
Abstract
Background
The aim of this study is to evaluate the impact of commonly administered sedatives (Propofol, Alfentanil, Fentanyl, and Midazolam) and vasopressor (Dobutamine, Ephedrine, Noradrenaline and Vasopressin) agents on cerebrovascular reactivity in moderate/severe TBI patients. Cerebrovascular reactivity, as a surrogate for cerebral autoregulation was assessed using the long pressure reactivity index (LPRx). We evaluated the data in two phases, first we assessed the minute-by-minute data relationships between different dosing amounts of continuous infusion agents and physiological variables using boxplots, multiple linear regression and ANOVA. Next, we assessed the relationship between continuous/bolus infusion agents and physiological variables, assessing pre-/post- dose of medication change in physiology using a Wilcoxon signed-ranked test. Finally, we evaluated sub-groups of data for each individual dose change per medication, focusing on key physiological thresholds and demographics.
Results
Of the 475 patients with an average stay of 10 days resulting in over 3000 days of recorded information 367 (77.3%) were male with a median Glasgow coma score of 7 (4–9). The results of this retrospective observational study confirmed that the infusion of most administered agents do not impact cerebrovascular reactivity, which is confirmed by the multiple linear regression components having p value > 0.05. Incremental dose changes or bolus doses in these medications in general do not lead to significant changes in cerebrovascular reactivity (confirm by Wilcoxon signed-ranked p value > 0.05 for nearly all assessed relationships). Within the sub-group analysis that separated the data based on LPRx pre-dose, a significance between pre-/post-drug change in LPRx was seen, however this may be more of a result from patient state than drug impact.
Conclusions
Overall, this study indicates that commonly administered agents with incremental dosing changes have no clinically significant influence on cerebrovascular reactivity in TBI (nor do they impair cerebrovascular reactivity). Though further investigation in a larger and more diverse TBI patient population is required.
Similar content being viewed by others
Background
Guideline-based care for moderate/severe traumatic brain injury (TBI) patients use various pharmacological agents as the cornerstones of treatment. Sedation agents are employed to manage intracranial pressure (ICP), facilitate patient management and suppress cerebral metabolic demand [1,2,3]. Vasopressor agents are utilized to maintain cerebral perfusion pressure (CPP) targets, commonly at approximately 60–70 mmHg [3]. Despite these agents being utilized in care, a refined understanding of the momentary cerebral responses to these agents is limited, with only a small number of studies assessing their impact in TBI [4, 5].
The pressure reactivity index (PRx; correlation between slow-wave of ICP and mean arterial pressure (MAP)) is the most common measure of cerebrovascular reactivity in TBI [6,7,8], with multiple studies linking impaired cerebrovascular reactivity and poor patient outcome [9,10,11,12,13,14]. Furthermore, current therapies guided by the Brain Trauma Foundation (BTF), which includes the use of sedative and vasopressor agents, have demonstrated a limited impact on cerebrovascular reactivity [12, 15,16,17]. Thus, cerebrovascular reactivity monitoring, and its derived metrics, may offer a route to improve patient outcome and may play an important role in cerebral physiologic dysfunction [16, 18].
Currently within the literature there are only a few studies that have assessed the impact of guideline-based therapeutics on cerebrovascular reactivity, with most studies using large time aggregate data, which may miss high-frequency physiological associations [5, 12, 15, 16, 19, 20]. Moreover, the Collaborative European NeuroTrauma Effectiveness Research in TBI (CENTER-TBI) study documented that therapeutic intensity levels (TIL) had little connection to impaired cerebrovascular reactivity, further questioning the role of these agents [16]. Finally, two studies on small populations of critically ill patients found that incremental changes in sedative and vasopressor agents failed to provoke significant responses in cerebrovascular reactivity [4, 5]. Although, again besides from these last two studies, previous work conducted used aggregates of physiology and medication administration data which lacked high temporal resolution (relying on daily treatment measures) [21, 22].
Thus, to both improve therapeutic care and improve the management of CPP and ICP, it is imperative that analyses clearly document the temporal impacts of current therapeutics on cerebrovascular response. As such, the goal of this study was to assess the influence that some commonly utilized sedative and vasopressor agents have on PRx, with a secondary interest in the impact that such agents have on cerebral physiology (primarily ICP). All of this will be accomplished using archived high-frequency physiology data and treatment information from the Department of Neurosurgery, Karolinska University Hospital.
Materials and methods
Study design
Patients with moderate to severe TBI (diagnosed as GCS ≤ 8 and > 15 years old) admitted to the neurointensive care unit at Karolinska University Hospital, Stockholm, Sweden, a level one trauma center, between January 1, 2006 to December 31, 2019 were included in this study. These patients had invasive ICP monitoring and archived high-frequency physiology (ICP and arterial blood pressure; ABP) and were retrospectively analyzed (N = 475) in this observational study. Patients received treatment according to local guidelines in general concordance to that of the Brain Trauma Foundation (BTF) [3, 23, 24], and is described in detail elsewhere [25]. Note all patients were mechanically ventilated and PaCO2 targets were used, where normal to mild hyperventilation (defined here as PaCO2 4.5–5 kPa) was commonly applied as one of several measures to manage increased ICP. Heads are commonly elevated 30 degrees. CPP is calculated with the arterial pressure dome placed at the mid cerebral level.
IRB ethics
Study was approved by the Swedish Ethical Review Authority (#2020-05227) on November 17, 2020 and adheres to the Helsinki Declaration of 1975.
