
Abstract
Background
Different field tests are used to evaluate muscle capacity, in particular maximal voluntary isometric endurance. However, although there are some normative values for a few muscle endurance tests, these do not consider the weight, height, gender, or age of individuals, which are well-known factors that influence muscle performance.
Hypothesis/Purpose
The purpose of this study was to investigate the test–retest reproducibility of eight field tests and establish muscle endurance norms, in a healthy population, based on their anthropometric characteristics, which could allow the optimal evaluation of the entire muscle function in a quick manner.
Design
Case series.
Methods
This study was conducted in two phases. The first phase was to check the reproducibility inter- and intra-assessor for eight isometric muscle field tests on 20 volunteer subjects aged 40.9 ± 11.6 years old (age range, 21–58 years). The second part was to establish muscle maximal voluntary isometric endurance norms according to these tests on a total of 400 healthy participants grouped by age (50 males and females in each of the age brackets, 20–29; 30–39; 40–49; 50–59 years old, for a total of 200 males and 200 females).
Results
The intra- and inter-assessor reproducibility tests are good for all muscle measurements (the intraclass correlation coefficients varied between 0.915 and 0.996 and the coefficient of variation between 3.6 and 11.8%). The area under the receiver operating characteristic curves demonstrates a good sensibility with values greater than 0.7 for each test. Each muscle belt presents same ratio regardless of the age and gender group. The simultaneous multiple regression analyses highlight that the anthropometric characteristics of subjects influence significantly the performance of isometric tests.
Conclusion
This study has permitted establishing prediction equations in a healthy population according to their anthropometric characteristics as well as agonist/antagonist ratios for eight muscle isometric field tests after demonstrating a good reproducibility of all tests.
Similar content being viewed by others

Key Points
-
Predictive equations to establish muscle maximal voluntary isometric endurance present a good reproducibility for all muscle groups.
-
These equations are useful in the field of prevention and/or rehabilitation (risk of falling, low back pain, etc.) or sport (muscle injury risks).
Introduction
The assessment of muscle performance is a requirement in many fields such as prevention [1], sport [2], or rehabilitation [3], as the results of this assessment are used to prevent muscle injuries, guide and individualize training programs. Thus, the knowledge of reference values is a necessity to achieve the above goals. Muscle performance can be measured by different dynamometers, such as the isokinetic dynamometers [4], or the manual dynamometers [5]. Although the use of the isokinetic dynamometers is considered as the gold standard instrument to evaluate muscle strength [6], these devices remain very expensive, bulky, and require trained personnel to handle them and interpret the results. On the other hand, to measure muscle strength, the manual dynamometers present a good alternative, with a good reproducibility for the assessment of the upper and lower limbs [7, 8]. However, this reproducibility depends on the model of dynamometers used during the assessment [9]. In addition, although many authors propose reference values according to anthropometric data [5, 7, 10], these reference values depend on the model of the manual dynamometer and the calibration of the instrument [9]. So, the use of manual dynamometers remains limited as the comparison of the results between models is complicated.
Another way to simply evaluate muscle performance is by using field tests, which allows measuring maximal voluntary isometric endurance. In the literature, many field tests evaluating maximal voluntary isometric endurance have been validated, but, although some normative values exist for some muscle endurances tests [11, 12], these norms do not consider the weight, height, gender, and age of individuals. However, all these anthropometric data are well-known factors that positively or negatively influence muscle performance [13]. In addition, the postural position of some field tests often induces discomfort or pain [14] leading to an underestimation of muscle capacity because the test may be stopped prematurely. Therefore, it seems important to modify the postural positions of the subjects during field tests in order to decrease the limiting factors and to consider the anthropometric data of each subject while respecting the validity of the tests. Finally, the evaluation encountered in the literature on maximal voluntary isometric muscle endurance using isometric contractions is generally limited to four muscle groups: quadriceps, abdominals, lumbar, and quadratus lumborum muscles [12, 15]. Therefore, this assessment provides a somewhat limited overview of the muscle performance.
