
Abstract
Background
Power training (PT) has been shown to be an effective method for improving muscle function, including maximal strength, measured by one-repetition maximum (1RM), and power output in older adults. However, it is not clear how PT intensity, expressed as a percentage of 1RM, affects the magnitude of these changes. The aim of this systematic review (International prospective register of systematic reviews—PROSPERO—registration: CRD42022369874) was to summarize the evidence from randomized clinical trials (RCT) assessing the effects of low-intensity (≤ 49% of 1RM) and moderate-intensity (50–69% of 1RM) versus high-intensity (≥ 70% of 1RM) PT on maximal power output and maximal strength in older adults.
Methods
We included RCTs that examined the effects of different intensities of power training on maximum strength and power output in older people. The search was performed using PubMed, LILACS, Embase, and Scopus. Methodological quality was assessed using the preferred reporting items for systematic reviews and meta-analyses (PRISMA 2020 statement checklist), and the quality of evidence was determined using the PEDro scale. Data were analyzed using standardized mean differences (SMD) with a 95% confidence interval (CI), and random effects models were used for calculations. A significance level of p ≤ 0.05 was accepted.
Results
Three RCTs assessing 179 participants, all of high methodological quality, were included. There were no significant differences between different PT intensities in terms of power output gains for leg press [SMD = 0.130 (95% CI − 0.19, 0.45), p = 0.425] and knee extension exercises [SMD: 0.016 (95% CI − 0.362, 0.395), p = 0.932], as well as leg press 1RM increases [SMD: 0.296 (95% CI − 0.03, 0.62); p = 0.072]. However, high-intensity PT (70–80% of 1RM) was significantly more effective than low-intensity PT in increasing 1RM for knee extension exercise [SMD: 0.523 (95% CI 0.14, 1.91), p = 0.008].
Conclusions
PT performed at low-to-moderate intensities induces similar power gains compared to high-intensity PT (70–80% of 1RM) in older adults. Nonetheless, the influence of PT intensity on lower-limb strength gains seems to be dependent on the assessed exercise. Cautious interpretation is warranted considering the inclusion of only three studies.
Key Points
-
Different intensities of power training (PT) promote similar increases in power output of leg press and knee extension exercises, as well as maximum strength of leg press exercise in older adults.
-
High-intensity PT (70–80% of 1RM) seems to be more effective than low-intensity (20–40% of 1RM) PT in increasing maximum strength for knee extension.
-
The results advance knowledge regarding the power training prescription, as they indicate that low- to moderate-intensity is a sufficient stimulus to promote marked improvements in mechanical muscle function in older adults.
Similar content being viewed by others

Background
Power training, also known as explosive resistance training, is a type of resistance training that involves performing concentric muscle actions as fast as possible. This form of training has been widely recommended to improve physical functioning in older adults, as evidenced by several studies [1,2,3]. This recommendation has been applied not only to healthy older individuals [4,5,6,7], but also to those with chronic diseases such as diabetes mellitus and hypertension [8,9,10,11], geriatric syndromes [12,13,14], and even acutely hospitalized older patients [15, 16].
The rationale for prescribing power training in older adults is based on the following premises: first, muscle power output is more strongly associated with functional capacity than maximal strength and muscle size [17, 18]; second, muscle power output declines at a greater rate than maximal strength and muscle size during aging [19, 20]. Indeed, studies have shown that muscle power training induces superior gains in functional tests performance [21, 22], along with comparable gains in maximal strength and muscle hypertrophy [5] in older individuals.
Despite the recommendation for power training in older adults, the manipulation of power training variables (such as volume, intensity, and weekly frequency) to optimize its dose–response relationship has received less investigation compared to traditional resistance training variables. For instance, several meta-analyses have shown that maximal strength gains are optimized when resistance training intensity progresses to loads between 70 and 80% of one-repetition maximum (1RM) [23, 24]. However, research on power training intensity in older adults is limited, with few studies investigating the adaptations induced by different intensities (low- to moderate- vs. high-intensity) and showing no differences in maximal power output gains [25,26,27]. Regarding maximal strength gains, the results are controversial as one study observed an advantage in favor of high-intensity power training (i.e., 80% of 1RM) in single joint exercise, but no difference in multi-joint exercises was observed [27]. In addition, another study has shown that maximal strength increases with no differences between low and high-intensity power training, independently of the exercise [26].
