
Abstract
Objectives
Arterial catheters (ACs) are critical for haemodynamic monitoring and blood sampling but are prone to complications. We investigated the incidence and risk factors of AC failure.
Methods
Secondary analysis of a multi-centre randomised controlled trial (ACTRN 12610000505000). Analysis included a subset of adult intensive care unit patients with an AC. The primary outcome was all-cause device failure. Secondary outcomes were catheter associated bloodstream infection (CABSI), suspected CABSI, occlusion, thrombosis, accidental removal, pain, and line fracture. Risk factors associated with AC failure were investigated using Cox proportional hazards and competing-risk models.
Results
Of 664 patients, 173 (26%) experienced AC failure (incidence rate [IR] 37/1000 catheter days). Suspected CABSI was the most common failure type (11%; IR 15.3/1000 catheter days), followed by occlusion (8%; IR 11.9/1,000 catheter days), and accidental removal (4%; IR 5.5/1000 catheter days). CABSI occurred in 16 (2%) patients. All-cause failure and occlusion were reduced with ultrasound-assisted insertion (failure: adjusted hazard ratio [HR] 0.43, 95% CI 0.25, 0.76; occlusion: sub-HR 0.11, 95% CI 0.03, 0.43). Increased age was associated with less AC failure (60–74 years HR 0.63, 95% CI 0.44 to 0.89; 75 + years HR 0.36, 95% CI 0.20, 0.64; referent 15–59 years). Females experienced more occlusion (adjusted sub-HR 2.53, 95% CI 1.49, 4.29), while patients with diabetes had less (SHR 0.15, 95% CI 0.04, 0.63). Suspected CABSI was associated with an abnormal insertion site appearance (SHR 2.71, 95% CI 1.48, 4.99).
Conclusions
AC failure is common with ultrasound-guided insertion associated with lower failure rates.
Trial registration Australian New Zealand Clinical Trial Registry (ACTRN 12610000505000); date registered: 18 June 2010.
Similar content being viewed by others


Introduction
Arterial catheterisation is a common procedure in intensive care and anaesthetic departments worldwide. More than 10 million arterial catheters (ACs) are placed in the United States and Europe each year [1,2,3] to support continuous haemodynamic monitoring, blood sampling [2, 4] or arterial blood gas monitoring. ACs are associated with risks such as infection [2, 5,6,7,8], occlusion [4, 9,10,11,12], thrombosis [5, 6, 9, 13,14,15,16], and dislodgement [16, 17]. Such complications contribute to substantial patient morbidity by prolonging intensive care unit (ICU) length of stay [1, 14, 18], thereby increasing potential health care costs.
International cohort studies suggest significant variation in AC use and maintenance practices—more so than with central venous catheters [19,20,21]. This variation likely stems from a lack of data regarding appropriate AC maintenance and risk factors associated with AC complications [19, 20]. Few studies have investigated complications using multivariable analysis techniques, and all have focussed solely on infection outcomes [22,23,24,25,26,27]. A detailed understanding of such risk factors, and conversely, the protective factors is lacking. To address this gap, we conducted a secondary analysis of a multi-site randomised controlled trial (RCT) which compared the effectiveness and costs of 7-day (intervention) versus 4-day (control) infusion set replacement in patients requiring central venous and peripheral arterial access. Our objectives were to: i) determine the prevalence and cause of AC failure and device complications; and ii) determine predictors of AC failure and device complications. We hypothesised that specific patient-, provider- (inserter) and catheter-related characteristics would be associated with AC failure and complications. Given the omnipresence of ACs in the ICU we sought to identify modifiable risk factors which may inform interventions for future clinical trials.
Methods
Study design and sample population
We conducted a secondary analysis of data from a multi-site RCT. All adult patients aged > 16 years with an AC were included. Ethical approval was obtained from Griffith University (Ref No: 2021/834). The study reporting follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [28].
The parent study, from which the data was sourced, is the Replacement after Standard Versus Prolonged use (RSVP) trial, which tested the effect of 4- versus 7-day infusion set replacement intervals [17] in a ten-site (including 5 ICUs; all level 3 facilities) Australian RCT conducted between May 2011 and December 2016 [17] (ACTRN12610000505000). RSVP enrolled 2944 patients of all ages (excluding neonatal ICU patients). Eligible patients required the insertion of a central venous and/or AC, with the device in situ for > 24 h, and expected to be used for ≥ 7 days [29]. The primary endpoint was catheter-related bloodstream infections. Sites obtained institutional review approvals and informed written consent was obtained or waived as per local ethical requirements. Of the 2944 patients enrolled in RSVP, 664 adults received a PAC.