Data collection
For this ongoing prospective TBI database, all patient demographics, injury and treatment information were either manually collected by a medical professional or automatically recorded using Clinisoft (Centricity Critical Care, CCC, General Electric Company, Boston). The drug infusion rates and physiological variables were recorded with Clinisoft, which included the timestamped pharmacological and physiological data. In this study, continuous infusions as well as bolus doses of the sedatives propofol, midazolam, morphine, fentanyl and alfentanil and the vasopressor agents dobutamine, noradrenaline, vasopressin, and ephedrine, and the physiological variables (ABP and ICP) were analyzed.
Arterial blood pressure (ABP) was obtained through either radial or femoral arterial lines connected to pressure transducers (Baxter Healthcare Corp. CardioVascular Group, Irvine, CA, or similar devices). ICP was acquired via an intra-parenchymal strain gauge probe (Codman ICP MicroSensor; Codman & Shurtleff Inc., Raynham, MA), raumedic catheter Neurovent-P (Raumedic AG, Münchberg, Germany), parenchymal fiber optic pressure sensor (Camino ICP Monitor, Integra Life Sciences, Plainsboro, NJ, United States; https://www.integralife.com/) or using external ventricular drains (Medtronic, Minneapolis, MN). Again, both ABP and ICP data were directly linked to a Clinisoft database.
Signal processing
The following signal processing occurred using similar methodology, covered in other publications by our group and the senior author [4, 12, 18, 19, 26]. Data collected were stored in the database as the median for each time period, ranging from 0.5 to 5 min, generating unevenly sampled time-series data. To transform the data to an evenly sampled time series (at 1 min), we imputed the data over a 20-min window using locally weighted estimated scatterplot smoothing (LOWESS), thus generating an imputed minute-by-minute median time-series value for ICP and mean arterial blood pressure (MAP). CPP was then calculated as MAP-ICP.
Cerebrovascular reactivity was assessed through low-frequency PRx (LPRx) which was derived via the moving correlation coefficient of multiple consecutive minute-by-minute samples of ICP and MAP, to give a LPRx value updated every minute [27,28,29]. The LPRx was found for 10, 15, 20, 30 and 60 consecutive samples (10–60 min of time) and labeled as: LPRx_10, LPRx_15, LPRx_20, LPRx_30, and LPRx_60; in line with previous literature on LPRx in TBI [27,28,29]. LPRx values range from -1 to 1, with higher values indicating increasingly impaired cerebrovascular reactivity, indicated thresholds for impaired reactivity range from 0, 0.25 and 0.35. [27,28,29]
Statistical analysis
All statistical analysis was performed using R statistical computing software. (R Foundation for Statistical Computing (2020), Vienna, Austria, http://www.R-project.org/). This manuscript performed an exploration into the relationships between various treatment agents and cerebrovascular reactivity as well as generic blood pressure measures ICP, CPP and MAP. To accomplish this, the continuous infusion minute-by-minute data were compared to various physiological variables. Also, the mean physiological variable before and after an agent infusion change (both bolus and continuous) were compared, assessing how the change in dosing impacts the overall variable response.
Minute-by-minute continuous infusion evaluation
The minute-by-minute continuous infusion information was time linked with the pharmacological information from which various comparisons could be performed. Not all agents had continuous infusions thus only midazolam, morphine, propofol, dobutamine, vasopressin and adrenaline were assessed for this minute-by-minute analysis (see Additional file 1: Appendix C and O for more details about infusion timings).
LOESS infusion changes
From this data locally estimated scatterplot smoothing (LOESS) plots were used to visually compare the impact of different dosages of the infusion agents on given physiological measures: MAP, ICP, CPP, LPRx_10, LPRx_15, LPRx_20, LPRx_30 and LPRx_60. To derive the LOESS plots, the continuous agents’ infusion rates were paired with their respective minute-by-minute timestamped physiology, thus for every minute there was the physiology and indicated infusion rate. This data was then grouped for all desired continuous infusion agents over the entire data set to give one LOESS plot per agent per physiology. Dosing amounts were adjusted to a standard amount per kilogram (kg) of the patient.
Evaluation using multiple linear modeling
Given that most patients had multiple continuous infusions given at the same time, including different types of sedative and pressors, a multivariant linear regression analysis was performed on this data [30,31,32]. The general methodology for multiple linear regression modeling was done with the minute-by-minute drug infusion and physiological information. From past literature it is known that the physiological variables are inherently linear, thus a first-order difference was applied to all the physiological variables (ICP, CPP, LPRx_10 and LPRx_60) to give the first-order differenced variable response [7, 33,34,35]. A multiple linear regression model was created for just the time when vasopressor agents were given, just when sedative agents were given and all the time when both sedative and vasopressor agents were given. For more information about linear regression analysis, we refer the interested reader to the following literature [30,31,32]. It should be noted that vasopressin and morphine were excluded for some of this analysis, given vasopressin had a limited amount of recorded data as compared to the other agents and morphine is not used in a sedative or pressor medication strategy.
Injury severity
Using the same data for the multiple infusion evaluation, this data was further sub-divided based on the patient’s Marshall CT score. Again, a multiple linear regression model was created for just the vasopressor agents, just the sedative agents and both the sedative and vasopressor agents [30,31,32].
Finally on the minute-by-minute data a one-way analysis of variance (ANOVA) test was performed, over all the main physiological variables and Marshall CT score. A Bonferroni adjustment was applied to this data given the generic nature of the test and the number of patients.
Pre-/post-drug change evaluation
For both the continuously infused agents and the bolus doses, all points in time where any drug agent was changed (increase, decrease or a bolus dose given) was marked. From this indexed data, date, time, infusion rate, ICP, ABP, CPP and LPRx data could be found. Then the physiology data both pre-/post-infusion rate change was used to find the grand mean value or % time over key thresholds. A 30-min window pre-/post-dose with a 15 min delay was used (thus each change was assessed over 1.25 h of data) and this allowed all agents to reach full onset response, which was taken from our previous work [4]. Any time window that had less than 50% of the data was discarded from the study. Note, the bolus and continuous infusions were in different groups for all analyses, to allow for the comparison of difference between continuous and bolus drug impacts.