Thus, there are controversial findings regarding the necessity of using higher intensities during power training in older adults to maximize mechanical muscle function gains. Therefore, a systematic review with meta-analysis is necessary to provide more solid evidence, considering these scarce and controversial findings in the literature. This study aims to summarize the evidence regarding the effects of different intensities of power training on maximal strength and maximal power output in older adults. We hypothesize that there will be no differences between low- to moderate-intensity versus high-intensity power training for muscle power output, but an advantage will be observed in favor of high-intensity power training for maximal strength.
Methods
Protocol and Registration
This research followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA 2020 statement checklist) and was registered in the International Prospective Register of Systematic Reviews (PROSPERO, CRD42022369874) [28, 29].
Eligibility Criteria
The eligibility criteria were based on the previously defined PICOT strategy (P, population: older adults; I, intervention: power training; C, comparator: different intensities of power training; O, outcomes: maximal strength gains, power output and/or muscle hypertrophy; T, type: randomized clinical trials). Thus, the eligible articles for this study were randomized clinical trials that compared the effects of at least two power training intensities, specifically high intensity (≥ 70% of 1RM) versus moderate (50–69% of 1RM) or low intensity (≤ 49% of 1RM). The interventions needed to include encouragement to participants to exert their maximal velocity during the concentric phase of each repetition. The study outcomes assessed included maximal dynamic strength, muscle power, and muscle hypertrophy in older individuals. Only manuscripts published in English language peer-reviewed journals were considered, and studies were included if they assessed older populations aged 60 years or older. Studies were excluded if they assessed individuals with any muscle injury or clinical condition that directly influenced the outcomes of interest.
Search Strategy
The search was carried out in September of 2022 and updated in August 2023 using the electronic databases PubMed, LILACS, Embase, and Scopus. Additionally, manual searches of the references of the included studies were performed. There were no restrictions regarding the year of publication. The investigation comprised the following terms and MeSH terms (and their respective related terms): resistance training, power training, power-oriented resistance training, peak power, muscle performance, and hypertrophy. To optimize the capture of relevant references, such terms were combined by Boolean operators (OR and AND). Searches were delimited to the following fields: titles, descriptors, and abstract, and the selected descriptors should have been included in at least one of the three research fields. The full search strategy performed in the PubMed database is available in Additional file 1.
Selection of Studies
The selection of studies was based on the eligibility criteria previously described, and each phase was carried out separately by two researchers and analyzed by a third reviewer as follows. First, two researchers independently evaluated the titles and abstracts of all studies found in the search (M.B-G. and E.B-R.). Studies with abstracts that did not provide sufficient information as per the inclusion and exclusion criteria were assessed separately in full. Subsequently, each study was assesses by the reviewers independently. Disagreements were resolved by consensus and, in cases of persistence, a third investigator adjudicated on the disagreement between the researchers (E.L.C.).
Data Collection Process
Data extraction of each study selected was performed using a standardized form containing information on the methodological characteristics of the studies, participants (number of participants, sex, and age), interventions (intensity—% of 1RM, number of sessions and exercises) and outcomes (1RM and muscle power assessment). This process was performed independently by two researchers (M.B-G. and E.B-R.). Eventual disagreements were resolved by consensus or by a third reviewer (E.L.C.). When the studies did not present the data required for meta-analysis, the corresponding author was contacted. When the data were unavailable, the manuscript was excluded from the study. For data presented only graphically, the results were extracted using DigitizeIt®.
The extracted outcomes were the absolute deltas of the values referring to 1RM and muscle power. When not available, the delta was calculated from the values obtained before and after the intervention, and the delta standard deviation was imputed by the equation proposed by Higgins and Green [30].
Risk of Bias Quality of Individual Studies
The risk of bias was assessed independently by two reviewers (M.B-G. and E.B-R.) using the PEDro scale based on the Delphi list, described by Verhagen et al. [31]. This procedure evaluates the risk of bias in the studies according to the following criteria: (1) eligibility criteria were specified; (2) participants were randomly allocated to groups; (3) allocation was concealed; (4) the groups were similar at baseline regarding the most important prognostic indicators; (5) there was blinding of all participants; (6) there was blinding of all therapists; (7) there was blinding of all assessors; (8) measures of at least one key outcome were obtained for more than 85% of the participants initially allocated to groups; (9) all participants for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one main outcome were analyzed by “intention to treat”; (10) the results of between-group statistical comparisons were reported for at least one main outcome; (11) the study provided both point measures and measures of variability for at least one main outcome. When these characteristics were described in the study, the criteria were considered met and the score was determined. Studies that did not describe these aspects did not score (Table 1). PEDro scores of 0–3 are considered “poor”, 4–5 “fair”, 6–8 “good”, and 9–10 “excellent” [32].
