
Abstract
Thyroid eye disease (also known as Graves’ ophthalmopathy) is a complex orbital inflammatory disease, which can be sight threatening, debilitating and disfiguring. This overview discusses the epidemiology, risk factors, pathogenesis, presentation, ophthalmic clinical features, investigations and treatment of thyroid eye disease.
Similar content being viewed by others


The beauty of a woman must be seen from her eyes, because that is the doorway to her heart, the place where love resides.
Audrey Hepburn
Introduction
Thyroid eye disease (TED) is a complex orbital inflammatory disease, which can be sight threatening, debilitating and disfiguring. TED is also known as Graves’ ophthalmopathy, named after Robert J. Graves, an Irish physician who first described thyrotoxicosis in a woman presenting with goitre, rapid heartbeat and exophthalmos [1].
The acute progression of the disease is an ocular emergency, particularly optic nerve compression and corneal disease secondary to exposure. Most patients with TED have biochemical evidence of hyperthyroidism with the most common cause being Graves’ disease. However, TED may occur in patients who have hypothyroidism (most commonly Hashimoto’s thyroiditis) or euthyroidism. Hence, the timing of TED presentation may differ between patients. There are patients wherein thyroid dysfunction precedes TED development; there are patients in whom thyroid dysfunction and TED present at the same time, and there are patients where TED is the first manifestation, preceding thyroid dysfunction [2],[3].
Review
Epidemiology
The incidence of TED is 16 per 100,000 females and 2.9 per 100,000 males with an approximate prevalence of 0.25% with no significant ethnic predisposition [4]. The higher preponderance in females relates to the higher incidence of hyperthyroidism in females. However, for severe TED, the ratio of females to males reverses to approximately 1:4 [5].
Risk factors
Risk factors for the disease include female gender, middle age and smoking [6]. Smoking increases the risk of TED by 7–8 times [2] and it reduces the effectiveness of treatments [7]. There have been reports suggesting that polymorphisms in genes such as human leukocyte antigen (HLA), cytotoxic T-lymphocyte antigen 4 (CTLA4), interleukin 23 receptor (IL23R), protein tyrosine phosphatase nonreceptor 22 (PTPN22), CD40, CD86, thyroglobulin (Tg) and thyroid stimulating hormone receptor (TSHR) increase the risk of TED [8],[9]. However, reported associations may vary considerably between different populations and the majority of studies lack adequate sample size and power to detect associations with occurrence and severity of TED. Thus, although variations in genes, especially those encoding immunological factors, have been associated with TED, large and well controlled studies are required to determine the exact contribution of gene variations. A large recent study by Yin et al. concluded that patients with TED do not have a distinct genetic susceptibility to their eye disease and suggested that environmental and/or epigenetic influences are at play [10]. In addition, mechanical factors and orbital anatomy have been suggested to influence the occurrence and clinical course of TED [11].
In autoimmune cases of Graves' disease or Hashimoto's thyroiditis, there is also an increased prevalence and relative risk for coexisting autoimmune disorders [12]. Examples include rheumatoid arthritis, pernicious anaemia, systemic lupus erythematosus, Addison's disease, coeliac disease, and vitiligo. Hence, it is important to screen for other autoimmune diseases if subjects with autoimmune thyroid disease present with new or nonspecific symptoms.
Pathogenesis
TED is caused by retro-orbital inflammation to which orbital fibroblast activation is a key contributor. Fibroblast activation is presumed to occur secondary to stimulatory auto-antibodies [anti-TSHR and anti-insulin-like growth factor-1 (IGF-1)] [13]. These fibroblasts express the TSH receptor and produce extracellular matrix components and pro-inflammatory molecules. Further, there is an infiltration of immunocompetent T-helper cells (type-1), B lymphocytes, macrophages and mast cells [14]. Inflammation of the extraocular muscles can lead to restricted eye movements and proptosis. The optic nerve can be compressed which can cause optic neuropathy resulting in permanent visual loss.
However, there are situations when TSHR antibodies are not present, such as in cases of Hashimoto’s thyroiditis and eye disease and euthyroid Graves’ disease [15]. In addition, autoimmunity against the eye muscle antigen calsequestrin and the orbital connective tissue antigen collagen XIII plays a role in the pathogenesis of TED [15]-[17].
A unique feature of TED in comparison to other autoimmune diseases is that it is self-limiting. The suggested reason is the absence of lymphoid tissue (and hence, lymphoid neogenesis) within the orbit [18]. The disease commences with an active (inflammatory) phase with rapidly worsening symptoms and signs, reaching a point of maximum severity which then improves to a static plateau but does not resolve to baseline (inactive phase). This is known as Rundle’s curve [19] and can be plotted graphically for each patient but is rarely performed in practice. Rather, precise clinical documentation of the severity and activity of the disease is usually preferred.
