
Abstract
Purpose
Patient-reported experiences are a key source of information on quality in mental health care. Most patient experience surveys are limited to assessments from adults, including those conducted by parents or proxies on behalf of others. The aim of this study was to produce findings to inform development of modules on patient and parent experiences with medication in outpatient CAMHS in Norway, for use in previously validated instruments applied in national surveys.
Patients and methods
We developed survey questions based on a systematic literature review, expert-group consultations, interviews with adolescents and parents, and pretesting of the modules in a pilot study. This study included adolescents aged 12–17 years and parents with experiences from outpatient CAMHS and we present findings from semi-structured interviews.
Results
Adolescents with ADHD emphasized the following aspects as important concerning medication use in CAMHS: positive effects of medication like better function and concentration in school and change of behaviour. They also stressed the importance of side effects such as eating problems, nausea, loss of appetite, insomnia, and changes in thoughts and feelings. In addition, adolescents highlighted the significance of aspects as support in daily routines for taking medications, while parents highlighted needs for a professional follow-up care. Parents emphasized aspects regarding their children’s medication included both positive effects and change in behaviour, as well as their identification of negative side effects.
Conclusion
Our findings from semi-structured interviews identified important aspects reported by both patients and parents on functions, side effects and follow-up care related to medication. The results indicated that both groups emphasized corresponding aspects of what was important regarding medication. However, when it came to follow-up care, the two groups highlighted distinct aspects, indicating differing priorities or concerns in this area.
Similar content being viewed by others

Introduction
Patient-reported experiences are a core part of quality in healthcare. In Norway, patient-reported experiences are included in the national quality indicator system. The Norwegian Institute of Public Health (NIPH) along with its predecessors, has developed patient experience surveys and instruments for measuring experiences of various patient groups using standardized methods. These methods include literature reviews, expert group discussions, qualitative and cognitive interviews with patients, and pilot testing of questionnaires [1,2,3,4].
In the Child and Adolescents Mental Health Services (CAMHS) patients receive specialist consultations for the assessment and treatment of emotional, behavioural, or mental health difficulties. This includes initiation and adjustment of medication. NIPH has previously developed questionnaires to assess the experiences of both parents and patients with CAMHS. Recently, the Norwegian Directorate of Health commissioned that the CAMHS surveys should also include questions about experiences with the use of medication. These modules are planned to be integrated into previously validated questionnaires for use in national surveys in Norway [5,6,7].
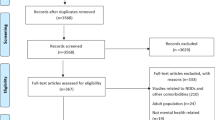
To our knowledge, there are few national surveys on the experiences of adolescents and parents with medications in CAMHS. We conducted a systematic literature search to identify studies related to experiences with the use of medications in the mental health care services. We found a substantial body of research on adult’s experiences on medications, surveys, and instrument validations [8,9,10,11,12]. However, validated instruments were assessed, but not included in our survey questions [13,14,15,16,17,18,19,20,21,22,23].
Research have shown that the medical treatment of mental health problems among young people is a subject of controversy, involving concerns about increased use, side effects, long-term treatment and the off-label use of medications primarily tested on adults [24]. Additionally, we found little published evidence regarding which aspects are important to adolescents. Therefore, there is a need to fill this knowledge gap. Research indicates a complex experience that encompassed both benefits and side effects reported by the participants [24,25,26,27,28]. Barriers to medication use included lack of information and autonomy for adolescents, while support from family and friends were facilitators for helping find the right medication and with least possible side effects [29,30,31].
Young people who were committed to taking medications had experiences that included perceiving medications as a desirable choice for treatment, finding medications helpful, and having no concern about side effects [32]. In addition, young people with less commitment to medication had experience that included feelings of being coerced into taking medications and concerns about side effects, perceived stigma associated with it, and worries about short and long-terms side effects [32].
Studies have identified important aspects of experiences with medications from the perspective of patients related to psychological reactions, adverse outcomes, adherence, and follow-up care, and how these aspects may interact. Researchers explored changes in mood, after experiencing adverse outcomes with medication [17, 28]. In a study of prescription stimulant medication, which tracked experience from childhood to adolescents: participants reported a history of taking medication, adherence to medications. In other studies researchers have explored aspects of recovery, adherence, and acceptance to transition to follow-up care [14, 33,34,35]. This involved a trade-off that encompassed perceived effects, side effects and benefits of the prescribed medications [26]. This multidimensional experience of medications profoundly shapes patients’ lives.
