), followed by elite (five studies, 31%), and amateur players (one study, 6%). Four studies (25%) reported data for players competing at multiple playing levels. Most studies (13 studies, 81%) did not report data according to playing position and grouped data for all players collectively.
When examining the protocols used to assess COD speed, eight studies (50%) reported the best performance time across three trials, and two studies (13%) used three trials but did not report how performance time was determined (i.e., mean or best). Four studies (25%) reported the best performance time across two trials, and two studies (13%) did not report the number of trials completed or how performance was determined. Fifteen studies (94%) reported COD performance time in seconds (s) using electronic light gates, and one study (6%) did not report the equipment used to measure performance time.
Aerobic Capacity
Table 5 shows data for the included tests examining proxy measures of aerobic capacity, predicting maximum rate of oxygen consumption (\(\dot{\mathrm{V}}\)O2max in mL kg−1 min−1) most frequently using the MSFT. A total of 27 studies examined estimated aerobic capacity in male, adolescent rugby league players aged between 12 and 19 years; one study [24] (4%) did not report predicted \(\dot{\mathrm{V}}\)O2max, and instead reported MSFT level obtained for 14-year-old players (academy = 8.0 ± 1.4; elite = 10.6 ± 1.5), 15-year-old players (academy = 9.4 ± 1.6; elite = 11.3 ± 1.5) and 16-year-old players (academy = 9.5 ± 1.8; elite = 12.3 ± 1.1). Most studies examined 17-year-old players (16 studies, 59%) with the least frequently studied age group being 12-year-old players (one study, 4%). A total sample of 5636 players were included across all studies examining aerobic capacity. Across all ages, studies most frequently assessed academy players (26 studies, 96%), followed by elite (eight studies, 30%), and amateur players (three studies, 11%). Seven studies (26%) reported data for players competing at multiple playing levels. Most studies (20 studies, 74%) did not report data according to playing position and grouped data for all players collectively.
Muscular Strength
Table 6 shows data for the included tests examining upper-body and lower-body muscular strength, most frequently measuring 1RM (kg) using bench press and back squat, respectively. A total of nine studies examined muscular strength in male, adolescent rugby league players aged between 14 and 19 years. Most studies examined 17-year-old players (seven studies, 78%), with the least frequently studied age group being 14-year-old players (one study, 11%). No included studies examined 12- or 13-year-old players. A total sample of 743 players were included across all studies examining muscular strength. Across all ages, studies most frequently assessed academy players (seven studies, 78%), followed by elite players (two studies, 22%), with one study (11%) examining amateur players. Most studies (seven studies, 78%) did not report data according to playing position and grouped data for all players collectively.
When examining the protocols used to assess 1RM, all studies (nine studies, 100%) clearly reported the range-of-motion required for each exercise. Five studies (56%) reported that three attempts were permitted to achieve 1RM, three studies (33%) did not report the number of attempts permitted, and one study (11%) reported three to five attempts were permitted. Six studies (67%) reported a 3-min rest between each attempt, two studies (22%) did not report the rest duration permitted between each attempt, and one study (11%) reported 2–4 min of rest was permitted between each attempt. Most studies (seven studies, 78%) reported use of a barbell to assess 1RM, with one study (11%) not specifying the equipment used, and one study (11%) reported use of a Smith machine to assess 1RM.
Muscular Power
Table 7 shows data for the included tests examining lower-body and upper-body muscular power, most frequently measuring jump height (cm) using a CMJ test and distance thrown (m) using a MBT test, respectively. A total of 31 studies examined muscular power in male, adolescent rugby league players aged between 12 and 19 years. Most studies examined 15-year-old players (18 studies, 58%), with the least frequently studied age group being 12-year-old players (one study, 3%). A total sample of 5797 players were included across all studies examining muscular power. Across all ages, studies most frequently assessed academy players (29 studies, 94%), followed by elite (10 studies, 32%), and amateur players (three studies, 10%). Eight studies (26%) reported data for players competing at multiple playing levels. Most studies (23 studies, 74%) did not report data according to playing position and grouped data for all players collectively.
When examining the protocols used to assess muscular power, most studies (19 studies, 61%) examining CMJ height (cm) reported no arm swing was permitted, three studies (10%) reported arm swing was permitted, and nine studies (29%) did not report whether arm swing was permitted during jumps. Nineteen studies (61%) reported the best jump height across three trials, and one study (3%) reported three trials were used but not how the final reported jump height was determined. Eight studies (26%) reported the best jump height across two trials, and three studies (10%) did not report the number of jumps permitted or how final reported jump height was determined. Twelve studies (39%) used the Just Jump Mat, 11 studies (35%) used a yardstick device, six studies (19%) used the Takei Jump System, one study (3%) used chalk markings on a wall, and one study (3%) did not report the equipment used to measure CMJ height. Six studies (60%) examining MBT distance (m) reported players throwing the medicine ball from a seated position and four studies (40%) reported players throwing the medicine ball from a squatting position. Six studies (60%) reported the best throw distance across three trials, three studies (30%) reported the best throw distance across two trials, and one study (10%) did not report the number of trials permitted or how final reported throw distance was determined. Six studies (60%) reported using a 2-kg medicine ball and four studies (40%) report using a 4-kg medicine ball.
Weighted Means for Physical Qualities
Table 8 shows the calculated weighted mean data for the included tests examining physical qualities in male, adolescent rugby league players.
Discussion
This review identifies the most frequently used tests in the literature to assess physical qualities, while concurrently scrutinising testing protocols that provide context to assist with data interpretation and future testing practices. The most frequently used tests to assess physical qualities were: (1) body mass; (2) standing height to measure height; and (3) Σ4 sites to measure skinfold thickness; (4) 10-m sprint test to assess linear speed; (5) 505 Agility Test to assess COD speed; (6) MSFT test to assess aerobic capacity; (7) back squat and bench press 1RM tests to assess lower-body and upper-body muscular strength, respectively; and (8) CMJ and MBT to assess lower-body and upper-body muscular power, respectively. Unfortunately, insufficient data were reported for each playing level and omissions combined with inconsistencies in categorising players according to positional groups across studies precluded the ability to calculate weighted means for each quality according to playing level and position. However, for most included tests in this review, sufficient data were available to provide a weighted mean value for test data according to age group. Notably, these weighted means only include studies which reported the most frequently used protocols consistently across all methodological considerations to permit collation of comparable data. Furthermore, when discussing each of the most frequently used tests below, we will present some critique regarding their application in practice using a recent framework proposed for test selection [37]. Specifically, we will identify the extent to which the reliability and validity of each test were reported specifically for adolescent, male rugby league players among the included studies, and also whether outcomes from each test can be used to guide training prescription [37]. Moreover, we will identify areas in need of further investigation such as additional testing options and deficiencies in evidence, while providing recommendations on the key protocols to adopt if implementing each test in practice.
