
Abstract
Purpose
Injuries are common in sports and can have significant physical, psychological and financial consequences. Machine learning (ML) methods could be used to improve injury prediction and allow proper approaches to injury prevention. The aim of our study was therefore to perform a systematic review of ML methods in sport injury prediction and prevention.
Methods
A search of the PubMed database was performed on March 24th 2020. Eligible articles included original studies investigating the role of ML for sport injury prediction and prevention. Two independent reviewers screened articles, assessed eligibility, risk of bias and extracted data. Methodological quality and risk of bias were determined by the Newcastle–Ottawa Scale. Study quality was evaluated using the GRADE working group methodology.
Results
Eleven out of 249 studies met inclusion/exclusion criteria. Different ML methods were used (tree-based ensemble methods (n = 9), Support Vector Machines (n = 4), Artificial Neural Networks (n = 2)). The classification methods were facilitated by preprocessing steps (n = 5) and optimized using over- and undersampling methods (n = 6), hyperparameter tuning (n = 4), feature selection (n = 3) and dimensionality reduction (n = 1). Injury predictive performance ranged from poor (Accuracy = 52%, AUC = 0.52) to strong (AUC = 0.87, f1-score = 85%).
Conclusions
Current ML methods can be used to identify athletes at high injury risk and be helpful to detect the most important injury risk factors. Methodological quality of the analyses was sufficient in general, but could be further improved. More effort should be put in the interpretation of the ML models.
Similar content being viewed by others

Background
Injuries are common in individual and team sports and can have significant physical, psychosocial and financial consequences [3, 13, 22]. Understanding injury risk factors and their interplay is thereby a key component of preventing future injuries in sport [4]. An abundance of research has attempted to identify injury risk factors [4, 6, 28]. However, sports injuries are a consequence of complex interactions of multiple risk factors and inciting events making a comprehensive model necessary [6, 28]. It has to account for the events leading to the injury situation, as well as to include a description of body and joint biomechanics at the time of injury [4]. Due to the many interactions between intrinsic and extrinsic risk factors as well as their sometimes highly unpredictable nature (e.g., contact with another player), the ability to foresee the occurrence of an inciting injury event is challenging. Therefore, predictive modelling should not only focus on the prediction of the occurrence of an injury itself but, moreover, it should try to identify injury risk at an individual level and implement interventions to mitigate the level of risk [28]. In order to plan effective preventive intervention, it is therefore important to be aware both of the various isolated risk factors and their interaction [6].
In recent years, the use of advanced Artificial Intelligence (AI) methods has appeared in sports medicine to tackle this challenging multi-faceted task [1, 5, 14, 16]. AI methods have already been used successfully in sports science within the realm of game analysis, tactics, performance analysis and outcome predictions [12, 17, 21] and are about to start transforming clinical medicine [9, 31, 33, 39, 42]. However, for clinicians, the application and the understanding of AI is often difficult [24]. Therefore, the explanations of the core terms for AI application are provided in Supplementary File S1.
AI is mostly narrowed down to Machine Learning (ML) methods although it is a very broad concept comprising every aspect of mimicking human intelligence. ML is the study of algorithms that can automatically learn from data to make new decisions [23]. Current ML methods include Neural Networks, Support Vector Machines, or Random Forests which are part of a 'Machine Learning pipeline' (Fig. 1). The available data for the ML model has to be of high quality and can be any data deemed useful for the purpose of injury prediction. This data is split in two parts (data splitting), the so-called training and test data. First, the algorithm has to learn the relationship between outcome of interest (injury or not) and the potential contributing factors (also called predictors/features/covariates/explanatory variables) from the training data set. The test data can then be used to test the prediction capacity of the algorithm learned from the training data. It is important that this quality check is not achieved on the training data, but on unseen data, hence the data splitting at the beginning. The quality and size of the data sets are important parameters for the quality of the results. To improve the quality of these large and complex datasets and to ensure optimal operation of the ML algorithms, data preprocessing methods (imputation, standardization, discretization), dimension reduction and feature selection can be applied (see Supplementary File S1). Most ML procedures further require parameter tuning, a sort of optimization of parameters which cannot be estimated directly from the data (e.g., number of trees to be used in a Random Forest). When the entire ML pipeline is fitted on the training data, the outcome of the test data is predicted. Since we know the true outcome of the test data, this allows us to evaluate our established prediction model. Finally, well-performing models provide an idea of the most important risk factors, by observing which factors have the largest influence in these models.