Data Synthesis and Analysis
Data analysis involved a meta-analysis comparing the effects of high-intensity power training (≥ 70%1RM) versus moderate (50–69% of 1RM) or low intensity (≤ 49%1RM) on the neuromuscular parameters of older individuals. The results are presented as standardized mean differences (SMD) for 1RM and maximal power output with 95% confidence intervals (CI). Calculations were performed using random effects models. The I2 inconsistency test was used to assess the statistical heterogeneity of treatment effects between studies, with values higher than 50% indicating high heterogeneity [31]. Values of α ≤ 0.05 were considered statistically significant.
To explore between-study heterogeneity further, we employed the “leave-one-out” strategy, where studies were removed individually from each meta-analysis. This exploratory procedure is recommended, particularly for meta-analyses with a limited number of studies [33]. We only considered analyses that included at least two studies in all comparisons.
We verified publication bias by visually inspecting the funnel plot for each analyzed variable. Asymmetry was tested using the Begg and Egger test, with significance set at p = 0.010. When publication bias was detected, we used the trim-and-fill test to estimate its effect on interpreting the results; however, when this was necessary the results were unchanged after the test. We performed all analyses using Stata version 15.1.
Results
Study Selection
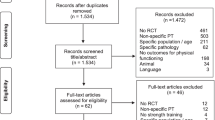
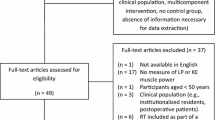
A search on the PubMed (Medline), LILACS, Embase and Scopus databases yielded a total of 7665 references, and an additional one study was identified through manual searches. After removing duplicates and reviewing titles, 7617 studies were excluded. Forty-eight articles were further examined by reading the abstracts, resulting in the exclusion of 46 articles. Upon a thorough reading of the two remaining studies and one additional study identified through manual searches, three studies met the inclusion criteria and were included in the quantitative analysis (see Fig. 1). While our study initially aimed to evaluate muscle power, maximal strength, and muscle hypertrophy, we found only one study that met the inclusion criteria for assessing muscle hypertrophy in older individuals [25]. Therefore, we were unable to conduct a meta-analysis for this outcome.

PRISMA 2020 flow diagram of included studies. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. https://doi.org/10.1136/bmj.n71
Study Characteristics
The general characteristics of selected studies are described in Table 2.
Description of the Participants
The three studies included in this meta-analysis assessed a total of 179 individuals, consisting of 71 men and 108 women. Participants' ages ranged from 63 to 83 years, and the sample sizes ranged from 43 to 84 participants [25,26,27]. All studies reported obtaining written informed consent from all participants before the start of the study, and all training sessions were supervised. The authors also reported a total of six exercise-related adverse events: one hamstring injury and back pain after a training session; and, a non-injurious fall outside of the laboratory after a training visit in study by Reid et al. [26]; three joint and musculoskeletal pain and one inguinal hernia in study by De Vos et al. [27]. These adverse events led to six withdrawals related to the training protocol: two in study by Reid et al. [26]; four in study by De Vos et al. [27]. Twenty six participants withdrew from the studies for reasons unrelated to the studies’ protocol [25,26,27].
Outcomes Assessment
Among the included studies, maximal strength was assessed by the 1RM test in the leg press and knee extension [25,26,27]. Concerning power output, both Reid et al. [26] and De Vos et al. [27] utilized pneumatic strength training equipment to assess peak power in the leg press and knee extension exercises. Rodriguez-Lopez et al. [25] utilized a linear position transducer and a force plate to assess peak power in the leg press exercise, and a custom-built rigid chair instrumented with a strain gauge to assess rate of force development in knee extension exercise.
Description of the Interventions
The studies by Rodriguez-Lopez et al. [25] and De Vos et al. [27] assessed a non-exercising control group; however, these control groups were not used in our analysis. Two studies conducted their interventions and assessments on lower-limbs exercises [25, 26], and one study combined both lower- and upper-limbs exercises [27].
Additional file 1: Tables S1 and S2 provide a summary of the study results, categorized by the assessed exercise (i.e., leg press and knee extension). All studies used fixed intensities throughout their interventions [25,26,27]. The intensities compared in the interventions were as follows: 20%, 50%, and 80% of 1RM [27], 40% and 80% of 1RM [25], and 40% and 70% of 1RM [26].
