
Abstract
Background
Childhood trauma exposures (CTEs) are frequent, well-established risk factor for the development of psychopathology. However, knowledge of the effects of CTEs in healthy individuals in a real life context, which is crucial for early detection and prevention of mental disorders, is incomplete. Here, we use ecological momentary assessment (EMA) to investigate CTE load-dependent changes in daily-life affective well-being and psychosocial risk profile in n = 351 healthy, clinically asymptomatic, adults from the community with mild to moderate CTE.
Findings
EMA revealed significant CTE dose-dependent decreases in real-life affective valence (p = 0.007), energetic arousal (p = 0.032) and calmness (p = 0.044). Psychosocial questionnaires revealed a broad CTE-related psychosocial risk profile with dose-dependent increases in mental health risk-associated features (e.g., trait anxiety, maladaptive coping, loneliness, daily hassles; p values < 0.003) and a corresponding decrease in factors protective for mental health (e.g., life satisfaction, adaptive coping, optimism, social support; p values < 0.021). These results were not influenced by age, sex, socioeconomic status or education.
Conclusions
Healthy community-based adults with mild to moderate CTE exhibit dose-dependent changes in well-being manifesting in decreases in affective valence, calmness and energy in real life settings, as well as a range of established psychosocial risk features associated with mental health risk. This indicates an approach to early detection, early intervention, and prevention of CTE-associated psychiatric disorders in this at-risk population, using ecological momentary interventions (EMI) in real life, which enhance established protective factors for mental health, such as green space exposure, or social support.
Similar content being viewed by others


Introduction
Childhood trauma exposures (CTEs) such as physical, sexual, and emotional abuse and physical and emotional neglect are recognized environmental risk factors for the development of a wide range of adverse health outcomes across the lifespan [1,2,3]. For example, physical abuse, emotional abuse and neglect in childhood roughly double the likelihood of psychiatric disorders such as depression, anxiety disorders and substance abuse in adulthood [4], with a dose-dependent relationship between cumulative CTE exposure and severity of psychopathology [3, 5]. CTEs are further associated with a range of somatic conditions, including altered neuroendocrinological stress response, cardiovascular, inflammatory, and metabolic diseases and premature death [6]. Given that up to 30% of the adult population have experienced some form of CTEs [7], this represents a massive public health burden.
Research have linked CTEs with maladaptive personality traits, such as higher trait anxiety, neuroticism and lower optimism, self-efficacy and life satisfaction, suggesting a dispositional vulnerability [8,9,10]. This idea is further supported by ambulatory assessment studies reporting a CTE-related increase in daily negative affect [11], and stress experience [12]. At the same time, our knowledge of the effects of CTEs on mental health is still incomplete. First, our understanding of possible CTE-related affective changes in the general population is limited, especially when it comes to milder forms of adverse exposures and related subclinical changes in everyday life. Here, community-based studies and the availability of smartphone-based Ecological Momentary Assessment (EMA) in real life provide an opportunity for new insights [13, 14]. Second, most studies on CTEs have focused on patient populations [15]. These results need to be complemented by information about the nature and extent of subclinical changes in healthy individuals with CTE to define their risk for and resilience against developing a psychiatric disorder.
To fill this gap in knowledge, this study combined methods from psychology, epidemiology and EMA to investigate the psychosocial risk profile along with changes in daily-life affective well-being in healthy individuals with CTE from the general population. Based on our previous work with at-risk populations [13, 14, 16], we hypothesized that CTE, even in a clinically healthy group, would predict reduced momentary affective well-being in daily life and increased psychosocial risk for mental illness.
Methods
Study participants
We recruited in total 351 healthy young adults (mean age: 24.80 ± 6.54 years, 162 males) from local communities in the Rhine-Neckar metropolitan area in Germany for this study, thereby over-sampling for CTE to ensure an enrichment of CTE in the total sample. We provide further demographic details in Table 1 and sTable1. General exclusion criteria included the presence of a significant general medical disorder, neurological disorder, or a current or lifetime psychiatric disorder as determined by clinical interviews [17, 18]. None of the recruited subjects reported clinical psychiatric symptoms at the time of the study entry. Study participants gave written informed consent for a study protocol approved by the Medical Ethics Committee II of Heidelberg University.
