
Abstract
Background
Torsion of the vermiform appendix is a rare disease with symptoms very similar to those of acute appendicitis. We herein report a case of torsion of the vermiform appendix diagnosed by intraoperative findings.
Case presentation
A 4-year-old boy presented to our hospital because of abdominal pain and vomiting. Laboratory data revealed a C-reactive protein level of 0.08 mg/dL and white blood cell count of 19,300/μL (neutrophils, 88.9%). Abdominal ultrasound showed a target sign-like finding in the ileocecal region. A computed tomography scan showed swelling of the appendix. We performed an emergency operation under suspicion of acute appendicitis. Laparoscopic examination showed that the appendix had twisted 720° in the clockwise direction. Appendectomy was performed, and the postoperative course was uneventful.
Conclusions
Although torsion of the vermiform appendix is a very rare disease and difficult to differentiate from appendicitis, an inappropriate treatment plan could lead to necrosis and perforation of the appendix. It is important to consider this disease as a differential diagnosis in patients with right lower abdominal pain.
Similar content being viewed by others

Background
Torsion of the vermiform appendix is a rare disease with symptoms very similar to those of acute appendicitis. Interval appendectomy for acute appendicitis has recently become popular. However, the use of conservative therapy with antibiotics for torsion of the vermiform appendix can cause necrosis of the appendix, leading to perforation of the appendix and peritonitis.
We herein present a case involving a boy who was admitted under the diagnosis of appendicitis and was subsequently found to have appendiceal torsion on laparoscopy.
Case presentation
A 4-year-old boy presented to the emergency room with abdominal pain. Abdominal ultrasonography (US) revealed no apparent cause of the pain. A massive bowel movement was achieved by an enema and the patient’s pain improved; thus, he was discharged home. However, he developed vomiting and intermittent abdominal pain than night and presented to our hospital again the following day.
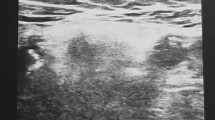
Assessment of the patient’s general appearance indicated that he was very painful, and his body temperature was 37 °C. Physical examination revealed tenderness throughout the entire abdomen with the maximum point in the right lower quadrant. Laboratory data revealed a C-reactive protein level of 0.08 mg/dL and white blood cell count of 19,300/μL (neutrophils, 88.9%). Abdominal US showed target sign-like findings in the ileocecal region (Fig. 1), and these findings were slightly different from the typical findings of intussusception. Enhanced computed tomography (CT) showed a swollen appendix (Fig. 2). An emergency operation was performed under the diagnosis of acute appendicitis.

Ultrasonography of the abdomen. a Axial view of the base of the appendix showed target sign-like appearance. b Longitudinal view showed pseudo-kidney sign

Computed Tomography scan of the abdomen. Swollen appendix (arrow) can be seen
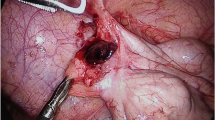
The operation was performed using the conventional three-port laparoscopic technique. Laparoscopy showed that the appendix was swollen and dark red in color and that it had twisted 720° in the clockwise direction at its base (Fig. 3). No adhesion was present between the appendix and surrounding tissues. A routine appendectomy was performed. The operation time was 51 min. Histopathological examination revealed an appendix with the main focus of inflammation in the serosa rather than mucosa. There was no evidence of neoplasia (Fig. 4). The postoperative course was uneventful, and the patient was discharged on the fourth postoperative day.