Outcomes
The primary outcome was all-cause AC failure, defined as cessation of catheter function prior to the completion of necessary therapy [30]. Secondary outcomes were individual complications including: suspected catheter associated bloodstream infection ([CABSI]; provider assessed) or microbiologically proven CABSI, defined in line with international recommendations [31], AC occlusion, thrombosis, accidental removal, or line fracture [32, 33].
Variables
The parent study (RSVP) collected patient demographic and clinical characteristics including age, sex, admission diagnosis, ICU length of stay, ventilation requirement and severity of critical illness (The Acute Physiology and Chronic Health Evaluation [APACHE II]), as well as device and provider characteristics (e.g., insertion site, catheter material, insertion technique and inserter designation) for each participant. Data were collected using the web-based platform Research Electronic Data Capture (REDCap; Vanderbilt University) [34].
Statistical analysis
Participant demographic and AC characteristics (1 AC per participant was studied) are reported descriptively using frequency (percentage) for categorical data and mean (standard deviation) or median (interquartile range; IQR) for continuous variables depending on normality of distribution. The incidence of device failure was calculated using Poisson regression, offset by the natural logarithm of days at risk. Failure and complications are presented as incidence rate per 1000 catheter days with 95% confidence interval (CI). To investigate risk factors for failure, a Cox proportional hazards model was used for all-cause failure. When investigating the component failure outcomes suspected/confirmed CABSI, blockage and accidental removal, competing-risks regression models were used to account for possible failure due to other reasons. Multivariable models were not constructed for other failure types due to low incidence. Risk estimates are presented as hazard ratio (HR) for failure, and sub-hazard ratio (SHR) for complication types. Patient, clinical and device characteristics, but not the RCT study group, were considered for inclusion in the best multivariable model. The Bayesian information criterion (BIC) statistic was used to identify the model with the most explanatory power relative to its complexity. The BIC was calculated for all possible models and the model with the smallest BIC was chosen as the best final model. Kaplan Meier and competing-risks regression curves were plotted. All analyses were performed using Stata v15.1 (StataCorp, College Station, TX).
Results
Patient characteristics
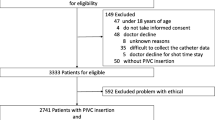
Included in this secondary analysis were 664 adults who required an AC (Fig. 1). Patients were predominately male (n = 449; 68%), aged between 16 and 59 years (n = 346; 52%) and admitted for a medical condition (n = 316, 48%; Table 1). Eighteen percent (n = 118) of patients had a current infection, most commonly respiratory (n = 65; 10%). Seventy-nine percent (n = 524) of patients required mechanical ventilation, with the median ICU length of stay, at time of device insertion 4 days (IQR 3, 4).

Patient flow chart. Uploaded as high quality DPI image
Figure 1 Flowchart illustrating how the analysis population evaluated in this secondary analysis was derived from the overall intention-to-treat population of the RSVP trial.
AC characteristics
All ACs were inserted by physicians, predominately in ICU (n = 422; 64%). ACs were generally inserted on the first attempt (n = 638; 98%), using landmark technique (n = 501; 76%) in the radial artery (n = 551; 83%). ACs were either peripheral venous catheters or arterial catheters (with introducer), secured with multiple dressing and securement products (n = 569; 85%), including simple transparent dressings. Heparin saline (2 iu/ml) or 0.9% normal saline were used in pressurised transducer tubing depending on local hospital policy.
AC and patient outcomes
Of the 664 patients with ACs, 491 (74%) completed therapy. One hundred and seventy-three patients (26%) experienced AC failure (Table 2). Median AC dwell was 6.5 days (IQR 4.8, 8.5) in all catheters and 4.8 days (IQR 3.5, 6.5) in catheters which failed. Most catheters were removed during daylight hours (0700–1900 h; n = 534; 80%). All-cause AC failure incidence rate (IR) was 37.0 per 1000 catheter days (95% confidence interval [CI] 31.7, 42.7). Suspected CABSI, with 11% was the most common reason for premature device removal (IR 15.3; 95% CI 12.2, 19.3). AC occlusion occurred in 8% of patients (IR 11.9, 95% CI 9.2, 15.5), followed by 4% accidental removal (IR 5.5; 95% CI 3.8, 8.1). CABSI was confirmed in 2% equating to 16/72 (22%) of suspected CABSI. Central venous catheters were ruled out as the source of the confirmed CABSI in ACs. Removal for fracture, pain and thrombus were rare.
