
Abstract
Background
In refractory out-of-hospital cardiac arrest, the patient is commonly transported to hospital with mechanical continuous chest compressions (CCC). Limited data are available on the optimal ventilation strategy. Accordingly, we compared arterial oxygenation and haemodynamics during manual asynchronous continuous ventilation and compressions with a 30:2 compression-to-ventilation ratio together with the use of 10 cmH2O positive end-expiratory pressure (PEEP).
Methods
Intubated and anaesthetized landrace pigs with electrically induced ventricular fibrillation were left untreated for 5 min (n = 31, weight ca. 55 kg), after which they were randomized to either the CCC group or the 30:2 group with the the LUCAS® 2 piston device and bag-valve ventilation with 100% oxygen targeting a tidal volume of 8 ml/kg with a PEEP of 10 cmH2O for 35 min. Arterial blood samples were analysed every 5 min, vital signs, near-infrared spectroscopy and electrical impedance tomography (EIT) were measured continuously, and post-mortem CT scans of the lungs were obtained.
Results
The arterial blood values (median + interquartile range) at the 30-min time point were as follows: PaO2: 180 (86–302) mmHg for the 30:2 group; 70 (49–358) mmHg for the CCC group; PaCO2: 41 (29–53) mmHg for the 30:2 group; 44 (21–67) mmHg for the CCC group; and lactate: 12.8 (10.4–15.5) mmol/l for the 30:2 group; 14.7 (11.8–16.1) mmol/l for the CCC group. The differences were not statistically significant. In linear mixed models, there were no significant differences between the groups. The mean arterial pressures from the femoral artery, end-tidal CO2, distributions of ventilation from EIT and mean aeration of lung tissue in post-mortem CTs were similar between the groups. Eight pneumothoraces occurred in the CCC group and 2 in the 30:2 group, a statistically significant difference (p = 0.04).
Conclusions
The 30:2 and CCC protocols with a PEEP of 10 cmH2O resulted in similar gas exchange and vital sign outcomes in an experimental model of prolonged cardiac arrest with mechanical compressions, but the CCC protocol resulted in more post-mortem pneumothoraces.
Similar content being viewed by others

Background
International cardiopulmonary resuscitation (CPR) guidelines recommend continuous ventilations with an advanced airway at a rate of 10–12 breaths per minute. When using a supraglottic airway device and there is a significant leak, a 30:2 ratio of compressions to ventilations is preferred [1, 2]. In cases of out-of-hospital cardiac arrest (OHCA), where return of spontaneous circulation (ROSC) is not achieved on scene, the patient is commonly transported to hospital with ongoing CPR. In these situations, mechanical chest compression devices are recommended to ensure rescuer safety and provide high-quality compressions [3, 4]. Nonetheless, even with a secured airway and the use of an FiO2 of 1.0, many patients arriving at hospital have severe hypoxia, hypercarbia and acidosis on blood gas analysis [5,6,7,8]. This may predispose patients to brain injury and life-threatening lung and immunological reactions in those who achieve ROSC or in whom ECPR is initiated.
Even though mechanical compression devices provide superior perfusing pressures in comparison to manual compressions [9], their effect on ventilation strategies is less known [10, 11]. During patient transport, when providing manual chest compressions is difficult or impossible, using a mechanical chest compression device has been shown to improve compression quality [3, 4]. But using a mechanical compression device could impair ventilatory performance because of dynamic air trapping [12] and atelectasis formation. Previously, we compared the 30:2 protocol with continuous chest compressions (CCC) in an experimental CPR model of prolonged resuscitation [13] and found no statistically significant differences between the study groups.
One option to improve gas exchange is the use of positive end-expiratory pressure (PEEP) in delivering ventilation. Experimental studies have suggested improved oxygenation with PEEP [14,15,16] but it has not been conclusively studied in the setting of prolonged CPR using mechanical chest compressions. In the current study, we compared oxygenation and ventilation between continuous compressions and a 30:2 compression-to-ventilation ratio, together with the use of 10 cmH2O of PEEP. We hypothesized that a 30:2 compressions to ventilation ratio would provide higher better oxygenation than continuous compressions and ventilation. The primary endpoint of this study was the levels of oxygen over time between the two groups. The secondary endpoints included arterial levels of carbon dioxide and lactate, brain oxygenation analysed with NIRS over time, the distribution of ventilation with electrical impedance tomography (EIT) recordings and post-mortem computed tomography (CT) scans.