Anthropometric Qualities
Our data show the most frequently used tests to assess anthropometric qualities are body mass using electronic scales, height measured as standing height using a stadiometer, and skinfold thickness measured as Σ4 sites using Harpenden callipers (Table 1). Indeed, measurement of height and body mass is standard practice, and prior work has demonstrated the importance of measuring these qualities in male, adult rugby league players. Specifically, data from male, semi-professional rugby league players (22.5 ± 4.9 years) demonstrated height is significantly correlated (p < 0.05) with play-the-ball ability (r = − 0.62), performing skills under fatigue (r = − 0.60), and passing ability (r = − 0.51) when assessed using subjective coach ratings [11]. Similarly, body mass was shown to be significantly correlated (p < 0.05) with the ability to hit and spin out of tackles (r = 0.49), offload out of tackles (r = 0.47), passing ability (r = − 0.42), and catching ability (r = − 0.38) when determined using subjective coach ratings [11]. To date, only one study has conducted similar investigation in male, adolescent rugby league players (15.8 ± 0.5 years) [38], but did not find any significant (p > 0.05) relationships between tackling proficiencies and standing height (r = − 0.17) or body mass (r = − 0.21). Nonetheless, given the known relationship between these physical qualities and career attainment [39], measurement of height and body mass and comparisons to benchmark standards may be appropriate in adolescent players. However, greater body mass alone is not desired [30]; instead, greater body mass coupled with lower skinfold thickness may be more advantageous to rugby league players [40]. Despite no available data in male, adolescent rugby league players, skinfold thickness assessed via Σ7 sites was shown to be significantly correlated (p < 0.05) with minutes played (r = − 0.32), tackle attempts (r = − 0.36), completed tackles (r = − 0.38), dominant tackles (r = − 0.36), and tackling efficiency (r = − 0.31) [41] in male, professional rugby league players (23.8 ± 3.8 years). These data demonstrate that players with lower skinfold thickness may spend more time on field and be more effective in executing tackles; however, these weak correlations should be interpreted with caution with further research required to determine the relationship of skinfold thickness to performance during match-play. Consequently, physical qualities appear to correlate with several critical subjective performance metrics, and the periodic measurement of these qualities is warranted to monitor and manage body mass and composition to enhance the prospective performance and career outcomes of male, adolescent rugby league players.
Generally, our data show that standing height and body mass increase with age among male, adolescent rugby league players (Tables 2, 8), which is consistent with previous reviews [3, 4]. Furthermore, our data demonstrate Σ4 skinfold thickness is typically stable across adolescence, and broad standard deviations may be indicative of variations in players across studies (Table 8). The variability in these data may be attributed to the seasonal phase in which testing was applied. In this regard, significant reductions in skinfold thickness (Σ7 sites) have been observed in male, academy rugby league players (17.2 ± 0.7 years) [42] after an early pre-season training intervention lasting 45 days. These data suggest that skinfold thickness depends on training phase and thus the timing of studies can have a considerable impact on this physical quality [43]. These findings highlight the need to better report the seasonal phase in which skinfold assessments are performed. Indeed, most physical qualities may change across seasonal phases, and we therefore recommend the use of periodic testing strategies to best manage and monitor long-term player development; but most critically, we recommend that future research report the seasonal phase to improve the specificity of data available. Nonetheless, the tests used to assess anthropometric qualities and testing protocols adopted were largely consistent in the literature. The most frequently used protocols to assess the Σ4 skinfold thickness were using Harpenden callipers at the biceps, triceps, subscapular, and supra-iliac sites. Given the most frequently used protocol to determine Σ4 sites aligns with those stipulated by The International Society for the Advancement of Kinanthropometry (ISAK) [44], we recommend they continue to be used to ensure consistency across studies while aligning with industry standards.
Across studies using the Σ4 skinfold site thickness assessments included in this review, 13 reported the reliability statistics (ICC = 0.95–0.99; [8, 14, 22, 23, 38, 42, 45,46,47,48,49,50,51] CV = 0.3–3.5% [14, 22, 23, 46]) and none reported the validity for this approach specifically in adolescent, male rugby league players, highlighting the need for more evidence in this population to better inform practitioners when selecting tests to assess skinfold thickness. Moreover, while the sum of skinfold thickness is recognised as a proxy measure for body composition, there are no benchmarks for optimal skinfold thickness in male, adolescent rugby league, nor specific guidance on whether a reduced number of sites is the most appropriate option for this assessment. In this regard, practitioners may consider examining specific player positions (Table 2) for guidance on skinfold thickness qualities, given greater skinfold thickness may be beneficial in some positions compared to others, particularly in those experiencing higher collision rates [22]. We speculate that the Σ4 skinfold sites is likely used most frequently due to its ease of implementation in practice (i.e., low number of sites for efficient measurement with accessible equipment). However, at present the ecological validity of skinfold thickness in male, adolescent rugby league players is unknown, and future research should investigate if there are any associations between skinfold thickness and match play metrics in this population, before further recommendations regarding skinfold assessments are made.
Linear Speed
Our data show the most frequently used test to assess linear speed is the 10-m sprint (s). Indeed, linear speed is a vital quality for rugby league players, with Waldron and colleagues [52] showing a significant relationship (p < 0.05) between 10-m sprint force (product of body mass and acceleration) and successful ball carries across all age groups (i.e., 15.1 ± 0.3 years, Spearman’s R = 0.61; 16.2 ± 0.3 years, Spearman’s R = 0.69; 17.0 ± 0.4 years, Spearman’s R = 0.64) examined in male, elite adolescent rugby league players (16.0 ± 1.3 years). These data not only demonstrate the importance of 10-m sprint speed, but clearly demonstrate the interdependence of key physical qualities in determining rugby league performance. Separate data from male, professional rugby league players (23.6 ± 0.5 years) demonstrate that ~ 68% of sprints during matches occur across distances < 20 m [53]. As such, these data clearly outline the utility of assessing 10-m sprint performances in relation to match demands. However, Gabbett [53] reported ~ 10% of sprints were > 40 m in distance for outside backs compared to ~ 5% for props and adjustables in male, professional rugby league players (23.6 ± 0.5 years). Therefore, certain positional groups may benefit from monitoring sprint performance over longer distances, given the relevance to position-specific match demands. Despite 10-m sprint testing being commonly employed, and evidence of a significant correlation (Pearson’s r = 0.60, p < 0.001) between tackling ability and 10-m sprint times in male, academy, adolescent rugby league players (15.8 ± 0.5 years) [38], further data supporting the validity of this test are derived only from older, professional, male rugby league players (24 ± 3 years) [54]. Consequently, research is required to objectively examine the validity of linear sprint tests in male, adolescent rugby league players, that is to determine whether test performance translates to the movement mechanics and demands experienced during match-play.
