
Abstract
Background
Solitary fibrous tumor (SFT) is a relatively rare mesenchymal tumor that mainly affects adults. Its prognosis is good after curative resection, but distant recurrences after 10 years or longer have been reported. Recurrent SFT usually arises as a local lesion; distant metastasis is rarely reported. Here, we report lung metastases that recurred a decade after excising a retroperitoneal primary SFT.
Case presentation
A 44-year-old woman had an SFT resected from her right retroperitoneum at our hospital. Ten years later, at age 54, she underwent a lung resection after CT showed three suspected metastases in her left lung. All three were histologically diagnosed as lung metastases from the retroperitoneal SFT. However, whereas the primary SFT had 1–2 mitotic cells/10 high power fields (HPF), the metastatic lesion increased malignancy, at 50/10 HPF.
Conclusion
Patients who have had resected SFTs should be carefully followed up, as malignancy may change in distant metastasis, as in this case.
Similar content being viewed by others


Background
Solitary fibrous tumor (SFT) is a spindle-cell neoplasm with a varied presentation. It is a rare disease, occurring in only 2.8/100,000 people. SFTs usually develop in the pleura, but 30–40% of SFTs arise in extra-pleural regions [1]. Few reports on retroperitoneal SFT are available. Its prognosis is good after curative resection. However, in rare instances, even benign SFTs can recur as distant metastases long after the primary is resected—sometimes after 10 years or more [2]. Here, we report a case of lung metastasis found 10 years after excision of the primary retroperitoneal SFT.
Case presentation
A 44-year-old woman presented with a chief complaint of abdominal distension. Her primary physician found a retroperitoneal tumor on palpation. She had no medical history and no comorbidities. Laboratory tests showed no significant abnormalities in total blood count, inflammation, liver function, renal function, electrolytes, or coagulation. Various hormone tests were all negative. Computed tomography (CT) showed a 16 × 16 × 10-cm tumor in the right retroperitoneum, which ventrally displaced the duodenum and right kidney (Fig. 1a, b). Magnetic resonance imaging (MRI) also showed the tumor in the retroperitoneum, with a low signal at T1 (Fig. 1c), and a partial high signal at T2 (Fig. 1d).

CT and MRI imaging before treatment of primary tumor. a Abdominal CT shows a solid encapsulated mass with nonuniform internal structure approximately 16 × 16 × 10 cm, compressing the right kidney and duodenum to the caudal side; b contrast-enhanced CT coronary cut; c MRI shows association-clear, T1-weighted tumors with predominantly low to equal signals; d T2-weighted image showed a high signal intensity tumor with low signal intensity area inside
No distant metastases were found, and the retroperitoneal mass was curatively resected by laparotomy. The tumor was detachable from the right adrenal gland and other organs, and was judged to be a retroperitoneal tumor. The specimen was 20 cm in size, elastic with soft tissue (Fig. 2a), and had a solid part and a cystic part. Histologically, the tumor consisted of spindle-shaped cells with a patternless pattern and hemangiopericytomatous appearance (Fig. 2b). The cells immunostained positive for CD34 (Fig. 2c) and vimentin (Fig. 2d) and negative for c-KIT, EMA, Desmin, α-SMA and S-100. No necrotic tissue was seen; the specimen showed 1–2 mitotic cells/10 high power fields (HPF). No tumor cells were found on the surgical margin. The tumor was diagnosed as a morphologically and immunologically benign SFT of the retroperitoneum.

Surgical specimen and histological findings (HE and immunohistochemical staining). a Macroscopic findings showed a well-circumscribed and encapsulated elastic hard tumor, 16 × 16 × 10 cm; b tumor consisted of spindle-shaped cells with a patternless arrangement and hemangiopericytomatous appearance (×200); c, d immunohistochemical stains were positive for c CD34, d and vimentin
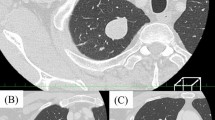
The tumor was diagnosed as benign, but because of its huge size, CT scans were performed every 6 months for 5 years. Ten years after resection, a CT scan incidentally revealed metastasis lesions. A CT scan found three nodular shadows in her left lung, including a 15-mm nodular shadow on the lower left lobe, and contrast effects indicating 9-mm and 8-mm margins on the upper lobe (Fig. 3a–c). They were suspected to be metastases of the SFT. She underwent a thoracoscopic-assisted partial left lower lobectomy and an upper left lobectomy. As with the SFT, the resected lung nodules exhibited a patternless pattern (Fig. 4a), positive immunostaining for CD34 (Fig. 4b) and vimentin (Fig. 4c), and negative stains for other interstitial markers. No evidence was seen to contradict these tumors as metastases of the retroperitoneal SFT. However, for the metastatic specimen, the mitotic figure count was 50/10 HPF, and the MIB-1 index was 20% (Fig. 4d), indicating much greater malignant potential. Six months have passed, since the lung metastasis was resected, but she is alive without recurrence.