Another variable which must be taken into account in the evaluation of muscle performance is muscle imbalance or the agonist/antagonist muscle ratios. Indeed, in the case of muscle imbalance, a joint disorder and/or pain can result because the stabilization of the joint is no longer ensured [16]. With the knowledge of the muscle deficits, it is possible to propose an individualized training program that can restore a normal ratio [16]. Generally, to obtain the values of the muscle ratios, it is necessary to measure the strength of the agonist and antagonist muscles and then calculate their ratios. The most widely used method is the isokinetic method, but with the limitations of its use explained previously. McGill et al. (1999) have proposed an easier methodology than the isokinetic method, to determine the ratios in a healthy young adult population, using the endurance time of field tests [17]. However, in their study, muscle ratios were limited to three muscle groups, namely, the abdominals, lumbar, and quadratus lumborum muscles. In addition, all muscle ratios were determined from the performance of the lumbar muscles. Therefore, it is not possible to detect the specific imbalance in relationship with its joint and this form of assessment remains marginal. In addition, as highlighted by the authors, their ratios were established from a young population, which might not be applicable to an older population.
Therefore, we first hypothesize that it would be possible to validate field tests of maximal voluntary isometric muscle endurance with adaptive postural positions to best measure muscle performance; secondly, we hypothesize that the anthropometric data of the subjects could influence the maximal voluntary isometric muscle performance.
The objectives of this study were (1) to validate eight field tests of maximal voluntary isometric muscle endurance with adaptive postural positions; (2) to establish predictive equations of the entire muscle performance in a healthy population based on its anthropometric characteristics, which could allow the prevention of muscle injuries and/or to optimize the individualization of training programs in a quick and cheap manner.
Materials and Methods
Study Design
This study was conducted in two phases. The first phase was to check the inter- and intra-assessor reproducibility for isometric muscle field tests, and the second part was to establish muscle maximal voluntary isometric endurance norms according to these tests. The isometric tests allow assessment of the trunk flexor, trunk extensor, quadratus lumborum, quadriceps, hamstring, and back and chest muscles (Fig. 1).

Figures illustrating the measurement muscle isometric endurance. (A) Trunk flexors, (B) trunk extensors, (C) quadratus lumborum muscles, (D) quadriceps muscles, (E) hamstrings muscles, (F) back muscles, and (G) chest muscles
To be included in the study, the selection criteria for the two phases were as follows: no history of chronic or acute disease; a score < 9 on the Baecke questionnaire, which does not correspond to a sporting way of life [18]; no psychiatric or psychological disorders; and no contraindication for exercise.
Before being included in the study, the design, rules, and protocol were explained to each subject as required by the Declaration of Helsinki. Then each subject signed a written consent form. The study protocol was approved by the Behavioral Science Ethics Committee of University of Lille under No. 2019-380-S77.
Part 1: Reproducibility of Muscle Maximal Voluntary Isometric Endurance Field Tests
The aim of this first part of the study was to examine intra- and inter-assessor reproducibility in a test–retest during isometric field tests in order to assess the maximal voluntary isometric endurance of the quadriceps, hamstring, abdominal, trunk extensor, right and left quadratus lumborum, and back and chest muscles (Fig. 1).
Subjects
Twenty subjects (9 males, 11 females), with a mean age of 40.9 ± 11.6 years (mean ± SD), were included (Table 1). Subjects completed the Baecke questionnaire [18] to determine their physical activity level and were asked about any history of medical conditions in order to verify the entry/exclusion criteria.
Protocol
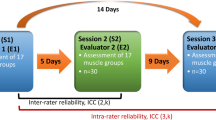
Two assessors, A and B, each performed two evaluation sessions (A1 and A2 for assessor A and B1 and B2 for assessor B). In order to avoid habituation effect, data from A- and B-rater were collected randomly. Prior to data collection, the assessors practised using the test protocols to ensure that standardized procedures were employed.
Each evaluation session lasted for 2 weeks with a break of at least 24 h between each one. This 24-h interval was chosen in order to avoid the impact of fatigue resulting from two sessions being too close together [19, 20]. Only the data of the last three evaluation sessions (A2, B1, and B2) were analyzed, with the first session (A1) serving as a familiarization and therefore the results of this session were not considered in the analysis of the data.
No attempt was made to standardize the order in which, or the time of day when, the evaluations were completed. Measurements from the two assessors were recorded on separate data collection forms to ensure that they were blinded to each other’s results and their own previous results. Both assessors carried out two assessment sessions for each subject and applied each field test in random order. The randomization was performed with the R software by assigning a number to each test. During the assessment, the antagonist muscle was tested after the agonist muscle. Prior to the assessment of each test, the assessors explained and demonstrated the test procedure to the subject.
Each assessment session started with 10 min of cardiorespiratory warm-up on a cycloergometer at 65% of the target heart rate, as determined by the Karvonen formula [21], and subjects benefited from at least 5-min rest between each test.