Schematic figure of the Machine Learning approach. The entire Machine Learning process is shown. Parts in dotted shapes are optional or not always necessary
Considering that sport injury prediction and prevention are trending topics in sport science [12, 13, 16], the intention of this systematic review is to synthesize the evidence of sophisticated ML algorithms in sport injury prediction and prevention. Our systematic review differs from the one by Claudino et al. [12] in that we focus on injury prevention and risk factor identification together with a deeper examination of the used ML analyses. The following three topics are assessed:
-
1.
Identify the currently used definition of ML as well as predominantly used ML methods.
-
2.
Identify the accuracy of the currently used ML methods to predict injury.
-
3.
Evaluate the used methods for sport injury prevention purposes.
Methods
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [30]. The review protocol was prospectively registered at PROSPERO (International prospective register of systematic reviews—ie, CRD42020177708).
Search strategy and inclusion/exclusion criteria
A systematic electronic search of the PubMed database was executed on March 24th 2020 to identify studies investigating Machine Learning methods in injury prediction and prevention. The following search term was used in all fields: (“deep learning” OR “artificial intelligence” OR “machine learning” OR “neural network” OR „neural networks “ OR „support vector machines “ OR „nearest neighbor “ OR „nearest neighbors “ OR „random forest “ OR „random forests “ OR „trees" OR „elastic net “ OR „ridge “ OR „lasso “ OR „boosting “ OR „predictive modeling “ OR “learning algorithms” OR „bayesian logistic regression “) AND (“sport” OR „sports “ OR “athlete” OR “athletes”) AND („injury “ OR "injuries"). We did not use limits to perform the search and no date restrictions were applied. Inclusion criteria were as follows: (i) Original studies investigating the role of machine learning for sport injury prediction and sport injury prevention, (ii) English-language studies, (iii) studies published online or in print in a peer-reviewed journal. Injury prediction had to refer to predicting either the occurrence, the severity, or the type of injuries on the basis of risk factors. The exclusion criteria were as follows: (i) not being sport-specific, (ii) not covering injury prevention or injury prediction, (iii) meeting abstracts and proceedings. Also, studies were excluded if the used approach was rather statistical than ML. This explains why, for example, two papers from Hasler et al. [19, 20] and one from Mendonça et al. [29] were not included here.
Study selection
The titles and abstracts of all articles were screened for relevance according to the inclusion and exclusion criteria (L.M. and T.T.). If no abstract was available, the full-text article was obtained to assess the relevance of the study. The full text was subsequently reviewed for possible inclusion in the systematic review for all articles that were not excluded during the initial screening process. A third reviewer (H.E.) resolved between-reviewer discrepancies. In addition to the electronic search, the reference lists of all included articles and review articles were manually searched (C.L., T.T., H.E.) for additional relevant articles. Moreover, if any systematic reviews on ML in sport injury prediction and prevention were identified during the screening process, the reference list was screened to identify any further studies.
Methodological quality
Methodological quality and risk of bias of included studies were determined by the Newcastle–Ottawa Scale (NOS) [45]. Eligible studies were independently rated by two authors blind to the study authors and institutions (L.M. and T.T.), with discrepancies resolved by a third author (H.E.). The NOS contains eight categories relating to methodological quality and each study was given an eventual score out of a maximum of 8 points. A score of 0–3 points equated to a low quality study, a score of 4–6 points equated to a moderate quality study, with a score of 7–8 points required for a study to be given a score of high quality.
Data extraction
Characteristics of all included studies (i.e. participants, type of study, sample size, etc.) and about ML used (i.e. data pre-processing, classification method, etc.) were extracted independently by two reviewers (H.E. and C.L.), with a third (L.M.) resolving potential discrepancies.
Data analysis
Two independent reviewers (L.M. and T.T.) assessed the quality of evidence using the GRADE methodology [18]. In the current review, evidence started at moderate certainty, since investigation of publication bias was not possible due to the small number of included trials. Then it was downgraded by one level for imprecision when the analysed sample was < 300 participants (serious imprecision was downgraded by two levels); and by one level for risk of bias when the mean NOS Score was < 6 out of 9. Between-reviewer discrepancies were resolved by a third investigator (R.S.).