Presentation
In approximately 40% of patients with TED, the ocular and systemic symptoms have a simultaneous onset [20]. Approximately 60% of patients with hyperthyroidism will develop TED. For those with TED, 85% have hyperthyroidism, 10% have hypothyroidism and 5% are euthyroid [21].
Ophthalmic clinical features
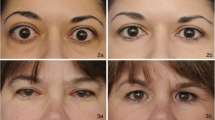
Symptoms include: dry eyes, red eyes, diplopia, pain on eye movement and cosmetic changes. Signs include: proptosis (exophthalmos), lid retraction, lid lag on downgaze, chemosis, conjunctival injection, orbital fat prolapse, keratopathy, periorbital swelling, restrictive myopathy and optic neuropathy [22]. However, the most common clinical sign is eyelid retraction (occurs in 90% of patients with TED), followed by exophthalmos (60%) and eye movement restrictions (40%) [23].
The two most serious signs are optic neuropathy and exposure keratopathy as both can abruptly lead to blindness and are therefore ocular emergencies. There are a number of grading systems available in an attempt to document the severity and activity of the disease such as the NOSPECS classification [24] and Mourits system [25]. However, such classifications tend only to be used for research purposes. Other grading systems include The European Group on Graves’ Orbitopathy (EUGOGO) protocol for assessment of Graves’ orbitopathy [26] and the VISA classification (V – vision, optic neuropathy; I – inflammation, congestion; S – strabismus, motility restriction; A – appearance, exposure).
Investigations
Investigations include thyroid function tests [TSH, free T4 and free T3 (if strong clinical suspicion but normal TSH and free T4)], thyroid auto-antibodies (anti-TSH receptor, anti-thyroid peroxidase and anti-Tg antibodies), orbital imaging [magnetic resonance imaging (MRI) is better for identifying active disease (muscle bellies show inflammation and enlargement with spared tendons) whereas computed tomography (CT) is better for bone resolution when planning decompression surgery], visual field analysis, orthoptic assessment and optometric assessment. It is also important to consider the use of questionnaires to assess traits such as quality of life, which can be markedly underestimated [27]. Examples of questionnaires used include the GO-QOL [28] and TED-QOL [29].
Treatment of TED
Treatment should be multidisciplinary with the ophthalmologist, endocrinologist, radiologist, optometrist, orthoptist and general physician (GP). The principal aim should be thyroid function control as this is associated with a reduction in the severity of TED. General supportive measures should be immediately implemented or considered including the use of ocular lubricants, head elevation (gravity supports lid closure), taping lids closed at night, prisms in spectacles (to control diplopia), tinted spectacles (to hide eye appearance), counselling and support groups.
In the active phase of TED, systemic corticosteroids are considered and are most effective early in this phase, which prevents most of the morbidity associated with the disease. Other agents including ciclosporin, azathioprine, methotrexate, infliximab and rituximab are gaining popularity and some are the subject of clinical trials [14]. Selenium supplementation may also be used as it has been shown to significantly improve quality of life, reduce ocular involvement, and slow progression in patients with mild Graves' orbitopathy [30]. Orbital radiotherapy can be used as an adjunctive therapy and is particularly effective at improving ocular motility during active disease, due to the sensitivity of orbital lymphocytes to radiotherapy [31]. Rarely, surgical orbital decompression is required in cases of acute progressive optic neuropathy or exposure keratopathy.
Surgery for the improvement of cosmetic appearance and symptoms (e.g. diplopia) should be avoided if possible until the inactive phase (end of Rundle’s curve). The surgical options include decompression, motility and lid surgery (in that order). Decompression aims to improve proptosis and lid position. Motility surgery involves extraocular muscle repositioning to reduce or eliminate diplopia and/or abnormal head postures. Finally, lid surgery is used to reposition the lid(s).
Treatment of hyperthyroidism
There are three main options in the treatment of hyperthyroidism: medical (carbimazole and propylthiouracil), radioactive iodine and surgery (ablation and thyroidectomy). Medical treatment blocks the production of thyroid hormones and is used until the patient is euthyroid. The drug is then tapered whilst maintaining normal free T4 levels. Alternatively a ‘block and replace’ regime may be used where higher drug doses are used along with thyroxine replacement. The major risk of this treatment is agranulocytosis. Radioactive iodine (single dose) is an effective alternative option but subsequent hypothyroidism is common. However, this treatment can cause progression of TED by a leakage of antigens from the thyroid gland, again eliciting an autoimmune response [3]. This risk can be reduced with the simultaneous use of corticosteroids [32]. Surgery is less commonly performed but may be used for patients with a large goitre.