In general, improvements (Tables 3, 8) in 10-m sprint times appear to occur throughout adolescence, between 12- and 18-year-old players. However, sprint times do not appear to improve on a year-to-year basis, but instead stabilise across 13- to 14-year-old players and 15- to 18-year-old players, with negligeable differences in sprint times (s) between age groups in later years. Indeed, the stability of 10-m sprint times in older adolescents may indicate the attainment of adequate 10-m sprint performance, at least when assessed using an independent sprinting task. For instance, mean sprint times across the 15- to 18-year age groups are comparable to those reported in male, senior, elite rugby league players (25 ± 3 years) (forwards: 2.08 ± 0.08 s and backs: 2.01 ± 0.10 s) [55]. Certainly, some variation in sprint times between studies examining players aged 16–18 years is evident by the large weighted standard deviations calculated in these age groups, which is likely due to the starting position that players attained prior to sprinting. For example, three studies stated the starting positions of players to be a “pre-determined” distance behind the start line [1, 22, 56], but no specified distance was provided (e.g., 0.5 m). Without this detail, it is unknown whether the starting positions of players in these studies was relatively close to the first light gate, which will create less momentum when initially triggering timing to increase sprint times compared to players starting further behind the first light gate [57]. Similarly, concerns are noted within the 16-year-old age group, with a single study [48] reporting slower sprint times compared to other studies in this age group whereby the starting distance behind the first light gate was also not reported. Collectively, these differences in testing protocols may have inflated sprint times in these older age groups. Given the most frequently used methods to determine 10-m linear sprint performance (i.e., commencing 0.5 m from the start line, best of three trials being used, and electronic timing gates) align with those stipulated by the National Strength and Conditioning Association (NSCA) [58], we recommend they be used in future linear speed assessments to ensure consistency in application while aligning with industry standards.
Across studies using the 10-m sprint included in this review, 20 reported the reliability statistics (ICC = 0.75–0.95 [1, 14, 22, 23, 38, 45, 47,48,49, 51, 56, 59,60,61,62,63,64,65]; CV = 1.3–4.5% [42, 56, 60,61,62, 65, 66]), while one [66] reported the validity of this test specifically for adolescent, male rugby league players. Moreover, while performance time taken from the 10-m sprint can be used to calculate sprint speed, it is unlikely that players will reach peak speed across this distance limiting the ability to prescribe training plans using these data. In this regard, practitioners may consider including sprints across longer distances for enhanced prescriptive utility as well as greater specificity to sprints performed during matches in some positions [53]. When assessing sprints across longer distances, we suggest adopting the previously recommended protocols for 10-m linear speed testing to improve consistency in the rugby league literature. Another important finding was that few studies combined player body mass measurements with sprint results to calculate sprint momentum, and no studies reported running momentum, which has been demonstrated to differentiate between age groups and playing positions in rugby union [67]; these factors should be considered in future research given the relevance of this variable to collision sports like rugby league [4, 68].
Change of Direction Speed
Our data show the most frequently used test to assess COD speed was the 505 Agility Test. Indeed, reactive movement patterns stimulated by an opponent’s actions [10], appropriate positioning when executing technically sound tackles [8, 40], and movements associated with line breaks [69] require highly developed COD speed. Given, the importance of COD speed to perform critical movement patterns during match-play, it is understandable that 505 Agility Test times have been identified as a significant determinant (p < 0.001) of career progression in male, adolescent rugby league players (13.6 ± 0.6 years) [8]. Indeed, COD speed appears a critical component for player success in rugby league; however, research exploring the relationships between COD speed and in-match metrics is not well documented. Specifically, only one study [38] has examined the relationship between 505 Agility Test time and tackling proficiencies (r = − 0.20, p > 0.05) assessed via subjective coach ratings in male, adolescent rugby league players (15.8 ± 0.5 years) without identifying significant relationships. Nonetheless, given the known relationship between COD speed and career attainment [8], measurement of this quality and comparisons to benchmark standards are likely appropriate in adolescent players. Consequently, future work is required to explore the ecological validity of the 505 Agility Test in male, adolescent rugby league players and objectively examine the relationships between COD speed and match metrics.
Typically, our data show improvement in COD speed with increasing age (Tables 4, 8); however, 505 Agility Test data are limited to few age groups (13–16 years) (Table 4), perhaps due to studies adopting multidirectional COD tests (i.e., the L-run test) in older players as demonstrated in our synthesis (Table 4). Our data appear consistent with findings from a previous review [4], with improvements in COD speed with increased age likely explained by development of musculoskeletal strength (Table 8) and coordination throughout adolescence and maturation [4]. Given the most frequently used methods to determine 505-Agility Test performance (i.e., best of three trials being used and electronic timing gates), align with those recommended for linear sprints and are logical to implement, we recommend they be used in future COD speed assessments to ensure consistency in application.
Across studies using the 505-Agility Test included in this review, eight reported the reliability statistics (ICC = 0.82–0.92 [14, 24, 38, 39, 45, 47, 48, 51]; none reported CV), while none reported the validity of this test specifically for adolescent, male rugby league players. Moreover, while performance time taken from the 505-Agility Test indicates COD speed, no assessment of agility (i.e., whole-body movement with change in velocity and/or direction in response to an external stimulus [70]) is provided, with a severe lack of evidence for this quality in male, adolescent rugby league players. Use of appropriate tests to assess agility is essential in future research examining this population given most changes in movement patterns occur in response to external stimuli (e.g., opponent, ball) during training and match scenarios [71]. Nevertheless, if assessment of COD speed is desired, the 505-Agility Test neglects the plethora of multidirectional movements performed in rugby league match-play. In this regard, practitioners may consider using the L-run test [22, 23, 49, 72] (Table 1) that contains multidirectional movement patterns.
Aerobic Capacity
Our data show the most frequently used test to estimate aerobic capacity was the MSFT, which incrementally applies increased speeds to measure endurance running capacity for estimation of \(\dot{\mathrm{V}}\)O2max. Indeed, the intermittent nature of adolescent rugby league match-play [11] combined with the large running distances covered [9] and high energetic demands associated with collisions [73], require a high capacity for aerobic energy supply to cope with match demands. Furthermore, a well-developed aerobic capacity allows for more rapid recovery between high-intensity activity bouts and less accumulated fatigue across matches [74], which is important to maintain skill execution given it deteriorates with increased fatigue, as previously demonstrated in soccer players [75, 76]. In this way, male, professional rugby league players (22.5 ± 4.9 years) with greater estimated \(\dot{\mathrm{V}}\)O2max determined via the MSFT (high = 56.8 ± 1.5 mL kg−1 min−1, low = 52.1 ± 1.9 mL kg−1 min−1) engaged in significantly more (p < 0.05; Cohen’s ES = 0.7) total collisions during matches [77]. Furthermore, male, semi-professional rugby league players (22.5 ± 4.9 years) with greater \(\dot{\mathrm{V}}\)O2max are reported to play-the-ball faster following line engagements (p < 0.05) compared to players with lower aerobic capacities as determined via the MSFT [11]. These findings suggest that a greater aerobic capacity may facilitate quicker recovery following intermittent bouts of running and tackle contests. Although aerobic capacity is undoubtedly an essential physical quality in rugby league, research exploring relationships between aerobic capacity and match metrics is derived from male, senior rugby league players, and yet to be determined for adolescent rugby league players.