Guidelines for Postures During the Tests
For this study, the objective was to reduce pain generated by the discomfort of the position tests during the evaluation. To do this, the postural position of some tests was modified (Fig. 1). These modifications and all instructions for all tests, including pretest cueing, starting position, subject instructions, and termination criteria, are presented in the Additional file 1: Appendix. Next, there followed a brief presentation of the used tests with their alterations or not: (1) trunk flexor muscles were evaluated with the test of Ito et al. [14]. Some modifications were carried out, including the position of the legs and the termination criteria; (2) trunk extension was evaluated using the test of Ito et al. [14] without modification; (3) right and left quadratus lumborum muscles were evaluated using a modification of the positions in McGill et al.’s tests [17]. The modification was the position of the legs; (4) the isometric test of quadriceps using the original Killy test described by Bernard et al. [22] was used; (5) for the hamstring muscles test, a derivative of the bridge exercise to the neutral spine alignment position described by Youdas et al. [23] was used. These modifications included the pelvis position and the feet position; (6) the back muscles test was an adaptation of the behind-the-neck lat pull-down described by Sperandei et al. [24]. This test required the same movement as the behind-the-neck lat pull-down but the subject sat on the floor, with their back, shoulders, elbows, hands, and head against the wall. In addition, this test was carried out without equipment and in an isometric way; (7) for the chest muscles test, a derivative of the push-up on the knees exercise described by Vossen et al. [25] was used. In our study, this test was performed in an isometric way, so the termination criteria were not the same.
Participants were individually instructed and supervised by experienced therapists specifically trained in the testing methodology. In each of these tests, the weight represented the load.
Part 2: Creation of Muscle Norms
Subjects
Four hundred healthy Caucasian participants segmented by age (50 males and 50 females in each age bracket, 20–29 years old; 30–39 years old; 40–49 years old; and 50–59 years old; a total of 200 males and 200 females) were included. The female group was aged 39.7 ± 11.5 years and the male group was aged 39.4 ± 11.4 years (Table 1).
Protocol
Prior to isometrics testing, participants performed 10 min of warm-up, including all articulations of the body. After that, all subjects performed the eight maximal voluntary isometric muscle endurance tests. Each test was carried out once per session. Tests were conducted in random order with at least 5-min rest between two tests. As for the first part, randomization was performed using the R software by assigning a number to each test. The antagonist muscles were systematically tested after the agonist muscles.
Prior to the performance of each test, the assessor explained and demonstrated the test to subjects using standardized instructions. For this part, the same researcher conducted all the tests.
Instructions for End of Tests Parts 1 and 2
For all endurance tests, in both parts 1 and 2, subjects were encouraged to hold the test position until exhaustion, and were given feedback if they deviated from the position. Tests were terminated when the subject could not maintain the position or if there were any obvious signs of fatigue (not maintaining the position in spite of verbal feedback, for example) or a significant emergence of pain or other symptoms. The maximum holding time was recorded in seconds using a stopwatch. The stopwatch was triggered when the subject was in the right position.
Statistical Analysis
Intra- and Inter-assessor Reproducibility
Intra- and inter-assessor reproducibility was estimated using intraclass correlation coefficients (ICCs). The intra-assessor reproducibility was quantified by calculating the ICC between the measurement conducted by the same assessor “B1” and “B2.” The inter-assessor reproducibility was measured by calculating the ICC between the measurement of assessor A (“A2”) and assessor B (“B1” and “B2”). For each ICC, error range and repeatability were calculated with standard error of the measurement (SEM), 95% confidence intervals (CIs), and 95% limits of agreement (LOAs). The standard error of the measurement (SEM) was calculated according to the formula SEM = SD √(1-ICC) [26], to provide an estimate of the precision of measurement, expressed in the units of the measure. The SEM was divided by the mean of the two measurements and multiplied by 100 to give a percentage value (SEM%) [27]. A percentage of 95% of LOA demonstrates the range of measurement error within the sample [28]. The interpretation of the ICCs was obtained according to the study by Shrout: reproducibility was considered strong if the ICC was between 1 and 0.81, moderate between 0.80 and 0.61, fair between 0.60 and 0.41, low between 0.40 and 0.11, and non-reproducible if less than 0.10 [29].
In order to determine the absolute reproducibility, the coefficient of variation (CV) was calculated. The CV is expressed as a percentage (CV%) and is calculated by dividing the standard deviation by the mean, multiplied by 100, for each test. The CV values of 10% [30] and 15% [31] have been used to consider the level of absolute reproducibility of the measurement (CV < 15% = good reproducibility; CV < 10% = excellent reproducibility).