Two studies used equal volume (sets and repetitions) to compare the groups throughout the interventions: one prescribed three sets of 10 repetitions [26], and the other prescribed three sets of eight repetitions on the first training session (Tuesdays) and two sets of eight repetitions on the second session (Thursdays) of the week [27]. Rodriguez-Lopez et al. [25] prescribed different volumes (sets) for low- and high-intensity power training groups, but equal total volume (number of repetitions × external load relative to 1-RM): the low-intensity group performed six sets of twelve repetitions with a load equivalent to 40% 1-RM, while the high-intensity group performed six sets of six repetitions with a load equivalent to 80% 1-RM.
The weekly training frequency was 2 times a week in all included studies, while the intervention period ranged from 8 to 16 weeks. The total number of training sessions ranged from 16 to 32 across studies. All included articles evaluated 1RM on knee extension and leg press exercises before and after training [25,26,27], as well all studies assessed maximal power output on knee extension and leg press exercises [25,26,27].
Risk of Bias
Among the included studies, three (100%) specified their eligibility criteria and reported that participants were randomly allocated to groups and the groups were similar at baseline. Two articles (66.6%) blinded the participants, one (33.3%) blinded the assessors and none blinded the therapists (0%). In addition, all three studies (100%) obtained measures of at least one key outcome from more than 85% of the participants, performed treatment or control regarding allocation or intention to treat, compared between-group statistics, and presented point measures and measures of variability for at least one main outcome (Table 1).
Effects of Interventions
Table 3 presents a summary of the meta-analysis results. One of the studies we selected [27] compared three different power training intensities: low-intensity (20%1RM), moderate-intensity (50%1RM), and high-intensity (80%1RM). Therefore, for each exercise and outcome (maximal strength and power output), we conducted two separate analyses. One analysis compared low- versus high-intensity from the study by De Vos et al. [27], while the other analysis compared moderate- versus high-intensity from the same study, along with the other studies [25, 26].
The maximum strength data for leg press were assessed in three studies [25,26,27] and included 179 participants. There were no significant differences between low and high-intensity power training for leg press 1RM (Fig. 2), as well as there was no significant difference between low- to moderate-intensity and high-intensity power training for leg press 1RM (Additional file 1: Fig. S1). The maximum strength data for knee extension were assessed in two studies [26, 27] and included 136 participants. No significant difference was found between low- to moderate-intensity and high-intensity power training for knee extension 1RM (Additional file 1: Fig. S2). However, high-intensity power training was significantly associated with greater strength gains for knee extension 1RM compared to low-intensity (p = 0.008 [I2: 0.0%]) (Fig. 3).

Forest plot of the effects of low-intensity (20–40% of 1RM) power training versus high-intensity (70–80% of 1RM) power training on the maximum strength assessed by leg press 1RM. The squares and error bars signify the SMDs and 95% CI values; the diamonds represent the pooled estimates of random effects meta-analyses. SMDs standardized mean differences, CI confidence interval

Forest plot of the effects of low-intensity (20–40%% of 1RM) power training versus high-intensity (70–80% of 1RM) power training on the maximum strength assessed by knee extension exercise 1RM. The squares and error bars signify the SMDs and 95% CI values; the diamonds represent the pooled estimates of random effects meta-analyses. SMDs standardized mean differences, CI confidence interval
Regarding muscle power output, three studies that assessed leg press exercises were analyzed, comprising 179 participants [25,26,27]. There were no significant differences between low-intensity and low- to moderate-intensity compared to high-intensity power training on this outcome [p = 0.425 (I2: 0.0%); and, p = 0.693 (I2: 0.0%), respectively] (Fig. 4 and Additional file 1: Fig. S3, respectively). Regarding the knee extension exercise, two studies that assessed muscle power output were analyzed, comprising 136 participants [26, 27]. There were no significant differences between low-intensity and low- to moderate-intensity compared to high-intensity power training on this outcome [p = 0.932 (I2: 40.3%); and, p = 0.488 (I2: 0.0%), respectively] (Fig. 5 and Additional file 1: Fig. S4, respectively).