Questionnaire data acquisition and analysis
CTE
For retrospective assessment of CTEs we used the Childhood Trauma Screener (CTS), a validated instrument covering sexual, emotional and physical abuse and emotional and physical neglect [19]. Here, according to published cut-offs [19], and severity classifications [20] mild and moderate CTE can be defined as fulfilling one or two trauma subtypes respectively (see sMethods for details).
Sociodemographic and Psychosocial risk measures
Participants also completed a battery of sociodemographic and psychosocial assessments aiming at quantifying established psychosocial risk factors for mental health. This included trait anxiety, loneliness, self-efficacy, sense of coherence, optimism, mental well-being, life satisfaction, daily hassles, coping strategies and social support. We provide a full overview of the measures in sTable2. Because of the skewed distribution of CTS scores, we examined dose-dependent (linear) associations between cumulative CTE (CTS sum score) and questionnaire scores in SPSS (IBM, SPSS, version 25) using nonparametric Spearman rank correlation analyses corrected for age, sex, education, and SES (see sFigure1 and Table 1 for details).
EMA and analysis
We assessed e-diary-ratings of the momentary social affective experience with study smartphones (Motorola Moto G, Motorola Mobility). EMA ratings were collected on 7 consecutive days in daily life with a flexible time- and location-dependent sampling schedule with an average of 12.51 ± 1.79 prompts per day, as previously described [14, 16, 21]. We assessed momentary well-being using a validated EMA short scale with good reliability and sensitivity [22]. The scale captures real-life affective valence, calmness and energetic arousal with two bipolar scales for each measure, presented as computerized visual analog scales with sliding locators (score range: 0 − 100). At an exploratory level, we also evaluated e-diary scales quantifying momentary social contact, social anhedonia, the appraisal of negative and positive events, and computed an established EMA measure of affective instability in daily life (mean square of successive differences, MSSD) from momentary affective valence scores [13, 14]. We nested within-subject e-diary assessments (level 1) within participants (level 2) and used multilevel models in SAS (version 9.4., SAS Institute Inc., Cary, NC, USA) to test for associations between cumulative CTE (CTS sum score) and EMA outcome measures. Since the distribution of the CTS sum variable was skewed (see sFigure 1) we log-transformed the variable using the natural logarithm. In addition, we added the level-1 predictors time of the day and time of the day squared, and age, sex, SES and years of education as level-2 covariates. Furthermore, we examined the distribution of the residuals of the models to rule out any bias due to the structure of the data (sFigure 2). We provide further methods details in the sMethods.
Results
Questionnaire data
Higher severity of CTE was significantly associated with older age, lower SES, and fewer years of education (p values < 0.026). After adjustment for age, sex, SES, and education, higher CTE load was significantly associated with higher scores for trait anxiety, loneliness, perceived daily hassles, and use of maladaptive coping strategies, as well as significantly lower scores for psychological well-being, life satisfaction, optimism, sense of coherence, self-efficacy, and perceived social support (p values < 0.021). We provide further details of the results in Table 1; Fig. 1. Details of the statistical relationships of the five CTS subdomains to the psychosocial measures are presented in sTable3 for exploratory purposes.

Relationship between CTE load and psychosocial risk and protective factors for mental health. Significant CTE dose-dependent increases in questionnaire measures capturing (upper row, from left to right) trait anxiety loneliness, daily hassles, and maladaptive coping (all p values < 0.003) and significant decrease in (bottom row, from left to right) life satisfaction, optimism, social support and adaptive coping (all p values < 0.021). X-axis: Childhood trauma screener (CTS) sum score; Y-axis: mean/sum values of questionnaire measures
Ecological momentary assessments
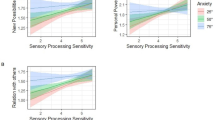
As hypothesized, higher trauma exposure during childhood was significantly associated with lower momentary affective valence in daily life in adulthood (p = 0.007). In addition, higher CTE related to lower momentary calmness and energetic arousal (p values < 0.044; see also Table 1; Fig. 2, and sTable4). Additional covariation for age, sex, SES, education and reported daily hassles did not change these results. In contrast, our exploratory analysis of EMA measures of affective instability, frequency and evaluation of momentary social contacts, and appraisal of positive and negative events in daily life revealed no significant associations with CTE burden. We provide further details of the EMA results in Table 1; Fig. 2, and sTable4.