The analyzed physiological variables thresholds were: % time LPRx > 0, % time LPRx > 0.25, % time LPRx > 0.35, % time ICP > 20 mmHg, % time ICP > 22 mmHg, % time CPP > 70 mmHg, and % time CPP < 60 mmHg [3, 36,37,38]. These thresholds are defined from previously described literature, with the time above these limits found to be associated with worse outcome at 6 to 12 months post-injury [3, 36,37,38].
With the pre-/post-drug change window data (the grand mean or % time over a key threshold) a Wilcoxon signed-ranked test was performed for this data for all agents separated into the agent dose change (increase, decrease or a bolus dose was given). Finally, a Bonferroni p value adjustment was used to account for multiple comparisons. The full list of agents assessed in this study was propofol, alfentanil, fentanyl, midazolam, morphine, dobutamine, ephedrine, noradrenaline and vasopressin which were assessed for the three outlined methods.
Evaluation of categories
The pre-/post- drug change window data were then further categorized into sub-groups based on physiology in the pre-dose window. Evaluation of the sub-groups included:
-
a.
Pre-time window over 50% time ICP > 20 mmHg.
-
b.
Pre-time window over 50% time ICP < 20 mmHg.
-
c.
Pre-time window over 50% time LPRx_10 > 0.
-
d.
Pre-time window over 50% time LPRx_10 < 0.
-
e.
Pre-time window over 50% time LPRx_10 > 0.35.
-
f.
Pre-time window over 50% time LPRx_10 < 0.35.
-
g.
Continuous infusion going from “Off to On” agent (and vice versa i.e., On to Off)—With the continuous infusion rate data, we could identify if the agent was switched on (from 0 to a positive number) or off (a positive number to 0).
-
h.
Assessing the high/medium/low infusion rates of continuous infusion agents (for more detail see Additional file 1: Appendix J)—The infusion rates were stratified by high, medium or low as described in Additional file 1: Appendix J. This allowed for further comparison of physiological response to the studied vasopressors and sedative pharmacologic agents.
For all comparisons, again a Wilcoxon signed-ranked test was performed between the pre- and post-physiological variable windows with Bonferroni correction to adjust for multiple comparisons.
Results
Patient characteristics
Table 1 provides the core patient characteristics for all the patients. The median age was 52 years (interquartile range; IQR: 34–62.5 years), with 367 (77.3%) being males with most patients having 10 days of recording resulting in over 3350 days of recording. The continuous infusion rates of these agents ranged from 0.001–7.5 mg/kg/h for propofol, 0.01–0.55 mg/kg/h for morphine, 0.001–0.8 mg/kg/h for midazolam, 0.001–19 μg/kg/min for dobutamine, 0.03–0.48 μg/kg/min for noradrenaline, and 0.07–1.1 Infusion Units/kg/h for vasopressin. Of the 475 patients, 49(10.3%) underwent a decompressive craniectomy and 88(18.5%) did not require hematoma evacuation surgery. These TBI demographics are in keeping with normal TBI cohorts.
Minute-by-minute continuous infusion evaluation
LOESS response
Figures 1 and 2 show the LOESS plot of propofol and noradrenaline, other data for this analysis can be found in Additional file 1: Appendix A and B. For the data there was a limited relation between the continuous infused agents and LPRx. Although morphine, propofol and midazolam LOESS curves can be seen related to changes in CPP and ICP at higher doses.

LOESS plots—propofol. Figure of the LOESS plots of different dose amounts of propofol and their associations to different physiological variables (ie minute-by- minute data paired with continuous infusion rate). Au, arbitrary units; CPP, cerebral perfusion pressure; hr, hour; ICP, intracranial pressure; kg, kilogram; LPRx_10, pressure reactivity over 10 min; LPRx_60, pressure reactivity over 60 min; mg, milligram; mmHg, millimeter of mercury; ug, microgram

LOESS plot—noradrenaline. Figure of the LOESS plots of different dose amounts of noradrenaline and their associations to different physiological variables (i.e. minute-by-minute data paired with continuous infusion rate). Au, arbitrary units; CPP, cerebral perfusion pressure; h, hour; ICP, intracranial pressure; kg, kilogram; LPRx_10, pressure reactivity over 10 min; LPRx_60, pressure reactivity over 60 min; mg, milligram; mmHg, millimeter of mercury; μg, microgram
Multiple linear regression evaluation
Using the minute-by-minute data, various multiple linear regression models were created. As demonstrated in Additional file 1: Appendix C, the various agents used had a limited impact on ICP, CPP, LPRx_10 or LPRx_60. Notably, no p values reached significance with any infusion agent given nor did any of them have a high mean correlation (<|0.5|).
Injury severity
Using the minute-by-minute data sub-divided for Marshal CT score, various multiple linear regression models were created. As demonstrated in Additional file 1: Appendix D, the various agents used had a limited impact on ICP, CPP, LPRx_10 or LPRx_60 and was similar to the full data assessment for all CT scores.
The one-way ANOVA test did have ICP being modulated by Marshall CT score, however with the application of p value adjustment this significance went away. All other variables demonstrated a non-significant relationship between Marshal CT score and the fluctuations in variables (see Additional file 1: Appendix E).
