
Abstract
Background
Malignant tumors with rhabdoid features are rare, highly aggressive, and some of them are characterized by SMARCB1 (INI1) loss. Although cases of rhabdoid carcinoma are extremely rare, its occurrence in the colon has been reported previously.
Case presentation
A 71-year-old Japanese female patient presented with loss of appetite, fatigue, and weight loss. Computed tomography demonstrated a tumor in the right colon that infiltrated the surrounding kidneys and swelling of the left supraclavicular and periaortic lymph nodes. Laparotomy revealed that the tumor was unresectable because it had directly invaded the head of the pancreas and duodenum. Therefore, ileocecal vascularized bulky lymph nodes were sampled, and gastrojejunostomy with Braun’s anastomosis and ileotransversostomy were performed as palliative procedures. Histopathological examination of the lymph nodes revealed that the neoplastic cells had rich eosinophilic cytoplasm and eccentrically located large nuclei characteristic of rhabdoid carcinoma. In addition, these neoplastic cells lacked SMARCB1 expression; therefore, the patient was diagnosed with SMARCB1-negative rhabdoid carcinoma. The postoperative course was uneventful. Molecular analysis confirmed that the neoplastic cells had high microsatellite instability (MSI); therefore, two cycles of pembrolizumab were administered. However, no clinical benefit was noted, and the patient died 3 months postoperatively.
Conclusion
This is the first report of a case of SMARCB1-negative rhabdoid colon carcinoma with high MSI treated with pembrolizumab. Rhabdoid carcinoma is highly aggressive; therefore, additional studies are required to determine the therapeutic strategy for SMARCB1-negative rhabdoid colorectal carcinoma.
Similar content being viewed by others


Background
Malignant tumors with rhabdoid features are extremely rare. These tumors are characterized by a rhabdomyoblast-like appearance due to the presence of neoplastic cells with cytoplasm containing rich hyaline-like filamentous paranuclear inclusions and eccentrically located large round-to-oval nuclei with conspicuous nucleoli. Sporadic occurrence of this type of tumor has been reported in various organs [1,2,3]. Prototypes of malignant tumors with rhabdoid features include malignant rhabdoid tumors of the kidneys and atypical teratoid/rhabdoid tumors of the central nervous system. These highly aggressive tumors frequently demonstrate loss of SMARCB1 (encoding INI1 protein) expression [4, 5]. It was demonstrated that carcinomas with rhabdoid features (rhabdoid carcinomas) show frequent loss of SMARCB1 and a highly aggressive course [1, 2]. Rhabdoid carcinomas can occur in the gastrointestinal tract [1,2,3]. Agaimy et al. analyzed the clinicopathological features of 39 previously reported and two new cases of rhabdoid carcinoma. The most common site of this type of tumor was the stomach (13 cases), followed by the colon (11 cases), small intestine (10 cases), and esophagus (5 cases), although not all of the previously reported cases involved the loss of SMARCB1 [1]. To the best of our knowledge, only five cases of rhabdoid carcinoma with SMARCB1 loss occurring in the colorectum have been reported [1, 2, 6,7,8]. Herein, we report the first case of SMARCB1-negative rhabdoid right-sided colon cancer treated with immune checkpoint inhibitors (ICIs) because of microsatellite instability (MSI)-high status. Further, we discuss the clinicopathological features of this type of tumor.
Case presentation
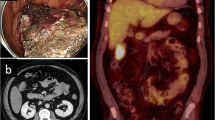
A 71-year-old Japanese female patient, with no remarkable clinical history, presented with loss of appetite, fatigability, and weight loss of 8 kg over 3 months when treated at an outpatient clinic. Computed tomography findings demonstrated a tumor, measuring 7.5 × 7 cm in diameter present in the right side of the colon, which infiltrated into the adjacent kidney, and swelling of the left supraclavicular and periaortic lymph nodes (Fig. 1). Therefore, she was referred to our hospital for further evaluation and treatment. At presentation, the patient was thin with a body mass index of 17.2 kg/m2 (height 176 cm and body weight 53.2 kg). Physical examination revealed that the eyelid conjunctiva was pale, and a palpable mass with poor mobility was present in the upper right abdomen. Laboratory tests revealed anemia (hemoglobin level 7.2 g/dL and hematocrit value 22.7%) and inflammation (white blood cell count 13,800/µL and C-reactive protein 6.534 mg/dL). The levels of tumor markers were within the normal range (cancer embryonic antigen 1.2 ng/mL and carbohydrate antigen 19–9 < 4.0 U/mL). Although colonoscopy revealed severe stenosis and edematous mucosa in the right colon that the endoscopic fiber could not pass through, no obvious neoplastic lesions were detected (Fig. 2).