Our mean data show aerobic capacity remains relatively stable with marginal fluctuations across age groups (Table 8). Indeed, although the absolute capacity to consume oxygen may increase [78], \(\dot{\mathrm{V}}\)O2max relative to body mass may remain relatively stable across adolescence [79], particularly when considering players are likely accruing lean muscle mass (Table 2). Except for 12-year-old players, the general consistency in estimated \(\dot{\mathrm{V}}\)O2max may suggest that players have obtained adequate levels of aerobic fitness, at least when assessed as an independent running task, to successfully compete as adolescent, rugby league players. Although our synthesis of male, adolescent rugby league players showed aerobic capacities similar to those of semi-professional, rugby league players (47.5 vs. 54.3 mL kg−1 min−1, respectively) [1], future research should confirm the capacity of this test to differentiate between differing playing levels [80]. Given the most frequently used protocols to determine aerobic capacity with the MSFT were uniform and in line with those originally stipulated by Ramsbottom et al. [26], we recommend they continue to be followed if implementing the MSFT.
Across studies using the MSFT included in this review, 12 reported the reliability statistics (ICC = 0.90–0.92 [1, 14, 22, 23, 45,46,47,48,49, 51, 60]; CV = 3.7% [52]), while none reported the validity of this test specifically for adolescent, male rugby league players. While there is support for the MSFT in providing an estimate of \(\dot{\mathrm{V}}\)O2max [26], outcomes taken from this test lack utility for training prescription. Moreover, included studies adopting this test were conducted 6–21 years ago, with many newer tests aimed at assessing aerobic capacity emerging in recent years. Consequently, more contemporary tests to assess aerobic capacity that have been less frequently adopted in adolescent, male rugby league players, such as the 30–15 Intermittent Fitness Test, may counter this practical limitation and provide data with strong support for their application for training prescription in team sports [81, 82].
Muscular Strength
Our data show the most frequently used tests to assess maximal muscular strength were the 1RM bench press and 1RM back squat, for upper-body and lower-body muscular strength, respectively. Desired outcomes in match scenarios such as physically dominating the opposition [69], halting attacking players [12], and generating maximal force when colliding with the defensive line [83], require highly developed muscular strength. Despite the prevalence of 1RM tests among the literature, no study has examined the relationship between 1RM performance and match metrics in male, adolescent rugby league players. However, Johnston and colleagues [74] reported that male, elite, adolescent rugby league players (19.2 ± 0.7 years) with greater strength assessed using the 3RM squat test (high: 145 ± 17 kg; low: 119 ± 9 kg) covered more total running distances (p = 0.04; Cohen’s ES = 0.73), covered more distance at high speed (> 5.1 km h−1; p = 0.01), were involved in more collisions (p = 0.03), and completed more repeated high-intensity efforts (p = 0.02) during match-play than players with less strength [74]. These data demonstrate the importance of assessing muscular strength; however, further research is essential to elucidate relationships between strength assessed via 1RM bench press and 1RM back squat tests and match metrics in male, adolescent rugby league players.
In general, improvements in upper-body maximal muscular strength (via the 1RM bench press and prone row tests) were apparent across consecutive age groups that were examined for this quality (Table 8). Similarly, improvements in lower-body muscular strength are evident between 14- and 18-year-old players, but improvements in 1RM squat strength are not evident at each age interval. Indeed, back squat performance between 14- and 15-year-olds is the only instance a younger age group demonstrated higher mean performance data than that of the successive age group. However, this finding is likely attributed to a single study examining 1RM back squat strength in 14-year-old players [84] using a Smith machine as opposed to a free barbell. Research suggests a Smith machine fully supports and stabilises the barbell [85], which may have permitted heavier loads to be lifted in this study of 14-year-old players [49] compared to studies examining 15-year-old players using a free barbell. Given the most frequently used methods to determine 1RM testing (i.e., three attempts to achieve 1RM with 3-min rest periods permitted between attempts using a 20-kg barbell) align with those stipulated by the NSCA, we recommend they continue to be used in future assessments involving 1RM testing to ensure consistency in application while aligning with industry standards.
Across studies using 1RM testing included in this review, three reported the reliability statistics (ICC = 0.80–0.98 [64, 84, 86]; CV = 3.6% [86]) while none reported the validity of these tests specifically for adolescent, male rugby league players. Despite 1RM testing being the most frequently used assessment of muscular strength, the isometric midthigh pull (IMTP) has been adopted more recently as an assessment of whole-body strength and power in senior (n = 33, 25.3 ± 3.4 years) and adolescent (n = 23, 18.3 ± 1.4 years) male, rugby league players [87]. While the IMTP has fewer technical demands, which may benefit adolescent rugby league players who likely have accrued less training experience than their senior counterparts [87], 1RM tests typically replicate fundamental resistance training movements with the acquired data allowing precise prescription of resistance exercise loads at an individual level [37]. Certainly, the IMTP may be used to determine peak force and rate of force development, providing information about whether emphasis should be placed on strength- or power-based training interventions [88]; however, the equipment required for IMTP assessment make it cost-prohibitive in many adolescent rugby league environments. While application of the IMTP is well documented [88], no evidence demonstrates the utility of IMTP data for exercise prescription in adolescent rugby league players, suggesting further research is needed on this topic.
Muscular Power
Our data show the most frequently used tests to assess muscular power were the CMJ and MBT tests, for lower-body and upper-body muscular power, respectively. Indeed, the application of instantaneous force in tackles [69] and high-velocity movement patterns [83] is dependent on the ability to produce high levels of muscular power. Jump height derived from the CMJ is often used as a proxy measure of lower-body muscular power [17]. Indeed, CMJ height (cm) has been demonstrated to significantly correlate (η = 0.44, p < 0.05) with beating an opposing player when assessed via subjective coach ratings in male, elite rugby league players (22.5 ± 4.9 years) [11]. However, to date, no work has evaluated the relationship between CMJ and match metrics in male, adolescent rugby league players. Furthermore, no research has evaluated whether the MBT test is related to any match metric in rugby league players at any age, despite this test being widely used in the rugby league literature. Nonetheless, significant correlations between upper-body muscular power measured using a plyometric push-up test and tackling ability (r = 0.65, p = 0.01) have been reported in male, semi-professional rugby league players (23.1 ± 3.6 years) [12]. The examination of similar relationships between the MBT test and match metrics is needed in future research.