Pre/post drug change evaluation
Overall dose response
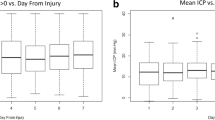
Table 2, Fig. 3 and Additional file 1: Appendix F show the bolus and continuous infusion agents for the full monitoring time. Though some agents demonstrated a significant p-value between the pre- and post-windows, the overall data had limited differences. Bolus noradrenaline had a slight decrease in % time of LPRx over key thresholds (previously indicated impaired/intact autoregulation thresholds), however given the small difference in these results and the fact that the median value was 0, the true impact of any of the investigated drugs on LPRx is likely negligible. Finally, noradrenaline and morphine did appear to be significantly associated with ICP, MAP, and CPP shown in Additional file 1: Appendix F.

Box plots for bolus doses—% time LPRx_10 > 0. Figure of the boxplots of different bolus agents (and only bolus infusions), with the Wilcoxon signed-ranked value between the pre–post dose. Au, arbitrary units; LPRx_10, pressure reactivity over 10 min; min, minutes
Subcategorization of the DATA
All of the subcategorization of the data can be found in Additional file 1: Appendix G–N. In general, incremental dose changes or bolus doses demonstrated little influence on LPRx or ICP, regardless of group adjustment. However, when separating the doses based on LPRx_10 pre-dose data, all agents had slightly significant p values in the LPRx relationships. Though this may have more to do with patient state rather than the drugs which is confirmed by the fact that for both increases and decreases in continuous agents the result in LPRx remains the same. Moreover, given that when LPRx was indicated to be impaired pre-time window (as LPRx_10 > 0 or 0.35) the dose appeared to reduce LPRx, but when LPRx was indicated to be intact (as LPRx_10 < 0 or 0.35) there was an increase in LPRx.
Discussion
From this temporally resolved dataset prospectively collected at the Karolinska University Hospital, an exploration into the relationships between various treatment agents and cerebrovascular reactivity was performed. The evaluation involved comparing physiologic responses to both continuous and bolus drug infusions, and thus some important aspects can be highlighted.
First, cerebrovascular reactivity, as measured through LPRx metrics, was not significantly impacted by the various medication agents used. These findings are corroborated by publications out of Leuven and Winnipeg for traditional, high-resolution PRx determination [4, 5]. Furthermore, this work is the first study to evaluate the cerebrovascular reactivity response to a large number of treatment agents. As these agents are employed in guideline-based treatment of moderate/severe TBI, their lack of impact on cerebrovascular reactivity carries significance to future analyses [3]. This work supports that small incremental and bolus dosing of recommended treatment agents, may not need to be accounted for in future studies on cerebrovascular reactivity and individualized physiologic targets derived from cerebrovascular reactivity [4]. Moreover, specifically high doses of noradrenaline were not associated with high LPRx values, which helps validate that in general TBI conditions under current CPP and ICP therapies do not significantly degrade cerebrovascular reactivity. Though it must be acknowledged, that more in-depth work assessing the full physiological impact is required.
Second, the variation in vasopressor drug dosing appears to mediate CPP within desired threshold targets (Fig. 2 and Additional file 1: Appendix A demonstrates stable CPP values despite changes in doses). Targeting CPP is an important aspect of future studies looking to mediate cerebrovascular reactivity through optimal CPP targeting. Many collaborative groups in Europe and Canada focus on PRx targeting through CPP [5, 14, 39, 40], and this was the subject of a phase II randomized control trial [41].
Moreover, the plateau wave of ICP vs increases in doses of vasopressin bears highlighting, as seen in Additional file 1: Appendix A. Vasopressin is used to spare noradrenaline at high doses in septic patients, thus this plateau wave in ICP, despite increases in vasopressin doses, might indicate that there is a threshold of ICP management through vasopressin. This fact may have to do with the ability of vasopressin to impact aquaporin-4 which affects the drug carrying implications for ICP control, given aquaporin-4 has a role in the blood brain barrier and water homeostasis [42,43,44,45]. However, this requires further exploration in larger multi-center data sets as it is unclear given the limited numbers in this data set.
Third, cerebrovascular reactivity appears to remain relatively unaffected by sedative agents and changes in dosing. In particular, changes in all sedative agents failed to elicit significant alterations in any LPRx or time spent with LPRx above indicated thresholds during the full monitoring time. Although morphine, propofol and midazolam LOESS curves can be seen related to changes in CPP and ICP at higher doses, this may have to do with a limited number of samples in these regions, or refractory intracranial hypertension (Fig. 1 and Additional file 1: Appendix A). Past literature on propofol and cerebral blood flow in TBI patients has noted that this agent has a limited impact on response [46,47,48,49,50,51]. Moreover work assessing midazolam found a non-significant response in ICP, cerebral blood flow or partial oxygenation [47, 52, 53]. Thus, given the significant number of doses of midazolam and propofol these results bolster that which has already been documented in past literature, noting the limited influence of sedative agents on cerebrovasculature [21, 22].
Next, though the subcategorization based on LPRx pre-dose did indicate some significance in the resulting LPRx, based on the uniformity of change (whether the drug infusion was increased or decreased in pre-dose cerebrovascular reactivity state), the resulting significance appears to have more to do with patient state then the agent itself. All other categorizations of the individual groups failed to have any significant outliers in terms of physiological response to medication agent.
Moreover, the sub-group breakdown of the data based on the Marshall CT score, found similar results across all injury severity. Thus, highlights that impaired cerebrovascular reactivity occurs in a variation of injury severity, and that current treatment regimens still have limited impact.
