
Abstract
Background
Although detachment of the implanted valve prosthesis was a well-known complication in patients with Behçet’s disease, complete detachment of an aortic bileaflet valve prosthesis has never been reported.
Case presentation
An 18-year-old boy with Behçet’s disease (HLA-A26 positive) who had previously undergone aortic valve replacement with an 18-mm ATS-Advanced Performance (ATS-AP) valve (ATS Medical, Inc., Minneapolis, MN) at the age of 12 years, presented sudden-onset general fatigue and was emergently transferred to the regional hospital. Chest X-ray showed displacement of the implanted mechanical valve. An echocardiogram revealed mobile valve prosthesis and severe aortic regurgitation. Just before leaving for our hospital for surgical treatment, a completely detached valve prosthesis was floating in the ascending aorta. On arrival, the valve prosthesis was stuck to the transverse arch. Emergent removal of the previous mechanical valve from the aortic arch and redo aortic valve replacement with a 24-mm ATS-AP valve were performed under total circulatory arrest. Infectious endocarditis was denied by histopathological examination. The patient was back to the intensive care unit with extracorporeal membrane oxygenation support, which was successfully decannulated 5 days later.
Conclusions
This was the first report of a patient with Behçet’s disease who encountered a complete detachment of implanted aortic valve prosthesis. The patient could be rescued by emergent surgery.
Similar content being viewed by others


Introduction
Although detachment of the implanted valve prosthesis was a well-known complication in patients with Behçet’s disease, complete detachment of an aortic bileaflet valve prosthesis has never been seen. Herein, we reported a young gentleman with Behçet’s disease who encountered a complete detachment of implanted aortic valve prosthesis 6 years later.
Case presentation
An 18-year-old boy with Behçet’s disease (HLA-A26 positive) who had previously undergone aortic valve replacement with an 18-mm ATS Open Pivot AP360 mechanical aortic valve prosthesis (ATS Medical, Inc, Minneapolis, MN) at the age of 12 years, presented sudden-onset general fatigue and was emergently transferred to the regional hospital. Since initial aortic valve replacement, 10 mg a day of prednisolone sodium succinate, 12 mg once weekly of methotrexate, 750 mg every 4–6 weeks of infliximab, and 35 mg every 2 weeks of alendronate sodium hydrate had been administered.
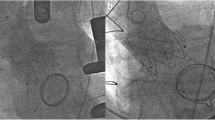
Chest X-ray showed displacement of the implanted mechanical valve (Fig. 1A, C). From a retrospective point of view, slight displacement of the valve prosthesis had been already confirmed 1 week ago at the scheduled follow-up (Fig. 1B). An echocardiogram revealed mobile valve prosthesis and severe aortic regurgitation. Just before leaving for our hospital for surgical treatment, a completely detached valve prosthesis was floating in the ascending aorta (Fig. 1C).

Chest X-ray findings 3 months ago (A), 1 week ago (B), at emergent admission to the regional hospital (C), at leaving for our hospital (D), and at arriving at our hospital (E). Black arrows indicating mechanical valve
On arrival, the valve prosthesis was stuck to the transverse arch (Fig. 1D). Emergent removal of the previous mechanical valve from the aortic arch and redo aortic valve replacement were performed under total circulatory arrest. After a removal of fibrous tissues around annulus on where previous valve prosthesis was placed, 14 pairs of pledgeted 2–0 polyester terephthalate braided, non-everting mattress suture from deep subannular left ventricular endocardium to the aortic wall just above the true annulus were placed to prevent recurrent detachment of implanted valve prosthesis. After that, a newly fashioned 24-mm ATS Open Pivot AP360 valve could be implanted in the supra-annular position without any annular enlargement procedures. The patient was back to the intensive care unit with extracorporeal membrane oxygenation support. Histopathology of the surrounding tissue around a previous valve prosthesis showed no bacterial infection sign, then only inflammatory change was noted (Fig. 2A, B).