The Breusch-Pagan test was used to verify the heteroscedasticity in the regression model. The heteroscedasticity of the model was confirmed when p value < 0.05 [32]. The performances in all isometric tests for each session of evaluation were expressed as mean ± standard deviation (mean ± SD). Statistical analysis was performed using the SPSS version 20.0 software and the Breusch-Pagan test was performed using the R software version 4.0.4.
Muscle Norms
A sample size of 34 participants per group was needed to detect a 10% difference (power of 0.9 and p < 0.05) according to the results of the studies by Claxton et al. (2009) [11] and Evans et al. (2007) [12]. However, the present data were part of a larger study in which more variables were assessed, which required a larger sample size. So, 400 subjects were included in this study.
The sensitivity of all tests was determined by a receiver operating characteristic (ROC) analysis, as a function of the age brackets 20–29 years and 50–59 years for male and female groups. The area under the ROC curve (AUC) is widely used to estimate the predictive accuracy of distributional models derived from presence/absence data [33]. The relationship between AUC and the sensitivity was considered excellent between 1 and 0.9, very good between 0.9 and 0.8, good between 0.8 and 0.7, average between 0.7 and 0.6, and poor between 0.6 and 0.5 [34].
The gender influence was evaluated by one-way ANOVA. To establish the norms for the eight muscle field tests, multiple regression analyses were conducted to determine the influence of the anthropometric data (age, weight, and height) on the performance of isometric tests. All values were expressed as mean ± standard deviation (mean ± SD). For the gender parameter, data normality was tested using the Shapiro–Wilk test. The significance level was set at the 0.05 level. The statistical analyses were performed using the R software version 3.5.0.
Results
Anthropometric characteristics of all subjects included in this study and the overall means of the last three assessments “A2,” “B1,” and “B2” for all the isometric tests are presented in Table 1.
Part 1: Reproducibility of Muscle Endurance Tests
Table 2 presents the results of the intra-assessor (“B1” and “B2”) reproducibility tests for all muscle measurements. The ICC values of the muscle endurance measurements vary between 0.946 and 0.989, thereby indicating excellent reproducibility. The bias values range from −3.9 to 1.0, staying close to zero and indicating a slight systematic improvement between measurements.
Tables 3 and 4 present the results of the inter-assessor (between assessments of “B1” and “A2” and between assessments of “B2” and “A2”) reproducibility tests for all muscle measurements. The ICC values indicate excellent inter-assessor reproducibility, with measurements varying between 0.915 and 0.996 for the measures of “B1” and “A2” assessments and between 0.955 and 0.996 for the measures of “B2” and “A2” assessments. For inter-assessor comparison, the bias values are negative (ranging from −5.6 to −0.8 for the measurement between “B1” and “A2” and from −4.9 to −0.6 for the measurement between “B2” and “A2”), indicating a slight systematic improvement between measurements.
Regarding the absolute reproducibility, the CV values vary between 3.6 and 11.8% (Tables 2, 3, 4). The intra-assessor (Table 2) absolute reproducibility is between good and excellent reproducibility for all tests (minimum measurement, 6.6% for the hamstring test; maximum measurement, 11.3% for the right quadratus lumborum test). The absolute reproducibility of inter-assessors (Tables 3 and 4) is also between good and excellent for all tests (minimum measurement, 3.6% for the hamstring test between “B2” and “A2;” maximum measurement, 11.8% for the chest muscle test between “B1” and “A2”).
With regard to absolute reproducibility, the values of SEM% demonstrate a good reproducibility of the accuracy and precision of the measured values. Indeed, the SEM values of intra- or inter-assessor measurements are less than 10% of the average measured value, so the measurement errors are small, and therefore the measurement is reliable [35].
The Breusch-Pagan p values for all tests are greater than 0.05 (the lowest value, BP = 3.6, df = 1, p value = 0.07 for the chest muscle tests between “B1” and “A2”); thus, the null hypotheses is accepted, i.e., the data are homoscedastic.
The intra-assessor and inter-assessor coefficient of variation (CV) was also used to measure the absolute reproducibility of agonist/antagonist ratios (Table 5). Muscle ratios were determined by dividing the holding time of the anterior chain muscles by the holding times of the posterior chain muscles for all muscle belts. For each muscle belt, the CV values vary between 5.8 and 12.9%, corresponding to between good to excellent reproducibility for all agonist/antagonist ratios.