Materials and methods
We conducted this experimental animal study on healthy landrace pigs (n = 31, both sexes) at the Laboratory Animal Centre, Large Animals Unit at the Viikki Campus of the University of Helsinki between May 2021 and December 2022. The study was approved by the Finnish National Animal Experiment Board (ESAVI/ 4121/2021). The study is reported in adherence to the ARRIVE guidelines [17], and a checklist is included in Additional file 1.
Preparation and monitoring
The fasted animals were premedicated with intramuscular injections of medetomidine (9–10 mg) and racemic ketamine (450–500 mg). An IV line was inserted into an ear vein, and anaesthesia was induced with IV propofol (dose 1–1.5 mg/kg) and fentanyl (3–4 mcg/kg), after which endotracheal intubation was performed (internal diameter 6.0–7.0 mm). Mechanical ventilation was started (Servo Ventilator 900C, Siemens-Elema, Solna, Sweden) with 21% oxygen (O2) and an end-tidal carbon dioxide (EtCO2) target of 5%. The internal jugular vein and femoral artery were cannulated (arrow, size 8.5 Fr. 16 cm, Teleflex Medical Europe Ltd, Westmeath, Ireland and Avanti+, size 6F, length 11 cm, Cordis, Tipperary, Ireland, respectively), and baseline blood samples were taken. A temporary pacemaker wire was inserted next, and the right ventricular location was confirmed with the achievement of ventricular pacing (Medtronic 5348 Single Chamber Temporary Pacemaker, Soma Tech INTL, Bloomfield, CT, USA).
Arterial blood samples were analysed with a point-of-care device (i-STAT System, Abbott Laboratories, Princeton, NJ, USA), and haemodynamic and respiratory variables, including spirometry, were monitored using a Datex-Ohmeda AS/3 monitor with a M-COVX gas module (GE Healthcare, Helsinki, Finland) and recorded using data collection software (iCentral® and S/5 Collect®, GE Healthcare, Helsinki, Finland). A rectal temperature probe was inserted, and a normal temperature of 38 °C–39 °C was targeted with the use of warm blankets when necessary. Cerebral oximetry was performed with NIRS (INVOS TM5100C Cerebral Oximeter, Somanetics Inc., Troy, MI, USA) with one sensor in the forehead and another on the belly as a control. The EIT belt was set around the chest just caudal to the compression device piston. The hair under the belt was shaved off, and the skin was cleaned with 70% ethanol to ensure the best possible conductivity. The EIT data were recorded with a Dräger Pulmovista® 500 (Drägerwerk AG & Co., Lübeck, Germany) and analysed with a Dräger SW EITdiag V1.6 (Drägerwerk AG & Co., Lübeck, Germany).
Experimental procedures
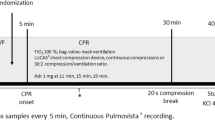
Figure 1 presents the experiment timeline. After VF was induced with a 9 V direct current, ventilation and anaesthesia were ceased and the pacing wire was removed. Randomization into the study groups of either CCC or the 30:2 protocol was performed with sealed opaque envelopes during the 5-min hands-off period. In the meantime, a Lucas 2® compression device (Jolife AB, part of Stryker, Lund, Sweden) was set up and the position of the pig was stabilized with a vacuum mattress and a handful of towels within the Lucas 2® arch. Manual bag-valve ventilation (LAERDAL Silicone Resuscitator, Laerdal Medical, Stavanger, Norway) was performed with 100% oxygen, either with a frequency of around 10 min−1 in the CCC group or twice during the compression pause in the 30:2 group, targeting an approximate tidal volume of 500 ml in both groups. The PEEP of 10 cmH2O was adjusted with an Ambu® PEEP valve (Ambu A/S, Ballerup, Denmark). Adrenaline was administered as a 1 mg IV dose at 11-, 15- and 19-min time points. A 20-s recording break from compressions for the EIT was held at the 30-min time point with continuous ventilation in both groups for the duration. Arterial blood samples were collected at 5-min intervals, and a venous sample was also taken at the 30-min time point. Monitoring, NIRS and EIT were recorded continuously through the experiment. The animals were killed with a 40 mmol dose of potassium chloride at the 40-min time point. Simultaneously, the intubation tube was clamped after insufflating the lungs with one full manual ventilation. The post-mortem CT scans were collected in the prone position approximately 15 min after the cessation of CPR.