Results
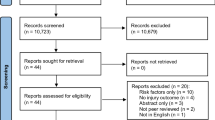
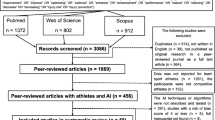
In the scope of this systematic literature review, 246 articles were found, and an additional three articles added by hand search from which a total of 11 articles were included according to the strict inclusion/exclusion criteria for this systematic review (Fig. 2).

PRISMA flow chart
Study characteristics
Table 1 lists all details of the included studies. Studies were prospective cohort studies (n = 9) [2, 11, 25, 27, 32, 35, 36, 38, 41] or case–control studies (n = 2) [41, 46]. Most of them were performed in soccer (n = 4) [2, 32, 35, 36] and Australian Football (n = 3).[11, 27, 38] Two studies incorporated athletes from multiple sports [25, 34]. The number of participants ranged between 25 and 363. In seven studies, the athlete was the unit of observation [2, 25, 32, 34, 35, 38, 46]. In the remaining 4 studies, there were multiple observations per player [11, 27, 36, 41]. Both occurrence (n = 11) [2, 11, 25, 27, 32, 34,35,36, 38, 41, 46] and type of injury (n = 2) (acute/overuse [35], contact/non-contact [27]) were evaluated, whereby lower limb muscle injury was the most often assessed outcome [2, 25, 38] and only one publication investigated specifically upper limb injuries [46].
Study Quality
The methodological quality of the included studies ranged from 5 to 8 in the NOS scale (Table 2). All studies had proper ascertainment of outcome/exposure; follow-up long enough for outcomes to occur, same method of ascertainment for cases and controls; and adequacy of follow-up of cohorts/non-response rate. Seven studies (63.63%) were downgraded for methodological quality due to imprecision and three (27.27%) because of risk of bias (Table 3).
Data analysis characteristics
In all 11 papers, the outcome variable was the occurrence of injury or the type of injury, which are categorical variables, making the base models classification models. From the 11 considered papers, 9 papers used tree-based models [2, 11, 25, 32, 34,35,36, 38, 41], 4 papers used Support Vector Machines [11, 34, 38, 46] and 2 papers used Artificial Neural Networks [27, 38]. Eight out of 9 papers using tree-based models applied a bagging strategy [2, 11, 25, 32, 34, 36, 38, 41], whereof 5 used a Random Forest approach [11, 34, 36, 38, 41]. Four papers used boosting algorithms to construct tree ensemble methods [2, 25, 32, 35].
The training, validation and test strategy for the used ML approaches varied largely between the different studies. For the evaluation and comparison of the methods, 7 papers [2, 25, 27, 32, 34, 36, 46] used cross-validation and 4 [11, 35, 38, 41] used a single data-splitting approach. Of the former, four [2, 25, 32, 36] used stratified cross-validation, which may be especially of interest in unbalanced data, because it ensures that in both training and test set the number of positive cases (injuries) is sufficiently high. In 4 papers [11, 34, 35, 38] the training dataset was split further for tuning the hyperparameters. In 3 papers [11, 36, 37] the authors repeated their entire analysis a large number of times to adjust for the randomness in the resampling and under/oversampling methods.
Three of the discussed papers used feature selection methods [34, 36, 46]. Rodas et al. [34] used the LASSO method for selecting significant features, Rossi et al. [36] eliminated features by applying cross-validation on a separate part of the data, and Whiteside et al. [46] evaluated all possible feature subsets. Carey et al. [11] used Principal Component Analysis for reducing the dimensionality of the data instead of feature selection.
To adjust for imbalanced data, the training datasets were over-and/or undersampled in 6 papers [2, 11, 25, 32, 36, 38]. All of them used oversampling of the minority class (injuries) and 4 of them applied undersampling of the majority class (non-injuries) [2, 11, 25, 32].
Data pre-processing was used in some papers to optimize the performance of the classification methods. To solve the missing values problem, three papers [2, 25, 34] mentioned using imputation methods. In three papers [2, 25, 32], the continuous variables were transformed into categorical variables, using cut-off values found in the literature or based on the data. There was only one paper [37] that mentioned a standardization of the continuous variables.