All this work highlights two major insights for the future of TBI care. First given that cerebrovascular reactivity has a limited impact from currently used guideline-based pharmacological regimens, means that the interest in mediation of cerebrovascular reactivity through other approaches should be explored. Methods like the optimal CPP, individualized ICP and the optimal depth of sedation focus on using physiological (not pharmacological) mediation to attain optimal cerebrovascular reactivity [28, 54,55,56,57,58]. This focus on pathophysiological mediation may overcome the limitations in current treatments and lead to more personalized targeted treatment.
Next, as LPRx seems to be unassociated with larger time aggregated pharmacological dosing regimens means that current practices in the intensive care unit may be inadequate to effectively target patient state. Most physiological responses are highly volatile with significant variation in response over hours and minutes. Thus, though this work has documented that current regimens of the agents do not significantly impact physiological response, there are always outliers and more momentary effects that are not accounted for. Any future acute TBI care study should have a focus on smaller aggregation of time then the common hourly measures.
Limitations
Despite the interesting results described above, there are some limitations which deserve highlighting. First, this study is based only on a single-center observational patient cohort taken from Sweden and given the nature of TBI, there is high heterogeneity not accounted for in this study. Thus, the more individualized injury patterns that directly impact cerebral physiological response were not accounted for in this manuscript apart from overall Marshal CT score injury polychotomization. Second, we focused on basic statistics and descriptive analysis for data, the full physiological impact of these agents would be more complete through an individualized moment by moment assessment. Third the drugs investigated were often administered at the same time, and thus the physiologic changes may be suppressed by changes in other infusions. Moreover, given the nature of retrospective observational studies it is impossible to truly determine if the change in drug concentration was a result in a change in cerebral physiology or vice versa. This is confirmed by the high doses of noradrenaline and propofol having confounding associations with ICP and CPP. Finally, given the relatively low resolution of the LPRx and limited overall data collection, this is the first work to compare LPRx to medication.
Future directions
Future investigation would benefit from time-series analytical methodologies, using multi-variate vector autoregressive integrative moving average (VARIMA) models, impulse response function analysis, and Granger causality testing both pre- and post-agent. Such complex work is the focus of ongoing efforts of both the Winnipeg Acute TBI laboratories and the Karolinska Institutet [5, 14, 39, 40]. In addition, despite the lack of significant results, future sub-group analysis to better determine outliers and physiological differences within patients would be beneficial. To what extent age and sex impact cerebral assessment is still unclear with work indicating that older age results in decreased ICP values [59, 60].
Conclusions
The results of the analysis confirmed that, overall, the continuous infusion or bolus doses of sedative (propofol, alfentanil, fentanyl, morphine and midazolam) and vasopressor (dobutamine, ephedrine, noradrenaline and vasopressin) agents do not impact or impair cerebrovascular reactivity. However, vasopressor agents do appear to maintain CPP and may be useful to target optimal CPP values. Overall, this study indicates that commonly administered sedative and vasopressor agents do not have a clinically significant influence on cerebrovascular reactivity in TBI. These results are still limited, requiring further temporal investigation.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its additional information files].
Abbreviations
- ABP:
-
Arterial blood pressure
- CPP:
-
Cerebral perfusion pressure
- GCS:
-
Glasgow Coma Scale
- ICP:
-
Intracranial blood pressure
- ICU:
-
Intensive care unit
- LOESS:
-
Locally estimated scatter plot smoothing
- LOWESS:
-
Locally weighted estimate scatter plot smoothing
- LPRx:
-
Long pressure reactivity index
- MAP:
-
Mean arterial blood pressure
- TBI:
-
Traumatic brain injury
- VARMA:
-
Vector autoregressive moving average filter
References
Chesnut R, Aguilera S, Buki A et al (2020) A management algorithm for adult patients with both brain oxygen and intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med 46:919–929. https://doi.org/10.1007/s00134-019-05900-x
Hawryluk GWJ, Aguilera S, Buki A et al (2019) A management algorithm for patients with intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med 45:1783–1794. https://doi.org/10.1007/s00134-019-05805-9
Carney N, Totten AM, O’Reilly C et al (2017) Guidelines for the management of severe traumatic brain injury, Fourth Edition. Neurosurgery 80:6–15. https://doi.org/10.1227/NEU.0000000000001432
Froese L, Dian J, Batson C et al (2020) The impact of vasopressor and sedative agents on cerebrovascular reactivity and compensatory reserve in traumatic brain injury: an exploratory analysis. Neurotrauma Reports 1:157–168. https://doi.org/10.1089/neur.2020.0028
