
Abstract
Diffusely infiltrating gliomas are among the most common central nervous system tumors in adults. Over the past decade, the subcategorization of these tumors has changed to include both traditional histologic features and more recently identified molecular factors. However, one molecular feature that has yet to be integrated is the presence/absence of chromosomal instability (CIN). Herein, we use global methylation profiling to evaluate a reference cohort of IDH-mutant astrocytomas with and without prior evidence of CIN (n = 42), and apply the resulting methylation-based characteristics to a larger test cohort of publicly-available IDH-mutant astrocytomas (n = 245). We demonstrate that IDH-mutant astrocytomas with evidence of CIN cluster separately from their chromosomally-stable counterparts. CIN cases were associated with higher initial histologic grade, altered expression patterns of genes related to CIN in other cancers, elevated initial total copy number burden, and significantly worse progression-free and overall survival. In addition, in a grade-for-grade analysis, patients with CIN-positive WHO grade 2 and 3 tumors had significantly worse survival. These results suggest that global methylation profiling can be used to discriminate between chromosomally stable and unstable IDH-mutant astrocytomas, and may therefore provide a reliable and cost-effective method for identifying gliomas with chromosomal instability and resultant poor clinical outcome.
Similar content being viewed by others

Introduction
With the recent introduction of the 2021 5th Edition of the WHO Classification of Tumours of the Central Nervous System, diffuse gliomas in adults are now defined by both histologic and molecular features, and in many cases molecular features outrank traditional histologic classification in both diagnosis and grade [18]. Oligodendrogliomas (WHO grades 2–3) are now defined by the presence of simultaneous deletion of chromosomal arms 1p and 19q, as well as mutation in either IDH1 or IDH2. Moreover, what was previously classified by histology as “astrocytoma” and “glioblastoma” has now been divided into IDH-mutant astrocytoma (WHO grades 2–4) and IDH-wildtype glioblastoma (WHO grade 4). Notably, IDH-mutant astrocytomas with homozygous CDKN2A deletion are now considered WHO grade 4 regardless of histologic features [2, 18], although numerous other mutations, specific copy number variants, and other molecular features have been suggested as relevant to prognosis and potentially tumor grade [21].
One potentially useful molecular feature that may help explain the underlying heterogeneity in clinical outcome between IDH-mutant astrocytomas of the same WHO grade is chromosomal instability (CIN). Previously, we have demonstrated that overall copy number variation (CNV), distributed across the entire genome, tends to increase with histologic grade in IDH-mutant astrocytomas [28], and IDH-mutant grade 2–3 astrocytomas with poor clinical outcomes have incongruously elevated overall CNV at the time of initial diagnosis [27, 29]. This high CNV occurs frequently in cases with other aggressive molecular features including CDK4 amplification and homozygous CDKN2A deletion, although in many cases elevated CNV is the only molecular factor present to suggest poor prognosis [22, 27, 29]. These IDH-mutant astrocytomas can be stratified solely by CNV level with thresholds of approximately 310–465 megabase pairs (Mbp) (~ 10–15% of the total genome) separating patient outcomes [23, 28, 32]. Additionally, CNS and other solid tumors with previously identified CIN [35] can reliably be identified based on mRNA profiles of specific gene sets (CIN25, CIN70) in cases with available whole exome sequencing [6, 28], although this method can add significant processing time and costs. There is a wealth of evidence suggesting that CIN is a contributing factor to the aggressiveness of a subset of otherwise lower-grade IDH-mutant astrocytomas, however because CIN is a dynamic and ongoing process and a single biopsy or resection specimen represents only a snapshot of the temporal and spatial molecular evolution of the neoplasm, detection may be difficult and impractical in many clinical settings [35, 36].
Global DNA methylation profiling is a technique that has become relatively common in the past 5 years to diagnose and categorize CNS neoplasms (as well as identify new entities) based on epigenetic features [5, 24]. In this report, we leverage global methylation profiling to distinguish CIN and chromosomal stable (CS) phenotypes in IDH-mutant astrocytomas. We utilized a small cohort of IDH-mutant astrocytomas (n = 42) with known CIN or CS status to identify epigenetic differences between the two groups, and then applied this method using an unbiased approach to a larger cohort of publicly-available IDH-mutant astrocytomas (n = 245) to verify these epigenetic signatures and investigate the clinical and molecular differences between cases clustering as CIN or CS by methylation profiling.