In general, our data show increased CMJ height with age among adolescent players (Table 8). Certainly, typical growth during adolescence in conjunction with an increase in resistance training programming likely contribute to the accruement of lean muscle mass [89], greater absolute strength [79] and power [90], and increased neuromuscular function [91] to increase force application. However, CMJ data among 17-year-old players are substantially lower than other age groups, which may be explained by four studies from the same authorship group that report considerably lower jump height [42, 62, 65, 66]. These studies report use of a correction equation, stipulated in previous research [92, 93], to be used when utilising the Just Jump system. Despite the use of this recommended equation, these studies have produced substantially lower jump heights than other work examining similar cohorts. Importantly, we note greater variability in equipment selection with the CMJ compared to any other test, which will likely impact data. For instance, evidence suggests substantial differences in jump height can result when using electronically predicted height (jump mat systems) compared to manual height determination (Yardstick device) [15, 94]; however, these findings may be due to differences in protocols and thus jump techniques, whereby manual devices require a reaching action that induce greater jump height. Differing protocols for the MBT were adopted between studies conducted by two authorship groups, primarily led by Till and colleagues [8, 45, 50, 51, 95] (62.5%) and by Dobbin and colleagues [42, 62, 66] (36.5%). Nevertheless, differences in protocols across studies did not appear to affect the increased performance during the MBT with advancing age.
Across studies using the CMJ test included in this review, 21 reported the reliability statistics (ICC = 0.90–0.97 [1, 14, 22, 23, 38, 42, 45, 46, 48, 49, 51, 52, 59,60,61,62, 64,65,66, 96, 97]; CV = 1.1–5.9% [42, 46, 52, 59,60,61,62, 65, 66, 96] while one [66] reported the validity of this test specifically for adolescent, male rugby league players. Although the CMJ test has been well investigated, the commonly reported jump height data is not directly used for exercise prescription nor a direct representation of muscular power. Consequently, alternative data derived from the CMJ may hold greater prescriptive utility [98]. Further, minor variations in jump strategies and equipment selection can profoundly affect test data; for instance, equipment that predicts jump height based on flight time such as jump mats, can be manipulated by the jump strategies adopted by players [99]. To this end, the lack of methodological consistency in protocols across studies included in this review meant we were unable to provide recommendations on the most frequently adopted protocols or calculate a weighted mean, and therefore benchmark data, for the CMJ. Given these variations, it is important that appropriate procedures with equipment suited to the desired data be adopted (e.g., force plate or linear position transducer for force or velocity measurement); however, the high expense associated with some technologies may make them cost-prohibitive for many adolescent rugby league teams, which should be considered. Across studies using the MBT test included in this review, six reported the reliability statistics (ICC = 0.74–0.97 [45, 51, 62]; CV = 0.6–9% [42, 65, 66]), while one [66] reported the validity of this test specifically for adolescent, male rugby league players. Similar to the CMJ test, alternative tests that offer greater prescriptive utility warrant further investigation, given throw distance is not directly translatable to an exercise prescription. Nonetheless, in line with the approach adopted in many studies included in this review and that recommended for other tests, the best of three trials should be adopted for the CMJ and MBT tests with suitable equipment employed to gather data meeting the practical needs in light of the constraints faced.
Limitations
Although our review provides the most comprehensive assessment of the tests used, testing protocols adopted, and data obtained for physical qualities in male, adolescent rugby league players, several limitations should be acknowledged. First, this review included only common physical qualities previously identified as key determinants of career success in male, adolescent rugby league players [4]. Other physical qualities may be useful to consider as the evidence base grows in this field, which may include but are not limited to muscular endurance [100], mobility, and agility [80]. Second, for consistency, the data synthesised in this review were obtained from the first testing occasion reported in any study (i.e., prior to intervention and repeated assessments across the season). As a result of this approach, data are reported irrespective of seasonal phase, which may add variability to the dataset. Therefore, we recommend future research investigate changes in physical qualities across seasonal phases to further advance the understanding of longitudinal development in male, adolescent rugby league players. Unfortunately, few studies explicitly report the seasonal phase that testing occurred, and therefore seasonal phase was inferred in some instances based on the month and location of studies. Given pre-season intervention influences physical test data [59, 101], future work should clearly report the seasonal phase in which testing occurred to enable comparisons of like data. Third, data were typically reported according to chronological age rather than maturity status across published studies on this topic, which also aligns with the typical approaches adopted to delineate levels within adolescent rugby league competitions. However, we acknowledge that maturity status varies across adolescence and may yield different trends than what we observed if categorised this way. Fourth, we collated and scrutinised only key protocol-related aspects of each test included in our review and acknowledge these do not encompass all aspects that may influence the acquired data. However, we identified key aspects for each test that require precise implementation and reporting to ensure consistency in test administration and to minimise variations in data reported across future studies. Finally, our weighted mean dataset is representative of players competing across all playing levels and positions regardless of the protocols adopted for each specific test. Although we acknowledge it is important to establish normative data according to playing level and playing position given their impact on match demands [53] as well as physical qualities among rugby league players, a lack of research attention given to amateur and elite players combined with omission of, and inconsistencies in assigning, positional groups across studies precluded these calculations.
Conclusion
Our review has identified the most frequently used tests as body mass, standing height, and Σ4 skinfold sites to assess anthropometric qualities, while the 10-m sprint, 505 Agility Test, MSFT, 1RM back squat and bench press, and CMJ and MBT were the most frequently used tests to assess linear speed, COD speed, aerobic capacity, muscular strength, and muscular power qualities, respectively. Further, our review identified and scrutinised the protocols adopted across studies for each of these tests, enabling us to provide recommendations in accordance with industry standards for most tests when implemented in future practice. While the reliability of most tests was supported across studies included in this review, many studies that reported reliability statistics within methodology sections did so without explicit mention of the procedures undertaken to derive them. Furthermore, the validity assessments were lacking, highlighting the need for further research exploring various forms of validity for each test to better inform practitioners on their suitability for implementation [37]. In addition, we synthesised and stratified data for each test according to age group, providing novel benchmarks for all the most frequently used tests except the CMJ test, which could not be provided due to variability and inconsistency in testing protocols across studies. These data may be used as age-specific references for male, adolescent rugby league players and should be further updated according to playing level and positional groups as more data become available.
Availability of Data and Materials
Data generated and analysed in this study are included in this published article and its supplementary information files.
Abbreviations
- COD:
-
Change of direction
- PRISMA:
-
Preferred reporting items of systematic reviews and meta-analyses
- 1RM:
-
1 Repetition maximum
- CMJ:
-
Countermovement jump
- MBT:
-
Medicine ball throw
- Σ4:
-
Sum of four skinfolds
- MSFT:
-
Multistage fitness test
- ISAK:
-
The International Society for the Advancement of Kinanthropometry
- \(\dot{\mathrm{V}}\)O2max :
-
Maximum oxygen consumption
References
Gabbett TJ. Physiological characteristics of junior and senior rugby league players. Br J Sports Med. 2002;36(5):334–9.
Dempsey GM, Gibson NV, Sykes D, Pryjmachuk BC, Turner AP. Match demands of senior and junior players during international rugby league. J Strength Cond Res. 2018;32(6):1678–84.