Univariable associations of patient, provider (inserter) and device characteristics with all types of AC failure are outlined in Additional file 1. The most appropriate multivariable models as identified using BIC are presented in Additional file 2.
Risk factors for all-cause failure
Variables associated univariably with increased AC failure were: female gender (HR 1.38, 95% CI 1.01, 1.88), abnormal site check (on nursing assessment; HR 2.09, 95% CI 1.31, 3.34), surgical emergency admission (HR 2.35, 95% CI 1.59, 3.47), or trauma and burns admission (HR 2.19, 95% CI 1.43 to 3.33), compared to a medical admission. Variables associated with decreased AC failure were increasing years of age (60–74 years, HR 0.64 95% CI 0.46, 0.91;75 + years, HR 0.36, 95% CI 0.21, 0.62) compared to being aged 16–59 years, ultrasound-guided AC insertion (HR 0.45, 95% CI 0.30, 0.69), antibiotics during AC dwell (HR 0.65, 95% CI 0.45, 0.93), and higher APACHE score (APACHE 20–29, HR 0.50, 95% CI 0.29, 0.86; APACHE 30–49 HR 0.49, 95% CI 0.22, 1.00) compared with an APACHE of 10–19).
When considering multivariable models (Table 3), ultrasound insertion (HR 0.48, 95% 0.31, 0.73) and increasing age (60–74 years HR 0.63, 95% CI 0.44 to 0.89; 75 + years HR 0.36, 95% CI 0.20, 0.64) compared to age 15–59 years were the two variables included in the most parsimonious model, with both models associated with reduced AC failure risk.
Risk factors for suspected CABSI
For suspected CABSI, univariable analyses identified AC placement in the femoral artery (SHR 2.21, 95% CI 1.15, 4.23) rather than the radial artery, trauma/burns diagnosis (SHR 2.61, 95% CI 1.42, 4.79) compared to medical diagnosis, and abnormal AC site on nursing check (SHR 2.70, 95% CI 1.47 to 4.96) as factors associated with increased risk. Being aged 60–74 years decreased risk compared to being aged 15–59 years (SHR 0.30 95% CI 0.11, 0.83).
On multivariable analyses, abnormal AC site on nursing check remained associated with suspected CABSI (SHR 2.71, 95% CI 1.48, 4.99).
Risk factors for proven CABSI
No variables were identified as being significantly associated with proven CABSI.
Risk factors for occlusion
On univariate analyses, AC occlusion was higher in females (SHR 2.66, 95% CI 1.57, 4.53), trauma or burn injuries (SHR 2.24, 95% CI 1.05, 4.80), or a surgical emergency (SHR 3.18, 95% CI 1.67, 6.02) compared to a medical admission, and in patients with AC placement in the dorsalis pedis rather than the radial artery (SHR 3.03, 95% CI 1.08, 8.45). Ultrasound-guided insertion (SHR 0.11, 95% CI 0.03, 0.47), receipt of antibiotic therapy (SHR 0.50, 95% CI 0.28, 0.90), and having a diabetes comorbidity (SHR 0.15, 95% CI 0.04, 0.63) were associated with less AC occlusion, as were increasing age (60–74 years, SHR 0.49, 95% CI 0.26, 0.93; 75 + years, SHR 0.32; 95% CI 0.11, 0.88) compared to being aged 16–59 years.
In the best multivariable model, ultrasound-guided insertion and diabetes remained associated with reduced occlusion (SHR 0.12, 95% 0.03, 0.49 and 0.18, 0.04, 0.73 respectively), whilst female gender remained associated with an increased risk of occlusion (SHR 2.44, 95% CI 1.43, 4.18; Table 3).
Risk factors for accidental removal
On univariable analyses, accidental AC removal was more likely to occur in patients admitted to ICU following a surgical emergency, compared to admission for a medical diagnosis (SHR 3.17, 95% CI 1.25, 8.03). Patients with an APACHE of 0–9 were more likely to experience accidental removal when compared with patients with an APACHE of 10–19 (SHR 3.47, 95% 1.18, 10.20).
No factors remained significantly associated with accidental removal in the multivariable models.