Timeline of the experimental protocol. Adr adrenaline, FiO2 fraction of inhaled oxygen, VF ventricular fibrillation, CPR cardiopulmonary resuscitation, KCl potassium chloride, CT computed tomography
Data processing
An illustration of the EIT analysis is provided in Fig. 2. Sections of interest were chosen from the raw recording (baseline, cardiac arrest and 5-min intervals throughout the CPR). The reconstruction settings are provided in Additional file 2. The reconstructed sections were analysed using automated methods provided by the analysis software to create visual slices and quantified data. The global tidal impedance change (dzGlo) was referenced to the 5-min section, except for the 30-min section, which was referenced to the baseline section. The ventral to dorsal (V/D) distribution indices were computed, as illustrated in Fig. 2. A V/D value of 1 represents an equal distribution of ventilation, and a value of 0 means that all tidal change happens dorsally.

Schematic illustration of the EIT analysis work chart. A The raw dzGlo curve. B The reconstructed sections after filtering. C Visual slices created with the automated analysis scheme from filtered sections. D Visual explanation of the V/D index. BL baseline, dzGlo global impedance change, TID tidal impedance change, CA cardiac arrest, V/D ventral to dorsal
The CT scans were evaluated by a veterinary radiologist (ML) blinded to the intervention group with Osirix MD version 12.5.0 (VetCT, Cambridge, UK). The Hounsfield unit (HU) values were measured from 10 lung slices chosen as described by Reske et al. [18]. The first slice was chosen from the most cranial aspect of the lungs, where both the left and right cranial lobes are visible on the same transverse slice. The most caudal slice was chosen similarly where there was still enough lung on both hemithoraces for segmentation into 2–3 segments, but where the accessory lobe was no longer visible. Eight evenly spaced slices were chosen from between them.
An illustrative figure of HU measurements is provided in Additional file 3. The lung parenchyma was manually delineated separately for the hemithoraces and accessory lobes. The measured mean HU values for each hemithorax, normalized to the area of the delineation, were used to calculate the mean HU of the overall lung. The hemithoraces were also divided into 2–3 ventro-dorsal segments of equal height, and representative HU values of these segments were averaged for the dorsal, middle and ventral HU values without normalization to area. Subjects with more than a mild pneumothorax were excluded from the analysis because of the dislocated anatomy.
Statistical analysis and sample size
For the sake of clarity, all variables are reported as medians and interquartile ranges (IQRs), since most variables violated the assumptions of parametric testing. Single comparisons were tested with the Mann–Whitney U test for statistical significance. Comparisons with multiple time point measurements were tested with a linear mixed-effects model and a heterogeneous Toeplitz covariance matrix. The effects of the interventional group, time and interaction between time and the intervention group were included in the model. The values over time were plotted as medians and IQRs.
The sample size was estimated based on arterial blood gas data from Kim et al. [19]. According to their data, a sample size of 30 divided into two equal groups would be sufficient to detect a 20 mmHg difference in PaO2 with a statistical power of 0.80 and an alpha of 0.05.
As an exploratory analysis, we also compared the results of the PEEP zero pigs from our previous study [13] to the PEEP 10 pigs of the current study.
Results
We randomized 31 animals (30:2 group: n = 16; CCC group: n = 15). Persisting agonal breathing until the 30-min time point was witnessed in 2 pigs in the 30:2 group and in 6 pigs in the CCC group. We encountered no cases of spontaneous ROSC. Most animals deteriorated to ASY soon after the perfusing pressures withered.
There were no significant differences in the baseline characteristics (Table 1). The FiO2, peak airway pressure or compliance levels during advanced life support (ALS) were similar between the groups (Table 2).