Conclusion
TED is a self-limiting orbital inflammatory condition with an active (inflammatory) and inactive phase. Risk factors include female gender, middle age and smoking. The majority of patients with TED have hyperthyroidism with the most common cause being Graves’ disease. There are numerous ophthalmic features; the two most serious being optic neuropathy and exposure keratopathy. Investigations include thyroid function, thyroid auto-antibodies, orbital imaging, visual field analysis, orthoptic assessment, and optometric assessment. There are a number of grading systems available to assess severity and to monitor activity of the disease. Management should be multidisciplinary with the ophthalmologist, endocrinologist, radiologist, optometrist, orthoptist and general practitioner.
References
Graves RJ: Clinical Lectures. London Medical and Surgical Journal. 1835, 7: 516-517.
Perros P, Neoh C, Dickinson J: Thyroid eye disease. BMJ. 2009, 338: b560-10.1136/bmj.b560.
Bahn RS: Graves' ophthalmopathy. N Engl J Med. 2010, 362: 726-738. 10.1056/NEJMra0905750.
Lazarus JH: Epidemiology of Graves' orbitopathy (GO) and relationship with thyroid disease. Best Pract Res Clin Endocrinol Metab. 2012, 26: 273-279. 10.1016/j.beem.2011.10.005.
Perros P, Crombie AL, Matthews JN, Kendall-Taylor P: Age and gender influence the severity of thyroid-associated ophthalmopathy: a study of 101 patients attending a combined thyroid-eye clinic. Clin Endocrinol (Oxf). 1993, 38: 367-372. 10.1111/j.1365-2265.1993.tb00516.x.
Sikder S, Weinberg RS: Thyroid eye disease: pathogenesis and treatment. Ophthalmologica. 2010, 224: 199-203. 10.1159/000260224.
Wiersinga WM: Smoking and thyroid. Clin Endocrinol (Oxf). 2013, 79: 145-151. 10.1111/cen.12222.
Maheshwari R, Weis E: Thyroid associated orbitopathy. Indian J Ophthalmol. 2012, 60: 87-93. 10.4103/0301-4738.94048.
Jacobson EM, Tomer Y: The CD40, CTLA-4, thyroglobulin, TSH receptor, and PTPN22 gene quintet and its contribution to thyroid autoimmunity: back to the future. J Autoimmun. 2007, 28: 85-98. 10.1016/j.jaut.2007.02.006.
Yin X, Latif R, Bahn R, Davies TF: Genetic profiling in Graves' disease: further evidence for lack of a distinct genetic contribution to Graves' ophthalmopathy. Thyroid. 2012, 22: 730-736. 10.1089/thy.2012.0007.
Stan MN, Bahn RS: Risk factors for development or deterioration of Graves' ophthalmopathy. Thyroid. 2010, 20: 777-783. 10.1089/thy.2010.1634.
Boelaert K, Newby PR, Simmonds MJ, Holder RL, Carr-Smith JD, Heward JM, Manji N, Allahabadia A, Armitage M, Chatterjee KV, Lazarus JH, Pearce SH, Vaidya B, Gough SC, Franklyn JA: Prevalence and relative risk of other autoimmune diseases in subjects with autoimmune thyroid disease. Am J Med. 2010, 123: 183-10.1016/j.amjmed.2009.06.030. e181-189
Smith TJ, Hegedus L, Douglas RS: Role of insulin-like growth factor-1 (IGF-1) pathway in the pathogenesis of Graves' orbitopathy. Best Pract Res Clin Endocrinol Metab. 2012, 26: 291-302. 10.1016/j.beem.2011.10.002.
Verity DH, Rose GE: Acute thyroid eye disease (TED): principles of medical and surgical management. Eye (Lond). 2013, 27: 308-319. 10.1038/eye.2012.284.
Lahooti H, Parmar KR, Wall JR: Pathogenesis of thyroid-associated ophthalmopathy: does autoimmunity against calsequestrin and collagen XIII play a role?. Clin Ophthalmol. 2010, 4: 417-425.
McCorquodale T, Lahooti H, Gopinath B, Wall JR: Long-term follow-up of seven patients with ophthalmopathy not associated with thyroid autoimmunity: heterogeneity of autoimmune ophthalmopathy. Clin Ophthalmol. 2012, 6: 1063-1071.