Part 2: Muscle Norms
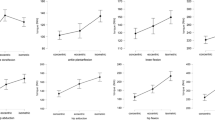
The ROC curves are presented in Fig. 2. The AUC demonstrates a good sensibility according to age brackets with values greater than 0.7 for each test (Tables 6 and 7).

ROC curves for all tests as a function of the age brackets. (A) Male group; (B) female group
For the male and female groups, the average hold time for each test is presented in Table 1. Each test carried out was stopped following muscle fatigue by the participant themself or by the assessor when the participant showed obvious signs of fatigue (maintaining of the initial position was impossible). No test was stopped following an emergence of pain or other symptoms.
Prediction equations to estimate muscle performance according to anthropometric criteria are presented in Tables 8 and 9. The muscle ratios of each muscle belt present no significant difference between men and women and no difference according to age bracket (Table 10).
Discussion
Our results have demonstrated the reproducibility of eight field tests to measure the maximal voluntary isometric muscle endurance with adapted postural positions and they have enabled the creation of predictive equations to calculate maximal theoretical voluntary isometric muscle endurance in a healthy population based on its anthropometric characteristics (age, weight, height, and gender).
The objective of the first phase of this study was to evaluate the relative and absolute reproducibility as well as the sensibility of muscle tests with modified postures for a healthy adult population, insofar as Ito et al. demonstrated that the original postures could induce pain or hyperlordosis [14]. Our results showed that all maximal voluntary isometric endurance tests present good levels of reproducibility. Indeed, for each test, the ICC was greater than 0.9, the CV less than 12% and the SEM less than 6%. The SEM of our tests was similar or lower to those found in the literature on other field tests [12, 36]. Our ICC values were higher than those obtained in other studies [12, 14, 17], but this is classic in studies using field tests to obtain an ICC > 0.81 [36, 12, 14]. The between-subject variability makes it difficult to compare the ICC between studies [26]. However, the higher ICC values in our study could be due to the fact that the population used for the reproducibility was heterogeneous, including both males and females of different ages. Nevertheless, the good to excellent absolute intra- and inter-assessor reproducibility measured by the coefficient of variation confirms our good level of reproducibility.
The sensitivity was measured by established and by analyzing for each test, whether the muscle performance is dependent on the age of the subjects. Our results showed that the observed values of the area under the ROC curves were greater than 0.7, demonstrating an influence of age on the muscle performance, which indicates young adults must have higher voluntary maximal isometric endurance than older adults. It is generally recognized that muscle endurance and strength decrease with aging [37, 38] and our study results on age-specific muscle maximal voluntary isometric endurance support the validity of our model.
The objective of the second phase of this study was to determine predictive equations of the muscle performance, taking into account the anthropometric criteria of the subjects. In the literature, the maximal voluntary isometric muscle endurance performance of field tests is often analyzed between gender and age, while height and weight are little discussed. Among all the anthropometric criteria, only the influence of age has been well established [11, 39] because of the well-known decline in muscle mass and muscle quality [40]. It is also accepted that an increase in weight has a negative influence on the performance of maximal voluntary isometric muscle endurance, but this variable is not discussed in the studies by Strand et al. and Latikka et al., which used isometric fields tests because the authors argued a weak relationship between weight and holding time during the isometric test [41, 39]. The influence of the other anthropometric criteria—gender and height—is still debated. Let us take the factor gender: one study demonstrated an absence of influence of gender on the muscle performance certain isometric tests [12], whereas other studies highlighted the effect of gender in favor of males [17, 41], or, conversely, in favor of females [42]. One hypothesis which could explain the sex-specific difference could be a difference in the muscle fiber-type distribution, muscle fiber cross-sectional area, capillary supply, oxidative and glycolytic capacity, citrate synthase, 3-hydroxyacyl-CoA-dehydrogenase, and lactate-dehydrogenase enzyme activities between men and women, but an absence of difference of these criteria between non-active adult men and women has been demonstrated [43]. With current knowledge, it is still impossible to generalize regarding the influence of gender on maximal voluntary isometric muscle endurance performance. With regard to the height factor, the literature demonstrates its influence on the holding time [39, 41], but the results of the studies are contradictory: either the holding time is better [39] or it is reduced [41] in maximal voluntary isometric muscle endurance measured with field tests. These differences could be explained by a different methodology, including athletic and non-athletic subjects [41], a group composed only of males with different age [39], or even a small number of subjects [12, 17]. In our study, the number of subjects used to analyze the influence of anthropometric parameters on the muscle performance was higher and more level-headed than the literature studies [12, 14, 17], and the profile used was the same for each group, namely, non-athletic Caucasian healthy adult subjects. Thus, our findings support that height, weight, and age are determining factors in predicting performance of maximal voluntary isometric endurance tests, unlike gender, which does not influence the performance.