Discussion
In this heterogeneous adult ICU cohort, unplanned early removal of ACs was common (1 in 4 ACs). ACs were most commonly removed due to suspected infection, followed by occlusion and accidental removal. We showed that ultrasound-guided AC insertion and increasing patient age reduced the relative risk of catheter failure, and that females have more than double the risk of AC occlusion, following adjustment for other patient, provider, and device specific factors.
Similar to peripheral IV catheter insertion [35, 36] we showed that use of ultrasound for AC insertion was a protective factor against all cause failure, suspected infection, and occlusion [37, 38]. Despite finding a high first attempt insertion rate, data suggests ultrasound use for AC insertion is beneficial, supporting appropriate vessel and site selection, shorten insertion time, and enhance procedural accuracy [39,40,41]. In this cohort only 24% of ACs were inserted using ultrasound, demonstrating the device is overlooked for this procedure despite international guidelines such as The Infusion Therapy Standards of Practice [42] recommending ultrasound use for AC insertion. Previous studies offer explanations for this lack of uptake, highlighting barriers such as resourcing, training, and organisational support as key contributors to the ad hoc use of ultrasound [38, 43, 44].
Suspected CABSI was the most common reason for premature device removal and patients who had their AC inserted with ultrasound had an almost twofold-reduced risk of suspected CABSI. While clinical practice varies, catheter-related infection is typically suspected when the patient exhibits new and unexplained signs of sepsis and the catheter has been in place for more than 4 days, and suspicion is heightened by any redness or discharge from the AC site [45]. Guidelines [46] for preventing catheter-related infections recommend that catheter cultures are performed when a catheter is removed for suspected infection so as to enable diagnosis and bacterial identification. Yet AC removal often requires insertion of a replacement device, while diagnosis of bloodstream infection and causative pathogens is time-consuming and retrospective. This may explain why many suspected CABSI cases lead to AC removal without cultures being taken, a situation likely leading to underdiagnosis of confirmed CABSI. Point of care diagnostics for the rapid detection of bacteraemia in ICU remain limited in application however would facilitate fast diagnosis, timely treatment and potentially decrease the volume of ACs removed on suspicion of infection [47]. This would be particularly useful in confirming diagnosis in ICU patients who typically have a higher bacterial load, while protecting those who have poor vessel health from unnecessary removals [48].
Our findings suggest that AC occlusion is a key complication necessitating premature device removal in ICU. AC occlusion often occurs in ICU due to intimal hyperplasia, intima–media thickening and luminal thrombosis [10]. We identified patients with diabetes who were 2.4 times more likely to develop an AC occlusion. Evidence suggests this may be a result of the increased platelet responsiveness (hyperactivity), making patients with diabetes more prone to developing thromboses [49]. Further diabetes is associated with atherosclerotic narrowing of peripheral arteries and thus may contribute to an increased rate of occlusions [50]. Female gender was the strongest, non-modifiable predictor of AC occlusion. Female patients were 2.7 times more likely to experience catheter blockage compared to male counterparts. Concerningly, full recovery of radial arterial blood flow can take up to 7 days post AC removal [51]. Our finding aligns with existing evidence which demonstrates female patients are three times more likely to develop AC thrombosis [15]. An increased thrombosis risk in females has also been demonstrated in other vascular catheters including peripheral intravenous catheters [52]. Studies have attributed this increased risk to females having higher fibrin production and reduced markers of fibrinolysis, thereby increasing their overall coagulation potential [53]. Further, females typically have a smaller vessel diameter, in this case arterial, which can contribute to stenosis and occlusion if the catheter to vein ratio is consistently reduced [54, 55]. Females’ predisposition towards higher fibrin generation highlights the need to ensure correct technique for blood draws on arterial catheters. Shear rates and turbulence – the speed at which the blood draw is completed—is an important factor in the coagulation cascade and intima–media thickening, with both platelet adhesion and activation and thrombin generation increased under conditions of shear stress [56, 57]. Further work should examine the impact of interventions which reduce the risk of catheter thrombosis (e.g., AC gauge) and address women’s unique clotting factors (e.g., addressing the clotting cascade, AC material).