Oxygen, carbon dioxide, lactate, mean arterial pressure, end-tidal carbon dioxide and near-infrared spectroscopy
The arterial blood oxygen, carbon dioxide, lactate and mean arterial pressure (MAP) results are shown in Fig. 3. There were no statistically significant differences between the groups in PaO2 (p = 0.51), PaCO2 (p = 0.42), lactate (p = 0.26) and MAP (p = 0.98) or in the time and group interaction terms in the PaO2 (p = 0.80), PaCO2 (p = 0.15), lactate (p = 0.80) and MAP levels (p = 0.17).

Arterial oxygen pressures (PaO2), carbon dioxide pressures (PaCO2), lactate levels and mean arterial pressures during experimental cardiopulmonary resuscitation shown as medians and interquartile ranges. The p value is given for a linear mixed model between the groups. CCC continuous chest compressions
The EtCO2 levels (Fig. 4) were similar between the groups (p = 0.28). The p value for the group and time interaction was 0.028.

EtCO2 levels of the 30:2 and CCC groups during experimental cardiopulmonary resuscitation shown as medians and interquartile ranges. The p value is given for a linear mixed model between the groups. EtCO2 end-tidal carbon dioxide, CCC continuous chest compressions
The cerebral NIRS values are presented in Fig. 5. One subject from the 30:2 group was removed from the analysis because of clearly abnormal measurement values, suggesting technical failure in the measurement. There was no significant difference between the groups (p = 0.96) or between the time and group interaction terms (p = 0.36).

NIRS values during experimental cardiopulmonary resuscitation shown as medians and interquartile ranges. The p value is given for a linear mixed model between the groups. NIRS near-infrared spectroscopy, rSO2 regional oxygen saturation index, CA cardiac arrest, CCC continuous chest compressions
Electrical impedance tomography and computed tomography
The main findings from the EIT data are reported in Table 3. One subject had missing data from the baseline measurement in the CCC group. There were no statistically significant differences in the recorded tidal impedance changes between the groups, although there was a nonsignificant trend of the CCC group having more dorsally distributed impedance changes in all the measurements. Figure 2 depicts the analysis method used to obtain the reported values.
Regarding the CT data, one pig in the CCC group did not have the planned scan due to logistical problems. There were no statistically significant differences between the groups in the number of rib fractures, mean lung density of the lungs or regional mean densities (V/D regions reported). One pig in the 30:2 group and 5 pigs in the CCC group were excluded from the HU analysis because of deformed lung anatomy due to pneumothoraces.
Table 3 shows the distribution of the different severity classes of pneumothoraces; 8/10 of the pneumothoraces accumulated in the CCC group and the finding reached statistical significance (p = 0.04 with Fisher’s exact test.)
Exploratory analyses
We analysed the non-randomized comparisons of the primary outcomes (PaO2, PaCO2, lactate, EtCO2 and MAP) of our prior experiment [13] to our current experiment, creating groups of PEEP = 0 cmH2O and PEEP = 10 cmH2O (n = 30 and 31, respectively). The results are reported in Additional file 4. The PaO2 levels were significantly higher and the PaCO2 levels were lower in the PEEP 10 cmH20 group compared to the PEEP 0 cmH2O group. Lactate, MAP and EtCO2 levels were similar.
We also compared the PaO2 levels between the 30:2 groups, the CCC groups and the 30:2 PEEP = 10cmH2O with CCC PEEP = 0 cmH2O (also in Additional file 4). The PaO2 levels were significantly higher in the 30:2 PEEP 10 cmH2O group compared to the 30:2 PEEP 0 cmH2O, but not compared to the CCC PEEP 0 cmH2O. The CCC PEEP 10 and PEEP 0 cmH2O groups had similar PaO2 levels. The p values were obtained with a linear mixed model.
Discussion
Key findings
Contrary to our primary hypothesis, we found no significant differences in arterial blood gases or lactate between CCC and a 30:2 CPR ratio when a PEEP of 10 cmH2O was used. Regarding the secondary outcomes, the haemodynamic markers and EtCO2 levels were similar between the groups, nor were there any significant differences in the distribution of ventilation or mean lung densities. However, there were significantly more pneumothoraces in the CCC group. These findings suggest that when using PEEP, the CCC and 30:2 protocols during prolonged CPR result in comparable oxygenation and ventilation.