Klein SP, Fieuws S, Meyfroidt G, Depreitere B (2020) Effects of norepinephrine, propofol and hemoglobin concentration on dynamic measurements of cerebrovascular reactivity in acute brain injury. J Neurotrauma. https://doi.org/10.1089/neu.2020.7160
Budohoski KP, Czosnyka M, de Riva N et al (2012) The relationship between cerebral blood flow autoregulation and cerebrovascular pressure reactivity after traumatic brain injury. Neurosurgery 71:652–661. https://doi.org/10.1227/NEU.0b013e318260feb1
Zeiler FA, Lee JK, Smielewski P et al (2018) Validation of intracranial pressure-derived cerebrovascular reactivity indices against the lower limit of autoregulation, part II: experimental model of arterial hypotension. J Neurotrauma 35:2812–2819. https://doi.org/10.1089/neu.2017.5604
Zeiler FA, Donnelly J, Calviello L et al (2018) Validation of pressure reactivity and pulse amplitude indices against the lower limit of autoregulation, part I: experimental Intracranial Hypertension. J Neurotrauma 35:2803–2811. https://doi.org/10.1089/neu.2017.5603
Zeiler FA, Kim D-J, Cabeleira M et al (2018) Impaired cerebral compensatory reserve is associated with admission imaging characteristics of diffuse insult in traumatic brain injury. Acta Neurochir (Wien) 160:2277–2287. https://doi.org/10.1007/s00701-018-3681-y
Sorrentino E, Diedler J, Kasprowicz M et al (2012) Critical thresholds for cerebrovascular reactivity after traumatic brain injury. Neurocrit Care 16:258–266. https://doi.org/10.1007/s12028-011-9630-8
Czosnyka M, Smielewski P, Kirkpatrick P et al (1997) Continuous assessment of the cerebral vasomotor reactivity in head injury. Neurosurgery 41:11–19. https://doi.org/10.1097/00006123-199707000-00005
Donnelly J, Czosnyka M, Adams H et al (2019) Twenty-five years of intracranial pressure monitoring after severe traumatic brain injury: a retrospective, single-center analysis. Neurosurgery 85:E75–E82. https://doi.org/10.1093/neuros/nyy468
Zeiler FA, Donnelly J, Smielewski P et al (2018) Critical thresholds of intracranial pressure-derived continuous cerebrovascular reactivity indices for outcome prediction in noncraniectomized patients with traumatic brain injury. J Neurotrauma 35:1107–1115. https://doi.org/10.1089/neu.2017.5472
Bennis FC, Teeuwen B, Zeiler FA et al (2020) Improving prediction of favourable outcome after 6 months in patients with severe traumatic brain injury using physiological cerebral parameters in a multivariable logistic regression model. Neurocrit Care. https://doi.org/10.1007/s12028-020-00930-6
Froese L, Batson C, Gomez A et al (2020) The limited impact of current therapeutic interventions on cerebrovascular reactivity in traumatic brain injury: a narrative overview. Neurocrit Care. https://doi.org/10.1007/s12028-020-01003-4
Zeiler FA, Ercole A, Beqiri E et al (2019) Cerebrovascular reactivity is not associated with therapeutic intensity in adult traumatic brain injury: a CENTER-TBI analysis. Acta Neurochir 161:1955–1964. https://doi.org/10.1007/s00701-019-03980-8
Weersink CSA, Aries MJH, Dias C et al (2015) Clinical and physiological events that contribute to the success rate of finding “optimal” cerebral perfusion pressure in severe brain trauma patients. Crit Care Med 43:1952–1963. https://doi.org/10.1097/CCM.0000000000001165
Zeiler FA, Beqiri E, Cabeleira M et al (2020) Brain tissue oxygen and cerebrovascular reactivity in traumatic brain injury: a collaborative European neurotrauma effectiveness research in traumatic brain injury exploratory analysis of insult burden. J Neurotrauma. https://doi.org/10.1089/neu.2020.7024
Froese L, Dian J, Batson C et al (2020) The impact of hypertonic saline on cerebrovascular reactivity and compensatory reserve in traumatic brain injury: an exploratory analysis. Acta Neurochir (Wien). https://doi.org/10.1007/s00701-020-04579-0
Dias C, Silva MJ, Pereira E et al (2014) Post-traumatic multimodal brain monitoring: response to hypertonic saline. J Neurotrauma 31:1872–1880. https://doi.org/10.1089/neu.2014.3376
Froese L, Dian J, Batson C et al (2020) Cerebrovascular response to propofol, fentanyl, and midazolam in moderate/severe traumatic brain injury: a scoping systematic review of the human and animal literature. Neurotrauma Reports 1:100–112. https://doi.org/10.1089/neur.2020.0040
Zeiler FA, Sader N, Gillman LM et al (2016) The cerebrovascular response to ketamine: a systematic review of the animal and human literature. J Neurosurg Anesthesiol 28:123–140. https://doi.org/10.1097/ANA.0000000000000234
Nordström C-H (2005) Physiological and biochemical principles underlying volume-targeted therapy–the “Lund concept.” Neurocrit Care 2:83–95. https://doi.org/10.1385/NCC:2:1:083
Grände P-O (2011) The Lund concept for the treatment of patients with severe traumatic brain injury. J Neurosurg Anesthesiol 23:358–362. https://doi.org/10.1097/01.ana.0000405612.20356.84
Thelin EP, Jeppsson E, Frostell A et al (2016) Utility of neuron-specific enolase in traumatic brain injury; relations to S100B levels, outcome, and extracranial injury severity. Crit Care. https://doi.org/10.1186/s13054-016-1450-y
Thelin EP, Raj R, Bellander B-M et al (2019) Comparison of high versus low frequency cerebral physiology for cerebrovascular reactivity assessment in traumatic brain injury: a multi-center pilot study. J Clin Monit Comput. https://doi.org/10.1007/s10877-019-00392-y
Santos E, Diedler J, Sykora M et al (2011) Low-frequency sampling for PRx calculation does not reduce prognostication and produces similar CPPopt in intracerebral haemorrhage patients. Acta Neurochir (Wien) 153:2189–2195. https://doi.org/10.1007/s00701-011-1148-5