Relationship between CTE load and real-life affective well-being. Significant CTE dose-dependent decreases (upper row, from left to right) in real-life affective valence (p = 0.007), energetic arousal (p = 0.032,) and calmness (p = 0.044) in healthy community-based individuals with mild to moderate CTE. Absence of such associations in social-affective EMA measures reflecting evaluation of (bottom row, from left to right) social anhedonia (p > 0.23), appraisal of negative events (p > 0.98) and affective (in)stability (valence MSSD, p > 0.50). X-axis: Childhood trauma screener (CTS) sum score; Y-axis: mean values of EMA indices across 7 days of measurement
Discussion
In this study, we aimed to answer the question of whether there are dose-dependent changes in real-life affective well-being and psychosocial risk profile even in healthy asymptomatic individuals from the community with self-reported mild to moderate CTE. Consistent with our hypothesis, we observed a significant CTE dose-dependent decrease in affective valence in everyday life. In addition, we found a significant negative association between CTE load and momentary energy and calmness. Notably, we have previously observed a similar sensitivity of these measures in relation to other established psychiatric risk and resilience factors, including in individuals with subclinical symptoms [13] and healthy persons who benefited in well-being from social contact [14], physical activity [21] and exposure to urban green space [16]. Our study extends these data by showing that even clinically healthy, asymptomatic individuals from the community with milder forms of CTEs exhibit dose-dependent changes in real-life affective well-being as adults, and that these EMA scales are well suited to capture such risk-associated changes in naturalistic settings. Further longitudinal studies in healthy exposed individuals are needed to investigate the value of these risk markers of the development of CTE-related mental disorders in adulthood.
Based on the collected questionnaire measures, we further identified a psychosocial risk profile in our individuals with CTE consistent with our hypothesis. The profile consisted of a dose-dependent increase in several known psychosocial risk factors for mental health (e.g., trait anxiety, maladaptive coping, daily stress) and a corresponding decrease in factors known to reduce the odds of developing a psychiatric disorder (e.g., social support, adaptive coping, life satisfaction, optimism). Here, our data confirm and extend the existing knowledge by showing that, in addition to clinical populations with more pronounced CTEs [8, 23] similar dose-dependent psychosocial associations can be found in healthy community-based individuals with milder forms of CTEs. Furthermore, they indicate potential psychological mechanisms through which CTEs reduce well-being in this population.
These results should be evaluated in light of several study limitations. First, although our study includes a comparatively large sample, we cannot draw any causal conclusions because of the cross-sectional design used. Second, as in many other studies, our measure of CTE burden is based on a retrospective self-report instrument. Although such surveys may be biased, previous data suggest that CTEs are underreported rather than overreported on such measures and that they are not crucially influenced by current emotional states [24]. Third, the distribution of CTE load was skewed in our population-based healthy sample, which was to be expected. Thus, we took special precautions to obtain robust results by using nonparametric methods, log-transforming predictors, and examining the distribution of model residuals.
Conclusion
In conclusion, we found that healthy, clinically asymptomatic individuals from the community with mild to moderate CTEs exhibit dose-dependent changes in well-being as adults. These changes manifest in a decrease in affective valence, calmness and energy in real life settings. We further identified a broad psychosocial risk profile, in which features detrimental to mental health accumulate. We hope that these data will contribute to a precision approach to early detection, early intervention, and prevention of CTE-associated psychiatric disorders in the general population. The risk-associated features established in this work (i.e., affective valence) could be targeted, for example, by EMI in real life, which enhance established protective factors for mental health, such as green space exposure, or social support [14, 16].
Data availability
The data supporting the findings of this study are available upon request from the corresponding author HT. The data are not publicly available due to sensitive information that could compromise research participant privacy/consent.
Abbreviations
- ABF:
-
Alltagsbelastungsfragebogen
- CTE:
-
Childhood Trauma Exposure
- BSSS:
-
Berlin Social Support Scale
- CSSS:
-
Chronic Stress Screening Scale
- CTS:
-
Childhood Trauma Screener
- CTQ:
-
Childhood Trauma Questionnaire
- EMA:
-
Ecological Momentary Assessment
- EA:
-
emotional abuse
- EMI:
-
ecological momentary intervention
- EN:
-
emotional neglect
- GSES:
-
General Self-Efficacy Scale
- LOT-R:
-
Revised Life Orientation Test
- M:
-
mean
- MLA:
-
multilevel analysis
- MSSD:
-
mean square of successive differences
- n:
-
number of participants with available data
- PA:
-
physical abuse
- PN:
-
physical neglect
- SD:
-
standard deviation
- SES:
-
socioeconomic status
- SA:
-
sexual abuse
- STAI-T:
-
State-Trait Anxiety Inventory
- SOC:
-
Sense of Coherence Scale
- UCLA:
-
UCLA Loneliness Scale
- WHO:
-
World health organization
- SWLS:
-
Satisfaction with Life Scale
References
McGrath JJ, McLaughlin KA, Saha S, Aguilar-Gaxiola S, Al-Hamzawi A, Alonso J, et al. The association between childhood adversities and subsequent first onset of psychotic experiences: a cross-national analysis of 23 998 respondents from 17 countries. Psychol Med. 2017;47(7):1230–45.