Forest plot of the effects of low-intensity (20–40% of 1RM) power training versus high-intensity (70–80% of 1RM) power training on the power output assessed in the leg press exercise. The squares and error bars signify the SMDs and 95% CI values; the diamonds represent the pooled estimates of random effects meta-analyses. SMDs standardized mean differences, CI confidence interval

Forest plot of the effects of low-intensity (20–40% of 1RM) power training versus high-intensity (70–80% of 1RM) power training on the power output assessed in the knee extension exercise. The squares and error bars signify the SMDs and 95% CI values; the diamonds represent the pooled estimates of random effects meta-analyses. SMDs standardized mean differences, CI confidence interval
Discussion
The purpose of this systematic review with meta-analysis was to summarize the evidence on the effects of low- to moderate-intensity versus high-intensity power training on maximal strength and power output in older adults. Unfortunately, due to the limited number of studies available, it was not possible to conduct a quantitative analysis of muscle hypertrophy. The main findings of the present review indicate that both low- to moderate-intensity (20–50% of 1RM) and high-intensity (70–80% of 1RM) power training induce similar gains in maximal power output. Additionally, the power training intensities analyzed induced comparable maximal strength gains in the leg press exercise, but higher intensities resulted in greater strength increases than low-intensity in the knee extension exercise.
All studies included in the present review found similar increases in maximal power output, regardless of the power training intensity [25,26,27]. In particular, the study by De Vos et al. [27] observed similar muscle power gains when comparing three different intensities (80% vs. 50% vs. 20% of 1RM). These findings are consistent with a systematic review by Straight et al. [34], which concluded that power training is an effective intervention for improving muscle power. In addition, in a previous systematic review with meta-analysis, Byrne et al. [35] have demonstrated the efficacy of different methods of power training interventions on muscle power gains. These results are important because muscle power is strongly associated with functional capacity, even more than maximal strength and muscle size [3, 34, 36, 37]. Muscle power also declines at a faster rate with age than maximal strength and muscle size [3, 20]. The gains induced by power training are associated with neural adaptations, such as increases in maximal motor unit recruitment capacity, maximal firing rate, and motor unit double discharges [19]. Nevertheless, no previous systematic review with meta-analysis has summarized the evidence on the effects of different intensities of power training on muscle function outcomes in older adults.
From a practical perspective, it is not necessary for older adults to exercise at high power training intensities (i.e., ≥ 70% of 1RM) to achieve gains in power output. Those who are not able to exercise at higher intensities due to clinical conditions, such as frail older adults and those with multiple comorbidities, may still achieve improvements by training at low- to moderate-intensities (20–50% of 1RM in the included studies). In fact, previous studies have demonstrated that low- to moderate-intensity training can promote several benefits, including muscle power gains in mobility-limited [26] and physically frail older individuals [12, 14, 16]. Furthermore, because training at higher intensities is associated with greater pain and discomfort post-exercise [38], training at lower intensities may reduce pain and discomfort, thus improving intervention adherence [39].
In our analysis of maximal strength gains (measured by 1RM) following power training, we found that higher intensities did not necessarily lead to greater gains in the leg press exercise. However, although there was no significant difference comparing low- to moderate-intensity (i.e., 40–50% of 1RM) versus high-intensity power training in the knee extension 1RM, we observed significant differences in strength gains for knee extension comparing low-intensity (20–40% of 1RM) versus high-intensity (SMD = 0.523), suggesting that the influence of relative intensity on maximal strength gains seems to be exercise-dependent.
Individual studies also showed significant improvements in maximal strength gains following different intensities [25, 27]. Rodriguez-Lopez et al. [25] found a significant difference in leg press 1RM between groups performing power training at 40% versus 80% of 1RM after 12 weeks. De Vos et al. [27] observed greater 1RM gains for several exercises (including knee extension) when training at 80% versus 20% of 1RM, while a significant difference in favor of high-intensity was observed only in the seated row exercise when comparing 80% versus 50% of 1RM.
Interestingly, our findings are consistent with those of traditional resistance training studies, in which greater maximal strength gains are observed when the intensity progresses up to 70–80% of 1RM [23, 24] for knee extension exercise. However, for the leg press exercise, we found that power training at intensities up to 50% of 1RM can be effective in promoting maximal strength gains. This finding has an interesting practical application, as the leg press exercise involves similar muscle groups to functional tasks like sit-to-stand and climbing stairs.
The reason for the different findings between exercises is not entirely clear, but one possible explanation is the characteristic of motor unit (MU) recruitment during power training. The threshold of muscle force at which MUs are recruited (i.e. recruitment threshold) is lower at high speed of muscle contraction [40], making it possible for type II MUs to be recruited even at low to moderate loading intensities. Since the recruitment of type II MUs is crucial for inducing maximal strength gains, this could explain the lack of difference in maximal strength gains between lower and higher intensities for the leg press exercise.
