
Abstract
Background
Mediastinal foreign bodies might cause mediastinal organ injury or mediastinal abscess. The prompt removal surgery of mediastinal foreign bodies is needed to prevent those complications. We report a case in which a mediastinal foreign body was removed by video-mediastinoscopy.
Case presentation
The patient, a 74-year-old man with a chief complaint of hoarseness, was referred to our department for surgical management of a wooden foreign body that had traumatically migrated into the superior mediastinum. During the surgery, the video-mediastinoscopy was introduced under the pneumomediastinal pressure. We could dissect the scar tissue and remove the azalea tree branch safely and carefully, without damaging the other mediastinal organs. He was discharged on postoperative day 5, with no complications.
Conclusions
Video-mediastinoscopic approach under pneumomediastinal pressure is minimally invasive and could provide wide surgical view. Therefore, we consider it useful and effective for removal of foreign bodies in the mediastinum.
Similar content being viewed by others


Background
Mediastinal foreign bodies might cause mediastinal organ injury or mediastinal abscess [1]. Furthermore, severe inflammation and the complexity of the mediastinal anatomy might make it difficult to remove them [2]. Thus, the prompt removal of mediastinal foreign bodies should be needed to prevent those complications. However, there is no consensus on the surgical managements and the timing of surgery. We herein used video-mediastinoscopy under pneumomediastinal pressure for a mediastinal foreign body removal operation.
Case presentation
A 74-year-old man was refered to our department for the surgical management of a superior mediastinal foreign body. In July 2018, he was pruning his garden on a stepladder. He accidentally fell from the ladder, and an azalea tree branch was lodged in the external sternocleidomastoid muscle of his his left neck. He was immediately transported to the other hospital, and underwent the removal operation on the same day. For a while after surgery, he had no symptoms, such as fever or difficulty in swallowing. However, after 4 months in November 2018, he gradually felt hoarseness and revisited the same hospital. As a result of precise examinations, he was strongly suspected of the tree branch remaining.
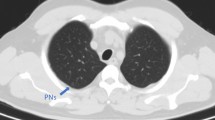
His physical examination and laboratory data revealed no remarkable findings. The left vocal cord was fixed in the paramedial position. Upper gastrointestinal endoscopy showed an elevated lesion on the anterior wall of the upper thoracic esophagus, 20 cm far from the incisors (Fig. 1). Contrast-enhanced computed tomography (CT) revealed a superior mediastinal linear foreign body with peripheral enhancement, located between trachea and esophagus (Fig. 2). The size was approximately 10 × 45 mm. There was no mediastinal abscess. To investigate the characteristics of the foreign body in detail, contrast-enhanced magnetic resonance imaging (MRI) was performed. The peripheral region revealed low intensity on both plain T1- and T2-weighted imaging, and on the other hand, the internal region revealed iso-intensity on plain T1-weighted imaging and high on plain T2 (Fig. 3A,B). And a non-signal line was revealed in the foreign body in contrast-enhanced T1-weighted imaging (Fig. 3C). As a result of the non-signal line and the MRI effect, we concluded that the foreign body was something wooden. He had the symptom of hoarseness and the risk of mediastinitis and esophagus perforation, so removal re-operation of the mediastinal foreign body was considered to be needed. Finally, in January 2019, we performed a foreign body removal re-operation by video-mediastinoscopy.

Preoperative upper gastrointestinal endoscopy. An elevated lesion was revealed on the anterior wall of the upper thoracic esophagus (arrowhead). This confirmed compression from something external

Contrast-enhanced CT. A superior mediastinal foreign body, located between trachea and esophagus, was sticking toward the internal, caudal side (arrowhead)

Contrast-enhanced MRI. Plain T1-weighted imaging (A), and plain T2 (B). Contrast-enhanced T1 (C) showed a non-signal line in the mediastinal foreign body
Under general anesthesia, along the surgical scar on the left neck made in the first operation in July 2018, a 7-cm oblique incision was made. After exposing the inner edge of the sternocleidomastoid muscle, 70-mm diameter EZ-Access™ and Lap-Protector™ (Hakkou Shoji, Japan) were covered over the incision, and one 12-mm port and two 5-mm ports were inserted (Fig. 4A). Then, the video-mediastinoscopy was introduced through the 12-mm port, under pneumomediastinal pressure (5–8 cm H2O). With the wide surgical view, we dissected the scar tissue between the left wall of the trachea and the left common carotid artery to the caudal and dorsal sides (Fig. 4B). The scar tissue had become hard due to inflammation. Proceeding with the careful dissection, we reached into the cavity, where several twigs were removed. We further dissected the cavity to the dorsal side, and found a large wooden foreign body filling the whole cavity (Fig. 4C). We carefully performed adhesiolysis and gradually extended the cavity. Finally, an azalea tree branch, 4 cm long, was safely removed (Fig. 4D, E). After removal, upper gastrointestinal endoscopy was introduced during the surgery, and we confirmed no damage to the mucosa in the esophagus. We also investigated the cavity and confirmed neither foreign bodies remaining nor abscess. Left recurrent laryngeal nerve was not detected during the surgery. One drainage tube was placed at the bottom of the cavity, and the neck incision was closed. Operation time was 166 min, and blood loss volume was 45 ml.