Laparoscopic finding. The appendix was twisted 720° clockwise direction

Histopathological findings of the appendix (Hematoxylin & Eosin staining). Mononuclear cell infiltration was observed mainly in serosa rather than mucosa, indicating that the possibility of acute appendicitis is low. There was no evidence of neoplasia. (a, original magnification:×40; b, original magnification:×400)
Discussion
Torsion of the vermiform appendix was first reported by Payne in 1918 [1], and sporadic case reports have since been published. A review of the English-language literature revealed only 22 pediatric cases (including our case), which are summarized in Table 1 [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19]. The patients’ ages ranged from 11 weeks to 18 years (mean, 7.6 years). The male/female ratio was 18/4. After admission, observation was adopted in two cases and CT-guided drainage was performed in one case. Emergency operations were performed in all three of these patients because the symptoms did not improve in two patients and a dark, foul-smelling bloody aspirate instead of the expected purulent drainage was obtained in the remaining patient.
Torsion of the vermiform appendix can be primary or secondary. The causes of secondary torsion include mucoceles [3, 20], fecaliths [21], tumors [22, 23], and similar conditions. Possible causes of primary torsion include an abnormal mesentery, such as that with a narrow base, absence of azygotic folds that usually fix the appendix or inflammation; peristaltic bowel movements; the use of laxatives; and vigorous physical exercise. As shown in Table 1, most cases in the pediatric population are primary. In the present case, we found no adhesion between the appendix and the surrounding tissues. Because of the torsion, we could not evaluate the shape of the mesentery. The medical interview revealed that the patient had been playing with a horizontal bar when his symptoms appeared. The enema, which we performed during the first check-up, might have increased the tension within the appendix. Either of these factors could have contributed to the torsion of the vermiform appendix. The pathological examination revealed that the inflammation of the appendix was mainly present in the serosa, not in the mucosal layer, indicating that appendicitis was not the cause of the torsion.
The symptoms of torsion of the vermiform appendix are similar to those of appendicitis. It is difficult to diagnose this entity by preoperative imaging, such as US or CT. In all but one case, the patients were not preoperatively diagnosed with torsion of the appendix. We were also unable to preoperatively diagnose this condition in the present case. In addition to abdominal pain, 17 of 22 patients also developed nausea and vomiting, which may prompt suspicion of other pathogeneses of the abdominal pain. Hamada et al. [20] reported that target-sign like appearance was a useful finding in identifying appendiceal torsion. Although rare, it is important to consider this condition as one of, and if we suspect, the best technique with which to simultaneously diagnose and treat this condition.
The idea of interval appendectomy or nonoperative management for acute appendicitis has recently become popular in the field of pediatrics [24]. The indications for this approach are expanding, and some institutes perform interval appendectomy in both perforated and nonperforated cases. If we adopt this strategy in patients with torsion of the vermiform appendix and treat them with antibiotics, necrosis, and perforation could result. Three cases in which observational treatment was attempted resulted in emergent operation in the end. When we start conservative treatment, we should be aware of the possibility of this rare condition.
Conclusion
Although torsion of the vermiform appendix is a very rare disease and difficult to differentiate from appendicitis, an inappropriate treatment plan could lead to necrosis and perforation of the appendix. Therefore, it is important to consider this disease as a differential diagnosis in patients with right lower abdominal pain.
Availability of data and materials