Methods
Case selection
Reference cohort: We analyzed 42 IDH-mutant astrocytomas (2021 WHO grades 2–4) from previous studies with multiple previously established lines of evidence suggesting either chromosomal instability (CIN) or chromosomal stability (CS) status, including mRNA profiling of gene panels linked to CIN (CIN70) [6, 28], evidence of cell-to-cell chromosomal heterogeneity [29], mutations in genes with known roles in the maintenance of chromosomal stability [22, 27, 28], copy number profile evidence of significant spatial chromosomal heterogeneity [19], and significantly elevated CNV with multiple biopsies/resections reflective of rapid chromosomal alteration (Additional File 1: Fig. 1 ). All cases represent the first resection specimen, before treatment was initiated, and were classified according to WHO 2021 integrated histologic/molecular criteria [18].
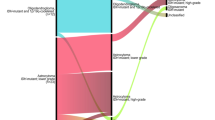
Test cohort: Using the cBioPortal interface [8, 14], we performed a search of IDH-mutant astrocytoma (WHO grade 2–4) from publicly-available datasets [1, 3, 4, 7]. The original histologic diagnoses reported included astrocytoma, anaplastic astrocytoma, oligodendroglioma, anaplastic oligodendroglioma, oligoastrocytoma, anaplastic oligoastrocytoma, and glioblastoma. All cases were reclassified according to WHO 2021 integrated histologic/molecular criteria using IDH1/2, 1p/19q, TP53, and ATRX status [18]. All cases included in this study represented the first resection specimen. From these large datasets, a total of 245 cases meeting the criteria for IDH-mutant astrocytoma (WHO grade 2–4) with available global methylation profiling, whole exome sequencing, mRNA expression levels, and copy number variation (CNV) were selected for further analysis.
Genetic and epigenetic analysis
As previously detailed [13, 22, 27, 28], DNA methylation data (Illumina Human Methylation 450) and gene expression data (Illumina HiSeq, RNASeq) were downloaded and analyzed with R 3.4.1 (http://www.R-project.org/), TCGAbiolinks (https://bioconductor.org/packages/release/bioc/html/TCGAbiolinks.html), and Qiagen’s IPA tool (www.qiagen.com/ingenuity) (Qiagen, Hilden, Germany) [10, 33]. The Affymetrix SNP 6.0 microarray data normalized to germline for copy number analysis for the same publicly-available cases was downloaded from Broad GDAC Firehose (http://gdac.broadinstitute.org/runs/stddata__2016_01_28/).
Molecular subtype classification was performed utilizing the cloud-based DNA methylation classifier (www.molecularneuropathology.org) [5]. Unsupervised hierarchical clustering of the most differently expressed DNA methylation regions was performed on each reference cohort case using Euclidian distance measures, Pearson correlation coefficient and average linkage, and then repeated in the larger test cohort [19, 34]. Heatmaps were generated using ComplexHeatmap (https://bioconductor.org/packages/release/bioc/html/ComplexHeatmap.html). Uniform Manifold Approximation and Projection (UMAP) [20] and t-Distributed Stochastic Neighbor Embedding (t-SNE) [5] plotting were performed with R umap and tsne packages, using the same distance metrics and default parameters. MGMT promoter methylation was reported in the majority of cases in cBioPortal and confirmed with methylation array data. For CIN70 RNAseq data, normalized gene expression level ranking was performed as previously described [28].
The fraction of CNV was calculated from data in cBioPortal as the fraction of the genome (expressed as percent of nucleotide base pairs) with log2 of copy number > 0.3 (gain or loss) following the procedure described by Gao et al. and visualized with the cBioPortal interface [14]. CNV was quantified by percentage of the total genome, as previously described [13, 22, 27]. Mutation analysis was performed on whole exome sequencing and included all recurrent mutations as well as genes with previously identified roles in cell proliferation, cancer and malignant progression in CNS neoplasms and other cancers, and maintenance of chromosomal stability [22, 27]. Gene variant annotation was performed using The 1000 Genomes Project, COSMIC, dbSNP, ClinVar, CanProVar 2.0, and FATHMM-MKL [12, 15, 16, 30, 31, 37].
Statistical analysis
Differences in patient age at diagnosis and CNV were evaluated using student’s t-test. The significance of Kaplan–Meier survival curves was calculated using the Mantel-Cox test (Log-rank test). Proportion of cases with mutations specifically associated with genome instability, as well as gender, CIN70, MGMT promoter methylation, and 2016/2021 WHO grade were calculated using Fisher’s Exact test. All statistical calculations were performed with GraphPad Prism version 9 (GraphPad, La Jolla, CA).