Intraoperative findings
After the surgery, the patient was extubated without difficulty. Perioperative antibiotic therapy was discontinued on postoperative day 1. On postoperative day 2, the drainage tube was removed, and enteral feeding was initiated. The patient was discharged from our hospital on postoperative day 5, without any complications. Follow-up CT after the discharge revealed no mediastinal foreign bodies remaining (Fig. 5). Subsequent follow-up visits every 4 months demonstrated good wound healing, but he still felt hoarseness despite two surgeries, so he was taking vocalization rehabilitation.

Postoperative CT. There were no remaining mediastinal foreign bodies
Discussion
Foreign bodies migrating into the mediastinum occur from direct injury or penetration by sharp foreign bodies in trachea and esophagus, for example, accidental ingestion or committing suicide. Mediastinal foreign bodies are associated with the considerable risk of descending necrotizing mediastinitis, mediastinal abscess, and the mediastinal organ injury, such as esophagus, trachea, or aorta [3]. Thus, the removal operation for them is considered to be required. However, multidisciplinary efforts of radiologists, gastroenterologists, anesthesiologists, and thoracic surgeons are needed for optimal preoperative planning, according to the shape, size and location of the mediastinal foreign bodies [2]. Furthermore, no consensus has been reached regarding surgical approach and the timing of surgery. But in our case, he had symptom of hoarseness and delayed treatment might lead esophagus perforation and mediastinitis, so he needed to undergo removal re-operation as prompt as possible.
A search on PubMed using the keywords “mediastinal foreign body” revealed 59 reported cases worldwide (iatrogenic migration cases were excluded). The cause of 13 cases (22.0%) is by direct injury. The types of foreign body have included fish bone (n = 8), needle (n = 7), a bullet (n = 7), teeth prosthesis (n = 5), and so on. Surgical removal approaches for them vary, and the most common approach is thoracotomy, 30 cases (50.8%). In recent years, thoracoscopic approaches have also increased. In any approach, to prevent damage to the mediastinal organs and foreign bodies remaining, we should remove them not by pulling out forcibly, but by dissecting the surrounding tissue carefully. Of 59 cases, there are only seven reported cases using video-mediastinoscopy (Table 1) [2, 4,5,6,7,8,9]. Four cases were caused due to direct injury by bullet, and three due to penetration into the mediastinum by accidental ingestion of pin stick, teeth prothesis, and fish bone. In all cases, the foreign bodies were located in the superior mediastinum. None of these reports described pneumomediastinal pressure.
Mediastinoscopy has high diagnostic value and low rates of mortality and morbidity, resulting in mediastinoscopy as a widely used method for mediasitnal pathology, like preoperative nodal staging of lung cancer. [10, 11]. Recently it has been applied in esophageal cancer resection and cervical lymphadenectomy [12, 13]. In 1970, Ward [4] first reported the removal operation of a bullet migrating into the superior mediastinum by mediastinoscopy under local anesthesia. The mediastinum consists of several important organs, vessels, and nerves. Thus, highly meticulous procedures for mediastinal surgery are required. Video-mediastinoscopy and pneumomediastinal pressure could provide the expanded surgical view in narrow mediastinal region, and make the precise surgery. And more, since mediastinal approach does not need intrathoracic procedures, it could be safely introduced for the patients who have difficulty in thoracotomy due to severe respiratory failure or preoperatively suspected pleural adhesion. Compared to thoracotomy, mediastinoscopic surgery is more minimally invasive, and offers the advantage of reduced recovery time, reduced pain, and improved cosmesis [14]. In contrast, we must recognize the risk and complications of mediastinoscopic approach. The common complications include bleeding, pneumothorax, wound infection, tracheal injury, and recurrent nerve injury [15]. And when the mediastinoscopy is inserted, it could cause compression of the innominate artery, resulting in dissection or transient ischemic attack [16]. Furthermore, while we could obtain wide surgical view, our handlings are limited within a narrow retractor, so interference between surgeons could become the major problem. We must also pay attention to pneumomediastinal pressure. In transcervical minimally invasive esophagectomy of the animal model, from the perspective of restricted circulatory blood flow and lower perfusion thereafter, pressure over 12 mmHg will be inappropriate [17]. So, in summary, when vascular injury occurs and results in poor surgical view, it is necessary not to hesitate to introduce thoracotomy. And when bilateral recurrent laryngeal nerve injury occurs, it is important to prepare surgical airway on the patient. In our case, the patient had hoarseness, and considered the risk of postoperative respiratory failure, video-mediastinoscopic approach was preferred rather than the thoracoscopic approach.