Ardley M, McCorquodale T, Lahooti H, Champion B, Wall JR: Eye findings and immunological markers in probands and their euthyroid relatives from a single family with multiple cases of thyroid autoimmunity. Thyroid Res. 2012, 5: 4-10.1186/1756-6614-5-4.
Naik VM, Naik MN, Goldberg RA, Smith TJ, Douglas RS: Immunopathogenesis of thyroid eye disease: emerging paradigms. Surv Ophthalmol. 2010, 55: 215-226. 10.1016/j.survophthal.2009.06.009.
Rundle FF: Management of exophthalmos and related ocular changes in Graves' disease. Metabolism. 1957, 6: 36-48.
Bahn RS, Heufelder AE: Pathogenesis of Graves' ophthalmopathy. N Engl J Med. 1993, 329: 1468-1475. 10.1056/NEJM199311113292007.
Soeters MR, van Zeijl CJ, Boelen A, Kloos R, Saeed P, Vriesendorp TM, Mourits MP: Optimal management of Graves orbitopathy: a multidisciplinary approach. Neth J Med. 2011, 69: 302-308.
Denniston AKO, Murray PI: Oxford Handbook of Ophthalmology. Second edition. ᅟ: Oxford University Press; 2009.
Bartley GB, Fatourechi V, Kadrmas EF, Jacobsen SJ, Ilstrup DM, Garrity JA, Gorman CA: Clinical features of Graves' ophthalmopathy in an incidence cohort. Am J Ophthalmol. 1996, 121: 284-290. 10.1016/S0002-9394(14)70276-4.
Wiersinga WM, Prummel MF, Mourits MP, Koornneef L, Buller HR: Classification of the eye changes of Graves' disease. Thyroid. 1991, 1: 357-360. 10.1089/thy.1991.1.357.
Mourits MP, Koornneef L, Wiersinga WM, Prummel MF, Berghout A, van der Gaag R: Clinical criteria for the assessment of disease activity in Graves' ophthalmopathy: a novel approach. Br J Ophthalmol. 1989, 73: 639-644. 10.1136/bjo.73.8.639.
Wiersinga WM, Perros P, Kahaly GJ, Mourits MP, Baldeschi L, Boboridis K, Boschi A, Dickinson AJ, Kendall-Taylor P, Krassas GE, Lane CM, Lazarus JH, Marcocci C, Marino M, Nardi M, Neoh C, Orgiazzi J, Pinchera A, Pitz S, Prummel MF, Sartini MS, Stahl M, von Arx G: Clinical assessment of patients with Graves' orbitopathy: the European Group on Graves' Orbitopathy recommendations to generalists, specialists and clinical researchers. Eur J Endocrinol. 2006, 155: 387-389. 10.1530/eje.1.02230.
Khadka J, McAlinden C, Pesudovs K: Quality assessment of ophthalmic questionnaires: review and recommendations. Optom Vis Sci. 2013, 90: 720-744. 10.1097/OPX.0000000000000001.
Terwee CB, Gerding MN, Dekker FW, Prummel MF, Wiersinga WM: Development of a disease specific quality of life questionnaire for patients with Graves' ophthalmopathy: the GO-QOL. Br J Ophthalmol. 1998, 82: 773-779. 10.1136/bjo.82.7.773.
Fayers T, Dolman PJ: Validity and reliability of the TED-QOL: a new three-item questionnaire to assess quality of life in thyroid eye disease. Br J Ophthalmol. 2011, 95: 1670-1674. 10.1136/bjophthalmol-2011-300487.
Marcocci C, Kahaly GJ, Krassas GE, Bartalena L, Prummel M, Stahl M, Altea MA, Nardi M, Pitz S, Boboridis K, Sivelli P, von Arx G, Mourits MP, Baldeschi L, Bencivelli W, Wiersinga W: Selenium and the course of mild Graves' orbitopathy. N Engl J Med. 2011, 364: 1920-1931. 10.1056/NEJMoa1012985.
Bartalena L, Marcocci C, Tanda ML, Rocchi R, Mazzi B, Barbesino G, Pinchera A: Orbital radiotherapy for Graves' ophthalmopathy. Thyroid. 2002, 12: 245-250. 10.1089/105072502753600223.
Bartalena L, Marcocci C, Bogazzi F, Panicucci M, Lepri A, Pinchera A: Use of corticosteroids to prevent progression of Graves' ophthalmopathy after radioiodine therapy for hyperthyroidism. N Engl J Med. 1989, 321: 1349-1352. 10.1056/NEJM198911163212001.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author declares that he has no competing interests.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
McAlinden, C. An overview of thyroid eye disease. Eye and Vis 1, 9 (2014). https://doi.org/10.1186/s40662-014-0009-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40662-014-0009-8