Heim C, Nemeroff CB. The role of childhood trauma in the neurobiology of mood and anxiety disorders: preclinical and clinical studies. Biol Psychiatry. 2001;49(12):1023–39.
McKay MT, Cannon M, Chambers D, Conroy RM, Coughlan H, Dodd P, et al. Childhood trauma and adult mental disorder: a systematic review and meta-analysis of longitudinal cohort studies. Acta Psychiatr Scand. 2021;143(3):189–205.
Norman RE, Byambaa M, De R, Butchart A, Scott J, Vos T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Med. 2012;9(11):e1001349.
Pietrek C, Elbert T, Weierstall R, Muller O, Rockstroh B. Childhood adversities in relation to psychiatric disorders. Psychiatry Res. 2013;206(1):103–10.
Brindle RC, Pearson A, Ginty AT. Adverse childhood experiences (ACEs) relate to blunted cardiovascular and cortisol reactivity to acute laboratory stress: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2022;134:104530.
Sethi D, Bellis M, Hughes K, Gilbert R, Mitis F, Gauden G, editors. European report on preventing child maltreatment: World Health Organization. Regional Office for Europe; 2013.
Mc Elroy S, Hevey D. Relationship between adverse early experiences, stressors, psychosocial resources and wellbeing. Child Abuse Negl. 2014;38(1):65–75.
Gorka AX, Hanson JL, Radtke SRH. Reduced hippocampal and medial prefrontal gray matter mediate the association between reported childhood maltreatment and trait anxiety in adulthood and predict sensitivity to future life stress. Biol Mood Anxiety Disord. 2014;4(1):1–10.
Broekhof R, Rius-Ottenheim N, Spinhoven P, van der Mast RC, Penninx BW, Zitman FG, et al. Long-lasting effects of affective disorders and childhood trauma on dispositional optimism. J Affect Disord. 2015;175:351–8.
Pries LK, Klingenberg B, Menne-Lothmann C, Decoster J, van Winkel R, Collip D, et al. Polygenic liability for schizophrenia and childhood adversity influences daily-life emotion dysregulation and psychosis proneness. Acta Psychiatr Scand. 2020;141(5):465–75.
van Nierop M, Lecei A, Myin-Germeys I, Collip D, Viechtbauer W, Jacobs N, et al. Stress reactivity links childhood trauma exposure to an admixture of depressive, anxiety, and psychosis symptoms. Psychiatry Res. 2018;260:451–7.
Berhe O, Höflich A, Mößnang C, Reichert M, Kremer T, Gana G, et al. Reduced real-life affective well-being and amygdala habituation in unmedicated community individuals at risk for depression and anxiety. Biol Psychiatry Cogn Neurosci Neuroimaging. 2022;in press.
Gan G, Ma R, Reichert M, Giurgiu M, Ebner-Priemer UW, Meyer-Lindenberg A, et al. Neural Correlates of Affective Benefit from Real-life Social Contact and Implications for Psychiatric Resilience. JAMA Psychiatry. 2021;78(7):790–2.
Fritz J, de Graaff AM, Caisley H, van Harmelen AL, Wilkinson PO. A systematic review of amenable resilience factors that moderate and/or mediate the relationship between Childhood Adversity and Mental Health in Young People. Front Psychiatry. 2018;9:230.
Tost H, Reichert M, Braun U, Reinhard I, Peters R, Lautenbach S, et al. Neural correlates of individual differences in affective benefit of real-life urban green space exposure. Nat Neurosci. 2019;22(9):1389–93.
Margraf J. Diagnostisches Kurz-Interview bei psychischen Störungen (Mini-DIPS). Berlin, Heidelberg, New York: Springer; 1994.