The limitations of this single case report must be acknowledged; it is still unclear whether video-mediastinoscopy could be applied in all mediastinal foreign body cases. Therefore, it is necessary to consider the surgical indication of the mediastinoscopy according to the size and location of the foreign bodies. And more, of course, we could not prove the superiority of the video-mediastinoscopy over the thoracoscopy. Thus, further more cases are needed.
Conclusions
This is the first reported case of the removal of mediastinal foreign bodies by video-mediastinoscopy under pneumomediastinal pressure. Our case suggests that it is minimally invasive and could provide expanded surgical view, so is recommended as one of the best surgical approaches for removal of mediastinal foreign bodies.
Availability of data and materials
The data supporting the conclusions of this article are included within the article.
Abbreviations
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
References
Birk M, Bauerfeind P, Deprez PH, Häfner M, Hartmann D, Hassan C, et al. Removal of foreign bodies in the upper gastrointestinal tract in adults: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2016;48:489–96.
Wang J, Wu WB, Chen L, Zhu Q. Video-mediastinoscopy assisted fish bone extraction and superior Medistinal abscess debridement. J Cardiothorac Surg. 2018;13:38. https://doi.org/10.1186/s13019-018-0732-7.
Ghimire A, Bhattarai M, Kumar M, Wakode PT. Descending necrotizing mediastinitis: a fatal complication of neglected esophageal foreign body. Kathmandu Univ Med J (KUMJ). 2007;5:98–101.
Ward PH. Mediastinoscopy under local anesthesia. A valuable diagnostic technique. Calif Med. 1970;112:15–22.
Larrieu AJ, Tyers GF, Williams EH, Derrick JR. Mediastinoscopic removal of a superior mediastinal foreign body. S Med J. 1980;73:1539–40.
Faries PL, Martella AT, Santos GH. Mediastinoscopy for the evaluation and treatment of projectile injuries. Am Surg. 1996;62:1073–5.
Lynch JB, Kerschner JE, Aiken JJ, Farber N, Bousamra M. Use of mediastinoscopy for foreign body removal. Int J Pediatr Otorhinolaryngol. 1999;50:225–8.
Tekinbas C, Erol M. Video-mediastinoscope: for extracting upper esophageal foreign bodies. Ann Thorac Surg. 2007;83:2239–40.
Metin B, Tözüm H, Kaya S. Removal of mediastinal foreign body (steel shot) using mediastinoscopy: case report. Ulus Travma Acil Cerrahi Derg. 2013;19:581–4.
Chauhan A, Kapoor S, Ganguly M, Nath P. Cervical mediastinoscopy: re-evaluation of an old technique in era of new imaging technology. Indian J Chest Dis Allied Sci. 2012;54:169–73.
Azarow KS, Pearl RH, Zurcher R, Edwards FH, Cohen AJ. Primary mediastinal masses. A comparison of adult and pediatric populations. J Thorac Cardiovasc Surg. 1993;106:67–72.
Fujiwara H, Shiozaki A, Konishi H, Otsuji E. Transmediastinal approach for esophageal cancer: a new trend toward radical surgery. Asian J Endosc Surg. 2019;12:30–6.
Song Y, Dai L, Xu G, Wang T, Yu W, Chen K, et al. Video mediastinoscopy-assisted superior mediastinal dissection in the treatment of thyroid carcinoma with mediastinal lymphadenopathy: preliminary results. BMC Surg. 2021;21:329. https://doi.org/10.1186/s12893-021-01326-9.
Harris RJ, Kavuru MS, Rice TW, Kirby TJ. The diagnostic and therapeutic utility of thoracoscopy. A review. Chest. 1995;108:828–41.
Kapicibasi HO. The role of mediastinoscopy in the diagnosis of thoracic disease: 107-case analysis. Med Glas (Zenica). 2019. https://doi.org/10.17392/1001-19.
Molina GMM, Díaz APO, Sánchez AC, Sarasúa LG, Heras IPDL, Seral CC, et al. Innominate artery dissection caused by video-mediastinoscopy. Ann Thorac Surg. 2021;111:e399-401.
Chen X, Xue S, Xu JS, Zhong M, Liu X, Lin G, et al. Transcervical minimally invasive esophagectomy: hemodynamic study on an animal model. J Thorac Dis. 2020;12:6505–13.
Acknowledgements
Not applicable.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
All authors participated in the management of the patient in this case report. TS performed the literature review and drafted the manuscript. TT supervised the case and also supervised the writing of the manuscript. MK is a chairperson of our department and supervised the entire process. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare no competing interests in association with the present study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sakuma, T., Tamura, T., Nambara, M. et al. The safe removal of a superior mediastinal foreign body by mediastinoscopy: a case report. surg case rep 8, 174 (2022). https://doi.org/10.1186/s40792-022-01525-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-022-01525-3