Results
Methylation profile, molecular features, and clinical characteristics of reference cohort
Methylation profiling was performed on 14 IDH-mutant astrocytomas with previously established evidence of chromosomal instability (CIN) [19, 22, 28, 29] and 28 “chromosomally stable” (CS) cases (Fig. 1), demonstrating two distinct methylation clusters with UMAP analysis: cluster 1, comprising 11 of the previously established CIN cases, and cluster 2, comprising all 28 CS cases and 3 CIN cases (78.6% sensitivity, 100% specificity, 100% positive predictive value (PPV), 90.3% negative predictive value (NPV)), suggesting that there may be epigenetic differences which can be determined by analysis of methylation sites. UMAP and t-SNE analysis demonstrated statistically equivalent results.

a Uniform manifold approximation and projection (UMAP) plotting demonstrating separate clustering between reference cohort WHO grade 2–4 IDH-mutant astrocytomas with chromosomal instability (CIN) and those with chromosomal stability (CS), and b cluster analysis heatmap summarizing DNA methylation profiles of the reference cohort (n = 42)
Compared to cluster 2, cluster 1 had significantly worse progression-free survival (PFS; 31.1 vs 95.1 months; p = 0.0077) and overall survival (OS; 36.8 vs 122.4 months; p < 0.0001) (Table 1). In addition, cluster 1 cases also had significantly higher overall copy number variation (CNV) compared to cluster 2 (20.2 ± 5.8% vs 7.0 ± 1.0%; p = 0.0018), significantly more frequent cases with high CIN70 mRNA expression levels (p < 0.0001), a set of 70 genes with tight correlation between high expression and the presence of CIN [6, 28], higher 2016 WHO grade (p = 0.0037), and higher 2021 WHO grade (p = 0.0224). No significant differences were identified in terms of patient gender, age at diagnosis, MGMT promoter methylation status, or other mutations or copy number changes.
Of particular interest are the three cases with known CIN that clustered with CS cases (Fig. 1a). All three cases demonstrated MGMT promoter methylation, and were 2021 WHO grade 2, 3, and 4. No difference in age was identified between these three cases and cluster 1 or the other cluster 2 cases. These cases have significantly higher overall CNV (15.3% ± 8.1%) compared to the other cluster 2 cases (p = 0.0285), but statistically equivalent CNV to cluster 1 (p = 0.6845). No significant differences were noted in PFS or OS between these three cases and cluster 1 or cluster 2, although there was a non-significant trend toward shorter PFS and OS in these cases compared to cluster 2 and longer PFS and OS compared to cluster 1.
Methylation profile, molecular features, and clinical characteristics of test cohort
Methylation profiling was performed with UMAP analysis on 245 IDH-mutant astrocytomas, and identified 57 cases (23.3%) with a similar pattern of methylation probe levels to cluster 1 of the reference cohort (CIN) and 188 cases with similar methylome characteristics to cluster 2 of the reference cohort (CS) (Fig. 2a–c). UMAP plotting demonstrated that all reference cohort cases aligned with their respective test cohort clusters. UMAP and t-SNE plotting methods demonstrated statistically equivalent results.

a–b Uniform manifold approximation and projection (UMAP) plotting demonstrating separate clustering between the test cohort WHO grade 2–4 IDH-mutant astrocytomas with chromosomal instability (CIN) and those with chromosomal stability (CS). c Cluster analysis heatmap summarizing DNA methylation profiles of the test cohort (n = 245). d Cases in cluster 1 (CIN) demonstrated significantly higher overall copy number variation on initial resection compared to cases in cluster 2 (CS)
Cluster 1 cases had an elevated level of CNV at initial biopsy (21.2 ± 1.9% vs 7.4 ± 0.5%; p < 0.0001) (Fig. 2d & Table 1), distributed across the entire genome [22, 27], as well as a higher percentage of cases with “high” CIN70 expression levels (75.5% vs 8.7%; p < 0.0001), compared to their cluster 2 counterparts (Table 1). Cases in cluster 1 also had significantly more frequent mutations in genes with known functions associated with maintaining overall genome stability [22, 27, 28] compared to cluster 2 cases (17.5% vs 7.9%; p = 0.0426). Overall, 81.4% of cases in cluster 1 were positive for CIN by at least one additional method compared to 12.7% of cases in cluster 2 (p = 0.0001; 65.7% sensitivity, 94.7% specificity, 83.0% PPV, 87.6% NPV) (Fig. 2b). Of note, definitive CIN/CS status could not be determined in 7 cases (4 cluster 1 and 3 cluster 2 cases). Cluster 1 cases also tended to initially present at higher 2021 WHO grades (p = 0.0007) with no significant difference in any other molecular alteration, including MGMT promoter methylation status (Table 1).