Computed tomography scan. a A tumor in the right transverse colon, directly invading the right kidney. b, c Swelling of the periaortic (b) and left supraclavicular lymph nodes (c) (arrows)

Colonoscopic findings. The presence of edematous mucosa in the right transverse colon is seen, however, no tumorous lesion is observed
A laparoscopic examination was performed under a clinical diagnosis of suspected right-sided colon cancer (clinical stage IV), which revealed no obvious peritoneal dissemination, and intraoperative cytological examination of the ascitic fluid was negative. Subsequently, laparotomy was performed to evaluate whether the tumor was resectable. When the omental bursa was opened, it showed that the tumor directly invaded the head of the pancreas, right kidney, and the second portion of the duodenum. In addition, direct invasion of the superior mesenteric vessels was observed. Therefore, radical resection of the tumor was considered impossible. A part of the tumor was resected and submitted for an intraoperative consultation, leading to the histopathological diagnosis of a malignant epithelioid tumor, unlike a typical colon cancer. Ileocecal vascularized bulky lymph nodes (No. 201 lymph node) with suspected metastases were sampled, and gastrojejunostomy with Braun’s anastomosis and ileotransversostomy were performed as palliative procedures. The surgery lasted 164 min, and the total blood loss was 13 mL.
Histopathological examination of the resected No. 201 lymph node demonstrated that the lymph node was occupied by sheets or irregular nests of neoplastic cells with geographic necrosis. These neoplastic cells were polygonal in shape with a rich eosinophilic cytoplasm and eccentrically located large round-to-oval nuclei containing conspicuous nucleoli, which are the characteristic features of rhabdoid appearance (Fig. 3a). Conventional tubular adenocarcinoma components were not observed. Immunohistochemical analyses revealed that these rhabdoid neoplastic cells were positive for keratin 20, CDX-2, and HNF4alpha (Fig. 3b–d) but negative for keratin 7, chromogranin A, and synaptophysin. These neoplastic cells showed a characteristic loss of INI1 (Fig. 3e). A metastatic SMARCB1-negative rhabdoid carcinoma in the lymph nodes was diagnosed.

Histopathological and immunohistochemical findings of the lymph node. a The proliferation of the polygonal neoplastic cells having rich eosinophilic cytoplasm and eccentrically located large round-to-oval nuclei containing nucleoli (hematoxylin and eosin, × 200). The neoplastic cells express CDX-2 (b), keratin 20 (c), and HNF4alpha (d) (× 200). e Loss of SMARCB1 expression is observed in the neoplastic cells (note: SMARCB1 expression is noted in the non-neoplastic cells) (× 200)
The postoperative course was uneventful, and the patient resumed eating on the 3rd postoperative day. Two cycles of pembrolizumab 200 mg every 3 weeks were administered because molecular analysis of the metastatic carcinoma in the lymph node confirmed that the neoplastic cells were RAS-wild type, BRAFV600E-mutant, and MSI-high. However, no clinical benefit was noted, and the patient died 3 months postoperatively.
Discussion
In the present report, we described the 6th case of SMARCB1-negative rhabdoid carcinoma occurring in the right colon. This is the first case of this type of tumor that was treated with pembrolizumab.
SMARCB1 is a tumor suppressor gene that constitutes the SWItch/Sucrose Non-Fermentable (SWI/SNF) chromatin remodeling complex that causes a conformational change in the nucleosome, alters histone–DNA binding, and facilitates transcription factor access [9, 10]. Loss of SMARCB1 is characteristic of malignant tumors with rhabdoid features. Some cases of rhabdoid carcinoma occurring in the gastrointestinal tract also showed the loss of this gene [1,2,3]. Fewer than 30 cases of colorectal rhabdoid carcinoma have been reported, although most were not analyzed for SMARCB1 [8]. Only six cases, including the present case, showed loss of SMARCB1 [1, 2, 6,7,8], and a few rhabdoid carcinoma cases with retained SMARCB1 expression occurring in the colorectum have also been reported [11, 12]. In a study that analyzed 3,051 cases of colorectal carcinoma, SMARCB1 loss was detected in only 0.46% of the cases. These tumors tended to have larger sizes, higher histological grading, and poorer prognosis [13]. Table 1 summarizes the clinicopathological features of previously reported cases of SMARCB1-negative rhabdoid carcinoma occurring in the colon, similar to the present case. The median age of the patients was 72 (range 41–81) years with male and female sexes being equally affected. All reported cases had a large tumor and metastases to lymph nodes and the liver. Most patients died of the disease within 6 months, although one case with SMARCB1-negative rhabdoid carcinoma in the cecum without tumor recurrence 48 months after surgery has been reported [7].