Some of the studies had small deficits in the Machine Learning Pipeline approach. Four papers in this review had multiple observations per athlete [11, 27, 36, 41] and it seems that players may appear in both the training and test datasets, which would be a violation of the rule that the training and test dataset should be independent from each other. The results of these studies can therefore not be generalized to a bigger population. The other mistakes were made in the preprocessing phase. Four papers [2, 25, 32, 38] seemed to perform discretization or standardization on the entire dataset (including test dataset), which in that case would be an example of data leakage, i.e. using the test data in the training process. This should be avoided since it does not reflect reality as the test dataset has to be seen as future data. On the other hand, Ruddy et al. [38] independently standardized the training and test dataset. Applying different transformations on the training and test dataset will cause non-optimal operation of the classifier and can lead to lower predictive performance. A structured overview of the data analysis characteristics can be found in Table 4.
Performance in predicting injury occurrence
In Table 5, the study results characteristics are given for each of the included papers. For predicting the occurrence of the outcome (injury in general, muscle injury, …), seven papers used Area Under the ROC Curve (AUC) as an evaluation measure [2, 11, 25, 32, 36, 38, 41], while the remaining four papers used only metrics based on the confusion matrix, e.g. accuracy, sensitivity, specificity, precision and f1-score. Eight out of eleven studies [2, 25, 27, 32, 35, 36, 41, 46] reported appropriate to good performance of the Machine Learning prediction methods. AUC values for predicting the outcome ranged between 0.64 and 0.87, and high values were found for accuracy (75%—82.9%), sensitivity (55.6%—94.5%), specificity (74.2%—87%) and precision (50%—85%). Three papers [11, 34, 38] reported low prediction potential for their built ML models, showing low AUC (0.52—0.65) and accuracy (52%) values.
Most important injury predictors
Analysed risk factors included both modifiable (training load, psychological and neuromuscular assessment, stress level, …) and non-modifiable (demographics, genetic markers, anthropometric measurements, previous injury, …) factors (for more details, see Table 1). In 4 papers [2, 25, 32, 41], the authors have counted the number of appearances of each feature in the final ensemble of decision trees. Two papers [34, 46] counted the number of times that a feature is selected by their feature selection procedure. Rossi et al. [36] used the decrease in Gini coefficient to measure the importance of variables and Rommers et al. [35] used a SHAP summary plot [26]. This plot was based on the Shapley values in game theory and shows the importance of the variables, as well as the relation between high/low feature values and high/low injury risk. Because of the wide variety of features used over the different papers, not much consistency was found in the reported important predictors. The features that were reported twice as important were previous injury [25, 36], higher training load [36, 41], and higher body size (in youth players only) [32, 35]. Note that lower training load after previous injury might indicate a not fully recovered athlete and can hence be considered being a risk factor after previous injury [36].
Discussion
The 11 studies included in this systematic review showed that ML methods can be successfully applied for sport injury prediction. The most promising results to predict injury risk were obtained in elite youth football players based on anthropometric, motor coordination and physical performance measures with a high accuracy of 85% [35], and in professional soccer based on a pre-season screening evaluation with a high sensitivity (77.8%) and specificity (83.8%).[2] This is in opposition with several authors who found that screening tests were not successful in predicting sports injuries [40, 43]. These results are promising in the sense that future models might help coaches, physical trainers and medical practitioners in the decision-making process for injury prevention.
Data inclusion was still limited in the analysed studies, where only selected variables were included (e.g., only anthropometric, motor coordination and physical performance measures in the study by Rommers et al. [35]). Nevertheless, the achieved accuracy was quite high and future prediction might become even higher by using smart machine learning approaches or by incorporating more data (e.g., using sensors, more intense monitoring of athletes) [44]. Future studies will need to refine the target of injury prediction with AI/ML. This can either be achieved with an increase of the number of different injuries affecting a specific population or a study cohort [35] or with a targeted inclusion of specific injuries with a high injury incidence like hamstring injuries in football or athletics [2, 38], or a high injury burden like anterior cruciate ligament (ACL) injuries in pivoting sports or ulnar collateral injuries in baseball [46]. The types and number of injury risk factors to be included in these studies are manifold and vary for each target. Large datasets may help the sports medicine community to improve the understanding of the respective influence of each factor on injury occurrence as well as their specific interactions in a given environment, allowing for a more systemic approach of sports injury prevention [6,7,8, 15].