Depreitere B, Güiza F, Van den Berghe G et al (2016) Can optimal cerebral perfusion pressure in patients with severe traumatic brain injury be calculated based on minute-by-minute data monitoring? Acta Neurochir Suppl 122:245–248. https://doi.org/10.1007/978-3-319-22533-3_49
Depreitere B, Güiza F, Van den Berghe G et al (2014) Pressure autoregulation monitoring and cerebral perfusion pressure target recommendation in patients with severe traumatic brain injury based on minute-by-minute monitoring data. J Neurosurg 120:1451–1457. https://doi.org/10.3171/2014.3.JNS131500
Douc R, Moulines E, Stoffer DS (2014) Nonlinear times series: theory, methods and applications with R examples. CRC Press, Taylor & Francis Group, Boca Raton
Gallagher C (2007) Extending the linear model with R: generalized linear, mixed effects and nonparametric regression models. J Am Stat Assoc 102:1477–1477. https://doi.org/10.1198/jasa.2007.s238
Lütkepohl H (2005) New Introduction to Multiple Time Series Analysis. Springer-Verlag, Berlin Heidelberg
Sainbhi AS, Froese L, Gomez A et al (2021) Continuous time-domain cerebrovascular reactivity metrics and discriminate capacity for the upper and lower limits of autoregulation: a scoping review of the animal literature. Neurotrauma Rep 2:639–659. https://doi.org/10.1089/neur.2021.0043
Zeiler FA, Cabeleira M, Hutchinson PJ et al (2021) Evaluation of the relationship between slow-waves of intracranial pressure, mean arterial pressure and brain tissue oxygen in TBI: a CENTER-TBI exploratory analysis. J Clin Monit Comput 35:711–722. https://doi.org/10.1007/s10877-020-00527-6
Froese L, Gomez A, Sainbhi AS, et al (2022) Dynamic temporal relationship between autonomic function and cerebrovascular reactivity in moderate/severe traumatic brain injury. Front Network Physiol 2
Balestreri M, Czosnyka M, Steiner LA et al (2005) Association between outcome, cerebral pressure reactivity and slow ICP waves following head injury. Acta Neurochir Suppl 95:25–28. https://doi.org/10.1007/3-211-32318-x_6
Zeiler FA, Ercole A, Beqiri E et al (2019) Association between cerebrovascular reactivity monitoring and mortality is preserved when adjusting for baseline admission characteristics in adult traumatic brain injury: a CENTER-TBI study. J Neurotrauma. https://doi.org/10.1089/neu.2019.6808
Lang EW, Kasprowicz M, Smielewski P et al (2015) Short pressure reactivity index versus long pressure reactivity index in the management of traumatic brain injury. J Neurosurg 122:588–594. https://doi.org/10.3171/2014.10.JNS14602
Maas AIR, Menon DK, Steyerberg EW et al (2015) Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI): a prospective longitudinal observational study. Neurosurgery 76:67–80. https://doi.org/10.1227/NEU.0000000000000575
Bernard F, Gallagher C, Griesdale D et al (2020) The CAnadian High-Resolution Traumatic Brain Injury (CAHR-TBI) Research Collaborative. Can J Neurol Sci. https://doi.org/10.1017/cjn.2020.54
Tas J, Beqiri E, van Kaam RC et al (2021) Targeting Autoregulation-Guided Cerebral Perfusion Pressure after Traumatic Brain Injury (COGiTATE): a feasibility randomized controlled clinical trial. J Neurotrauma 38:2790–2800. https://doi.org/10.1089/neu.2021.0197
Van Hoek AN, Bouley R, Lu Y et al (2009) Vasopressin-induced differential stimulation of AQP4 splice variants regulates the in-membrane assembly of orthogonal arrays. Am J Physiol Renal Physiol 296:F1396–F1404. https://doi.org/10.1152/ajprenal.00018.2009
Niermann H, Amiry-Moghaddam M, Holthoff K et al (2001) A novel role of vasopressin in the brain: modulation of activity-dependent water flux in the neocortex. J Neurosci 21:3045–3051. https://doi.org/10.1523/JNEUROSCI.21-09-03045.2001
Poulsen SB, Kim Y-H, Frøkiær J et al (2013) Long-term vasopressin-V2-receptor stimulation induces regulation of aquaporin 4 protein in renal inner medulla and cortex of Brattleboro rats. Nephrol Dial Transplant 28:2058–2065. https://doi.org/10.1093/ndt/gft088
Wang X, Li T, Liu Y et al (2021) Aquaporin 4 differentially modulates osmotic effects on vasopressin neurons in rat supraoptic nucleus. Acta Physiol 232:e13672. https://doi.org/10.1111/apha.13672
James ML, Olson DM, Graffagnino C (2012) A pilot study of cerebral and haemodynamic physiological changes during sedation with dexmedetomidine or propofol in patients with acute brain injury. Anaesth Intensive Care 40:949–957. https://doi.org/10.1177/0310057X1204000605
Tanguy M, Seguin P, Laviolle B et al (2012) Cerebral microdialysis effects of propofol versus midazolam in severe traumatic brain injury. J Neurotrauma 29:1105–1110. https://doi.org/10.1089/neu.2011.1817
Johnston AJ, Steiner LA, Chatfield DA et al (2003) Effects of propofol on cerebral oxygenation and metabolism after head injury. Br J Anaesth 91:781–786. https://doi.org/10.1093/bja/aeg256
Steiner LA, Johnston AJ, Chatfield DA et al (2003) The effects of large-dose propofol on cerebrovascular pressure autoregulation in head-injured patients. Anesth Analg 97:572–576. https://doi.org/10.1213/01.ane.0000070234.17226.b0
Pinaud M, Lelausque JN, Chetanneau A et al (1990) Effects of propofol on cerebral hemodynamics and metabolism in patients with brain trauma. Anesthesiology 73:404–409. https://doi.org/10.1097/00000542-199009000-00007
Lee JH, Kelly DF, Oertel M et al (2001) Carbon dioxide reactivity, pressure autoregulation, and metabolic suppression reactivity after head injury: a transcranial Doppler study. J Neurosurg 95:222–232. https://doi.org/10.3171/jns.2001.95.2.0222