The primary tumor was unresectable in the present case. The diagnosis of SMARCB1-negative rhabdoid carcinoma was histopathologically and immunohistochemically confirmed using a metastatic lymph node specimen. The neoplastic cells in the metastatic lymph nodes showed the colorectal phenotype because CDX-2 (intestinal marker) and HNF4alpha (gastrointestinal marker) were expressed. Keratin 7-negative and keratin 20-positive phenotypes were typical for colorectal carcinomas, although the loss of CDX-2 expression was noted in some colon rhabdoid carcinomas [6, 8]. Thus, we considered that the neoplastic cells in the metastatic lymph node were of right-sided colon origin, based on clinical and imaging test findings.
The deficiency of the mismatch repair system has been recognized in approximately 15% of colorectal carcinomas [14]. MLH1 epigenetic silencing is the most frequent event responsible for MSI. MSI-high status is characterized by a frequent right-sided colon location, poorly differentiated histology, signet ring cell carcinoma or mucinous carcinoma component, and numerous infiltrating lymphocytes [15]. BRAF V600E mutation is also frequently noted in right-sided colon cancer, and patients with tumors with MSI-high status more commonly have this mutation [16]. Loss of MLH1 or MSH6 was also noted in SMARCB1-negative rhabdoid carcinoma of the colon (Table 1), and the present patient showed an MSI-high phenotype. Therefore, we administered two cycles of pembrolizumab because its efficacy was reported in patients with colorectal cancer with MSI-high status [17]. However, the patient died 3 months after the surgery without any clinical benefits. The most important factor in the resistance to ICIs therapy might be the high-grade aggressive rhabdoid tumor. In generally, the infiltration of CD8+ T cells into the tumor microenvironment is important for the efficacy of ICIs [18, 19]. Although details of CD8+ T cells in the tumor microenvironment were not available in this case because of the lack of the main tumor specimen. The use of ICIs is a promising therapeutic strategy, and therapeutic efficacy has already been reported in SMARCB1-negative sarcomas [20]. Additional clinical studies of ICI therapy for SMARCB1-negative colorectal rhabdoid carcinoma are required to establish a therapeutic strategy for this type of tumor.
Moreover, in some patients with metastatic colorectal cancer with the BRAF V600E mutation, the combination of encorafenib, cetuximab, and binimetinib significantly prolonged overall survival and demonstrated a high response rate compared to the standard therapy [21]. Although it might be difficult to administer this triple therapy because of poor performance status, future combination therapy might be considered for treating rhabdoid colorectal cancer with BRAF V600E mutation. In addition, the efficacy of EZH2 inhibitors in patients with advanced SMARCB1-negative epithelioid sarcoma has been reported [22]. Thus, colorectal rhabdoid carcinoma with loss of SMARCB1 may benefit from these inhibitors. However, additional clinical studies are needed to clarify the therapeutic strategy for SMARCB1-negative rhabdoid colorectal carcinoma.
Availability of data and materials
All data generated or analyzed in the present study are included in this published article.
Abbreviations
- CDX-2:
-
Caudal-type homeobox-2
- HNF4alpha:
-
Hepatocyte nuclear factor 4 alpha
- ICI:
-
Immune checkpoint inhibitor
- INI1:
-
Integrated interactor 1
- MSI:
-
Microsatellite instability
- EZH2:
-
Enhancer of zeste homolog 2; MLH1; MHS6
References
Agaimy A, Rau TT, Hartmann A, Stoehr R. SMARCB1 (INI1)-negative rhabdoid carcinomas of the gastrointestinal tract: clinicopathologic and molecular study of a highly aggressive variant with literature review. Am J Surg Pathol. 2014;38(7):910–20.
Tessier-Cloutier B, Schaeffer DF, Bacani J, Marginean CE, Kalloger S, Köbel M, Lee CH. Loss of switch/sucrose non-fermenting complex protein expression in undifferentiated gastrointestinal and pancreatic carcinomas. Histopathology. 2020;77(1):46–54.