CT imaging of metastases, 10 years after first resection. a CT shows 8-mm nodular shadow on the upper left lobe; b another 8-mm nodular shadow on the upper left lobe; c 15-mm nodular shadow on the lower left lobe

Histological findings (HE and immunohistochemical staining). a Lung tumors consisted of spindle-shaped cells with a patternless arrangement and hemangiopericytomatous appearance (×200); b, c immunohistochemical stains were positive for b CD34 and c vimentin; d MIB-1 index was 20%
Discussion
SFT is an uncommon soft-tissue neoplasm that was first reported as a type of pleural neoplasm in 1931 [3]. SFT derives from fibroblastic or myofibroblastic cells under the mesothelium [4]. It occurs mainly in the thoracic cavity, and rarely, in the retroperitoneal region, as in this case. Simple excision is considered curative for benign SFTs, and is recommended to prevent malignant transformation and metastasis [5]. About 15% of resected SFTs recur, mostly as local metastases. Distant recurrences are rare, but may appear a long time after the primary tumor has been removed [6].
Microscopically, SFTs show multiplying spindle cells with a patternless arrangement, and hemangiopericytoma-like appearance with prominent vascularity [7]. Among immunostains, CD34 is especially useful for differentiating SFT from the other spindle-cell neoplasia [5, 6]. England et al. described high cellularity, high mitotic activity (more than 4/10 HPF), pleomorphism, necrosis, and hemorrhagic changes as criteria for morphological malignancy of SFT [5].
Although SFTs are typically benign, they can become malignant, especially if they grow to a large size or repeatedly recur [1, 8, 9]. According to England’s criteria, the current case was also diagnosed as benign at the initial resection, but the metastases were malignant. This change in malignancy bears concern. Although the primary tumor was considered benign, it potentially harbored highly malignant cells. SFT is often a large tumor, and pathological evaluation of all its cells is difficult; therefore, in an otherwise benign SFT, the possibility of malignant cells, or benign cells that could change morphologically over time, cannot be easily ruled out. Because the tumor was large in this case, we followed up with CT every 6 months for 5 years according to the malignant tumor. Lung metastasis has been pointed out by CT 10 years later coincidentally. Currently, there are no rules regarding follow-up. However, we think that it may be better to follow up for 10 years, because there is a possibility of distant recurrence like this time. However, accumulation of more cases is necessary to better understand this rare tumor.
Conclusion
Patients who have had resected SFTs should be carefully followed up, as malignancy may change in distant metastasis, as in this case.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- SFT:
-
Solitary fibrous tumor
References
Gold JS, Antonescu CR, Hajdu C, Ferrone CR, Hussain M, Lewis JJ, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer. 2002;94(4):1057–68.
Baldi GG, Stacchiotti S, Mauro V, Dei Tos AP, Gronchi A, Pastorino U, et al. Solitary fibrous tumor of all sites: outcome of late recurrences in 14 patients. Clin Sarcoma Res. 2013;3:4.
Klemperer P, Coleman BR. Primary neoplasms of the pleura. A report of five cases. Am J Ind Med. 1992;22(1):1–31.
Said JW, Nash G, Banks-Schlegel S, Sassoon AF, Shintaku IP. Localized fibrous mesothelioma: an immunohistochemical and electron microscopic study. Hum Pathol. 1984;15(5):440–3.
England DM, Hochholzer L, McCarthy MJ. Localized benign and malignant fibrous tumors of the pleura. A clinicopathologic review of 223 cases. Am J Surg Pathol. 1989;13(8):640–58.
Maki T, Fujino S, Misu K, Kaneko H, Inomata H, Omi M, et al. Integrally calcified solitary fibrous tumor in the retroperitoneum: a case report and review of the literature. Surg Case Rep. 2016;2(1):14.
Kunieda K, Tanaka Y, Nagao N, Yamaguchi K, Sano J, Osada S, et al. Large solitary fibrous tumor of the retroperitoneum: report of a case. Surg Today. 2004;34(1):90–3.
Kanthan R, Torkian B. Recurrent solitary fibrous tumor of the pleura with malignant transformation. Arch Pathol Lab Med. 2004;128(4):460–2.
Krishnadas R, Froeschle PO, Berrisford RG. Recurrence and malignant transformation in solitary fibrous tumour of the pleura. Thorac Cardiovasc Surg. 2006;54(1):65–7.
Acknowledgements
We thank Marla Brunker and Joe Barber Jr, Ph.D., from Edanz Group (https://en-author-services.edanz.com/), for editing a draft of this manuscript.
Funding
This study was not funded.
Author information
Authors and Affiliations
Contributions
KM wrote the article. KE edited the article. HB supervised the editing of the manuscript. Other remaining co-authors collected the data and discussed the content of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Matsuishi, K., Eto, K., Morito, A. et al. Retroperitoneal fibrous tumor recurring as lung metastases after 10 years: a case report. surg case rep 7, 127 (2021). https://doi.org/10.1186/s40792-021-01209-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-021-01209-4