Relationship to previous studies
Limited patient data on intra-arrest ventilation in patients receiving mechanical chest compressions are available. Mechanical compression devices do not appear to improve survival in patients compared to manual compressions [10], and according to experimental data, their use may be linked to ventilation problems and lung injury [12, 20]. Some previous studies have investigated the use of PEEP as a means of improving oxygenation. One trial on the use of PEEP during CPR with pigs was performed in 1980, showing improved ventilation at the cost of reduced carotid blood flow [16]. This early study was performed with 3:1 and 5:1 compression-to-ventilation ratios. Ruemmler et al. [21] compared guideline-recommended CCC with asynchronous ventilation with and without a PEEP of 5 cmH2O PEEP in a porcine model. They found no differences in intra-arrest gas exchange or pulmonary shunting, but found less shunting immediately post-ROSC with the use of PEEP and less immunological mRNA activity in brain tissue samples obtained after ROSC. The intra-arrest peak pressures remained lower with PEEP.
Renz et al. [15] studied the effect of PEEP 8 mbar and 16 mbar on both conventional and ultralow tidal volume ventilation protocols in a prolonged experimental model similar to ours. Within the conventional protocols with varying PEEP levels, they found significant improvements in PaO2 levels with 8 mbar of PEEP. In addition, they found lower driving pressures and less post-mortem lung tissue sample trauma findings with 8 compared to 0 mbar of PEEP. Interestingly, the PEEP 16 mbar group had quite poor PaO2 in their final measurement point of 25 min, possibly suggesting deleterious intrathoracic pressure development, even though this did not influence the MAP values. The measured level of shunting remained reasonably low in the study with all groups. Also, Levenbrown et al. [14] reported rising PaO2 with increasing PEEP (0–5–10–15–20 cmH2O) and dose-dependent decreases in measured CO (cardiac output) with rising PEEP levels. They found optimal DO2 (oxygen delivery to tissue) with a PEEP level of 5 cmH2O.
Comparing our primary outcome results to our previous study in the same setting [13], the findings of higher PaCO2 and EtCO2 levels in the 30:2 protocol were not reproduced in this experiment. The PaO2 levels throughout the experiment were significantly higher in the 30:2 group with PEEP than without it (figures and statistics reported in Additional file 4). In the CCC group, paO2 was similar with and without PEEP. This points to the possibility of positive effects of PEEP when added to the 30:2 protocol, but not with the CCC protocol, contrary to some previous findings by other research groups. The possible benefit to ventilatory performance in the 30:2 protocol with the added PEEP possibly results from the prevention of atelectasis formation during the compression phase. In future, it could be worthwhile to research the 30:2 protocol with continuous ventilations preserving the short compression breaks for uninterrupted ventilations.
Mälberg et al. [22] recently published a 20-min experimental CPR model comparing CCC and 30:2 with monitoring focussed on airway pressures and tidal volumes and found peak airway pressures rising higher in the CCC group when the tidal volumes were strictly kept similar between the groups. The CO2 levels were lower in the arterial samples and expiratory gases and pH were higher in the CCC group, reinforcing the trends found in our previous work.
Study strengths and limitations
The landrace pig is the most established model animal of CPR, and we used fairly large animals resembling more mature anatomy and physiology. The current study utilized a model of prolonged CPR. The importance of ventilatory performance in ALS is pronounced when the cardiac arrest time exceeds 10 min and rising PaCO2 levels start to cause acidosis, which makes the heart more resistant to defibrillations and possibly results in an aggravated insult to brain tissue, derangements of cerebral blood flow and more pronounced general immunological reactions analogous to a trauma-induced DO2 debt [23]. Research on ECPR has demonstrated that CPR times with a low-flow state last up to 60 min amongst recruited patients [24], and we believe that our experimental setup modelled this situation with clinical relevance.