Two limitations would be considered for the interpretation of these data. Our study was carried out in a French Caucasian population; thus, as explained by Hogrel et al. (2007) [44], our results could present a few variations depending on the race of the subjects (African, Asian) because of morphologic, anatomic, and cultural differences. In addition, the age bracket of the participants included in this study was from 20 to 59 years old. Thus, our predictive equations and the muscle agonist/antagonist ratios may be not be adapted for subjects who are younger or older than our participants.
Conclusion
Our study has permitted the validation of the reproducibility of field tests and the creation of predictive equations to calculate maximal voluntary isometric muscle endurance in a healthy population according to its anthropometric characteristics, namely, age, weight, height, and gender. The creation of these normative values responds to the need to be able to assess muscle function to identify weakness or muscle imbalance in order to establish personalized training programs in the fields of prevention, sport, or rehabilitation [45].
Practical Applications
These normative equations permit the determination of the weakness of a muscle, a muscle group, or a muscle imbalance according to the anthropometric data of the subject. The assessor simply has to complete the prediction equations with the anthropometric data of the subject (Tables 8 and 9) to obtain the theoretical value which would need to be reached at the target test. If the result is below the maximum theoretical value or if a muscle imbalance exists, physical activity management is required in the field of prevention and/or rehabilitation (risk of falling, difficulty climbing stairs, low back pain, etc.) or sport (muscle injuries risks). In addition, the predictive equations can be integrated into software or a mobile application to allow subjects to self-evaluate and benefit from an individualized program from a distance.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ICC:
-
Intraclass correlation coefficient
- SEM:
-
Standard error of the measurement
- CI:
-
Confidence interval
- LOA:
-
Limit of agreement
- SEM%:
-
Percentage of standard error of the measurement
- CV:
-
Coefficient of variation
- CV%:
-
Percentage of coefficient of variation
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curve
References
Bennie JA, Lee DC, Khan A, Wiesner GH, Bauman AE, Stamatakis E, et al. Muscle-strengthening Exercise among 387,423 U.S. Adults: Prevalence, Correlates, and Associations with Health Conditions. Am J Prev Med. 2018;55(6):864–74.
Lacome M, Avrillon S, Cholley Y, Simpson B, Guilhem G, Buchheit M. Hamstring Eccentric Strengthening Program: Does Training Volume Matter? Int J Sports Physiol Perform. 2020;15(1):81–90.
Mostagi FQ, Dias JM, Pereira LM, Obara K, Mazuquin BF, Silva MF, et al. Pilates Versus General Exercise Effectiveness on Pain and Functionality in Non-specific Chronic Low Back Pain Subjects. J Bodyw Mov Ther. 2015;19(4):636–45.
Zapparoli FY, Riberto M. Isokinetic Evaluation of the Hip Flexor and Extensor Muscles: a Systematic Review. J Sport Rehabil. 2017;26(6):556–66.
Alvarenga G, Kiyomoto HD, Martinez EC, Polesello G, Alves VLDS. Normative Isometric Hip Muscle Force Values Assessed by a Manual Dynamometer. Acta Ortop Bras. 2019;27(2):124–8.
Stark T, Walker B, Phillips JK, Fejer R, Beck R. Hand-held Dynamometry Correlation with the Gold Standard Isokinetic Dynamometry: a Systematic Review. PM&R. 2011;3(5):472–9.
Andrews WA, Thomas MW, Bohannon RW. Normative Values for Isometric Muscle Force Measurements Obtained with Hand-held Dynamometers. Phys Ther. 1996;76(3):248–59.
Pasco JA, Stuart AL, Holloway-Kew KL, Tembo M, Sui SX, Anderson KB, et al. Lower-limb Muscle Strength: Normative Data from an Observational Population-based Study. BMC Musculoskelet Disord. 2020;21(1):89.
Amaral JF, Mancini M, Novos Jùnior JM. Comparison of Three Hand Dynamometers in Relation to the Accuracy and Precision of the Measurements. Rev Bras Fisioter. 2012;16(3):216–24.