In the new field of ML for sports injury prevention, the level of quality of the published studies is of utmost importance. The analysis of the methodological quality of the 11 included studies indicates that they had very-low to moderate methodological quality according to the GRADE analysis. Imprecision (i.e., a study including relatively few participants/events) is an issue that may be improved with multicentric studies. Only 3 studies [11, 36, 41] had a NOS score under 6 and only 1 study [32] scored in comparability. In fact, the main reason to a lower NOS score was lack of comparability, which indicates that either cases and controls or exposed and non-exposed individuals were not matched in the design and/or confounders were not adjusted for in the analysis. Oliver et al., the only paper considering comparability, recruited 6 professional football teams of the English Premier League and Championship and followed 355 athletes [32]. Injured and non-injured players were compared in all continuous variables and all 95% CI presented had proper range, indicating adequate matching between groups. Future studies should be aware of this common limitation and include the comparison between groups.
In terms of ML methodology, the following observations can be made from this review. (i) Tree-based models are currently the most popular ML models in sports medicine. They are easy to visualize and interpret, and they can be extended to ensemble methods for boosting and bagging purposes or adapted to be cost-sensitive. The two publications that did not use tree-based models were the first to be published on the subject [27, 46], thereby confirming the trend that more recent studies seem to adhere to this methodology. (ii) Concerning training and evaluating the ML models, a big variety between the 11 papers could be noticed. It was surprising to see that only 4 papers [11, 34, 35, 38] mentioned having tuned the hyperparameters to optimize the performance of the ML methods, since tuning hyperparameters is recommendable (though not mandatory) in order to take the most out of the ML methods. The other studies may have used values from the literature or the default values from the used software, which may have led to a failure to identify the optimal model. (iii) The findings from this review further reveal that future studies involving ML approaches in the field of sports injury prevention should aim for a higher methodological quality. One of the identified deficits of the analysed studies was the dependency between training and test datasets.
The predictive performance of the considered publications was very heterogeneous. It should be emphasized that the reported predictive performances cannot be seen as a quality measure of the ML analysis per se, because they are depending on many other factors, like the kind of included risk factors, the design of the study, the sample size or the unit of observation. This also appeared when the publications of Ayala et al. [2], Lopez-Valenciano et al. [25] and Oliver et al. [32] were compared to each other. They used similar preprocessing and processing steps and classification trees, but reported very different performance values (AUC ranging from 0.663 to 0.873). Furthermore, the reported measures (AUC, accuracy, sensitivity, specificity) might not be the best measures to evaluate the prediction models, since these measures only see black and white (injured or not injured), while probabilistic scoring rules, such as the Brier Score and the Logarithmic Loss, would be able to evaluate the exactness of a predicted probability (e.g. this player has 30% chance to get injured) as is stated by Carey et al.[10]. From a clinical point of view, it could be more informative to know the probability of injury instead of only the classification into a high or low risk profile.
When dealing with injury prediction and prevention, it is important to identify especially modifiable risk factors, which can be intrinsic or extrinsic [28]. While some studies did not provide any information on the relative importance or influence of an individual risk factor, others used the number of times that a considered variable appeared in the ensemble of decision trees. Rossi et al. [36] measured how much the predictive performance of an algorithm would decrease if a specific variable would be left out as a predictor. Rommers et al. [35] provided a visualisation of the influence of the risk factors on the predicted injury risk. Therefore, it appeared that more efforts should be done to understand the relative weight of individual risk factors on the injury risk. This approach may help guiding practitioners to apply targeted interventions to the athletes at high injury risk.
Limitations of the systematic review
Besides investigating the outcome of machine learning algorithms in injury prediction and prevention, this systematic review also focused on the methodology of AI/ML studies, which makes some parts probably challenging to read for sports medicine clinicians. To avoid misinterpretation, a brief summary of AI/ML methods was included. It is important to stress that a previous review of Claudino et al. [12] about the use of AI in team sports provided a first overview of the topic, however it included methods that were used in a clearly statistical way, such as Bayesian logistic regression and single decision tree classifiers. Using this categorization implies that studies which were performed before the era of AI/ML and including statistical methods like linear or logistic regression would need to be considered to get a complete overview of the topic. This would seriously dilute true ML approaches. Another limitation is the fact that only PubMed database was included in this review. Even though, more relevant studies were found compared to reviews using other databases, such as e.g. in Claudino et al. [12].