Our analysis is associated with several strengths. First, we used high-quality data from a large multisite RCT, prospectively collected. Secondly, device complications were prospectively monitored using rigorous definitions and, in the case of CABSI, blinded outcome assessors. The finding of increasing age being a protective factor against AC failure may be related to the reduced inflammatory response in elderly patients [58], or the effect of aging on vascular endothelium and structural integrity in arteries [59] which warrants further enquiry, Our analysis has some limitations, mainly its exploratory nature and its setting in one country. Due to the low event rates, results should be interpreted with caution, particularly the accidental removal analysis which had fewer patients. Secondly, as a secondary analysis we were not able to collect additional data restricting the number of predictor variables in risk-adjustment models points (e.g., sedation level, coagulation profile/ platelet inhibition, institutional practices, race). Third, routine replacement may have been a competing risk with 20% of devices routinely replaced, a practice not recommended in clinical guidelines. In the pragmatic RCT, AC maintenance was based on local guidelines informed by international evidence (Centre for Disease Control guidelines) [41]. There was some variation in AC maintenance and we did not adjust for site-level clustered variables such as use of heparinized or non-heparinized saline flush infusions, although these have not been shown effective in prior research [60]. Overall, further interventional studies are required to ascertain the benefit of strategies in female patients to reduce thrombosis risk and understand factors promoting translation of ultrasound guided AC insertion for patients across critical care and anaesthetic settings.
Conclusion
Our secondary analysis of the RSVP trial demonstrated a clinically concerning incidence of AC failure. We identified younger age to be associated with increased risk, female patients as at significantly higher risk of occlusion, while patients with diabetes had reduced risk. Ultrasound-guided insertion was significantly associated with reduced AC failure and occlusion, lending support to increased use of this technology.
Availability of data and materials
The data that support the findings of this study may be made available on request to the corresponding author, but ethical restrictions apply to the availability of these data, and so are not publicly available. Data may be made available upon reasonable request and with permission of Griffith University HREC at research-ethics@griffith.edu.au.
Abbreviations
- AC:
-
Arterial catheter
- APACHE II:
-
Acute Physiology and Chronic Health Evaluation
- BIC:
-
Bayesian Information Criterion
- CABSI:
-
Catheter associated blood stream infection
- CI:
-
Confidence Interval
- HR:
-
Hazard Ratio
- ICU:
-
Intensive care unit
- IR:
-
Incidence rate
- IQR:
-
Interquartile range
- RCT:
-
Randomised controlled trial
- RSVP:
-
Replacement after Standard Versus Prolonged use trial
- SHR:
-
Sub-hazard ratio
- STROBE:
-
Strengthening the Reporting of Observational Studies in Epidemiology
References
Cousins TR, O’Donnell JM. Arterial cannulation: a critical review. AANA J. 2004;72(4):267–71.
Gleich SJ, Wong AV, Handlogten KS, Thum DE, Nemergut ME. Major short-term complications of arterial cannulation for monitoring in children. Anesthesiology. 2021;134(1):26–34.
Scheer B, Perel A, Pfeiffer UJ. Clinical review: complications and risk factors of peripheral arterial catheters used for haemodynamic monitoring in anaesthesia and intensive care medicine. Crit Care. 2002;6(3):199–204.
Wujtewicz M, Regent B, Marszałek-Ratnicka R, Smugała A, Szurowska E, Owczuk R. The incidence of radial artery occlusion in critically ill patients after cannulation with a long catheter. J Clin Med. 2021;10(14):3172.
Kim D, Arbra CA, Simon Ivey J, Burchett P, Gonzalez G, Herrera FA. Iatrogenic radial artery injuries: variable injury patterns, treatment times, and outcomes. Hand (N Y). 2021;16(1):93–8.
Garg K, Howell BW, Saltzberg SS, Berland TL, Mussa FF, Maldonado TS, et al. Open surgical management of complications from indwelling radial artery catheters. J Vasc Surg. 2013;58(5):1325–30.
Safdar N, O’Horo JC, Maki DG. Arterial catheter-related bloodstream infection: incidence, pathogenesis, risk factors and prevention. J Hosp Infect. 2013;85(3):189–95.
Hambsch ZJ, Kerfeld MJ, Kirkpatrick DR, McEntire DM, Reisbig MD, Youngblood CF, et al. Arterial catheterization and infection: toll-like receptors in defense against microorganisms and therapeutic implications. Clin Transl Sci. 2015;8(6):857–70.
Brotschi B, Hug MI, Latal B, Neuhaus D, Buerki C, Kroiss S, et al. Incidence and predictors of indwelling arterial catheter-related thrombosis in children. J Thromb Haemost. 2011;9(6):1157–62.
Brancati MF, Burzotta F, Coluccia V, Trani C. The occurrence of radial artery occlusion following catheterization. Expert Rev Cardiovasc Ther. 2012;10(10):1287–95.