Luna-Heredia E, Martin-Peña G, Ruiz-Galiana J. Handgrip Dynamometry in Healthy Adults. Clin Nutr. 2005;24:250–8.
Claxton M, McIntosh G. Sidebridge Muscle Endurance Testing: Normative Data for Adults. Ortho Division Rev. 2009:35–9.
Evans K, Refshauge KM, Adams R. Trunk Muscle Endurance Tests: Reliability, and Gender Differences in Athletes. J Sci Med Sport. 2007;10:447–55.
Samson MM, Meeuwsen IBAE, Crowe A, Dessens JAG, Duursma SA, Verhaar HJJ. Relationships Between Physical Performance Measures, Age, Height and Body Weight in Healthy Adults. Age Ageing. 2000;29(3):235–42.
Ito T, Shirado O, Suzuki H, Takahashi M, Kaneda K, Strax TE. Lumbar Trunk Muscle Endurance Testing: an Inexpensive Alternative to a Machine for Evaluation. Arch Phys Rehabil. 1996;77(1):75–9.
Demoulin C, Fauconnier C, Vanderthommen M, Henrotin Y. Recommendations for a Basic Functional Assessment of Low Back Pain. Rev Med Liège. 2005;60:661–8.
Padasala M, Joksimovic M, Bruno C, Melino D, Manzi V. Muscle injuries in athletes. The relationship between H/Q ratio (hamstring/quadriceps ratio). Ita J Sports Reh Po. 2020;7(1):1478–98.
McGill S, Childs A, Liebenson C. Endurance Times for Low Back Stabilization Exercises: Clinical Targets for Testing and Training from a Normal Database. Arch Phys Med Rehabil. 1999;80:941–4.
Bigard A, Duforez F, Portero P, Guezennec C. Assessment of Physical Activity by Questionnaire: Validity of the Baecke Questionnaire. Sci Sports. 1992;7:215–21.
Birmingham TB. Test-retest Reliability of Lower Extremity Functional Instability Measures. Clin J Sport Med. 2000;10(4):264–8.
Loss JF, Neto ESW, de Siqueira TB, Winck AD, de Moura LS, Gertz LC. Portable, One-dimensional, Trunk-flexor Muscle Strength Measurement System. J Sport rehabil. 2020;29(6):851–4.
Karvonen M, Kentala E, Mustala O. The Effects of Training Heart Rate: a Longitudinal Study. Ann Med Exp Biol Fenn. 1957;35:307–15.
Bernard J, et al. Muscle Assessment in Healthy Teenagers Comparison with Teenagers with Low Back Pain. Ann Readapt Med Phys. 2008;51:274–83.
Youdas J, et al. Magnitudes of Muscle Activation of Spine Stabilizers, Gluteals, and Hamstrings During Supine Bridge to Neutral Position. Physiother Theory Pract. 2015;31:418–27.
Sperandei S, Barros M, Silveira-Junior P, Oliviera C. Electromyographic Analysis of Three Different Types of Lat Pull-down. J Strength Cond Res. 2009;23:2033–8.
Vossen J, Kramer J, Burke D, Vossen D. Comparison of Dynamic Push-up Training and Plyometric Push-up Training on Upper-body Power and Strength. J Strength Cond Res. 2000;14:248–53.
Weir J. Quantifying Test-retest Reliability Using the Intra Class Correlation Coefficient and the SEM. J Strength Cond Res. 2005;19:307–10.
Svensson E, Waling K, Hager-Ross C. Grip Strength in Children: Test-retest Reliability Using Grippit. Acta Paediatr. 2008;97:1226–31.
Bland J, Altman D. Statistical Methods for Assessing Agreement Between Two Method of Clinical Measurement. Lancet. 1986;1:307–10.
Shrout P. Measurement Reliability and Agreement in Psychiatry. Stat Methods Med Res. 1998;7:301–17.
Stockes M. Reliability and Repeatability of Methods for Measuring Muscle in Physiotherapy. Physiotherapy Practice. 1985;1:71–6.
Carnet AS, Bateman ND, Jones NS. Reliable and Reproducible Anterior Active Rhinomanometry for the Assessment of Unilateral Nasal Resistance. Clin Otolaryngol. 2000;25:499–503.
Breusch TS, Pagan AR. A Simple Test for Heteroscedasticity and Random Coefficient Variation. Econometrica: J Econometric Soc. 1979:1287–94.