Methylation profiling of CIN as a prognostic factor
In the test cohort, cluster 1 had significantly worse PFS (38.0 vs 62.0 months; p = 0.0034) (Fig. 3a) and OS (50.5 months vs 98.2 months; p = 0.0002) (Fig. 3b), compared to cluster 2. Stratifying cases by these methylation profiles yielded results comparable to stratifying by current 2021 WHO grade (Additional File 2: Fig. 2), overall CNV threshold of 10% or 15% [23, 28], and CIN70 mRNA expression levels [28].

Combined 2021 WHO grade 2–4 cases from the test cohort demonstrating worse progression-free survival (PFS) a and overall survival (OS) b in cluster 1 compared to cluster 2. 2021 WHO grade 2–3 combined cases (“lower-grade astrocytoma”) from cluster 1 had worse PFS c and OS d compared to grade 2–3 cases from cluster 2
“Lower-grade astrocytomas” (WHO grade 2–3) demonstrated a significant difference in overall CNV (22.0 ± 2.4% vs 7.8 ± 1.8; p = 0.0003), patient age at diagnosis (43.3 ± 2.1 vs 36.9 ± 1.3 years; p = 0.0245), PFS (38.0 vs 68.9 months; p = 0.0021) and OS (50.8 vs 114; p < 0.0001) in the cluster 1 cases (n = 41) compared to the cluster 2 cases (n = 167) (Fig. 3c, d and Table 2). In a grade-for-grade analysis (Fig. 4), WHO grade 2 cluster 1 cases had significantly worse PFS (29.1 vs 87.1 months; p = 0.0006) and OS (62.9 vs 122.4 months; p = 0.0093), compared to WHO grade 2 cluster 2 cases. WHO grade 3 cluster 1 cases had significantly worse OS (47.9 vs 93.1 months; p = 0.0243) compared to WHO grade 3 cluster 2 cases, however no significant difference was identified between the two WHO grade 3 clusters in terms of PFS (p = 0.1132), and no significant difference was identified in terms of PFS (p = 0.4384) or OS (p = 0.8505) in the WHO grade 4 tumors. Additionally, WHO grade 2, 3, and 4 IDH-mutant astrocytomas in cluster 1 had significantly higher CIN compared to their grade-matched cluster 2 counterparts, but no other significant clinical or molecular differences (Table 2).

2021 WHO grade 2 cases from cluster 1 had worse progression-free survival (PFS) a and overall survival (OS) b compared to grade 2 cases from cluster 2. No significant difference was found between 2021 WHO grade 3 cases from cluster 1 and 2 in terms of PFS c, however grade 3 cases from cluster 1 had significantly worse OS compared to grade 3 cases from cluster 2 d. No significant difference was found between 2021 WHO grade 4 cases from cluster 1 and 2 in terms of PFS e or OS f
Discussion
Diffuse gliomas in adults remain a largely incurable disease [21, 25]. However, more recently identified molecular features and epigenetic classification systems have helped to refine the diagnostic criteria beyond traditionally used histologic features, as well as identify novel, potentially targetable genetic alterations, some of which have now been codified into official diagnostic algorithms as the new standard of care [18, 26]. Still, there is significant variation in terms of individual patient morbidity and mortality that is partially unaccounted for by recent changes to the WHO diagnostic and grading system.