Papazian L, Albanese J, Thirion X et al (1993) Effect of bolus doses of midazolam on intracranial pressure and cerebral perfusion pressure in patients with severe head injury. Br J Anaesth 71:267–271. https://doi.org/10.1093/bja/71.2.267
Oddo M, Crippa IA, Mehta S et al (2016) Optimizing sedation in patients with acute brain injury. Crit Care. https://doi.org/10.1186/s13054-016-1294-5
Aries MJ, Czosnyka M, Budohoski K et al (2012) Continuous determination of optimal cerebral perfusion pressure in traumatic brain injury*. Crit Care Med 40:2456–2463. https://doi.org/10.1097/CCM.0b013e3182514eb6
Donnelly J, Czosnyka M, Adams H et al (2017) Individualizing thresholds of cerebral perfusion pressure using estimated limits of autoregulation. Crit Care Med 45:1464–1471. https://doi.org/10.1097/CCM.0000000000002575
Matchett KB, Lynam-Lennon N, Watson RW, Brown JAL (2017) Advances in precision medicine: tailoring individualized therapies. Cancers (Basel). https://doi.org/10.3390/cancers9110146
Froese L, Gomez A, Sainbhi AS et al (2022) Continuous determination of the optimal bispectral index value based on cerebrovascular reactivity in moderate/severe traumatic brain injury: a retrospective observational cohort study of a novel individualized sedation target. Crit Care Explor 4:e0656. https://doi.org/10.1097/CCE.0000000000000656
Froese L, Gomez A, Sainbhi AS et al (2022) Optimal bispectral index level of sedation and cerebral oximetry in traumatic brain injury: a non-invasive individualized approach in critical care? Intensive Care Med Exp 10:33. https://doi.org/10.1186/s40635-022-00460-9
Batson C, Froese L, Gomez A et al (2021) Impact of age and biological sex on cerebrovascular reactivity in adult moderate/severe traumatic brain injury: an exploratory analysis. Neurotrauma Rep 2:488–501. https://doi.org/10.1089/neur.2021.0039
Batson C, Froese L, Sekhon MS et al (2022) Impact of chronological age and biological sex on cerebrovascular reactivity in moderate/severe traumatic brain injury: a CAnadian High-Resolution TBI (CAHR-TBI) Study. J Neurotrauma. https://doi.org/10.1089/neu.2022.0293
Acknowledgements
FAZ receives research support from NSERC, CIHR, the MPI Neuroscience Research Operating Fund, the Health Sciences Centre Foundation Winnipeg, the Canada Foundation for Innovation (CFI) (Project #: 38583), Research Manitoba (Grant #: 3906), the University of Manitoba VPRI Research Investment Fund (RIF), and the University of Manitoba MPI Professorship in Neuroscience. LF is supported through the University of Manitoba—Biomedical Engineering (BME) Fellowship Grant, Research Manitoba—Health Sciences PhD Studentship, NSERC (ALLRP-576386-22) and the University of Manitoba Graduate Enhancement of Tri-Agency Stipend (GETS) program. EPT is supported through the Strategic Research Area Neuroscience (STRATNeuro), The Erling-Persson Foundation, Region Stockholm Clinical Research Appointment (#FoUI-981490) and Karolinska Institutet Research Grants (#2022-01576).
Funding
Open access funding provided by Karolinska Institute. This work was directly supported through the Natural Sciences and Engineering Research Council of Canada (NSERC) (DGECR-2022-00260, RGPIN-2022-03621 and ALLRP-576386-22) and the Manitoba Public Insurance (MPI) Neuroscience Research Operating Fund.
Author information
Authors and Affiliations
Contributions
LF prepared, analyzed and interpreted the patient data. EH, CA, JT, EH, CL, DN and ET helped collect and interpret patient data. FAZ and LF formalized methods and main analysis for this manuscript and were major contributors in writing the first draft manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Study was approved by the Swedish Ethical Review Authority (#2020-05227) on November 17, 2020) and adheres to the Helsinki Declaration of 1975. Swedish Ethics Review Authority has waived the need for informed consent.
Consent for publication
Not applicable.
Competing interests
The authors have no financial disclosures or conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Appendix A. LOESS Curves – CPP/ICP/LPRx_10/LPRx_60. Appendix B. LOESS Curves – MAP/LPRx_15/LPRx_20/LPRx_30. Appendix C1. Multiple lnear model for all data. Appendix C2. Multiple linear model for sedatives data. Appendix C3. Multiple linear model for vasopressor data. Appendix D. Multiple linear model for segment Marshall CT score data. Appendix D1. Multiple linear model for Marshall CT data = 1. Appendix D2. Multiple linear model for Marshall CT data = 2. Appendix D3. Multiple linear model for Marshall CT data = 3. Appendix D5. Linear model for Marshall CT data = 5. Appendix E. One-Way ANOVA of physiology and Marshall CT score. Appendix F. Infusions of all data. Appendix G. Pre-time window over 50% time ICP > 20 mmHg. Appendix H. Pre-time window over 50% time ICP < 20 mmHg. Appendix I. Pre-time window over 50% time L-PRx_10 > 0. Appendix J. Pre-time window over 50% time L-PRx_10 < 0. Appendix K. Pre-time window over 50% time L-PRx_10 > 0.35. Appendix L. Pre-time window over 50% time L-PRx_10 < 0.35. Appendix M. Continuous infusion going from nothing to agent (and vice versa ie, On to Off). Appendix N. Assessing the High/Medium/Low of different infusion agent. Appendix O. Histogram distributions of continuous infusion agents.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Froese, L., Hammarlund, E., Åkerlund, C.A.I. et al. The impact of sedative and vasopressor agents on cerebrovascular reactivity in severe traumatic brain injury. ICMx 11, 54 (2023). https://doi.org/10.1186/s40635-023-00524-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40635-023-00524-4