Brewer J, Davis J. Applied physiology of rugby league. Sports Med. 1995;20:129–35.
Till K, Scantlebury S, Jones B. Anthropometric and physical qualities of elite male youth rugby league players. Sports Med. 2017;47(11):2171–86.
Chiwaridzo M, Ferguson GD, Smits-Engelsman BCM. Qualities or skills discriminating under 19 rugby players by playing standards: a comparative analysis of elite, sub-elite and non-rugby players using the SCRuM test battery. BMC Res Notes. 2019;12(1):536.
Usher WT. National rugby league’s junior performance and participation initiatives: evaluating stratergies. 2019.
Gabbett TJ. Physiological and anthropometric characteristics of elite women rugby league players. J Strength Cond Res. 2007;21(3):875–81.
Till K, Cobley S, O’Hara J, Morley D, Chapman C, Cooke C. Retrospective analysis of anthropometric and fitness characteristics associated with long-term career progression in rugby league. J Sci Med Sport. 2015;18(3):310–4.
Whitehead S, Till K, Weaving D, Hunwicks R, Pacey R, Jones B. Whole, half and peak running demands during club and international youth rugby league match-play. Sci Med Footb. 2018;3(1):63–9.
Delaney JA, Scott TJ, Ballard DA. Contributing factors to change-of-direction ability in professional rugby league players. J Strength Cond Res. 2015;29(10):2688–96.
Gabbett T, Kelly J, Pezet T. Relationship between physical fitness and playing ability in rugby league players. J Strength Cond Res. 2007;21(4):1126–33.
Sparanza MJ, Gabbett TJ, Johnston RD, Sheppart JM. Muscular strength and power correlates of tackling ability in semiprofessional rugby league players. J Strength Cond Res. 2015;29(8):2071–8.
Kirkpatrick J, Comfort P. Strength, power, and speed qualities in english junior elite rugby league players. J Strength Cond Res. 2013;27(9):2414–9.
Gabbett T, Kelly J, Ralph S, Driscoll D. Physiological and anthropometric characteristics of junior elite and sub-elite rugby league players, with special reference to starters and non-starters. J Sci Med Sport. 2009;12(1):215–22.
McMahon J, Jones P, Comfort P. Comment on: “Anthropometric and physical qualities of elite male youth rugby league players.” Sports Med. 2017;47(12):2667–8.
Chiwaridzo M, Oorschot S, Dambi JM, Ferguson GD, Bonney E, Mudawarima T, et al. A systematic review investigating measurement properties of physiological tests in rugby. BMC Sports Sci Med Rehabil. 2017;9:24.
McMahon J, Murphy S, Rej S, Comfort P. Countermovement jump phase characteristics of senior and academy rugby league players. Int J Sports Physiol Perform. 2017;12(6):803–11.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52:377–84.
Naughton M, Jones B, Hendricks S, King D, Murphy A, Cummins C. Quantifying the collision dose in rugby league: a systematic review, meta-analysis, and critical analysis. Sports Med Open. 2020;6(1):6.
Glassbrook D, Doyle T, Alderson J, Fuller J. The demands of professional rugby league match-play: a meta-analysis. Sports Med Open. 2019;5:24.
Deeks J, Dinnes J, D’Amico R, Sowden A, Sakarovitch C, Petticrew M, et al. Evaluating non-randomised intervention studies. Health Technol Assess. 2003;7(27):1–173.
Gabbett T. A comparison of physiological and anthropometric characteristics among playing positions in junior rugby league players. Br J Sports Med. 2005;39(9):675–80.
Gabbett TJ. Physiological and anthropometric characteristics of junior rugby league players over a competitive season. J Strength Cond Res. 2005;19(4):764–71.
Gabbett TJ, Herzig PJ. Physiological characteristics of junior elite and sub-elite rugby league players. Strength Cond Coach. 2004;12:19–24.
McKay AKA, Stellingwerff T, Smith ES, Martin DT, Mujika I, Goosey-Tolfrey VL, et al. Defining training and performance caliber: a participant classification framework. Int J Sports Physiol Perform. 2022;17(2):317–31.
Ramsbottom R, Brewer J, Williams C. A progressive shuttle run test to estimate maximal oxygen uptake. Br J Sports Med. 1988;22(4):141–4.
Morehen JC, Clarke J, Batsford J, Highton J, Erskine RM, Morton JP, et al. Development of anthropometric characteristics in professional rugby league players: is there too much emphasis on the pre-season period? Euro J Sport Sci. 2020;20(8):1013–22.
Till K, Cobley S, O’Hara J, Chapman C, Cooke C. An individualized longitudinal approach to monitoring the dynamics of growth and fitness development in adolescent athletes. J Strength Cond Res. 2013;27(5):1313–21.
Till K, Jones B, O’Hara J, Barlow M, Brightmore A, Lees M, et al. Three-compartment body composition in academy and senior rugby league players. Int J Sports Physiol Perform. 2016;11(2):191–6.
Cheng HL, O’Connor H, Kay S, Cook R, Parker H, Orr R. Anthropometric characteristics of Australian junior representative rugby league players. J Sci Med Sport. 2014;17(5):546–51.
Baker D. Comparison of upper-body strength and power between professional and college-aged rugby league players. J Strength Cond Res. 2001;15(1):30–5.
Ireton MRE, Till K, Weaving D, Jones B. Differences in the movement skills and physical qualities of elite senior and academy rugby league players. J Strength Cond Res. 2019;33(5):1328–38.
Till K, Jones B. Monitoring anthropometry and fitness using maturity groups within youth rugby league. J Strength Cond Res. 2015;29(3):730–6.
Mandigout S, Alaphilippe A, Dudognon P, Bouteille B. Physical and anthropometric parameters evolution of the young elite of French rugby players. Sci Sports. 2008;23(1):16–8.
McMahon JJ, Suchomel TJ, Lake JP, Comfort P. Relationship between reactive strength index variants in rugby league players. J Strength Cond Res. 2021;35(1):280–5.
Scott TJ, Delaney JA, Duthie GM, Sanctuary CE, Ballard DA, Hickmans JA, et al. Reliability and usefulness of the 30–15 intermittent fitness test in rugby league. J Strength Cond Res. 2015;29(7):1985–90.
Weakley J, Black G, McLaren S, Scantlebury S, Suchomel TJ, McMahon E, et al. Testing and profiling athletes: recommendations for test selection, implementation, and maximizing information. Strength Cond J. 2023. https://doi.org/10.1519/SSC.0000000000000784.
Gabbett TJ, Jenkins DG, Abernethy B. Physiological and anthropometric correlates of tackling ability in junior elite and subelite rugby league players. J Strength Cond Res. 2010;24(11):2989–95.
Till K, Cobley S, Morley D, O’hara J, Chapman C, Cooke C. The influence of age, playing position, anthropometry and fitness on career attainment outcomes in rugby league. J Sports Sci. 2016;34(13):1240–5.
