
Abstract
Background
Chronic hepatitis is a major public health problem. Hepatitis B virus is the primary cause, and Hepatitis B and C together are responsible for 60% of cirrhosis and 80% of hepatocellular carcinomas. This study measured the prevalence of HBsAg among Senegalese military to develop an appropriate strategy to prevent cirrhosis and hepatocellular carcinoma.
Methods
We conducted a descriptive cross-sectional study among Senegalese military aged 25 to 60 years. A sample of 1224 participants was selected following a two-level-stratification. The mark of surface HBs antigen using chemiluminescence concerned 1195 participants. The presence of HBsAg was analyzed according to age, marital status, alcohol consumption and glomerular filtration rate. Epi-info6fr and R software were used, respectively, for data capture and analyses. A Chi-square test was performed to compare proportions considering a significance level of 5% and a confidence interval of 95%.
Results
The average age was 39.8 ± 9.2 years. Participants in the age groups of 25–34 years, 45–60 years and 35–44 years were respectively 30.7%, 34.4% and 34.9% of the sample. Married persons represented 82.6% of participants and 17.08% were single. Most participants were educated (99%), and 56% had reached at least secondary school level. Alcohol consumption was at 11.5%. The HBsAg prevalence rate was 10.8% [9.1% to 12.7%] with a significant difference between age groups (P < 0.001), which ranged from 5.6% for 45–60 years, 9.62% for 25–34 years to 16.9% for 35–44 years. Marital status and alcohol consumption did not affect the carriage of HBsAg. HBsAg prevalence was more common among participants who had a glomerular filtration rate greater than 90 ml/min. Transaminases rate exceeded the normal threshold for 43 participants (3.6%); the increase was 6.6% [2.7% to 11.8%] for HBsAg carriers and 3.2% [1.2% to 6.7%] for alcohol users.
Conclusions
The high prevalence of HBsAg in the military requires the implementation of an effective prevention and care program to reduce the risk of cirrhosis and hepatocellular carcinoma and contribute to reducing the burden of communicable diseases, such as hepatitis and HIV/AIDS, and non-communicable diseases.
Similar content being viewed by others

Background
Chronic viral hepatitis is a worldwide major public health problem, particularly in developing countries that are facing a range of barriers to contain the epidemic [1-5]. Approximately 9% of the world population is suffering from chronic hepatitis. Lemoine et al. [1] reported that 350–400 million of the 550 million people who were infected were infected by the hepatitis B virus (HBV), 170–180 million by the hepatitis C virus (HCV) and 15 million were due to the hepatitis D virus (HDV) [1,6-8]. The poorest regions are the most affected [1,9]. HBV and HCV are responsible for 60% of cirrhosis and 80% of hepatocellular carcinomas, with more than one million deaths annually, mainly in disadvantaged areas [1,6,8,10]. These figures illustrate the role of hepatitis B, which are also confirmed by other authors. The WHO estimates that 2 billion people are infected with HBV worldwide and approximately 380 million are chronic carriers (6% of the world population). Approximately 4.5 million new infections occur annually, and 620,000 deaths due to HBV are reported worldwide [1,11]. The prevalence of HBV is estimated between 8%-15% in endemic areas, such as Africa [1,12,13]. The prevalence in the general population in Senegal was estimated as 11% in 2012 according to the Ministry of Health. One study of pregnant women at the Military Hospital of Ouakam, between 2006 and 2009, showed a prevalence of HBV of 11.6% [14], which indicates the importance of the presence of the virus in the Senegalese general population.
This high prevalence justifies the implementation of a national program against hepatitis and the integration of the vaccine in the Expanded Immunization Program.
The fight against viral hepatitis B is not well structured in the army. The current situation of infection prevalence is unknown. Therefore, one of the objectives of this study was to determine the prevalence of HBsAg in the military to develop strategies for cirrhosis and hepatocellular carcinoma prevention.
Methods
We performed a descriptive and analytical cross-sectional study in the Senegalese military in the period from May 2013 to February 2014.
Military aged men 25 to 60 years who were present in the country during the survey were included in the study.
Soldiers who had less than 2 years of duty in the military or were unable to answer the questions were excluded.
The enrolled population was divided into three (3) age groups: 25–34, 35–44 and 45–60 years. The survey was conducted in all Senegalese regions.
The sample size was calculated in the framework of STEPS investigation in the military, which provided an estimate of 1,296 men who were divided into three strata. Each member was consistently linked to only one training unit. Therefore, we proceeded with a first selection to determine the number of respondents in each training unit using the human resources central database. A second simple random sampling was performed from the local unit file to identify participants for each stratum.
Information regarding the socio-demographic (age, gender, ethnicity, marital status, educational level, ranks…) and behavioral characteristics (alcohol) of the subjects were collected using a revised STEPS questionnaire [15].