Conclusion
This systematic review showed that ML methods may be used to identify athletes at high injury risk during sport participation and that it may be helpful to identify risk factors. However, although the majority of the analysed studies did apply machine learning methods properly to predict injuries, the methodological study quality was moderate to very low. Sports injury prediction is a growing area and further developments in this promising field should be encouraged with respect to the big potential of AI/ML methods.
Availability of data and materials
Not applicable.
References
Adetiba E, Iweanya VC, Popoola SI, Adetiba JN, Menon C (2017) Automated detection of heart defects in athletes based on electrocardiography and artificial neural network. Cogent Eng 4:1411220
Ayala F, López-Valenciano A, Gámez Martín JA, De Ste CM, Vera-Garcia FJ, García-Vaquero MDP, Ruiz-Pérez I, Myer GD (2019) A Preventive Model for Hamstring Injuries in Professional Soccer: Learning Algorithms. Int J Sports Med 40:344–353. https://doi.org/10.1055/a-0826-1955
Bahr R, Clarsen B, Ekstrand J (2018) Why we should focus on the burden of injuries and illnesses, not just their incidence. Br J Sports Med 52:1018–1021. https://doi.org/10.1136/bjsports-2017-098160
Bahr R, Krosshaug T (2005) Understanding injury mechanisms: a key component of preventing injuries in sport. Br J Sports Med 39:324–329. https://doi.org/10.1136/bjsm.2005.018341
Bartlett JD, O’Connor F, Pitchford N, Torres-Ronda L, Robertson SJ (2017) Relationships Between Internal and External Training Load in Team-Sport Athletes: Evidence for an Individualized Approach. Int J Sports Physiol Perform 12:230–234. https://doi.org/10.1123/ijspp.2015-0791
Bittencourt NFN, Meeuwisse WH, Mendonça LD, Nettel-Aguirre A, Ocarino JM, Fonseca ST (2016) Complex systems approach for sports injuries: moving from risk factor identification to injury pattern recognition-narrative review and new concept. Br J Sports Med 50:1309–1314. https://doi.org/10.1136/bjsports-2015-095850
Bolling C, van Mechelen W, Pasman HR, Verhagen E (2018) Context Matters: Revisiting the First Step of the “Sequence of Prevention” of Sports Injuries. Sports Med Auckl NZ 48:2227–2234. https://doi.org/10.1007/s40279-018-0953-x
Bolling C, Mellette J, Pasman HR, van Mechelen W, Verhagen E (2019) From the safety net to the injury prevention web: applying systems thinking to unravel injury prevention challenges and opportunities in Cirque du Soleil. BMJ Open Sport Exerc Med 5:e000492. https://doi.org/10.1136/bmjsem-2018-000492
Cabitza F, Locoro A, Banfi G (2018) Machine Learning in Orthopedics: A Literature ReviewFront Bioeng Biotechnol 6.https://doi.org/10.3389/fbioe.2018.00075
Carey DL, Crossley KM, Whiteley R, Mosler A, Ong K-L, Crow J, Morris ME (2018) Modeling Training Loads and Injuries: The Dangers of Discretization. Med Sci Sports Exerc 50:2267–2276. https://doi.org/10.1249/MSS.0000000000001685
Carey DL, Ong K, Whiteley R, Crossley KM, Crow J, Morris ME (2018) Predictive modelling of training loads and injury in Australian football. Int J ComputSci Sport 17:49–66
Claudino JG, de Capanema D, O, de Souza TV, Serrão JC, Machado Pereira AC, Nassis GP, (2019) Current Approaches to the Use of Artificial Intelligence for Injury Risk Assessment and Performance Prediction in Team Sports: a Systematic Review. Sports Med - Open 5:28. https://doi.org/10.1186/s40798-019-0202-3
Emery CA, Pasanen K (2019) Current trends in sport injury prevention. Best Pract Res ClinRheumatol 33:3–15. https://doi.org/10.1016/j.berh.2019.02.009
Ertelt T, Solomonovs I, Gronwald T (2018) Enhancement of force patterns classification based on Gaussian distributions. J Biomech 67:144–149. https://doi.org/10.1016/j.jbiomech.2017.12.006
Fonseca ST, Souza TR, Verhagen E, van Emmerik R, Bittencourt NFN, Mendonça LDM, Andrade AGP, Resende RA, Ocarino JM (2020) Sports Injury Forecasting and Complexity: A Synergetic Approach. Sports Med Auckl NZ 50:1757–1770. https://doi.org/10.1007/s40279-020-01326-4