Gabbett T. Physiological and anthropometric correlates of tackling ability in rugby league players. J Strength Cond Res. 2009;23(2):540–8.
Gabbett TJ, Jenkins DG, Abernethy B. Relationships between physiological, anthropometric, and skill qualities and playing performance in professional rugby league players. J Sports Sci. 2011;29(15):1655–64.
Dobbin N, Gardner A, Daniels M, Twist C. The influence of` preseason training phase and training load on body composition and its relationship with physical qualities in professional junior rugby league players. J Sports Sci. 2018;36(24):2778–86.
Meir RA. Seasonal changes in estimates of body composition in professional rugby league players. Sport Health. 1993;11:27–31.
Stewart A, Marfell-Jones M, Olds T, Hans De Ridder J. International standards for anthropometric assessment. Wellington: International Society of the Advancement of Kinanthropometry; 2011.
Till K, Cobley S, O’Hara J, Brightmore A, Cooke C, Chapman C. Using anthropometric and performance characteristics to predict selection in junior UK rugby league players. J Sci Med Sport. 2011;14(3):264–9.
Waldron M, Worsfold P, Twist C, Lamb K. Changes in anthropometry and performance, and their interrelationships, across three seasons in elite youth rugby league players. J Strength Cond Res. 2014;28(11):3128–36.
Gabbett TJ, Johns J, Riemann M. Performance changes following training in junior rugby league players. J Strength Cond Res. 2008;22(3):910–7.
Gabbett TJ. Physiological and anthropometric characteristics of starters and non-starters in junior rugby league players, aged 13–17 years. J Sports Med Phys Fit. 2009;49(3):233–9.
Gabbett TJ. Performance changes following a field conditioning program in junior and senior rugby league players. J Strength Cond Res. 2006;20(1):215–21.
Till K, Morley D, O’Hara J, Jones BL, Chapman C, Beggs CB, et al. A retrospective longitudinal analysis of anthropometric and physical qualities that associate with adult career attainment in junior rugby league players. J Sci Med Sport. 2017;20(11):1029–33.
Till K, Cobley S, O’Hara J, Chapman C. Anthropometric, physiological and selection characteristics in high performance UK junior rugby league players. Talent Dev Excell. 2013;2(2):193–207.
Waldron M, Worsfold PR, Twist C, Lamb K. The relationship between physical abilities, ball-carrying and tackling among elite youth rugby league players. J Sports Sci. 2014;32(6):542–9.
Gabbett TJ. Sprinting patterns of national rugby league competition. J Strength Cond Res. 2012;26(1):121–30.
Austin DJ, Gabbett TJ, Jenkins DG. Reliability and sensitivity of a repeated high-intensity exercise performance test for rugby league and rugby union. J Strength Cond Res. 2013;27(4):1128–35.
Cross MR, Brughelli M, Brown SR, Samozino P, Gill ND, Cronin JB, et al. Mechanical properties of sprinting in elite rugby union and rugby league. Int J Sports Physiol Perform. 2015;10(6):695–702.
Nicholson B, Dinsdale A, Jones B, Till K. Sprint and jump mechanical profiles in academy rugby league players: positional differences and the associations between profiles and sprint performance. Sports (Basel). 2021;9(7):93.
Altmann S, Hoffmann M, Kurz G, Neumann R, Woll A, Haertel S. Different starting distances affect 5-m sprint times. J Strength Cond Res. 2015;29(8):2361–6.
Miller T. NSCA’s guide to tests and assessments. Champaign: Human Kinetics; 2012.
Till K, Jones B, Emmonds S, Tester E, Fahey J, Cooke C. Seasonal changes in anthropometric and physical characteristics within english academy rugby league players. J Strength Cond Res. 2014;28(9):2689–96.
Tredrea M, Dascombe B, Sanctuary CE, Scanlan AT. The role of anthropometric, performance and psychological attributes in predicting selection into an elite development programme in older adolescent rugby league players. J Sports Sci. 2017;35(19):1897–903.
Till K, Jones B, Darrall-Jones J, Emmonds S, Cooke C. Longitudinal development of anthropometric and physical characteristics within academy rugby league players. J Strength Cond Res. 2015;29(6):1713–22.
Dobbin N, Hunwicks R, Highton J, Twist C. A reliable testing battery for assessing physical qualities of elite academy rugby league players. J Strength Cond Res. 2018;32(11):3232–8.
Darrall-Jones JD, Jones B, Roe G, Till K. Reliability and usefulness of linear sprint testing in adolescent rugby union and league players. J Strength Cond Res. 2016;30(5):1359–64.
Coutts AJ, Murphy AJ, Dascombe BJ. Effect of direct supervision of a strength coach on measures of muscular strength and power in young rugby league players. J Strength Cond Res. 2004;18(2):316–23.
Dobbin N, Highton J, Moss SL, Twist C. Factors affecting the anthropometric and physical characteristics of elite academy rugby league players: A multiclub study. Int J Sports Physiol Perform. 2019;14(7):958–65.
Dobbin N, Highton J, Moss SL, Twist C. The discriminant validity of a standardized testing battery and Its ability to differentiate anthropometric and physical characteristics between youth, academy, and senior professional rugby league players. Int J Sports Physiol Perform. 2019;14(8):1110–6.
Darrall-Jones JD, Jones B, Till K. Anthropometric, sprint, and high-intensity running profiles of English academy rugby union players by position. J Strength Cond Res. 2016;30(5):1348–58.
Weakley J, McCosker C, Chalkley D, Johnston R, Munteanu G, Morrison M. Comparison of sprint timing methods on performance, and displacement and velocity and timining initiation. J Strength Cond Res. 2022. https://doi.org/10.1519/JSC.0000000000004223.
Johnston RD, Gabbett TJ, Jenkins DG. Applied sport science of rugby league. Sports Med. 2014;44(8):1087–100.
Young W, Rayner R, Talpey S. It’s time to change direction on agility research: a call to action. Sports Med Open. 2021;7(1):12.
Gabbett T, Benton D. Reactive agility of rugby league players. J Sci Med Sport. 2009;12(1):212–4.
Pearce A, Sinclair W, Leicht A, Anthony S, Woods C. Physical, anthropometric, and athletic movement qualities discriminate development level in a rugby league talent pathway. J Strength Cond Res. 2018;32(11):3169–76.
Lovell D, Harvey L, McLellan C. The upper and lower body aerobic fitness of semi-elite rugby league. J Aero Fit. 2016. https://doi.org/10.4172/JAFO.1000101.
Johnston RD, Gabbett TJ, Jenkins DG, Hulin BT. Influence of physical qualities on post-match fatigue in rugby league players. J Sci Med Sport. 2015;18(2):209–13.
Silverman MN, Deuster PA. Biological mechanisms underlying the role of physical fitness in health and resilience. Interface Focus. 2014;4(5):20140040.
Sun H, Soh KG, Roslan S, Wazir M, Soh KL. Does mental fatigue affect skilled performance in athletes? A systematic review. PLoS ONE. 2021;16(10):e0258307.