For each participant, 5 ml of venous blood taken from the elbow crease were collected in a dry test tube and centrifuged. Sera were decanted and maintained at 4°C if the analyses were not performed within 4 hours.
HBsAg was initially detected using the DETERMINE HBs Agkit ® (Alere) and ARCHITECT HBsAg QUANTITATIVE II (Abbott Diagnostics) ®. In a second step, measurement of transaminases (AST and ALT) was performed using the controller from Biochemistry Cobas400 ® of Roche Diagnostic laboratories and the Spectrophotometer CYPRESS diagnostic ®.
Chronic renal disease was defined by a glomerular filtration rate expressed in ml per min. The assessment of the glomerular filtration rate (GFR) was performed using the Modification of Diet in Renal Disease (MDRD) formula [16]. Two stages were identified: Stage 1 represented a GFR value greater than 90 ml/min and Stage 2 a GFR between 60 and 90 ml / min [17,18].
Biochemical results were reported on the questionnaire.
Data were entered in Epi-info6 software and analyzed using R software. The Chi-square test was performed to compare proportions with 5% for the significance level and 95% for the confidence interval (CI).
Participation was voluntary. Each participant signed a consent letter at the beginning of the investigation and had the opportunity to stop participating at any stage of the process. All results were returned to the subjects, and participants who were detected as HBs antigen carriers were referred to specialists for treatments.
Results
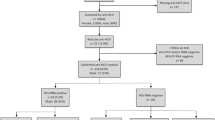
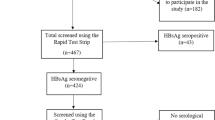
Instead of the 1,296 participants who were planned to be involved in the survey, 1,224 soldiers were enrolled, and 1,195 were tested for HBsAg and transaminase levels. The lack of HBsAg research for 29 participants was related to the mobility of soldiers and stock out of test, while not their status.
The mean age was 39.8 years, and it was equal to the median (normal distribution). The sample consisted mostly of men with a sex ratio of 31.2, which followed the personnel structure in the armed forces. Soldiers were more represented (48.0%), followed by non-commissioned officers (45.6%) and officers (6.4%). Most participants were married (82.6%), singles represented 17.08% and other 0.32% of the sample. Serere (25.0%) and Ouolof (24.3%) ethnic groups were more frequent, followed by Diola (18.3%) and Pulaar (16.3%). Almost all respondents were literate (99.1%), and 56.0% had at least achieved secondary level at school (See Table 1).
The GFR identified two stages of chronic kidney disease (CKD) among participants: it was higher than 90 ml per min for 68% of participants (CKD stage 1) and between 60 and 90 ml per min for 32% (CKD stage 2).
The prevalence of HBsAg was estimated at 10.8% [9.1% to 12.7%], and it varied significantly between the different age groups (P < 0.001). It was 9.62% [6.8% to 13.1%], 16.90% [13.4% to 20.8%] and 5.60% [3.6% to 8.3%] for the age groups 25–34, 35–44 and 45–60 years, respectively (see Figure 1).

Prevalence rate of HBsAg carriers according to age group among tested Senegalese soldiers.
Table 2 shows that the carriage of HBsAg was not influenced by ethnic group, marital status and alcohol consumption (P > 0.05). However, it was significantly higher among participants who were classified as GFR stage 1 (12.3%) compared to GFR stage 2 (7.7%) with a p-value equal to 0.023. Similarly, the frequency was different according to rank and was greater for the soldiers (13.6%) than non-commissioned officers (7.9%).
Transaminase rates were higher than the normal threshold in 43 participants (3.6%); it was 6.6% [2.7% to 11.8%] among carriers of HBsAg and 3.2% [1.2% to 6.7%] among drinkers. However, an increase two times greater than normal was exceptional.
Discussion
HBsAg prevalence is a public health problem, especially in sub-Saharan Africa [5,19]. An area is classified as a highly endemic area of hepatitis B [20,21] when HBsAg seroprevalence is higher than 8% for adults. Kiire et al. estimated the prevalence of hepatitis B in sub-Saharan Africa between 9% and 12% [19], and the results of this study confirmed that estimate. Indeed, the prevalence of HBsAg was 10.8%, which shows the high endemicity of hepatitis B among Senegalese troops. This result correlated with the observed prevalence in the general population (11%) in 2012 according to the Ministry of Health [22,23], but it is lower than the prevalence among men (21%) stated by Lo et al. in 2014 [23]. The difference in the figures may be due to different target groups these studies on HBsAg. Our study targeted subjects who were apparently in good health, but the study conducted by Gora was based on sick patients who were admitted to the laboratory for further investigation. The current practice in Senegal is the performance of exploratory tests to confirm a clinical diagnosis. Therefore, there may be an overestimation of the prevalence compared to the general population. In fact, the observed prevalence of HBsAg in pregnant women (11.57%), who are representative of the general population, corroborates this hypothesis [14].