First M, Spitzer R, Gibbon M, Williams J. Structured clinical interview for DSM-IV-TR Axis I Disorders, Research Version, Patient Edition with psychotic screen (SCID-I/P W/ PSY SCREEN). New York: New York Psychiatric Institute; 2001.
Glaesmer H, Schulz A, Häuser W, Freyberger HJ, Brähler E, Grabe HJ. [The childhood trauma screener (CTS) - development and validation of cut-off-scores for classificatory diagnostics]. Psychiatr Prax. 2013;40(4):220–6.
Agorastos A, Pittman JO, Angkaw AC, Nievergelt CM, Hansen CJ, Aversa LH, et al. The cumulative effect of different childhood trauma types on self-reported symptoms of adult male depression and PTSD, substance abuse and health-related quality of life in a large active-duty military cohort. J Psychiatr Res. 2014;58:46–54.
Reichert M, Braun U, Gan G, Reinhard I, Giurgiu M, Ma R, et al. A neural mechanism for affective well-being: Subgenual cingulate cortex mediates real-life effects of nonexercise activity on energy.Sci Adv. 2020;6(45).
Wilhelm P, Schoebi D. Assessing mood in daily life: structural validity, sensitivity to change, and reliability of a short-scale to measure three basic dimensions of mood. Eur J Psychol Assess. 2007;23:258–67.
Kuzminskaite E, Penninx B, van Harmelen AL, Elzinga BM, Hovens J, Vinkers CH. Childhood trauma in adult depressive and anxiety Disorders: an Integrated Review on Psychological and Biological Mechanisms in the NESDA Cohort. J Affect Disord. 2021;283:179–91.
Spinhoven P, Penninx BW, Hickendorff M, van Hemert AM, Bernstein DP, Elzinga BM. Childhood Trauma Questionnaire: factor structure, measurement invariance, and validity across emotional disorders. Psychol Assess. 2014;26(3):717–29.
Acknowledgements
We thank Gabriela Gan, PhD, Beate Höchemer, MA, Janina I. Schweiger, MD, Carina Sebald, MSc, Alexander Moldavski, MD, Mirjam Melzer, MSc, and our research assistants for valuable support.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
HT, AML and UEP designed the study. OB, RM, MR recruited the participants and collected the data. OB, MR, CM, AH performed the data analysis. OB, MR, CM, RM, AH, JT, CH, UEP, AML, HT interpreted the data. OB, AML, HT drafted the first version of the manuscript. All authors revised the manuscript critically for important intellectual content and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study approved by the Medical Ethics Committee II of the Medical Faculty Mannheim at the Ruprecht-Karls-University in Heidelberg, Germany. All participants provided written informed consent for the participation in the study.
Consent for publication
Not applicable.
Competing interests
Dr Meyer-Lindenberg has received lecture fees from the Lundbeck International Foundation, Paul-Martini-Stiftung, Lilly Deutschland, Atheneum, Fama Public Relations, IDIBAPS, Janssen-Cilag, Hertie-Stiftung, Bodelschwingh-Klinik, Pfizer, Universität Freiburg, Schizophrenia Academy, Hong Kong Society of Biological Psychiatry, Spanish Society of Psychiatry, Italian Society of Biological Psychiatry, Reunions I Ciencia S.L. Brain Center Rudolf Magnus UMC Utrecht, Friedrich-Merz-Stiftung, and consultant fees from Boehringer Ingelheim, Elsevier, Brainsway, Lundbeck Int. Neuroscience Foundation, Lundbeck A/S, Sumitomo Dainippon Pharma Co., Academic Medical Center of the University of Amsterdam, Synapsis Foundation-Alzheimer Research Switzerland, IBS Center for Synaptic Brain Dysfunction, Blueprint Partnership, University of Cambridge, Dt. Zentrum für Neurodegenerative Erkrankungen, Zürich University, Brain Mind Institute, L.E.K. Consulting, ICARE Schizophrenia, Science Advances, Fondation FondaMental, von Behring Röntgen Stiftung, The Wolfson Foundation, Sage Therapeutics. Dr. Ebner-Priemer reports consultancy for Boehringer-Ingelheim. The other authors report no biomedical financial interests or potential conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Berhe, O., Moessnang, C., Reichert, M. et al. Dose-dependent changes in real-life affective well-being in healthy community-based individuals with mild to moderate childhood trauma exposure. bord personal disord emot dysregul 10, 14 (2023). https://doi.org/10.1186/s40479-023-00220-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40479-023-00220-5