Chromosomal instability (CIN) is a known mechanism for malignant progression in many systemic cancers. This process results in large scale and rapid alterations to whole chromosomes or chromosomal regions that may affect numerous genes and cell processes and may cause significant intratumoral and cell-to-cell molecular heterogeneity, producing clones that may vary in malignancy, tendency to invade surrounding tissue, ability to evade immune regulation, and/or resistance to traditional therapies [36]. While this process is relatively well known and the mechanisms underlying it have long been studied, detecting the presence of CIN from a single biopsy or resection specimen may be challenging and impractical to perform from a technical standpoint, and a number of direct and indirect methods for CIN detection have been proposed [35]. Additionally, while CIN frequently results in more aggressive behavior in cancer, the process itself may be targeted by a number of therapeutic agents that are currently FDA-approved or in clinical trials for other cancer types [35], raising the possibility that these drugs may be useful as adjuvant therapies in diffuse gliomas with CIN. While there are few studies that investigate the effect of CIN and overall CNV in diffuse gliomas, we and others have used large publicly-available and institutional cohorts of IDH-mutant astrocytoma and IDH-wildtype glioblastoma to demonstrate that CIN can be readily identified through whole genome copy number profiling and whole exome sequencing in certain subsets. Importantly, stratification of cases using these methods has as good or better predictive power as previously codified histologic or molecular features [22, 23, 27,28,29, 32].
In this report, we analyzed a small cohort of IDH-mutant astrocytomas with known CIN or CS status, determined by multiple distinct methods, to determine if this one characteristic would yield separate methylation profile clusters (Fig. 1). We then analyzed a larger cohort to verify that the identified methylome characteristics and resulting clustering pattern would be corroborated in a blindly evaluated cohort (Fig. 2). Our findings demonstrate that methylation profiling can distinguish IDH-mutant astrocytomas with and without CIN: cluster 1 had a distinct methylation profile, significantly greater proportion of cases with at least one measure of CIN, significantly higher CNV levels at the time of initial surgery, and significantly worse PFS and OS compared to cluster 2 (Table 1). It is worth noting that cluster 1 cases tended to be higher grade at first diagnosis, which perhaps is to be expected since higher grades tended to be associated with more genomic instability [9, 28]. On the other hand, cases with CIN may present at higher histologic grades simply because they progress more rapidly and so on average may be identified later in their evolution [29]. However, methylation profiling identified 15 grade 2 cases and 26 grade 3 cases in the CIN cluster, suggesting that methylation profiling is a potentially viable method for identifying cases with CIN and resulting poor prognosis even in these lower-grade astrocytomas (Table 2).
This report helps to further solidify the concept that CIN and CNV are features that can be measured and used as prognostic factors in subsets of IDH-mutant astrocytomas in certain situations. The fact that the CIN cluster cuts across 2021 WHO grades and the fact that the CIN cluster has significantly elevated overall CNV, even in grade 2 tumors, supports the idea that CIN is present in a subset of these tumors and may be detected before histologic indicators of tumor progression or aggressive behavior are present, and suggests that CIN is present early in tumor development, representing a fundamentally altered biology compared to IDH-mutant astrocytomas without this feature. Incongruously elevated CNV identified in newly diagnosed lower-grade IDH-mutant astrocytomas likely results from underlying CIN and may be a driver of poor clinical behavior and outcome, rather than simply being a reflection of other molecular processes.
These data represent only a small sample of IDH-mutant astrocytomas with methylation profiling paired with other molecular and clinical data and as such does not necessarily define the full molecular parameters of these tumors. Nonetheless, our findings do serve as a proof-of-concept that methylation profiling, an already widely accepted modality for diagnosing CNS neoplasms, may be employed to identify this underlying characteristic and separate out cases with CIN which may have more aggressive clinical courses. Given the role that global methylation profiling is beginning to play in clinical practice, this may be an ideal way to routinely screen for characteristics such as CIN, rather than relying on more intensive and less practical methods, such as single cell sequencing to identify the minority of cases in which CIN may be present [35]. Still, more work is needed to further define the epigenetic signature associated with CIN in much larger and more diverse cohorts of IDH-mutant astrocytoma, as well as to place these CIN-positive diffuse gliomas in the greater context of all CNS neoplasms by methylome profiling [24]. It is important to rapidly identify genetic and epigenetic characteristics that affect diagnosis and prognosis to ensure appropriate treatment, and multiple studies have recently shown that this type of in-depth molecular data can be available in time to guide neurooncological treatment [11, 17, 26].
In conclusion, these data further support the idea that the presence of CIN and elevated CNV levels are crucial data points in predicting clinical outcome, and may one day be useful targets for personalized therapies. Methylation profiling has proven to be a powerful tool for CNS neoplasm diagnosis and may potentially identify IDH-mutant astrocytomas with underlying CIN, even if histologically consistent with 2021 WHO grade 2 or 3, to help further refine prognosis and improve therapeutic design in the future.