An important issue that needs to be mentioned is that, among the few studies included in our systematic review with meta-analysis, only one study used moderate intensity (i.e., 50% of 1RM), which is lower than the intensity used in several studies that have reported marked strength gains using this type of intervention (i.e., progressing to 60% of 1RM) [5, 7, 12, 14, 16]. Therefore, more studies are needed to compare low- versus high-intensities, and mainly moderate- versus high-intensities, and to assess the strength gains from different exercises to determine if low- to moderate-intensities are sufficient to optimize strength gains during power training.
Limitations and Strengths
This systematic review presents some limitations that should be acknowledged. The small number of included studies did not allow for sensitivity analyses. Furthermore, only one study analyzed the effects of different power training intensities in upper body exercises, and our results cannot be extrapolated to these exercises. Additionally, the included studies only assessed older participants without diseases that could directly interfere with outcome measures. Therefore, our findings cannot be extrapolated to older individuals with different clinical conditions (e.g., geriatric syndromes, musculoskeletal injuries, chronic conditions). It is important to note that the authors of the present systematic review were unable to control for these limitations.
However, it is worth noting that this review implemented a rigorous process that adhered to recommended practices in systematic reviews. This process included two independent researchers in all stages of study selection and data extraction. Additionally, the methodological quality of the included studies assessed by the PEDro scale was classified as “good” (i.e., low risk of bias). Moreover, to the best of our knowledge, this is the first systematic review with a meta-analysis assessing the effects of different power training intensities on neuromuscular adaptations in older adults.
Conclusions
In summary, power training performed at low-intensity (20–40% of 1RM), low-to-moderate intensity (40–50% of 1RM) and high-intensity (70–80% of 1RM) induces similar muscle power output gains in older adults. Additionally, these intensities also promote comparable maximal strength gains in the leg press exercise, but there is an advantage in favor of high-intensity compared to low-intensity power training in the knee extension exercise. These findings advance knowledge regarding the power training prescription, as they indicate that low- to moderate-intensity is a sufficient stimulus to promote marked improvements in mechanical muscle function in older adults. From a practical standpoint, considering the findings summarized by the present systematic review, exercise professionals dealing with power training prescription for older adults may optimize muscle power output gains as well as maximal strength from multi-joint lower-body exercises using low to moderate intensities (40–50% of 1RM), while higher intensities (70–80% 1RM) may be advantageous to develop maximal strength in single-joint lower-body exercise compared to low intensity power training (20–40% of 1RM). Nevertheless, considering the few studies were found in our search, further randomized clinical trials comparing different intensities of power training with different exercises should be designed to enhance the strength of the evidence.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PT:
-
Power training
- 1RM:
-
One-repetition maximum
- PROSPERO:
-
International prospective register of systematic reviews
- SMD:
-
Standardized mean differences
- CI:
-
Confidence interval
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- MU:
-
Motor unit
References
Fragala MS, et al. Resistance training for older adults. J Strength Cond. 2019;33:2019–52. https://doi.org/10.1519/jsc.0000000000003230.
Izquierdo M, et al. International exercise recommendations in older adults (ICFSR): expert consensus guidelines. J Nutr Health Aging. 2021;25:824–53. https://doi.org/10.1007/s12603-021-1665-8.
Radaelli R, et al. Power training prescription in older individuals: Is it safe and effective to promote neuromuscular functional improvements? Sports Med. 2022;53:569–76. https://doi.org/10.1007/s40279-022-01758-0.
Izquierdo M, et al. Effects of strength training on muscle power and serum hormones in middle-aged and older men. J Appl Physiol. 2001;90:1497–507. https://doi.org/10.1152/jappl.2001.90.4.1497.
Müller DC, et al. Adaptations in mechanical muscle function, muscle morphology, and aerobic power to high-intensity endurance training combined with either traditional or power strength training in older adults: a randomized clinical trial. Eur J Appl Physiol. 2020;120:1165–77. https://doi.org/10.1007/s00421-020-04355-z.
Müller DC, et al. Effects of high-intensity interval training combined with traditional strength or power training on functionality and physical fitness in healthy older men: a randomized controlled trial. Exp Gerontol. 2021;149:111321. https://doi.org/10.1016/j.exger.2021.111321.
Radaelli R, et al. Higher muscle power training volume is not determinant for the magnitude of neuromuscular improvements in elderly women. Exp Gerontol. 2018;110:15–22. https://doi.org/10.1016/j.exger.2018.04.015.