A study in Nigeria estimated an HBV seroprevalence 14.6% with a higher frequency in the 20-30-year-old age group [20]. Our study showed a slightly lower prevalence with a higher frequency among 35–44 year-olds. Other authors had already reported a prevalence of HB antigens that was higher among young adults aged 20 to 30 years [14,20]. The hypothesis stated for this finding was that there were more frequent sexual activities among young people. In our study, participants aged 35–44 years were more affected. The decreased prevalence rate in the elders might be related to the impact of condom use campaigns and the extensive ongoing National Hepatitis Program.
The military is considered a gateway group for sexually transmitted diseases (STDs) and HIV/AIDS. The observed prevalence of HBsAg in this study confirms the results of the national survey of combined HIV surveillance in the military, which had shown prevalence figures identical to the general population [24].
HBsAg seroprevalence was 12.3% and 7.7% in participants with CKD stage 1 and stage 2, respectively. Diouf et al. [25] reported an HBsAg seroprevalence (6.7%) among patients receiving dialysis at Aristide Le Dantec Hospital in Dakar (Senegal) that was comparable to our patients with CKD stage 2.
Some authors attempted to link the carrying of HBsAg and CKD [26-30]. In our study, 23.3% of patients with HBsAg were CKD stage 2 versus 33.6% in patients who were seronegative. These results need further investigation in a cohort or case–control study to elucidate the causality.
Limitations
This study was conducted among soldiers who were selected through incorporation screening based on comprehensive clinical data that satisfied medical fitness criteria to serve in the armed forces. However, this medical screening did not include liver function tests. Accordingly, symptomatic carriers should have been eliminated. In addition, the sample was essentially composed of men. The cross-sectional nature of the study did not allow a demonstration of a causal relationship
Conclusion
The highly endemic HBsAg prevalence mentioned in this study is similar to the prevalence in the general population. This finding makes sense because no specific measures were taken to expect a different situation until now. The detection of HBsAg is not yet introduced into the army incorporation screening.
The interest of this work was to promote the introduction of Hepatitis B prevention in the overall fight against non-communicable diseases in the army program and communicable diseases, such as HIV/AIDS and hepatitis. Conducting awareness campaigns among the military, periodic screening, improving access to treatment and the training of health personnel will be the major components of this program, which seeks to reduce cirrhosis and hepatocellular carcinoma morbidity and mortality and the burden of non-communicable diseases.
Abbreviations
- CI:
-
Confidence interval
- CKD:
-
Chronic kidney disease
- GFR:
-
Glomerular filtration rate
- HBV:
-
Hepatitis B virus
- HCV:
-
Hepatitis C virus
- HDV:
-
Hepatitis D virus
- MDRD:
-
Modification of Diet in Renal Disease
- STDs:
-
Sexually transmitted diseases
References
Lemoine M, Nayagam S, Thursz M. Viral hepatitis in resource-limited countries and access to antiviral therapies. Future Virol. 2013;8:371–80.
Jemal A, Bray F, Forman D, O’Brien M, Ferlay J, Center M, et al. Cancer burden in Africa and opportunities for prevention. Cancer. 2012;118:4372–84.
Zanetti AR, Van Damme P, Shouval D. The global impact of vaccination against hepatitis B: a historical overview. Vaccine. 2008;26:6266–73.
Allain JP, Candotti D, Soldan K, Sarkodie F, Phelps B, Giachetti C, et al. The risk of hepatitis B virus infection by transfusion in Kumasi, Ghana. Blood. 2003;101(6):2419–25.
WHO. Global status report on noncommunicable diseases 2010. Geneva; 2011. Available at: http://whqlibdoc.who.int/publications/2011/9789240686458_eng.pdf (accessed on 25 February 2015).
Lavanchy D. Evolving epidemiology of hepatitis C virus. Clin Microbiol Infect. 2011;17(2):107–15.
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–917.
WHO. Hepatitis B. http://www.who.int/csr/disease/hepatitis/HepatitisB_whocdscsrlyo2002_2.pdf (Accessed 25 February 2015).
UN Development Program. http://hdr.undp.org/sites/default/files/hdr14_statisticaltables.xls (Accessed 25 February 2015).
International Agency for Research on Cancer. GLOBOCAN factsheet 2008. http://globocan.iarc.fr/ia/World/atlas.html (Accessed 25 February 2015).
WHO. Prevention and control of viral hepatitis infection: framework for global action. http://www.who.int/csr/disease/hepatitis/GHP_framework.pdf (Accessed 25 February 2015).