We note certain limitations of this experimental study. The variance between our subjects remained high, especially after prolonged CPR (> 15 min). This may relate to factors influencing the efficiency of blood flow, such as small compression point variations [25, 26]. A clinically more relevant experimental model ideally should be extended to as long as 60 min of CPR. In the current model we did however often experience loss of systemic perfusion pressure within the 20–30 min frame based on a drop in EtCO2, deterioration of VF to asystole and increasing lactate, hypoxia and hypercarbia contradicting the timeframe expansion.
Also, the occurrence of agonal breaths seemed to affect oxygenation, but these may occur in humans as well. The thoracic anatomy differs markedly from humans and some phenomena seen in this study may not be relevant to patient work. The pig anatomy may predispose it to more trauma from compressions.
We found no significant differences in the peak airway pressures. Ventilations were provided by a member of the team and it is possible that in case of increased resistance, the rescuer used less force. On the other hand, this may correspond to the clinical situation.
In this experiment, we chose the prearrest recording as the reference section in the EIT analysis for the 30-min compression break recording after realizing that the intra-arrest recordings of our study groups differed too much to provide a reasonable reference point for this more uniform recording point. The distribution of ventilation seemed more dorsally distributed, especially in the CCC group, compared to our previous study. Part of this is probably due to the accumulation of pneumothoraces in the CCC group because the formation of a pneumothorax shifts the distribution dorsally.
The capability of the EIT to produce spatial discrimination was probably reduced due to the untypical tidal ventilatory pattern of two sequential ventilations with a long pause during compressions with the 30:2 protocol. We explored the effect of insufflating the lungs and clamping the endotracheal tube at the end of experiment on the findings in CT scans by re-insufflating the lungs after the first scans and performing a second CT scan round. With some subjects, the atelectatic lung regions differed significantly between these two rounds, depicting the still dynamic state of lung aeration post-mortem and possibly reducing the discriminatory power.
Conclusions
Our study suggests no difference in arterial blood levels of oxygen, carbon dioxide or lactate, haemodynamics or the distribution of ventilation with compression-to-ventilation ratios of 30:2 compared to CCC during prolonged CPR with 10 cmH2O PEEP.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALS:
-
Advanced life support
- CCC:
-
Continuous chest compressions
- CPR:
-
Cardiopulmonary resuscitation
- CT:
-
Computed tomography
- DO2 :
-
Oxygen delivery to tissues
- ECPR:
-
Extracorporeal cardiopulmonary resuscitation
- EIT:
-
Electrical impedance tomography
- EtCO2 :
-
End-tidal carbon dioxide
- FiO2 :
-
Fraction of inspired oxygen
- HU:
-
Hounsfield unit
- IQR:
-
Interquartile range
- MAP:
-
Mean arterial pressure
- NIRS:
-
Near-infrared spectroscopy
- OHCA:
-
Out-of-hospital cardiac arrest
- PaCO2 :
-
Partial pressure of carbon dioxide
- PaO2 :
-
Partial pressure of oxygen
- PEEP:
-
Positive end-expiratory pressure
- ROSC:
-
Return of spontaneous circulation
- V/D:
-
Ventral to dorsal
- VF:
-
Ventricular fibrillation
References
Soar J, Böttiger BW, Carli P et al (2021) European Resuscitation council guidelines 2021: adult advanced life support. Resuscitation 161:115–151. https://doi.org/10.1016/j.resuscitation.2021.02.010
Panchal AR, Bartos JA, Cabañas JG et al (2020) Part 3: adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 142:S366–S468. https://doi.org/10.1161/CIR.0000000000000916
Magliocca A, Olivari D, De Giorgio D et al (2019) LUCAS versus manual chest compression during ambulance transport: a hemodynamic study in a porcine model of cardiac arrest. J Am Heart Assoc. https://doi.org/10.1161/JAHA.118.011189