Ibanez J, et al. Twice-weekly progressive resistance training decreases abdominal fat and improves insulin sensitivity in older men with type 2 diabetes. Diabetes Care. 2005;28:662–7. https://doi.org/10.2337/diacare.28.3.662.
Botton CE, et al. Effects of resistance training on neuromuscular parameters in elderly with type 2 diabetes mellitus: a randomized clinical trial. Exp Gerontol. 2018;113:141–9. https://doi.org/10.1016/j.exger.2018.10.001.
Machado CLF, et al. Acute blood pressure response to high- and moderate-speed resistance exercise in older adults with hypertension. J Aging Phys Act. 2021;30:1–8. https://doi.org/10.1123/japa.2021-0214.
Pfeifer LO, et al. Effects of a power training program in the functional capacity, on body balance and lower limb muscle strength of elderly with type 2 diabetes mellitus. J Sports Med Phys Fit. 2021;61:1529–37. https://doi.org/10.23736/s0022-4707.21.11880-8.
Cadore EL, et al. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. Age (Dord). 2013;36:773–85. https://doi.org/10.1007/s11357-013-9586-z.
Cadore EL, et al. Strength and endurance training prescription in healthy and frail elderly. Aging Dis. 2014;5:183. https://doi.org/10.14336/ad.2014.0500183.
Izquierdo M, et al. Two-year follow-up of a multimodal intervention on functional capacity and muscle power in frail patients with type 2 diabetes. J Am Med Dir Assoc. 2021;22:1906–11. https://doi.org/10.1016/j.jamda.2021.06.022.
Sáez de Asteasu ML, et al. Inter-individual variability in response to exercise intervention or usual care in hospitalized older adults. J Cachexia Sarcopenia Muscle. 2019;10:1266–75. https://doi.org/10.1002/jcsm.12481.
Sáez de Asteasu ML, et al. Changes in muscle power after usual care or early structured exercise intervention in acutely hospitalized older adults. J Cachexia Sarcopenia Muscle. 2020;11:997–1006. https://doi.org/10.1002/jcsm.12564.
Reid KF, Fielding RA. Skeletal muscle power. Exerc Sport Sci Rev. 2012;40:4–12. https://doi.org/10.1097/jes.0b013e31823b5f13.
Casas-Herrero A, et al. Functional capacity, muscle fat infiltration, power output, and cognitive impairment in institutionalized frail oldest old. Rejuvenation Res. 2013;16:396–403. https://doi.org/10.1089/rej.2013.1438.
Aagaard P, et al. Role of the nervous system in sarcopenia and muscle atrophy with aging: strength training as a countermeasure. Scand J Med Sci Sports. 2010;20:49–64. https://doi.org/10.1111/j.1600-0838.2009.01084.xe.
McKinnon NB, et al. Neuromuscular contributions to the age-related reduction in muscle power: mechanisms and potential role of high velocity power training. Ageing Res Rev. 2017;35:147–54. https://doi.org/10.1016/j.arr.2016.09.003.
Ramírez-Campillo R, et al. Effects of plyometric training on endurance and explosive strength performance in competitive middle- and long-distance runners. J Strength Cond Res. 2014;28:97–104. https://doi.org/10.1519/jsc.0b013e3182a1f44c.
da Rosa Orssatto LB, et al. Effects of resistance training concentric velocity on older adults’ functional capacity: a systematic review and meta-analysis of randomised trials. Exp Gerontol. 2019;127:110731. https://doi.org/10.1016/j.exger.2019.110731.
Borde R, Hortobágyi T, Granacher U. Dose-response relationships of resistance training in healthy old adults: a systematic review and meta-analysis. Sports Med. 2015;45:1693–720. https://doi.org/10.1007/s40279-015-0385-9.
Csapo R, Alegre LM. Effects of resistance training with moderate vs heavy loads on muscle mass and strength in the elderly: a meta-analysis. Scand J Med Sci Sports. 2016;26:995–1006. https://doi.org/10.1111/sms.12536.
Rodriguez-Lopez C, et al. Neuromuscular adaptations after 12 weeks of light- vs. heavy-load power-oriented resistance training in older adults. Scand J Med Sci Sports. 2022;32:324–37. https://doi.org/10.1111/sms.14073.