El-Serag HB. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology. 2012;142(6):1264–73.
de Martel C, Ferlay J, Franceschi S, Vignat J, Bray F, Forman D, et al. Global burden of cancers attributable to infections in 2008: a review and synthetic analysis. Lancet Oncol. 2012;13(6):607–15.
Lo G, Diawara PS, Diouf NN, Faye B, Seck MC, Sow K, et al. Prévalence de l’antigène de surface du virus de l’hépatite B (AgHBs) chez les femmes enceintes au laboratoire de l’Hôpital Militaire de Ouakam (HMO), Dakar. Med Afr Noire. 2012;5905:241–4.
World Health Organization. Instrument STEPS de l’OMS pour la surveillance des facteurs de risque des maladies chroniques(STEPS). http://www.who.int/chp/steps/en/ (Accessed 25 February 2015).
Cockcroft DW, Gault MH. Memorial University Research Unit, The General Hospital, St. John’s, Newfoundland A1 A 1E5 (Canada). Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41.
National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification and stratification. Am J Kidney Dis. 2002;39:S1–266.
Agence Nationale d’Accréditation et d’Évaluation en Santé. Diagnostic de l’insuffisance rénale chronique chez l’adulte. Recommandations pour la pratique clinique. Paris: ANAES; 2002. p. 124.
Kiire CF. The epidemiology and prophylaxis of hepatitis B in sud-saharan Africa: a review from tropical and subtropical Africa. J Gastroenterol Hepatol. 1996;38:S5–12.
Uneke CJ, Ogbu O, Inyama PU, Anyanwu GI, Njoku MO, Idoko JH. Prevalence of hepatitis-B surface antigen among blood donors and human immunodeficiency virus-infected patients in Jos, Nigeria. Mem Inst Oswaldo Cruz. 2005;100:13–6.
Hodges M, Sanders E, Aitken C. Seroprevalence of hepatitis markers: HAV, HBV, HCV, and HBV amongst primary school children in Freetown Sierra Leone. West Afr J Med. 1998;17:36–7.
Programme National de lutte contre les hépatites (PNLH). Ministère de la Santé et de l’action sociale, Sénégal. http://www.hepatites.sn/le-pnlh/les-hepatites-au-senegal.html (Accessed 25 February 2015).
Lo G, Diouf NN, Sow-Sall A, Ndiaye-Diop H, Diawara PS, Faye B, et al. Prévalence de l’antigène de surface du virus de l’hépatite B au laboratoire de l’hôpital militaire de Ouakam entre 2006 et 2010. Med Afr Noire. 2014;6102:87–93.
Conseil National de Lutte contre le Sida, Sénégal, Dakar. Rapport national de surveillance combinée du VIH/sida dans les Armées. 2006;1:1-194
Diouf ML, Diouf B, Niang A, Ka EH, Pouye A, Seck A, et al. Prevalence of hepatitis B and C viruses in a chronic hemodialysis center in Dakar. Dakar Med. 2000;45(1):1–4.
Huang JF, Chuang WL, Dai CY, Ho CK, Hwang SJ, Chen SC, et al. Viral hepatitis and proteinuria in an area endemic for hepatitis B and C infections: another chain of link? J Intern Med. 2006;260:255–62.
Mocroft A, Neuhaus J, Peters L, Ryom L, Bickel M, Grint D, et al. Hepatitis B and C co-infection are independent predictors of progressive kidney disease in HIV-positive, antiretroviral-treated adults. PLoS One. 2012;7(7):e40245. doi:10.1371/journal.pone.0040245.
Lee JJ, Lin MY, Yang YH, Lu SN, Chen HC, Hwang SJ. Association of hepatitis C and B virus infection with CKD in an endemic area in Taiwan: a cross-sectional study. Am J Kidney Dis. 2010;56:23–31. PubMed Abstract | Publisher Full Text.
Lai KN, Li PK, Lui SF, Au TC, Tam JS, Tong KL, et al. Membranous nephropathy related to hepatitis B virus in adults. N Eng J Med. 1991;324:1457–63 [PubMed].
George E, Nadkarni GN, Estrella MM, Lucas GM, Sperati CJ, Atta MG, et al. The impact of hepatitis C coinfection on kidney disease related to human immunodeficiency virus (HIV): a biopsy study. Medicine (Baltimore). 2011;90:289–95 [PubMed].
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors conceived, designed, conducted and wrote the study. NAA analyzed the data. All the authors also read and approved the final manuscript
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Ndiaye, A.A., Fall, I.S., Lo, G. et al. HBsAg seroprevalence among Senegalese militaries. Military Med Res 2, 5 (2015). https://doi.org/10.1186/s40779-015-0032-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40779-015-0032-7