Researchers have examined how adolescents experience the effects of psychotropic drugs and how access to professional support and follow-up care impact their social lives [24, 30]. These studies have identified facilitators for accessibility and acceptability, such as psychiatric openness to client’s perspective, availability of services outside office hours, and support from mental health care providers [29, 36].
We found a limited number of studies that examine which aspects of the experience are important from both perspective of patients and parents on medications [37,38,39]. Patient perspectives offers qualitative insights into which aspects are perceived as significant and can provide valuable insights into how they perceive medication use. The aim of this study was to generate and validate findings to inform the development of survey questions modules focusing on the experiences of patients aged 12–15 years and parent regarding medication use in outpatient CAMHS.
Methods
NIPH launched the development of two modules of survey questions related to experiences with medication in CAMHS. We drafted these modules after reviewing free-text comments from a national survey among parents in CAMHS 2018 [40], a literature review, and meetings with a reference group. Separate drafts were created for adolescents’ and their parents. The semi-structured interviews, conducted with both patients and parents, were divided into two parts. The first part involved a pre-determined set of open questions, allowing the interviewer to follow-up on themes or responses. The second part, a cognitive interview, enabled informants to vocalize their thoughts regarding survey questions and response categories (see Tables 1 and 2). We used ChatGPT 3.0 for feedback on style, spelling and grammar.
Participants
The participants included adolescents with Attention-deficit/hyperactivity disorder (ADHD) and parents with experiences from different outpatient clinics in CAMHS. We opted to include approximately 12 to 15 participants in each group for the interviews, following the recommendations of previous studies. The inclusion criteria for adolescents were prior experiences with medication as part of their treatment in CAMHS and sampling of age, gender, and duration of treatment. By including participants with diverse backgrounds, we aimed to better represent the broader population and ensure that our findings are more valid. All participants received written and verbal information about voluntarily participation. Parent`s provided consent for their children participation in the interviews.
Data collection
Data were collected through semi-structured interviews conducted between June and August 2021. The interview-guides (see Additional file 1 and 2) were pre-tested, and these interviews are not included in our analysis of data. We pilot-tested the procedure for conducting digital interviews [41].
Due to the constraints posed by Covid-19, along with limited time and resources, conducting physical interviews at outpatient clinics was not feasible. We recruited participants from voluntarily organizations, specifically ADHD Norway and Mental Health Carers Norway (LPP). Our sample consisted therefore of adolescent with ADHD, which reflect the specific focus of our study. Our digital interviewing approach was restricted to no recording possibilities. Consequently, our data primarily relied on the researchers’ field notes rather than full-transcribed interviews. Field notes were made during the interviews, as small, keyword-based notes. More comprehensive notes were written immediately after interviews [42, 43].
Two researchers conducted the interviews, with open-ended questions to explore participants experiences regarding the use of medications: “Can you tell us about what it is like for you to take medications?” We wanted to identify what informants immediately emphasized, as important aspects and if these correspond with our survey questions. We explored both positive and negative experiences with taking medications. We asked how participants had experienced consultations from the CAMHS regarding medications. The cognitive interviews aimed to explore the informants’ assessments of the survey questions. During the cognitive interviews, we presented the draft questionnaire and solicited feedback regarding their perceptions of survey questions and response categories (results not presented here).
Data analysis
We conducted data analysis using a qualitative content analysis approach [44,45,46]. Our data coding process followed several stages: (1) Decontextualization (2) Recontextualization, (3) Categorization and (4) Compilation [45]. Two researchers independently coded the data in NVivo. The content analysis involved developing a coding system with main categories and subcategories. We used Graneheim and Lundman`s method, focusing on the main stages of their approach to guide our analysis. However, we did not implement every stage in our study. Our intention was to use their framework as a general guide rather than strictly following the method in its entirety [46]. Initially, interviews were thoroughly examined for condensed themes, important aspects, and manifest and latent content. This process helped us to summarize the critical aspects that were most relevant for our informants. Codes were compared and similarities and differences were identified and analysed. Preliminary codes were discussed by the two researchers conducting the interviews until consensus was reached.
Our analysis followed these steps: (1) Descriptions of adolescents’ and parents’ experiences (2) Identifying main categories and subcategories (3) Exploring similarities and differences between the two groups. (4) Developing new concepts that emerged from our analysis of the datasets. We will now describe the results from the interviews.