Availability of data and materials
Data used in this study is available at www.cbioportal.org, https://portal.gdc.cancer.gov/, and https://www.cancer.gov/about-nci/organization/ccg/research/structural-genomics/tcga. The cases used in this study are included as Additional File 3: Table 1.
References
Barthel FP, Johnson KC, Varn FS, Moskalik AD, Tanner G, Kocakacuk E, Anderson KJ, Abiola O, Aldape K, Alfaro KD et al (2019) Longitudinal molecular trajectories of diffuse glioma in adults. Nature 576:112–120. https://doi.org/10.1038/s41586-019-1775-1
Brat DJ, Aldape K, Colman H, Figrarella-Branger D, Fuller GN, Giannini C, Holland EC, Jenkins RB, Kleinschmidt-DeMasters B, Komori T et al (2020) cIMPACT-NOW update 5: recommended grading criteria and terminologies for IDH-mutant astrocytomas. Acta Neuropathol 139:603–608. https://doi.org/10.1007/s00401-020-02127-9
Cancer Genome Atlas Research N (2008) Comprehensive genomic characterization defines human glioblastoma genes and core pathways. Nature 455:1061–1068. https://doi.org/10.1038/nature07385
Cancer Genome Atlas Research N, Brat DJ, Verhaak RG, Aldape KD, Yung WK, Salama SR, Cooper LA, Rheinbay E, Miller CR, Vitucci M et al (2015) Comprehensive, integrative genomic analysis of diffuse lower-grade gliomas. N Engl J Med 372:2481–2498. https://doi.org/10.1056/NEJMoa1402121
Capper D, Jones DTW, Sill M, Hovestadt V, Schrimpf D, Sturm D, Koelsche C, Sahm F, Chavez L, Reuss DE et al (2018) DNA methylation-based classification of central nervous system tumours. Nature 555:469–474. https://doi.org/10.1038/nature26000
Carter SL, Eklund AC, Kohane IS, Harris LN, Szallasi Z (2006) A signature of chromosomal instability inferred from gene expression profiles predicts clinical outcome in multiple human cancers. Nat Genet 38:1043–1048. https://doi.org/10.1038/ng1861
Ceccarelli M, Barthel FP, Malta TM, Sabedot TS, Salama SR, Murray BA, Morozova O, Newton Y, Radenbaugh A, Pagnotta SM et al (2016) Molecular profiling reveals biologically discrete subsets and pathways of progression in diffuse glioma. Cell 164:550–563. https://doi.org/10.1016/j.cell.2015.12.028
Cerami E, Gao J, Dogrusoz U, Gross BE, Sumer SO, Aksoy BA, Jacobsen A, Byrne CJ, Heuer ML, Larsson E et al (2012) The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov 2:401–404. https://doi.org/10.1158/2159-8290.CD-12-0095
Cohen A, Sato M, Aldape K, Mason CC, Alfaro-Munoz K, Heathcock L, South ST, Abegglen LM, Schiffman JD, Colman H (2015) DNA copy number analysis of Grade II-III and Grade IV gliomas reveals differences in molecular ontogeny including chromothripsis associated with IDH mutation status. Acta Neuropathol Commun 3:34. https://doi.org/10.1186/s40478-015-0213-3
Colaprico A, Silva TC, Olsen C, Garofano L, Cava C, Garolini D, Sabedot TS, Malta TM, Pagnotta SM, Castiglioni I et al (2016) TCGAbiolinks: an R/Bioconductor package for integrative analysis of TCGA data. Nucleic Acids Res 44:e71. https://doi.org/10.1093/nar/gkv1507
Euskirchen P, Bielle F, Labreche K, Kloosterman WP, Rosenberg S, Daniau M, Schmitt C, Masliah-Planchon J, Bourdeaut F, Dehais C et al (2017) Same-day genomic and epigenomic diagnosis of brain tumors using real-time nanopore sequencing. Acta Neuropathol 134:691–703. https://doi.org/10.1007/s00401-017-1743-5
Forbes SA, Bindal N, Bamford S, Cole C, Kok CY, Beare D, Jia M, Shepherd R, Leung K, Menzies A et al (2011) COSMIC: mining complete cancer genomes in the catalogue of somatic mutations in cancer. Nucleic Acids Res 39:D945-950. https://doi.org/10.1093/nar/gkq929