Gastin PB, Hunkin SL, Fahrner B, Robertson S (2019) Deceleration, Acceleration, and Impacts Are Strong Contributors to Muscle Damage in Professional Australian Football. J Strength Cond Res 33:3374–3383. https://doi.org/10.1519/JSC.0000000000003023
Groll A, Ley C, Schauberger G, Eetvelde HV (2019) A hybrid random forest to predict soccer matches in international tournaments. J Quant Anal Sports 15:271–287. https://doi.org/10.1515/jqas-2018-0060
Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, Schünemann HJ (2008) GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 336:924–926. https://doi.org/10.1136/bmj.39489.470347.AD
Hasler RM, Berov S, Benneker L, Dubler S, Spycher J, Heim D, Zimmermann H, Exadaktylos AK (2010) Are there risk factors for snowboard injuries? A case-control multicentre study of 559 snowboarders. Br J Sports Med 44:816–821. https://doi.org/10.1136/bjsm.2010.071357
Hasler RM, Dubler S, Benneker LM, Berov S, Spycher J, Heim D, Zimmermann H, Exadaktylos AK (2009) Are there risk factors in alpine skiing? A controlled multicentre survey of 1278 skiers. Br J Sports Med 43:1020–1025. https://doi.org/10.1136/bjsm.2009.064741
Hubáček O, Šourek G, Železný F (2019) Learning to predict soccer results from relational data with gradient boosted trees. Mach Learn 108:29–47. https://doi.org/10.1007/s10994-018-5704-6
Klein C, Luig P, Henke T, Platen P (2020) Injury burden differs considerably between single teams from German professional male football (soccer): surveillance of three consecutive seasons. Knee Surg Sports TraumatolArthrosc Off J ESSKA 28:1656–1664. https://doi.org/10.1007/s00167-019-05623-y
Kuhn M, Johnson K (2013) Applied predictive modeling. Springer, New York
Liu Y, Chen P-HC, Krause J, Peng L (2019) How to Read Articles That Use Machine Learning: Users’ Guides to the Medical Literature. JAMA 322:1806–1816. https://doi.org/10.1001/jama.2019.16489
López-Valenciano A, Ayala F, PuertaJosM DE, Ste Croix MBA, Vera-Garcia FJ, Hernández-Sánchez S, Ruiz-Pérez I, Myer GD (2018) A Preventive Model for Muscle Injuries: A Novel Approach based on Learning Algorithms. Med Sci Sports Exerc 50:915–927. https://doi.org/10.1249/MSS.0000000000001535
Lundberg SM, Lee S-I (2017) A Unified Approach to Interpreting Model Predictions. In: Guyon I, Luxburg UV, Bengio S, Wallach H, Fergus R, Vishwanathan S, Garnett R (eds) 30th Conference on Neural Information Processing Systems (NIPS 2017). Curran Associates, Inc., LongBeach, p 4765–4774
McCullagh J, Whitfort T (2013) An investigation into the application of Artificial Neural Networks to the prediction of injuries in sport. Int J Sport Health Sci 7:356–360
Meeuwisse WH, Tyreman H, Hagel B, Emery C (2007) A dynamic model of etiology in sport injury: the recursive nature of risk and causation. Clin J Sport Med Off J Can Acad Sport Med 17:215–219. https://doi.org/10.1097/JSM.0b013e3180592a48
Mendonça LD, Ocarino JM, Bittencourt NFN, Macedo LG, Fonseca ST (2018) Association of Hip and Foot Factors With Patellar Tendinopathy (Jumper’s Knee) in Athletes. J Orthop Sports PhysTher 48:676–684. https://doi.org/10.2519/jospt.2018.7426
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Myers TG, Ramkumar PN, Ricciardi BF, Urish KL, Kipper J, Ketonis C (2020) Artificial Intelligence and Orthopaedics: An Introduction for Clinicians. JBJS 102:830–840. https://doi.org/10.2106/JBJS.19.01128
Oliver JL, Ayala F, De Ste Croix MBA, Lloyd RS, Myer GD, Read PJ (2020) Using machine learning to improve our understanding of injury risk and prediction in elite male youth football players. J Sci Med Sport. https://doi.org/10.1016/j.jsams.2020.04.021
Parker W, Forster BB (2019) Artificial intelligence in sports medicine radiology: what’s coming? Br J Sports Med 53:1201–1202. https://doi.org/10.1136/bjsports-2018-099999