Results
We conducted interviews with 13 patients who had experiences with the CAMHS. Most of the patients were between 12 and 16 years. Among the participants, there were six girls and seven boys. Their duration of medication use varied: eight had been treated for 1–2 years, four for 3–5 years, and one for more than 6 years. Most of our participants were adolescents with ADHD. They reported a range of medications use as stimulants, anxiolytics, hypnotics, antidepressants, mood stabilisers, antipsychotics and alimemazine (for sleep disturbance).
Additionally, we conducted interviews with ten mothers and only two fathers.
Adolescents experience
Adolescents with ADHD experienced positive effects of medication, such as improved function, behaviour changes, and better concentration in school. However, they also experienced side effects such as eating problems, nausea, insomnia, and changes in thoughts and feelings. Many adolescents with ADHD reported difficulties in maintaining their medication routines and expressed a need for assistance in remembering to take medications. The main themes emerging from our data analysis were aspects related to medication impacts on functions and behaviour, perceived side effects, and adolescents’ challenges with the follow-up of their daily medication routine (see Table 3). We will now describe these themes in more detail.
Most of the adolescents with ADHD reported significant change and improvement in functions. They reported better coping with everyday life, enhanced concentration in school and improved self-control. Some of the effects of the medication were described as feeling more relaxed, less stressed, and less irritable, aggressive, or restless. A few even reported receiving more attention from friends due to these changes. Some adolescents used words like “feeling more normal”, but a few reported a sense of losing their personality, stating: “I am more myself without medication”.
Some patients reported positive experience such as improved concentration, presence, self-control, a sense of calmness, and perceived effectiveness on educational achievement. They felt more engaged in school and when spending time with friends. However, some individuals mentioned changes in their thoughts and feeling, such as feeling “flat”, or “numb”, being slower to respond to others, and this reduced motivation to continue taking medications. Many of the adolescents had mixed experiences when it came to finding the right medications, including type of medication and appropriate dosage. Other had to make medication changes due to lack of effect, side-effects, and no improvement in symptoms.
Some of the patients expressed a desire for better information about how medications work and their potential side-effects. Adolescents expressed significant concerns about the adverse side effects of medical treatment. The most mentioned side effects included loss of appetite, nausea, insomnia, and a notable flattening of mood. Additionally, participants reported side effects such as stomach pain, feelings of feverishness, fatigue, tics, breathing problems, depression, and even hallucinations. Adolescents with ADHD experienced a range of symptoms, including stress, changes in energy levels, tics, breathing problems, restlessness, diffuse pain, and alterations in their mood (feelings and thoughts). Furthermore, participants discussed the consequences stemming from these side effects. For instance, the loss of appetite raises concerns about weight loss or an inability to gain weight. Some individuals described the balance they had to maintain between the treatment’s benefits and its substantial side effects.
While most of adolescents were generally satisfied with the counselling and information, they received from the CAMHS, there was a recognized need for ongoing care and support from mental health services during the transition from CAMHs to general practitioners (GPs). Some adolescents highlighted the challenges they faced in adhering to prescribed medications and follow-up care; their practical needs for help emphasized the importance of reminders. Others reported the need for follow-up care by GPs, and guidance on dosage and time-schedules as important aspects.
Some stated that their need for counselling and help decreased after receiving a diagnosis and being prescribed medications from CAMHS. Additionally, a few adolescents explained why they refused to take medications, citing reasons such as dislike for the medications, feeling better without them, psychological reactions (adverse events), changes in their personality, difficulties in stabilizing their disorders, sleep restrictions, fears of relapse, and self-harm concerns.
Parents experience
Parents had both positive and negative experience with their children’s medication use. The main theme that emerged included behaviour and functioning changes, and experiences with side effects. Parents also shared their views on the professional support and follow-up care provided by CAMHS, especially the transition from CAMHs to the GPs. We will now describe these themes in more detail (see Table 4).
The parents reported both positive and negative experiences regarding the effects of medications on their children’s functioning in school, as well as within the family and with friends. They also discussed their child’s ability to cope with the medication’s effects during the day, which could be disrupted with other medications given for sleep disturbance.