Galbraith K, Kumar A, Abdullah KG, Walker JM, Adams SH, Prior T, Dimentberg R, Henderson FC, Mirchia K, Sathe AA et al (2020) Molecular correlates of long survival in IDH-wildtype glioblastoma cohorts. J Neuropathol Exp Neurol 79:843–854. https://doi.org/10.1093/jnen/nlaa059
Gao J, Aksoy BA, Dogrusoz U, Dresdner G, Gross B, Sumer SO, Sun Y, Jacobsen A, Sinha R, Larsson Eet al (2013) Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci Signal 6: pl1. https://doi.org/10.1126/scisignal.2004088
Genomes Project C, Abecasis GR, Auton A, Brooks LD, DePristo MA, Durbin RM, Handsaker RE, Kang HM, Marth GT, McVean GA (2012) An integrated map of genetic variation from 1,092 human genomes. Nature 491:56–65. https://doi.org/10.1038/nature11632
Harrison SM, Riggs ER, Maglott DR, Lee JM, Azzariti DR, Niehaus A, Ramos EM, Martin CL, Landrum MJ, Rehm HL (2016) Using ClinVar as a Resource to Support Variant Interpretation. Curr Protoc Hum Genet 89: 8 16 11–18 16 23. https://doi.org/10.1002/0471142905.hg0816s89
Hench J, Bihl M, Bratic Hench I, Hoffmann P, Tolnay M, Bosch Al Jadooa N, Mariani L, Capper D, Frank S (2018) Satisfying your neuro-oncologist: a fast approach to routine molecular glioma diagnostics. Neuro Oncol 20:1682–1683. https://doi.org/10.1093/neuonc/noy128
Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, Hawkins C, Ng HK, Pfister SM, Reifenberger G et al (2021) The 2021 WHO classification of tumors of teh central nervous system: a summary. Neuro Oncol 23:1231–1251. https://doi.org/10.1093/neuonc/noab106
Lyon JF, Vasudevaraja V, Mirchia K, Walker JM, Corona RJ, Chin LS, Tran I, Snuderl M, Richardson TE, Viapiano MS (2021) Spatial progression and molecular heterogeneity of IDH-mutant glioblastoma determined by DNA methylation-based mapping. Acta Neuropathol Commun 9:120. https://doi.org/10.1186/s40478-021-01221-7
McInnes L, Healy J, Saul N, Großberger L (2018) UMAP: uniform manifold approximation and projection. J Open Source Softw 3:861. https://doi.org/10.21105/joss.00861
Mirchia K, Richardson TE (2020) Beyond IDH-mutation: emerging molecular diagnostic and prognostic features in adult diffuse gliomas. Cancers (Basel) 12: 1817 https://doi.org/10.3390/cancers12071817
Mirchia K, Sathe AA, Walker JM, Fudym Y, Galbraith K, Viapiano MS, Corona RJ, Snuderl M, Xing C, Hatanpaa KJ et al (2019) Total copy number variation as a prognostic factor in adult astrocytoma subtypes. Acta Neuropathol Commun 7:92. https://doi.org/10.1186/s40478-019-0746-y
Mirchia K, Snuderl M, Galbraith K, Hatanpaa KJ, Walker JM, Richardson TE (2019) Establishing a prognostic threshold for total copy number variation within adult IDH-mutant grade II/III astrocytomas. Acta Neuropathol Commun 7:121. https://doi.org/10.1186/s40478-019-0778-3
Papanicolau-Sengos A, Aldape K (2022) DNA methylation profiling: an emerging paradigm for cancer diagnosis. Annu Rev Pathol 17:295–321. https://doi.org/10.1146/annurev-pathol-042220-022304
Perry A (2003) Pathology of low-grade gliomas: an update of emerging concepts. Neuro Oncol 5:168–178. https://doi.org/10.1215/S1152851702000443
Pratt D, Sahm F, Aldape K (2021) DNA methylation profiling as a model for discovery and precision diagnostics in neuro-oncology. Neuro Oncol 23:S16–S29. https://doi.org/10.1093/neuonc/noab143
Richardson TE, Sathe AA, Kanchwala M, Jia G, Habib AA, Xiao G, Snuderl M, Xing C, Hatanpaa KJ (2018) Genetic and epigenetic features of Rapidly progressing IDH-mutant astrocytomas. J Neuropathol Exp Neurol 77:542–548. https://doi.org/10.1093/jnen/nly026
Richardson TE, Sathe AA, Xing C, Mirchia K, Viapiano MS, Snuderl M, Abdullah KG, Hatanpaa KJ, Walker JM (2021) Molecular signatures of chromosomal instability correlate with copy number variation patterns and patient outcome in IDH-mutant and IDH-wildtype astrocytomas. J Neuropathol Exp Neurol 80:354–365. https://doi.org/10.1093/jnen/nlab008