Hollmann TJ, Hornick JL. INI1-deficient tumors: diagnostic features and molecular genetics. Am J Surg Pathol. 2011;35:e47-63.
Verstege I, Sevent N, Lange J, Rouseau-Merck MF, Ambros P, Handgretinger R, Aurias A, Delatre O. Truncating mutations of hSNF5/INI1 in aggressive paediatric cancer. Nature. 1998;394(6689):203–6.
Biegel JA, Tan L, Zhang F, Wainwright L, Russo P, Rorke LB. Alterations of the hSNF5/INI1 gene in central nervous system atypical teratoid/rhabdoid tumors and renal and extrarenal rhabdoid tumors. Clin Cancer Res. 2002;8(11):3461–7.
Pancione M, Remo A, Sabatino L, Zanella C, Votino C, Fucci A, Di Blasi A, Lepore G, Daniele B, Fenizia F, Molinari E, Normanno N, Manfrin E, Vendraminelli R, Colantuoni V. Right-sided rhabdoid colorectal tumors might be related to the serrated pathway. Diagn Pathol. 2013;8:31.
D’Amico F, Bertacco A, Cesari M, Mescoli C, Caturegli G, Gondolesi G, Cillo U. Extraordinary disease-free survival in a rare malignant extrarenal rhabdoid tumor: a case report and review of the literature. J Med Case Rep. 2018;12(1):39.
Kojima M, Miyake T, Ueki T, Ohta H, Kushima R, Shiohara M, Mizuta H, Iida H, Yamaguchi T, Kaida S, Takebayashi K, Maehira H, Nishina Y, Shimizu T, Mekata E, Tani M. INI1-negative colorectal undifferentiated carcinoma with rhabdoid features and postoperative rapidly growing liver metastases: a case report and review of the literature. Surg Case Rep. 2021;7(1):104.
Kadoch C, Hargreaves DC, Hodges C, Elias L, Ho L, Ranish J, Crabtree GR. Proteomic and bioinformatic analysis of mammalian SWI/SNF complexes identifies extensive roles in human malignancy. Nat Genet. 2013;45(6):592–601.
Masliah-Planchon J, Bièche I, Guinebretière JM, Bourdeaut F, Delattre O. SWI/SNF chromatin remodeling and human malignancies. Annu Rev Pathol. 2015;10:145–71.
Kalyan A, Pasricha G, Monga D, Singhi A, Bahary N. Case report of rhabdoid colon cancer and review of literature. Clin Colorectal Cancer. 2015;14(1):e5-8.
Samalavicius NE, Stulpinas R, Gasilionis V, Baltruskeviciene E, Aleknavicius E, Mickys U. Rhabdoid carcinoma of the rectum. Ann Coloproctol. 2013;29(6):252–5.
Wang J, Andrici J, Sioson L, Clarkson A, Sheen A, Farzin M, Toon CW, Turchini J, Gill AJ. Loss of INI1 expression in colorectal carcinoma is associated with high tumor grade, poor survival, BRAFV600E mutation, and mismatch repair deficiency. Hum Pathol. 2016;55:83–90.
Le DT, Durham JN, Smith KN, Wang H, Bartlett BR, Aulakh LK, Lu S, Kemberling H, Wilt C, Luber BS, Wong F, Azad NS, Rucki AA, Laheru D, Donehower R, Zaheer A, Fisher GA, Crocenzi TS, Lee JJ, Greten TF, Duffy AG, Ciombor KK, Eyring AD, Lam BH, Joe A, Kang SP, Holdhoff M, Danilova L, Cope L, Meyer C, Zhou S, Goldberg RM, Armstrong DK, Bever KM, Fader AN, Taube J, Housseau F, Spetzler D, Xiao N, Pardoll DM, Papadopoulos N, Kinzler KW, Eshleman JR, Vogelstein B, Anders RA, Diaz LA Jr. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science. 2017;357(6349):409–13.
Shia J, Ellis NA, Paty PB, Nash GM, Qin J, Offit K, Zhang XM, Markowitz AJ, Nafa K, Guillem JG, Wong WD, Gerald WL, Klimstra DS. Value of histopathology in predicting microsatellite instability in hereditary nonpolyposis colorectal cancer and sporadic colorectal cancer. Am J Surg Pathol. 2003;27(11):1407–17.