A Photomicrograph (×2, scale bar = 500 μm) by elastica van Gieson staining showed fibrous tissue with granulation and degeneration. B Photomicrograph (×200, scale bar = 50 μm) by hematoxylin and eosin staining showed granulation tissue and degenerated collagen fibers, with microvasculature, fibroblast, and inflammatory cells
Extracorporeal membrane oxygenation was successfully decannulated 5 days later. Intra-arterial balloon pump and hemodialysis could be weaned off on post-operative day 8. Intra-cranial computed tomography was performed on post-operative day 29, which revealed the hypoxic ischemic change in bilateral basal ganglia and multiple old microinfarctions. Left ventricular dysfunction has remained since then, but catecholamine support could be discontinued 2 months later. Now 3 months have been passed since the emergent surgery. He was still supported by phosphodiesterase III inhibitor, but no longer supported by mechanical ventilator. Left ventricular end-diastolic diameter and ejection fraction were 43 mm and 25%, respectively.
Sixty mg a day of soluble predonine had been initiated since post-operative day 13, which then was gradually tapered to 30 mg a day for 3 months.
Discussion
Detachment of implanted aortic valve prostheses is a well-known complication after aortic valve replacement in patients with Behçet’s disease [1, 2]. As well as an aggressive immunosuppression therapy with oral steroid administration, several technical modifications at initial valve implantation have been recently reported to prevent later valve prosthesis dehiscence [3,4,5,6].
Although complete detachment of valve prosthesis was reported in an autopsy case that was complicated by infective endocarditis [7], complete detachment of bileaflet mechanical aortic valve prosthesis in patients with Behçet’s disease has never been reported. Behçet’s disease is known to be typically associated with HLA-B51, however, a previous study showed that HLA-B51 positive did not result in frequent manifestations or severe disease course [8]. Rather, the association of atypical class I HLA antigen, such as HLA-A26 (which is positive in this patient), might be affected. Or, annular dilatation may progress during interstage period from initial aortic valve replacement to this sudden complete detachment, because mechanical valve size up from 18 to 24 mm was possible at this emergent surgery without any annular enlargement procedures.
Emergent surgery was performed just after arriving at our center. Fortunately, previously detached implanted valve prosthesis could be easily retrieved via distal ascending aortotomy under total circulatory arrest without injuring the surrounding structures. A new mechanical valve was implanted at the supra-annular position with non-everting mattress suture from deep left ventricular side with pledgets, according to a concept of previous report but subannular ring was not used [3]. Left ventricular dysfunction remained, but catecholamine support could be discontinued 2 months later. From a retrospective point of view, slight displacement of the valve prosthesis had been already confirmed 1 week before emergent admission, at scheduled follow-up (Fig. 1B). Although valve implantation technique was modified and stronger immunosuppression therapy has been initiated, care should be taken not to overlook a repeat detachment of implanted valve prosthesis.
Conclusions
This was the first report of a patient with Behçet’s disease who encountered a complete detachment of implanted aortic valve prosthesis. The patient could be rescued by emergent surgery.
Availability of data and materials
No additional data.
References
Rae SA, Vandenburg M, Scholtz CL. Aortic regurgitation and false aortic aneurysm formation in Behçet’s disease. Postgrad Med J. 1980;56:438–9.
Suzuki A, Amano J, Tanaka H, Sakamoto T, Sunamori M. Surgical consideration of aortitis involving the aortic root. Circulation. 1989;80:1222–32.
Azuma T, Yamazaki K, Saito S, Kurosawa H. Aortic valve replacement in Behcet’s disease: surgical modification to prevent valve detachment. Eur J Cardiothorac Surg. 2009;36:771–2.
Liang MY, Yao JP, Zhang X, Wang ZP. Surgical technique for aortic regurgitation attributable to Behcet’s disease: modified aortic valve replacement with reinforcement of the aortic wall. Eur J Cardiothorac Surg. 2012;41:647–8.
Tang Y, Xu Z, Liao Z, Xu J. Supraannular aortic replacement for severe valve detachment attributable to Behçet’s disease. Ann Thorac Surg. 2012;94:e55–7.
Jung Y, Ahn BH, Lee KS, Jeong IS, Kim KH, Na KJ, et al. A novel solution to prosthetic valve dehiscence after aortic valve surgery in Behçet’s disease. Interact Cardiovasc Thorac Surg. 2017;24:342–7.
Grubwieser P, Pavlic M, Hoefer D, Rabl W. Complete detachment of an aortic valve prosthesis 10 years after implantation. Int J Legal Med. 2003;117:367–70.
Gül A, Uyar FA, Inanc M, Ocal L, Tugal-Tutkun I, Aral O, et al. Lack of association of HLA-B*51 with a severe disease course in Behçet’s disease. Rheumatology (Oxford). 2001;40:668–72.
Acknowledgements
We would like to thank Dr. Tsugumi Satoh for the histopathological analysis.
Funding
None.
Author information
Authors and Affiliations
Contributions
NH wrote the manuscript (original draft) and contributed to the creation of the figures and table. TH and TS supervised and authorized this study. AM, KH, KT and AY performed the surgery and/or perioperative patient management. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
His parent permitted the utilization of his personal data for the development of medical science (18th/June/2022).
Competing interests
The authors have no competing interests to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nagase, H., Hoashi, T., Masuoka, A. et al. Completely detached mechanical aortic valve prosthesis stuck to the aortic arch in a patient with Behçet’s disease. surg case rep 8, 143 (2022). https://doi.org/10.1186/s40792-022-01506-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-022-01506-6