Furthermore, parents described their adolescent`s experiences with the CAMHS in general terms, and especially consultations which included clinical interviews, investigations, mapping, assessment, and diagnosis of mental health conditions. They also discussed experiences with challenges their child faced in managing both getting diagnosis and trying out medications. Additionally, they expressed their experiences with finding the right medication, the prescriptions of medications following diagnostics, the trial-and-error method with various types of medications, and how adolescents responded to medication in the short- and long-term.
Parents reported side effects experienced by their children, including decreased appetite, as well as perceived psychological reactions and changes in mood, thoughts and emotions attributed to specific medication. They expressed a need for more information from CAMHS about the possibility of side effects of medications. Experiences varied, ranging from heavy side effects to medications not working at all.
Parents suggested a yearly follow-up by a child psychiatrist, including updated assessment of medications (medical check-ups) and specialist consultations regarding prescribed medications. Others expressed a desire for more extended follow-up care within CAMHS, while some appreciated CAMHS’ transparency in acknowledging the trial-and-error method of finding the right medication. Additionally, some parents felt it was necessary to get a new psychiatric assessment and diagnosis of mental health conditions, especially due to changes in mood or psychological development during adolescence. Furthermore, parents also highlighted the need for a seamless transition from CAMHS to GPs and clarified the responsibility of follow-up of prescribed medications. One important aspect was clarifying responsibilities for medication follow-up and access to other health services.
One significant area of divergence pertained to parents’ apprehension regarding the long-term implications of medication and the necessity for ongoing care. They expressed concerns about the lasting effects on their adolescents and advocated for improved access to professional follow-up care. Conversely, adolescents were more concerned about the practical aspects of medication management. They were interested in strategies for adhering to medication routines, establishing proper time schedules, and receiving reminders. For them, long-term follow-up care was less of an important aspect of medication use.
Discussion
The aim of this study was to explore which aspects of experiences are important from the perspective of patient’s and parents related to medication use in CAMHS. We identified important aspects reported by both groups related to functions, side effects and follow-up care, and we will now discuss our findings, and how these aspects are important in survey questions and could be applied in national surveys.
The trade-off are comparable with findings from other studies that have found patients weighting positive effects, such as better functions, symptoms management and health improvement, against negative side effects, lack of perceived effects, and personal aspects related to medications [26, 38]. As a result, some of them refused to take the prescribed medications, viewing the side effects as a too high a price to pay. “Is it worth it?” reflects the process of trading off the benefits of the prescribed medications against the heavy burden of side effects.
In McMillan’s (2020) narrative review of young people’s experiences with mental health medications, a wide range of both negative and positive encounters were reported, which had the potential to influence medication acceptance. Challenges included a lack of autonomy, and the influence of family members, alongside considerations of medication benefit and side effects. Additionally, factors such as routines, medication adherence [47,48,49], perceived burden and responsibility, as well as the use of non-medication therapies, played significant roles. Our study has found similar findings.
Why adolescents refuse to take their medications may be related to a complex interplay of different social factors, including family dynamics [50], peer influences, and perspectives on health care policies. Our current research has emphasized patients views of significant impact of social life family, parents, and friends on how adolescents perceive changes in mood and behaviour, as well as how medications impact daily mood fluctuations, symptoms, mental health conditions and well-being.
The utilization of a triangulation in qualitative methods with data from two groups, offered a more comprehensive understanding [25, 51]. Parents played a crucial role in validating their adolescents’ experiences, shedding light on aspects including functionality, benefits, and potential side effects, which were confirmed by them.
Strengths and limitations
A potential source of bias in this study was related to our participants and selection biases. Most of the participants were recruited through a national organisation for ADHD-patients. These participants were assumed to have a higher rate of medication use compared to young people with mental illness in general [52].To reduce bias in our sample, we used purposive sampling methods, including factors like age, gender, and duration of treatment. Another limitation was the overrepresentation of mothers among the parents, while fathers were underrepresented.
One methodological limitation of our digital interviewing approach was the absence of recording possibilities. Consequently, our data primarily relied on the researchers’ field notes rather than full-transcribed interviews. This limitation introduced possibility of biases, and information loss.
A strength of our study was qualitative interviews conducted with both adolescents and parents. This approach provided a more comprehensive perspective, covering a wide range of aspects such as their views on medication benefits, functions, side-effects, follow-up care and strategies for coping with medication routines. Furthermore, these perspectives were enriched by the exploration of differences and similarities between both groups. Parents played a crucial role in validating adolescents’ experiences and contextualizing them within a broader scope, including individual relationships and the perceived impact on family, school, and health service’s needs. Additionally, adolescents reported and validated the significance of parent’s experiences with medication, underscoring the importance of improved communication regarding information about medications and their potential side effects.