Bekgöz B, Şan İ, Ergin M (2020) Quality comparison of the manual chest compression and the mechanical chest compression during difficult transport conditions. J Emerg Med 58:432–438. https://doi.org/10.1016/J.JEMERMED.2019.11.045
Daou O, Winiszewski H, Besch G et al (2020) Initial pH and shockable rhythm are associated with favorable neurological outcome in cardiac arrest patients resuscitated with extracorporeal cardiopulmonary resuscitation. J Thorac Dis 12:849. https://doi.org/10.21037/JTD.2019.12.127
Shou BL, Ong CS, Premraj L et al (2023) Arterial oxygen and carbon dioxide tension and acute brain injury in extracorporeal cardiopulmonary resuscitation patients: Analysis of the extracorporeal life support organization registry. J Heart Lung Transplant 42:503–511. https://doi.org/10.1016/j.healun.2022.10.019
Nelskylä A, Skrifvars MB, Ångerman S, Nurmi J (2022) Incidence of hyperoxia and factors associated with cerebral oxygenation during cardiopulmonary resuscitation. Resuscitation 170:276–282. https://doi.org/10.1016/J.RESUSCITATION.2021.10.001
Spindelboeck W, Gemes G, Strasser C et al (2016) Arterial blood gases during and their dynamic changes after cardiopulmonary resuscitation: a prospective clinical study. Resuscitation 106:24–29. https://doi.org/10.1016/J.RESUSCITATION.2016.06.013
Axelsson C, Karlsson T, Axelsson ÅB, Herlitz J (2009) Mechanical active compression-decompression cardiopulmonary resuscitation (ACD-CPR) versus manual CPR according to pressure of end tidal carbon dioxide (P(ET)CO2) during CPR in out-of-hospital cardiac arrest (OHCA). Resuscitation 80:1099–1103. https://doi.org/10.1016/J.RESUSCITATION.2009.08.006
Rubertsson S, Lindgren E, Smekal D et al (2014) Mechanical chest compressions and simultaneous defibrillation vs conventional cardiopulmonary resuscitation in out-of-hospital cardiac arrest: the LINC randomized trial. JAMA 311:53–61. https://doi.org/10.1001/JAMA.2013.282538
Perkins GD, Lall R, Quinn T et al (2015) Mechanical versus manual chest compression for out-of-hospital cardiac arrest (PARAMEDIC): a pragmatic, cluster randomised controlled trial. The Lancet 385:947–955. https://doi.org/10.1016/S0140-6736(14)61886-9
Rezoagli E, Magliocca A, Grieco DL et al (2022) Impact of lung structure on airway opening index during mechanical versus manual chest compressions in a porcine model of cardiac arrest. Respir Physiol Neurobiol. https://doi.org/10.1016/J.RESP.2021.103807
Kopra J, Litonius E, Pekkarinen PT et al (2023) Ventilation during continuous compressions or at 30:2 compression-to-ventilation ratio results in similar arterial oxygen and carbon dioxide levels in an experimental model of prolonged cardiac arrest. Intensive Care Med Exp. https://doi.org/10.1186/S40635-022-00485-0
Levenbrown Y, Hossain MJ, Keith JP et al (2020) The effect of positive end-expiratory pressure on cardiac output and oxygen delivery during cardiopulmonary resuscitation. Intensive Care Med Exp. https://doi.org/10.1186/S40635-020-00330-2
Renz M, Müllejans L, Riedel J et al (2022) High PEEP levels during CPR improve ventilation without deleterious haemodynamic effects in pigs. J Clin Med. https://doi.org/10.3390/JCM11164921
Hodgkin BC, Lambrew CT, Lawrence FH, Angelakos ET (1980) Effects of PEEP and of increased frequency of ventilation during CPR. Crit Care Med 8:123–126. https://doi.org/10.1097/00003246-198003000-00005
du Sert NP, Ahluwalia A, Alam S et al (2020) Reporting animal research: explanation and elaboration for the ARRIVE guidelines 2.0. PLoS Biol 18:e3000411. https://doi.org/10.1371/JOURNAL.PBIO.3000411
Reske AW, Reske AP, Gast HA et al (2010) Extrapolation from ten sections can make CT-based quantification of lung aeration more practicable. Intensive Care Med 36:1836–1844. https://doi.org/10.1007/S00134-010-2014-2/TABLES/4
Kim YW, Il KH, Hwang SO et al (2018) Single ventilation during cardiopulmonary resuscitation results in better neurological outcomes in a porcine model of cardiac arrest. Yonsei Med J 59:1232–1239. https://doi.org/10.3349/YMJ.2018.59.10.1232