Rodas G, Osaba L, Arteta D, Pruna R, Fernández D, Lucia A (2019) Genomic Prediction of Tendinopathy Risk in Elite Team Sports. Int J Sports Physiol Perform: 1–7.https://doi.org/10.1123/ijspp.2019-0431
Rommers N, RÖssler R, Verhagen E, Vandecasteele F, Verstockt S, Vaeyens R, Lenoir M, D’Hondt E, Witvrouw E, (2020) A Machine Learning Approach to Assess Injury Risk in Elite Youth Football Players. Med Sci Sports Exerc 52:1745–1751. https://doi.org/10.1249/MSS.0000000000002305
Rossi A, Pappalardo L, Cintia P, Iaia FM, Fernàndez J, Medina D (2018) Effective injury forecasting in soccer with GPS training data and machine learning. PLoS ONE 13:e0201264. https://doi.org/10.1371/journal.pone.0201264
Ruddy JD, Cormack SJ, Whiteley R, Williams MD, Timmins RG, Opar DA (2019) Modeling the Risk of Team Sport Injuries: A Narrative Review of Different Statistical Approaches. Front Physiol 10:829. https://doi.org/10.3389/fphys.2019.00829
Ruddy JD, Shield AJ, Maniar N, Williams MD, Duhig S, Timmins RG, Hickey J, Bourne MN, Opar DA (2018) Predictive Modeling of Hamstring Strain Injuries in Elite Australian Footballers. Med Sci Sports Exerc 50:906–914. https://doi.org/10.1249/MSS.0000000000001527
Shah P, Kendall F, Khozin S, Goosen R, Hu J, Laramie J, Ringel M, Schork N (2019) Artificial intelligence and machine learning in clinical development: a translational perspective. NPJ Digit Med 2:69. https://doi.org/10.1038/s41746-019-0148-3
Tervo T, Ermling J, Nordström A, Toss F (2020) The 9+ screening test score does not predict injuries in elite floorball players. Scand J Med Sci Sports 30:1232–1236. https://doi.org/10.1111/sms.13663
Thornton HR, Delaney JA, Duthie GM, Dascombe BJ (2017) Importance of Various Training-Load Measures in Injury Incidence of Professional Rugby League Athletes. Int J Sports Physiol Perform 12:819–824. https://doi.org/10.1123/ijspp.2016-0326
Topol EJ (2019) High-performance medicine: the convergence of human and artificial intelligence. Nat Med 25:44–56. https://doi.org/10.1038/s41591-018-0300-7
Trinidad-Fernandez M, Gonzalez-Sanchez M, Cuesta-Vargas AI (2019) Is a low Functional Movement Screen score (≤14/21) associated with injuries in sport? A systematic review and meta-analysis. BMJ Open Sport Exerc Med 5:e000501. https://doi.org/10.1136/bmjsem-2018-000501
Verhagen E, Bolling C (2015) Protecting the health of the @hlete: how online technology may aid our common goal to prevent injury and illness in sport. Br J Sports Med 49:1174–1178. https://doi.org/10.1136/bjsports-2014-094322
Wells G, Shea B, O’Connell D, Robertson J, Peterson J, Welch V, Losos M, Tugwell P The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta- Analysis. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 28 June 2020
Whiteside D, Martini DN, Lepley AS, Zernicke RF, Goulet GC (2016) Predictors of Ulnar Collateral Ligament Reconstruction in Major League Baseball Pitchers. Am J Sports Med 44:2202–2209. https://doi.org/10.1177/0363546516643812
Acknowledgements
Not applicable
Funding
No special funding existed for the performed study.
Author information
Authors and Affiliations
Contributions
TT, HVE and LDM designed the search strategy and the overall setup of the systematic review. HVE and CL performed the technical analysis of the included studies. TT and LDM performed the methodological quality analysis of the articles. All authors drafted the manuscript and performed multiple revisions. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: S1.
Definitions of core terms important for AI application in sport injury prediction and prevention.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Van Eetvelde, H., Mendonça, L.D., Ley, C. et al. Machine learning methods in sport injury prediction and prevention: a systematic review. J EXP ORTOP 8, 27 (2021). https://doi.org/10.1186/s40634-021-00346-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40634-021-00346-x