Schindler E, Kowald B, Suess H, Niehaus-Borquez B, Tausch B, Brecher A. Catheterization of the radial or brachial artery in neonates and infants. Paediatr Anaesth. 2005;15(8):677–82.
Hadad MJ, Puvanesarajah V, Deune EG. Complications of transradial catheterization and cannulation. J Hand Surg Am. 2019;44(11):973–9.
Handlogten KS, Wilson GA, Clifford L, Nuttall GA, Kor DJ. Brachial artery catheterization: an assessment of use patterns and associated complications. Anesth Analg. 2014;118(2):288–95.
Singh A, Bahadorani B, Wakefield BJ, Makarova N, Kumar PA, Tong MZ, et al. Brachial arterial pressure monitoring during cardiac surgery rarely causes complications. Anesthesiology. 2017;126(6):1065–76.
Fleury Y, Arroyo D, Couchepin C, Robert-Ebadi H, Righini M, Lobrinus JA, et al. Impact of intravascular thrombosis on failure of radial arterial catheters in critically ill patients: a nested case-control study. Intensive Care Med. 2018;44(5):553–63.
Schellenberg M, Hawley L, Biswas S, Clark DH, Cobb JP. Complications following brachial arterial catheterization in the surgical intensive care unit. Am Surg. 2020;86(10):1260–3.
Rickard CM, Marsh NM, Larsen EN, McGrail MR, Graves N, Runnegar N, et al. Effect of infusion set replacement intervals on catheter-related bloodstream infections (RSVP): a randomised, controlled, equivalence (central venous access device)-non-inferiority (peripheral arterial catheter) trial. Lancet. 2021;397(10283):1447–58.
Lorente L, Santacreu R, Martín MM, Jiménez A, Mora ML. Arterial catheter-related infection of 2949 catheters. Crit Care. 2006;10(3):R83-R.
Gershengorn HB, Wunsch H, Scales DC, Zarychanski R, Rubenfeld G, Garland A. Association between arterial catheter use and hospital mortality in intensive care units. JAMA Intern Med. 2014;174(11):1746–54.
Gershengorn HB, Garland A, Kramer A, Scales DC, Rubenfeld G, Wunsch H. Variation of arterial and central venous catheter use in United States intensive care units. Anesthesiology. 2014;120(3):650–64.
Mahendra M, McQuillen P, Dudley RA, Steurer MA. Variation in arterial and central venous catheter use in pediatric intensive care units. J Intensive Care Med. 2021;36(11):1250–7.
Hammarskjöld F, Berg S, Hanberger H, Malmvall BE. Low incidence of arterial catheter infections in a Swedish intensive care unit: risk factors for colonisation and infection. J Hosp Infect. 2010;76(2):130–4.
Koh DB, Gowardman JR, Rickard CM, Robertson IK, Brown A. Prospective study of peripheral arterial catheter infection and comparison with concurrently sited central venous catheters. Crit Care Med. 2008;36(2):397–402.
Lorente L, Jiménez A, Martín MM, Naranjo C, Roca I, Mora ML. Lower catheter-related bloodstream infection in arterial than in venous femoral catheter. Eur J Clin Microbiol Infect Dis. 2012;31(4):487–90.
O’Horo JC, Maki DG, Krupp AE, Safdar N. Arterial catheters as a source of bloodstream infection: a systematic review and meta-analysis. Crit Care Med. 2014;42(6):1334–9.
Lucet JC, Bouadma L, Zahar JR, Schwebel C, Geffroy A, Pease S, et al. Infectious risk associated with arterial catheters compared with central venous catheters. Crit Care Med. 2010;38(4):1030–5.
Buetti N, Mimoz O, Schwebel C, Ruckly S, Castry M, Dupuis C, et al. Insertion site and infection risk among peripheral arterial catheters. Am J Respir Crit Care Med. 2021;203(5):630–3.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147(8):573–7.
Rickard CM, Marsh NM, Webster J, Gavin NC, McGrail MR, Larsen E, et al. Intravascular device administration sets: replacement after standard versus prolonged use in hospitalised patients—a study protocol for a randomised controlled trial (The RSVP Trial). BMJ Open. 2015;5(2): e007257.
Schults JA, Long D, Pearson K, Takashima M, Baveas T, Schlapbach LJ, et al. Insertion, management, and complications associated with arterial catheters in paediatric intensive care: a clinical audit. Aust Crit Care. 2019;33(4):326–32.