Magliocca A, Rezoagli E, Zani D et al (2021) Cardiopulmonary resuscitation–associated lung edema (CRALE): a translational study. Am J Respir Crit Care Med 203:447–457. https://doi.org/10.1164/rccm.201912-2454OC
Ruemmler R, Ziebart A, Kuropka F et al (2020) Bi-Level ventilation decreases pulmonary shunt and modulates neuroinflammation in a cardiopulmonary resuscitation model. PeerJ 8:e9072. https://doi.org/10.7717/peerj.9072
Mälberg J, Marchesi S, Spangler D et al (2023) Continuous chest compressions are associated with higher peak inspiratory pressures when compared to 30:2 in an experimental cardiac arrest model. Intensive Care Med Exp. https://doi.org/10.1186/S40635-023-00559-7
Bjerkvig CK, Strandenes G, Eliassen HS et al (2016) “Blood failure” time to view blood as an organ: how oxygen debt contributes to blood failure and its implications for remote damage control resuscitation. Transfusion (Paris) 56(Suppl 2):S182–S189. https://doi.org/10.1111/TRF.13500
Belohlavek J, Smalcova J, Rob D et al (2022) Effect of intra-arrest transport, extracorporeal cardiopulmonary resuscitation, and immediate invasive assessment and treatment on functional neurologic outcome in refractory out-of-hospital cardiac arrest: a randomized clinical trial. JAMA 327:737–747. https://doi.org/10.1001/JAMA.2022.1025
Teran F, Owyang CG, Martin-Flores M et al (2023) Hemodynamic impact of chest compression location during cardiopulmonary resuscitation guided by transesophageal echocardiography. Crit Care 27:319. https://doi.org/10.1186/s13054-023-04575-7
Marshall RA, Morton JS, Luchkanych AMS et al (2022) Left ventricle chest compression improves ETCO2, blood pressure, and cerebral blood velocity in a swine model of cardiac arrest and cardiopulmonary resuscitation. Resusc Plus. https://doi.org/10.1016/J.RESPLU.2022.100326
Acknowledgements
The authors wish to thank Olli Valtanen for expert technical help with the experiments.
Funding
Open Access funding provided by University of Helsinki (including Helsinki University Central Hospital). This study was supported by academic grants from Sigrid Juselius Stiftelse (Grant recipient MBS), Svenska Kulturfonden, Medicinska Understödsföreningen Liv och Hälsa and Finska Läkaresällskapet.
Author information
Authors and Affiliations
Contributions
MBS, EL, JK and PTP planned the study. All the authors but ML took part in the experiments. ML performed the CT image analysis. JK performed the data processing and statistical analysis. JK, MBS and EL prepared a first draft of the manuscript. All authors have read and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Finnish National Animal Experiment Board (ESAVI/16960/2020).
The study is reported in adherence to the ARRIVE guidelines.
Consent for publication
Not applicable.
Competing interests
MBS reports speaker fees from BARD Medical (Ireland). The other authors state that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
The Arrive Checklist and notations of adherence concerning the manuscript.
Additional file 2.
The reconstruction options used to process the raw global change in impedance data.
Additional file 3.
An illustrative image of the workflow used to obtain the mean and regional HU values within one lung CT slice. The lungs have been delineated. The mean HU values of each hemithorax and the accessory lobe are multiplied the according area and the sum of these values divided by the sum of the areas to obtain the mean HU value of the lung tissue in the whole CT slice. The regional mean HU values are obtained as the sum of HU values of the according region divided by the amount of summed regions.
Additional file 4.
The exploratory analyses performed using the current dataset and the prior dataset of our group [13].
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
Cite this article
Kopra, J., Litonius, E., Pekkarinen, P.T. et al. Oxygenation and ventilation during prolonged experimental cardiopulmonary resuscitation with either continuous or 30:2 compression-to-ventilation ratios together with 10 cmH20 positive end-expiratory pressure. ICMx 12, 36 (2024). https://doi.org/10.1186/s40635-024-00620-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40635-024-00620-z