Cohen J. A Coefficient of Agreement for Nominal Scales. Educ Psychol Meas. 1960;20(1):37–46.
Yesilnacar, E. K. (2005). The Application of Computational Intelligence to Landslide Susceptibility Mapping in Turkey. University of Melbourne, Department, 200.
Liaw L, et al. The Relative and Absolute Reliability of Two Balance Performance Measures in Chronic Stroke Patients. Disabil Rehabil. 2008;30:656–61.
Brotons-Gil E, García-Vaquero MP, Peco-González N, Vera-Garcia FJ. Flexion-rotation Trunk Test To Assess Abdominal Muscle Endurance: Reliability, Learning Effect, and Sex Differences. J Strength Cond Res. 2013;27(6):1602–8.
Danneskiold-Samsøe B, Bartels EM, Bülow PM, Lund H, Stockmarr A, Holm CC, et al. Isokinetic and Isometric Muscle Strength in a Healthy Population with Special Reference to Age and Gender. Acta Physiol. 2009;197(673):1–68.
Tieland M, Trouwborst I, Clark BC. Skeletal Muscle Performance and Ageing. J Cachexia Sarcopenia Muscle. 2018;9(1):3–19.
Latikka P, Battié MC, Videman T, Gibbons LE. Correlations of Isokinetic and Psychophysical Back Lift and Static Back Extensor Endurance Tests in Men. Clin Biomech. 1995;10(6):325–30.
McGregor RA, Cameron-Smith D, Poppitt SD. It Is Not Just Muscle Mass: A Review of Muscle Quality, Composition and Metabolism During Ageing As Determinants of Muscle Function and Mobility in Later Life. Longev Healthspan. 2014;3(1):1–8.
Strand SL, Hjelm J, Shoepe TC, Fajardo MA. Norms For An Isometric Muscle Endurance Test. J Hum Kinet. 2014;40(1):93–102.
Kankaanpää M, Laaksonen D, Taimela S, Kokko SM, Airaksinen O, Hänninen O. Age, Sex, and Body Mass Index as Determinants of Back and Hip Extensor Fatigue in the Isometric Sørensen Back Endurance Test. Arch Phys Rehabil. 1998;79:1069–75.
Torres SH, de Oca MM, Loeb E, Mata A, Hernandez N. Gender and Skeletal Muscle Characteristics in Subjects with Chronic Obstructive Pulmonary Disease. Respir Med. 2011;105(1):88–94.
Hogrel JY, et al. Development of a French Isometric Strength Normative Database for Adults Using Quantitative Muscle Testing. Arch Phys Med Rehabil. 2007;88:1289–97.
Calmels P, Minaire P. A Review of the Role of the Agonist/Antagonist Muscle Pairs Ratio in Rehabilitation. Disabil Rehabil. 1995;17(6):265–76.
Acknowledgements
The authors would like to thank Dr. Camille Amoura and Dr. Gabor Orosz for the advice during the statistic study of this manuscript and professionals of the Oignies rehabilitation center for the advice during the implementation of the assessment protocol. This project benefited from CIFRE financing no. 2018/0103.
Funding
This project benefited from CIFRE financing no. 2018/0103. The program CIFRE (“Conventions Industrielles de Formation par la Recherche” – Industrial Training and Research Agreement) is a partnership between a French company, a laboratory of research and a graduate. This convention between three partners allows a company to host a PhD student for 3 years.
Author information
Authors and Affiliations
Contributions
FJ and CF wrote the first draft of the manuscript; CT contributed to revisions of the manuscript. ALS, BM, and FB supervised the study and contributed to data acquisition, procedural protocols. All authors contributed to the study design, procedural protocols, and the drafting of this paper. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Before being included in the study, the design, rules, and protocol were explained to each subject. Then each subject signed a written consent form. The study protocol was approved by the Ethics Committee under No. 2019-380-S77. The ethics committee is supported by the University of Lille and there is only one committee within this institution. Its name is Behavioral Science Ethics Committee.
Consent for Publication
Not applicable.
Competing Interests
The authors, Frédérick Janik, Claire Toulotte, Anne Laure Seichepine, Bernadette Masquelier, Fabienne Barbier, and Claudine Fabre, declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Janik, F., Toulotte, C., Seichepine, A.L. et al. Isometric Strength Database for Muscle Maximal Voluntary Endurance Field Tests: Normative Data. Sports Med - Open 7, 47 (2021). https://doi.org/10.1186/s40798-021-00338-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-021-00338-2