National Healthcare Safety Network. Bloodstream infection event (central line-associated bloodstream infection and non-central line-associated bloodstream infection). Atlanta: Centres for Disease Control; 2017.
Larsen EN, Ray-Barruel G, Takashima M, Marsh N, Friese CR, Chopra V, et al. Peripheral intravenous catheters in the care of oncology and haematology patients. Aust J Cancer Nurs. 2022;23(1):16–22.
Chopra V, Ratz D, Kuhn L, Lopus T, Lee A, Krein S. Peripherally inserted central catheter-related deep vein thrombosis: contemporary patterns and predictors. J Thromb Haemost. 2014;12(6):847–54.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–81.
Schults JA, Calleja P, Slaughter E, Paterson R, Rickard CM, Booker C, et al. Peripheral intravenous catheter insertion and use of ultrasound in patients with difficult intravenous access: Australian patient and practitioner perspectives to inform future implementation strategies. PLoS ONE. 2022;17(6): e0269788.
Paterson RS, Schults JA, Slaughter E, Cooke M, Ullman A, Kleidon TM, et al. Review article: Peripheral intravenous catheter insertion in adult patients with difficult intravenous access: a systematic review of assessment instruments, clinical practice guidelines and escalation pathways. Emerg Med Australas. 2022. https://doi.org/10.1111/1742-6723.14069.
Wang A, Hendin A, Millington SJ, Koenig S, Eisen LA, Shiloh AL. Better with ultrasound: arterial line placement. Chest. 2020;157(3):574–9.
Zochios VA, Wilkinson J, Dasgupta K. The role of ultrasound as an adjunct to arterial catheterization in critically ill surgical and intensive care unit patients. J Vasc Access. 2014;15(1):1–4.
Shiver S, Blaivas M, Lyon M. A prospective comparison of ultrasound-guided and blindly placed radial arterial catheters. Acad Emerg Med. 2006;13(12):1275–9.
Wilson C, Rose D, Kelen GD, Billioux V, Bright L. Comparison of ultrasound-guided Vs traditional arterial cannulation by emergency medicine residents. West J Emerg Med. 2020;21(2):353–8.
O’Grady NP, Alexander M, Dellinger EP, Gerberding JL, Heard SO, Maki DG, et al. Guidelines for the prevention of intravascular catheter-related infections. Centers for disease control and prevention. MMWR Recomm Rep. 2002;51(10):1–29.
Infusion Nurses Society. Infusion therapy standards of practice. Norwood: Infusion Nurses Society Wolters Kluwer; 2016. p. 2016.
Schults JA, Woods C, Cooke M, Kleidon T, Marsh N, Ray-Barruel G, et al. Healthcare practitioner perspectives and experiences regarding vascular access device data: an exploratory study. Int J Healthc Manag. 2021;14(4):948–55.
Zhang W, Li K, Xu H, Luo D, Ji C, Yang K, et al. Efficacy of ultrasound-guided technique for radial artery catheterization in pediatric populations: a systematic review and meta-analysis of randomized controlled trials. Crit Care. 2020;24(1):197.
Pearse I, Corley A, Rickard CM, Marsh N. Unnecessary removal of vascular access devices due to suspected infection in Australian intensive care units. Aust Crit Care. 2022;35(6):644–50.
Mermel LA, Allon M, Bouza E, Craven DE, Flynn P, O’Grady NP, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;49(1):1–45.
Kashef MT, Helmy OM. Development of a multiplex polymerase chain reaction-based DNA lateral flow assay as a point-of-care diagnostic for fast and simultaneous detection of MRSA and vancomycin resistance in bacteremia. Diagnostics (Basel). 2022;12(11):2691.
Afshari A, Schrenzel J, Ieven M, Harbarth S. Bench-to-bedside review: rapid molecular diagnostics for bloodstream infection—a new frontier? Crit Care. 2012;16(3):222.
Vaidya AR, Wolska N, Vara D, Mailer RK, Schröder K, Pula G. Diabetes and thrombosis: a central role for vascular oxidative stress. Antioxidants (Basel). 2021;10(5):706.
Thiruvoipati T, Kielhorn CE, Armstrong EJ. Peripheral artery disease in patients with diabetes: epidemiology, mechanisms, and outcomes. World J Diabetes. 2015;6(7):961–9.
Liu LJ, Zhou HM, Tang HL, Zhou QH. Evaluation of radial and ulnar artery blood flow after radial artery decannulation using colour Doppler ultrasound. BMC Anesthesiol. 2021;21(1):312.