The dataset supporting the conclusions of this article is included in the article.
Abbreviations
- CT:
-
Computed tomography
- US:
-
Ultrasonography
References
Payne J. A case of torsion of the appendix. Br J Surg. 1918;6:327.
Carter AE. Torsion of the Appendix. Postgrad Med J. 1959;35:671–2.
Chan KP. Volvulus complicating mucocele of the appendix. Br J Surg. 1965;52:713–4.
Ghent WR, Carnovale BV. Primary volvulus of the appendix. Can Med Assoc J. 1966;95:926–7.
Finch DR. Torsion of the appendix. Br J Clin Pract. 1974;28:391–2.
Willan PT, Wickham MH. Torsion of the appendix. Ir J Med Sci. 1983;152:168.
Dewan PA, Woodward A. Torsion of the vermiform appendix. J Pediatr Surg. 1986;21:379.
Waters DJ, Wilson BE, Salow W. Acute appendiceal torsion--a rare surgical entity: report of a case and review of the literature. J Am Osteopath Assoc. 1986;86:224–5.
Merrett ND, Lubowski DZ, King DW. Torsion of the vermiform appendix: a case report and review of literature. Aust N Z J Surg. 1992;62:981–3.
Gilchrist BF. Torsion of the appendix. J Pediatr Surg. 1995;30:901–2.
Val-Bernal JF, González-Vela C, Garijo MF. Primary acute torsion of the vermiform appendix. Pediatr Pathol Lab Med. 1996;16:655–61.
Uroz-Tristan J, García-Urgelles X, Poenaru D, Avila-Suarez R, Valenciano-Fuentes B. Torsion of vermiform appendix: value of ultrasonographic findings. Eur J Pediatr Surg. 1998;8:376–7.
Oğuzkurt P, Oğuzkurt L, Kayaselcuk F, Oz S. An unusual cause of acute abdomen: torsion of colonic duplication over a duplicated appendix. Pediatr Surg Int. 2004;20:722–3.
Gopal K, Kumar S, Grewal H. Torsion of the vermiform appendix. J Pediatr Surg. 2005;40:446–7.
Sarin YK, Pathak D. Torsion of vermiform appendix. Indian Pediatr. 2006;43:266–7.
Montes-Tapia F, Quiroga-Garza A, Abrego-Moya V. Primary torsion of the vermiform appendix and undescended cecum treated by video-assisted transumbilical appendectomy. J Laparoendosc Adv Surg Tech A. 2009;19:839–41.
Perger L, Muensterer OJ. Laparoscopic appendectomy for torsed appendix presenting as an acute abdomen in an infant female. JSLS. 2011;15:565–7.
D'Souza GF, Abdessalam S. Volvulus of the appendix: a case report. J Pediatr Surg. 2011;46:E43–4.
Hirpara DH, Azzie G. Acute torsion and ischemia of the appendix in a young child. J Pediatr Surg Case Rep. 2018;31:77–9.
Hamada T, Kosaka K, Shigeoka N, Hashimoto Y, Yamauchi M, Cho S, et al. Torsion of the appendix secondary to appendiceal mucocele: gray scale and contrast-enhanced sonographic findings. J Ultrasound Med. 2007;26:111–5.
Wani I, Kitagawa M, Rather M, Singh J, Bhat G, Nazir M. Torsion of vermiform appendix with fecalith: a case report. Cases J. 2008;1:20.
Kitagawa M, Kotani T, Yamano T, Tsurudome H, Hatakeyama T, Kuriu Y, et al. Secondary torsion of vermiform appendix with mucinous cystadenoma. Case Rep Gastroenterol. 2007;1:32–7.
Grebic D, Lovasic F, Benjak I, Lovasic I. Secondary torsion of vermiform appendix with mesoappendiceal lipoma. Ann Saudi Med. 2015;35:173–5.
Gorter RR, The SML, Gorter-Stam MAW, Eker HH, Bakx R, van der Lee JH, et al. Systematic review of nonoperative versus operative treatment of uncomplicated appendicitis. J Pediatr Surg. 2017;52:1219–27.
Acknowledgments
We thank Angela Morben, DVM, ELS, from Edanz Group (www.edanzediting.com/ac), for editing a draft of this manuscript.
Funding
None of the authors received any funding for this study.
Author information
Authors and Affiliations
Contributions
KE drafted the manuscript, and KS and AH critically revised the manuscript. MS and YM supervised the writing of the manuscript. KS and KE performed the operation and perioperative management of the patient. YY performed the histopathological evaluation of the specimen of the appendix. MS and YM supervised the management of the patient. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the family of the patient for publication of this case report.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Endo, K., Sato, M., Saga, K. et al. Torsion of vermiform appendix: case report and review of the literature. surg case rep 6, 6 (2020). https://doi.org/10.1186/s40792-020-0771-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-020-0771-x