Gabbett TJ, Stein JG, Kemp JG, Lorenzen C. Relationship between tests of physical qualities and physical match performance in elite rugby league players. J Strength Cond Res. 2013;27(6):1539–45.
Armstrong N, Welsman J, Winsley R. Is peak VO2 a maximal index of children’s aerobic fitness? Int J Sports Med. 1996;17(5):356–9.
Meyer F, Timmons BW. The Encyclopedia of sports medicine. 2013:359–68.
Gabbett T, Kelly J, Sheppard J. Speed, change of direction speed, and reactive agility of rugby league players. Strength Cond. 2008;22(1):174–81.
Buchheit M. The 30–15 intermittent fitness test: accuracy for individualizing interval training of young intermittent sport players. J Strength Cond Res. 2008;22(2):365–74.
Scott T. Testing, prescribing and monitoring training in team sports: the efficiency and versatility of the 30–15 Intermittent Fitness Test. Sport Perf Sci. 2018.
Redman KJ, Kelly VG, Beckman EM. Seasonal changes in strength and power in elite rugby league: a systematic review and meta-analysis. J Sports Sci Med. 2021;20(4):721–31.
Alonso-Aubin DA, Chulvi-Medrano I, Cortell-Tormo JM, Picón-Martínez M, Rial Rebullido T, Faigenbaum AD. Squat and bench pess force-velocity profiling in male and female adolescent rugby players. J Strength Cond Res. 2021;35(1):S44-S50.
Schwanbeck S, Chilibeck PD, Binsted G. A comparison of free weight squat to Smith machine squat using electromyography. J Strength Cond Res. 2009;23(9):2588–91.
Fernandes JFT, Daniels M, Myler L, Twist C. Influence of playing standard on upper- and lower-body strength, power, and velocity characteristics of elite rugby league players. J Funct Morphol Kinesiol. 2019;4(2):22.
Dobbin N, Hunwicks R, Jones B, Till K, Highton J, Twist C. Criterion and construct validity of an isometric midthigh-pull dynamometer for assessing whole-body strength in professional rugby league players. Int J Sports Physiol Perform. 2018;13(2):235–9.
Martin EA, Beckham GK. Isometric mid-thigh pull performance in rugby players: a systematic literature review. J Funct Morphol Kinesiol. 2020;5(4):91.
Brown KA, Patel DR, Darmawan D. Participation in sports in relation to adolescent growth and development. Transl Pediatr. 2017;6(3):150–9.
Ratel S, Martin V. Is there a progressive withdrawal of physiological protections against high-intensity exercise-induced fatigue during puberty? Sports. 2015;3(4):346–57.
Gillen Z, Shoemaker M, McKay B, Bohannon N, Gibson S, Cramer J. Muscle strength, size, and neuromuscular function before and during adolescence. Eur J Appl Physiol. 2019;119(7):1619–32.
Dobbin N, Hunwicks R, Highton J, Twist C. Validity of a jump mat for assessing countermovement jump performance in elite rugby players. Int J Sports Med. 2017;38(2):99–104.
McMahon JJ, Jones PA, Comfort P. A correction equation for jump height measured using the just jump system. Int J Sports Physiol Perform. 2016;11(4):555–7.
McMahon JJ, Lake T, Dos’Santos T, Jones PA, Thomasson ML, Comfort P. Countermovement jump standards in rugby league: what is a “good” performance? J Strength Cond Res. 2020;36(6):1691–8.
Till K, Cobley S, O’Hara J, Cooke C, Chapman C. Considering maturation status and relative age in the longitudinal evaluation of junior rugby league players. Scand J Med Sci Sport. 2014;24(3):569–76.
Till K, Tester E, Jones B, Emmonds S, Fahey J, Cooke C. Anthropometric and physical characteristics of english academy rugby league players. J Strength Cond Res. 2014;28(2):319–27.
Till K, Darrall-Jones J, Weakley JJ, Roe GA, Jones BL. The influence of training age on the annual development of physical qualities within academy rugby league players. J Strength Cond Res. 2017;31(8):2110–8.
Morin JB, Jimenez-Reyes P, Brughelli M, Samozino P. When jump height is not a good indicator of lower limb maximal power output: theoretical demonstration, experimental evidence and practical solutions. Sports Med. 2019;49(7):999–1006.
Vaverka F, Jandacka D, Zahradnik D, Uchytil J, Farana R, Supej M, et al. Effect of an arm swing on countermovement vertical jump performance in elite volleyball players: final. J Hum Kinet. 2016;53:41–50.
Gabbett T, King T, Jenkins D. Applied physiology of rugby league. Sports Med. 2008;38(2):119–38.
Argus CK, Gill N, Keogh J, Hopkins WG, Beaven CM. Effects of a short-term pre-season training programme on the body composition and anaerobic performance of professional rugby union players. J Sports Sci. 2010;28(6):679–86.
Till K, Cobley S, O’Hara J, Chapman C, Cooke C. A longitudinal evaluation of anthropometric and fitness characteristics in junior rugby league players considering playing position and selection level. J Sci Med Sport. 2013;16(5):438–43.
Till K, Jones B, Geeson-Brown T. Do physical qualities influence the attainment of professional status within elite 16–19 year old rugby league players? J Sci Med Sport. 2016;19(7):585–9.
Dobbin N. Sprint mechanical properties of professional rugby league players according to playing standard, age and position, and the association with key physical characteristics. J Sports Med Phys Fit. 2022;62(4):467–75.
Baker D. Differences in strength and power among junior-high, senior-high, college-aged, and elite professional rugby league players. J Strength Cond Res. 2002;16(4):581–5.
Acknowledgements
Not applicable.
Funding
MC is the recipient of a Elevate Scholarship at Central Queensland University which is co-funded by St Brendan’s College. MC is the recipient of a Central Queensland University International Excellence Award.
Author information
Authors and Affiliations
Contributions
Authors MC, AS, and TD contributed to the study conception and design. Material preparation, data collection, and analysis were performed by MC. Secondary confirmation of data collection was performed by CP. The first draft of the manuscript was written by MC. AS and TD reviewed and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
This systematic review complies with ethical standards and practices.
Consent for Publication
Informed consent was not required to conduct this systematic review.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table A.
Search terms and strategy used to retrieve studies examining the physical qualities of adolescent rugby league players.
Additional file 2: Table B.
Modified Downs and Black checklist used to assess the methodological quality of the included studies.
Additional file 3: Table C.
Results of risk of bias and methodological quality assessment for the included studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Carron, M.A., Scanlan, A.T., Power, C.J. et al. What Tests are Used to Assess the Physical Qualities of Male, Adolescent Rugby League Players? A Systematic Review of Testing Protocols and Reported Data Across Adolescent Age Groups. Sports Med - Open 9, 106 (2023). https://doi.org/10.1186/s40798-023-00650-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-023-00650-z