Ikoma T, Shimokawa M, Kotaka M, Matsumoto T, Nagai H, Boku S, et al. Clinical and prognostic features of patients with detailed RAS/BRAF-mutant colorectal cancer in Japan. BMC Cancer. 2021;21(1):518.
André T, Shiu KK, Kim TW, Jensen BV, Jensen LH, Punt C, Smith D, Garcia-Carbonero R, Benavides M, Gibbs P, de Fouchardiere C, Rivera F, Elez E, Bendell J, Lee DT, Yoshino T, Van Cutsem E, Yang P, Farooqui MZH, Marinello P, Diaz LA. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N Engl J Med. 2020;383(23):2207–18.
Kumagai S, Togashi Y, Kamada T, Sugiyama E, Nishinakamura H, Takeuchi Y, Vitaly K, Itahashi K, Maeda Y, Matsui S, Shibahara T, Yamashita Y, Irie T, Tsuge A, Fukuoka S, Kawazoe A, Udagawa H, Kirita K, Aokage K, Ishii G, Kuwata T, Nakama K, Kawazu M, Ueno T, Yamazaki N, Goto K, Tsuboi M, Mano H, Dou T, Shitara K, Nishikawa H. The PD-1 expression balance between effector and regulatory T cells predicts the clinical efficacy of PD-1 blockade therapies. Nat Immunol. 2020;21(11):1346–58.
Jenkins RW, Barbie DA, Flaherty KT. Mechanisms of resistance to immune checkpoint inhibitors. Br J Cancer. 2018;118(1):9–16.
Ngo C, Postel-Vinay S. Immunotherapy for SMARCB1-Deficient Sarcomas: current evidence and future developments. Biomedicines. 2022;10(3):650.
Kopetz S, Grothey A, Yaeger R, van Cutsem E, Desai J, Yoshino T, Wasan H, Ciardiello F, Loupakis F, Hong YS, Steeghs N, Guren TK, Arkenau HT, Garcia-Alfonso P, Pfeiffer P, Orlov S, Lonardi S, Elez E, Kim TW, Schellens JHM, Guo C, Krishnan A, Dekervel J, Morris V, Calvo Ferrandiz A, Tarpgaard LS, Braun M, Gollerkeri A, Keir C, Maharry K, Pickard M, Christy-Bittel J, Anderson L, Sandor V, Tabernero J. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E–mutated colorectal cancer. N Engl J Med. 2019;381(17):1632–43.
Gounder M, Schöffski P, Jones RL, Agulnik M, Cote GM, Villalobos VM, Attia S, Chugh R, Chen TW, Jahan T, Loggers ET, Gupta A, Italiano A, Demetri GD, Ratan R, Davis LE, Mir O, Dileo P, Van Tine BA, Pressey JG, Lingaraj T, Rajarethinam A, Sierra L, Agarwal S, Stacchiotti S. Tazemetostat in advanced epithelioid sarcoma with loss of INI1/SMARCB1: an international, open-label, phase 2 basket study. Lancet Oncol. 2020;21(11):1423–32.
Acknowledgements
None of the authors received any financial support.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
TK contributed to the conception and design of the study; TK, HM, MI, YM, MH, HS, and MS contributed to the acquisition and analysis of data; and TK and MI contributed to the drafting of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Kansai Medical University Hospital (approval no. #2021108). Informed consent was obtained from the patients via the opt-out method, owing to the study’s retrospective design, with no risk to the participants.
Consent for publication
Consent was obtained from the patient to publish the clinical and imaging data in this report.
Competing interests
Hironaga Satake received research funding from Ono Pharmaceutical Co., Ltd., Daiichi Sankyo, Taiho Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., and Sanofi; honoraria from Bayer Co., Ltd.; Bristol-Myers Squibb Co., Ltd., Chugai Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., Eli Lilly Japan Co., Ltd., Merck Bio Pharma Co., Ltd., MSD Co., Ltd., Ono Pharmaceutical Co., Ltd., Sanofi Co., Ltd., Taiho Pharmaceutical Co., Ltd., Takeda Co., Ltd., and Yakult Honsha Co., Ltd.
The other authors disclose no conflict of interest related to the content of this report.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kobayashi, T., Matsui, Y., Miki, H. et al. Case report: administration of immune checkpoint inhibitor for SMARCB1 (INI1)-negative rhabdoid carcinoma with microsatellite instability (MSI)-high in the right colon. surg case rep 9, 17 (2023). https://doi.org/10.1186/s40792-023-01594-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-023-01594-y