Reid KF, et al. Comparative effects of light or heavy resistance power training for improving lower extremity power and physical performance in mobility-limited older adults. J Gerontol A Biol Sci Med Sci. 2014;70:374–80. https://doi.org/10.1093/gerona/glu156.
de Vos NJ, Singh NA, Ross DA, et al. Optimal load for increasing muscle power during explosive resistance training in older adults. J Gerontol A Biol Sci Med Sci. 2005;60:638–47. https://doi.org/10.1093/gerona/60.5.638.
Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ Br Med J. 2020;2021:372. https://doi.org/10.1136/bmj.n71.
Shamseer L, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. Brit Med J. 2015;349:g7647–g7647. https://doi.org/10.1136/bmj.g7647.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane handbook for systematic reviews of interventions version 6.3. Cochrane. 2022.
Verhagen AP, et al. The delphi list. J Clin Epidemiol. 1998;51:1235–41. https://doi.org/10.1016/s0895-4356(98)00131-0.
Cashin AG, McAuley JH. Clinimetrics: physiotherapy evidence database (PEDro) scale. J Physiother. 2020;66:59. https://doi.org/10.1016/j.jphys.2019.08.005.
Viechtbauer W, Cheung MW. Outlier and influence diagnostics for meta-analysis. Res Synth Methods. 2010;1:112–25. https://doi.org/10.1002/jrsm.11.
Straight CR, et al. Effects of resistance training on lower-extremity muscle power in middle-aged and older adults: a systematic review and meta-analysis of randomized controlled trials. Sports Med. 2016;46:353–64. https://doi.org/10.1007/s40279-015-0418-4.
Byrne C, et al. Ageing, muscle power and physical function: a systematic review and implications for pragmatic training interventions. Sports Med. 2016;46:1311–32. https://doi.org/10.1007/s40279-016-0489-x.
Foldvari M, et al. Association of muscle power with functional status in community-dwelling elderly women. J Gerontol A Biol Sci Med Sci. 2000;55:M192–9. https://doi.org/10.1093/gerona/55.4.m192.
Marsh AP, et al. Lower extremity muscle function after strength or power training in older adults. J Aging Phys Act. 2009;17:416–43. https://doi.org/10.1123/japa.17.4.416.
MacIntyre DL, Reid WD, McKenzie DC. Delayed muscle soreness. Sports Med. 1995;20:24–40. https://doi.org/10.2165/00007256-199520010-00003.
Collado-Mateo D, et al. Key factors associated with adherence to physical exercise in patients with chronic diseases and older adults: an umbrella review. Int J Environ Res Public Health. 2021;18:2023. https://doi.org/10.3390/ijerph18042023.
Duchateau J, Enoka RM. Human motor unit recordings: origins and insight into the integrated motor system. Brain Res. 2011;1409:42–61. https://doi.org/10.1016/j.brainres.2011.06.011.
Acknowledgements
The authors thank the National Council for Scientific and Technological Development (CNPq, Brazil), Coordination for the Improvement of Higher Education Personnel (CAPES, Brazil) and Foundation for Research Support of the State of Rio Grande do Sul (FAPERGS) for their support.
Standards of Reporting
The present study following the recommendations of PRISMA for Systematic reviews and meta-analyses.
Funding
The authors declare they did not receive any funding for the publication of this manuscript.
Author information
Authors and Affiliations
Contributions
MB-G had the idea for the article, defined the PICOT strategy, made the literature search, data extraction and analyses, and had a major contribution in the original draft of the manuscript. ELC had the idea for the article, defined the PICOT strategy, and had a major contribution in the original draft of the manuscript. EB-R had the idea for the article, defined the PICOT strategy, made the literature search, data extraction and analyses, and contributed to the original draft of the manuscript. AFV defined the PICOT strategy, analysed the data, and contributed in the original draft of the manuscript. MLSdeA contributed to the idea of the article, defined the PICOT strategy, and had a major contribution in the original draft of the manuscript. RSP contributed to the idea of the article, defined the PICOT strategy, and contributed in the original draft of the manuscript. MI contributed to the idea of the article, defined the PICOT strategy, and had a major contribution in the original draft of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate:
Not applicable.
Consent for Publication
Not applicable.
Competing interests
The authors declare that they have no competing interests with the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search strategy, additional table and figures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bandeira-Guimarães, M., Blanco-Rambo, E., Vieira, A.F. et al. Chronic Effects of Different Intensities of Power Training on Neuromuscular Parameters in Older People: A Systematic Review with Meta-analysis. Sports Med - Open 9, 98 (2023). https://doi.org/10.1186/s40798-023-00646-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-023-00646-9