Wallis MC, McGrail M, Webster J, Marsh N, Gowardman J, Geoffrey Playford E, et al. Risk factors for peripheral intravenous catheter failure: a multivariate analysis of data from a randomized controlled trial. Infect Control Hosp Epidemiol. 2014;35(1):63–8.
Wang J, Lim HY, Nandurkar H, Ho P. Age, sex and racial differences in fibrin formation and fibrinolysis within the healthy population. Blood Coagul Fibrinolysis. 2022;33(2):141–4.
Coderech Carretero J, Corella Montoya F, Grande Barez M, Corella Montoya MÁ, Ocampos Hernández M, Larrainzar-Garijo R. Description and analysis of the dynamic and morphological flow pattern of the main arteries of the wrist and hand in a healthy Spanish population. Rev Esp Cir Ortop Traumatol. 2020;64(3):167–76.
Pancholy SB, Heck LA, Patel T. Forearm arterial anatomy and flow characteristics: a prospective observational study. J Invasive Cardiol. 2015;27(4):218–21.
Ranucci M, Laddomada T, Ranucci M, Baryshnikova E. Blood viscosity during coagulation at different shear rates. Physiol Rep. 2014;2(7): e12065.
Sakariassen KS, Orning L, Turitto VT. The impact of blood shear rate on arterial thrombus formation. Future Sci OA. 2015;1(4):Fso30.
Ní Chróinín D, Ray-Barruel G, Carr PJ, Frost SA, Rickard CM, Mifflin N, et al. The burden of peripheral intravenous catheters in older hospital inpatients: a national cross-sectional study part of the one million global peripheral intravenous catheters collaboration. Australas J Ageing. 2023;42(1):98–107.
Xu X, Wang B, Ren C, Hu J, Greenberg DA, Chen T, et al. Age-related impairment of vascular structure and functions. Aging Dis. 2017;8(5):590–610.
Tamura T, Kobayashi E, Kawaguchi M, Matsuoka Y, Fujii A, Ando M, et al. Comparison between the effects of normal saline with and without heparin for the prevention and management of arterial catheter occlusion: a triple-blinded randomized trial. J Anesth. 2021;35(4):536–42.
Acknowledgements
We would like to acknowledge the assistance of Ms Daner Ball and Ms Rita Nemeth for their assistance with manuscript submission.
Funding
This study was not funded.
Author information
Authors and Affiliations
Consortia
Contributions
All authors contributed to the conception and design of the study. EY and RW analysed the data. JS, CR, EY and RW interpreted the results. JS drafted the manuscript with EY and RW major contributors. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from Griffith University (Ref No: 2021/834). Written informed consent was obtained for each participant in the parent RCT.
Consent for publication
Not applicable.
Competing interests
JAS, ERY, RSW, MM, MM, JG, KRC, AR, HY have no conflicts to disclose. NM: Griffith University and The University of Queensland have received on her behalf investigator-initiated grants from 3 M, Cardinal Health and Eloquest, and consultancy payments from 3 M and Becton Dickinson for expert advice/ educational sessions. EL: EL’s affiliate (University of Queensland) has received, on her behalf: an investigator-initiated research grant from Eloquest Healthcare, unrelated to this work; EL was also awarded scholarship for conference attendance, by Angiodynamics, unrelated to this work. AC: ACs employer, on my behalf, has received investigator-initiated grants from 3 M, Cardinal Health and Eloquest Healthcare. These grants are unrelated to this work. EA: EA’s employer (Southwestern Sydney Local Health District) has received investigator-initiated research grants from Becton Dickinson-Bard and Eloquest Healthcare. EA has also received consultancy payments for educational lectures/expert advice from 3 M and ITL medical. CMR: CMR’s employer’s (Griffith University or The University of Queensland) received on her behalf unrestricted research or education grants from 3 M, BD-Bard, Cardinal Health, Eloquest and consultancy payments from 3 M, BD-Bard and ITL Healthcare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Risk factors for catheter failure and complications (univariate analyses).
Additional file 2.
Bayesian information criterion values by failure type.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Schults, J.A., Young, E.R., Marsh, N. et al. Risk factors for arterial catheter failure and complications during critical care hospitalisation: a secondary analysis of a multisite, randomised trial. j intensive care 12, 12 (2024). https://doi.org/10.1186/s40560-024-00719-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40560-024-00719-1