Richardson TE, Snuderl M, Serrano J, Karajannis MA, Heguy A, Oliver D, Raisanen JM, Maher EA, Pan E, Barnett S et al (2017) Rapid progression to glioblastoma in a subset of IDH-mutated astrocytomas: a genome-wide analysis. J Neurooncol 133:183–192. https://doi.org/10.1007/s11060-017-2431-y
Sherry ST, Ward MH, Kholodov M, Baker J, Phan L, Smigielski EM, Sirotkin K (2001) dbSNP: the NCBI database of genetic variation. Nucleic Acids Res 29:308–311. https://doi.org/10.1093/nar/29.1.308
Shihab HA, Rogers MF, Gough J, Mort M, Cooper DN, Day IN, Gaunt TR, Campbell C (2015) An integrative approach to predicting the functional effects of non-coding and coding sequence variation. Bioinformatics 31:1536–1543. https://doi.org/10.1093/bioinformatics/btv009
Shirahata M, Ono T, Stichel D, Schrimpf D, Reuss DE, Sahm F, Koelsche C, Wefers A, Reinhardt A, Huang K et al (2018) Novel, improved grading system(s) for IDH-mutant astrocytic gliomas. Acta Neuropathol 136:153–166. https://doi.org/10.1007/s00401-018-1849-4
Silva TC, Colaprico A, Olsen C, D'Angelo F, Bontempi G, Ceccarelli M, Noushmehr H (2016) TCGA Workflow: Analyze cancer genomics and epigenomics data using Bioconductor packages. F1000Res 5: 1542. https://doi.org/10.12688/f1000research.8923.2
Tang K, Kurland D, Vasudevaraja V, Serrano J, DeLorenzo M, Radmanesh A, Thomas C, Spino M, Gardner S, Allen JC et al (2020) Exploring DNA methylation for prognosis and analyzing the tumor microenvironment in pleomorphic xanthoastrocytoma. J Neuropathol Exp Neurol 79:880–890. https://doi.org/10.1093/jnen/nlaa051
Thompson LL, Jeusset LM, Lepage CC, McManus KJ (2017) Evolving therapeutic strategies to exploit chromosome instability in cancer. Cancers (Basel). https://doi.org/10.3390/cancers9110151
Vishwakarma R, McManus KJ (2020) Chromosome instability; implications in cancer development, progression, and clinical outcomes. Cancers (Basel). https://doi.org/10.3390/cancers12040824
Zhang M, Wang B, Xu J, Wang X, Xie L, Zhang B, Li Y, Li J (2017) CanProVar 2.0: an updated database of human cancer proteome variation. J Proteome Res 16:421–432. https://doi.org/10.1021/acs.jproteome.6b00505
Acknowledgements
Not applicable
Funding
J.M.W. and T.E.R. are supported in part by National Institute on Aging (NIA) P30AG066546.
Author information
Authors and Affiliations
Contributions
Conception of the work: TER.; Design of the work: YL, KJH, JMW, TER; Acquisition/analysis/interpretation of the data: YL, AAS, SHA, CX, TER; Creation of new software used in the work: not applicable; Drafted the work or substantially revised it: YL, KGA, SKM, AJB., MSV, JMW, TER; all authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The results presented in this paper have not been published previously in whole or part. The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Fig. 1
Copy number variation differences between initial biopsies and tumor recurrences in IDH-mutant and IDH-wildtype astrocytomas (A) and IDH-mutant astrocytomas with known CIN and CS status (B)
Additional file 2. Fig. 2
Kaplan-Meier analysis of the full test cohort demonstrating significant differences in progression-free (A) and overall survival (B) between cases stratified by 2021 WHO grade
Additional file 3. Table 1
List of IDH-mutant astrocytoma cases
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, Y., Sathe, A.A., Abdullah, K.G. et al. Global DNA methylation profiling reveals chromosomal instability in IDH-mutant astrocytomas. acta neuropathol commun 10, 32 (2022). https://doi.org/10.1186/s40478-022-01339-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40478-022-01339-2