Conclusion
The aim of this study was to generate and validate findings to inform the development of modules on patients aged 12–15 years and parent experiences regarding medication use, and we incorporated survey questions about information about medications, side-effects, and follow-up care, which was important aspects reported by both patients and parents.
Interestingly, there were only minor differences between the aspects reported by parents and adolescents. Notably, parents emphasized the importance of follow-up care after assessment. The results from this current study hold implications for comprehending adolescents’ perceptions of medication use, with important aspects, but also validating important themes for survey questions.
Furthermore, more research is essential to delve into how adolescents’ ambivalence and mixed thoughts and feelings about medications use influence their behaviour. Such knowledge can prove crucial in understanding how adolescents approach adherence to and compliance with treatment.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to protection of personal data.
References
Garratt AM, Bjertnaes OA, Holmboe O, Hanssen-Bauer K. Parent experiences questionnaire for outpatient child and adolescent mental health services (PEQ-CAMHS outpatients): reliability and validity following a national survey. Child Adolesc Psychiatry Ment Health. 2011;5:18.
Iversen HH, Haugum M, Bjertnaes O. Reliability and validity of the Psychiatric Inpatient patient experience questionnaire – continuous electronic measurement (PIPEQ-CEM). BMC Health Serv Res. 2022;22(1):897.
Iversen HH, Bjertnaes O, Helland Y, Skrivarhaug T, The Adolescent Patient Experiences of Diabetes Care Questionnaire (APEQ-DC). Reliability and validity in a study based on data from the Norwegian Childhood Diabetes Registry. Patient Relat Outcome Meas. 2019;10:405–16.
Iversen HH, Helland Y, Bjertnaes O, Skrivarhaug T. Parent experiences of diabetes care questionnaire (PEQ-DC): reliability and validity following a national survey in Norway. BMC Health Serv Res. 2018;18(1):774.
Holmboe O, Iversen HH, Hanssen-Bauer K. Determinants of parents’ experiences with outpatient child and adolescent mental health services. Int J Ment Health Syst. 2011;5:22.
Bjertnaes ØA, Garratt A, Helgeland J, Holmboe O, Dahle KA, Hanssen-Bauer K, et al. [Parent assessment of outpatient child and adolescent mental health services]. Tidsskr nor Laegeforen. 2008;128(9):1041–5.
Haugum MDK, Iversen HH. Development of a questionnaire to measure children’s and adolescents’ experiences with outpatient child and adolescent mental health services. Oslo: Norwegian Institute of Public Health; 2019.
Atkinson MJ, Sinha A, Hass SL, Colman SS, Kumar RN, Brod M, et al. Validation of a general measure of treatment satisfaction, the treatment satisfaction questionnaire for medication (TSQM), using a national panel study of chronic disease. Health Qual Life Outcomes. 2004;2:12.
Bharmal M, Payne K, Atkinson MJ, Desrosiers MP, Morisky DE, Gemmen E. Validation of an abbreviated treatment satisfaction questionnaire for medication (TSQM-9) among patients on antihypertensive medications. Health Qual Life Outcomes. 2009;7:36.
Katusiime B, Corlett S, Reeve J, Krska J. Measuring medicine-related experiences from the patient perspective: a systematic review. Patient Relat Outcome Meas. 2016;7:157–71.
Price J, Cole V, Goodwin GM. Emotional side-effects of selective serotonin reuptake inhibitors: qualitative study. Br J Psychiatry. 2009;195(3):211–7.
Ruiz MA, Pardo A, Rejas J, Soto J, Villasante F, Aranguren JL. Development and validation of the treatment satisfaction with Medicines Questionnaire (SATMED-Q). Value Health. 2008;11(5):913–26.
Cox DJ, Davis MT, Cox BS, Burket RC, Merkel RL, Mikami AY, et al. Quantifying the relationship between perceived consequences of ADHD medication and its usage. J Atten Disord. 2015;19(1):78–83.
Martins MJRV, Pinto AM, Castilho P, Macedo AF, Pereira AT, Bajouco M, et al. Assessing beliefs and attitudes towards antipsychotic medication from a recovery-based perspective: psychometric properties of a new scale. Psychiatry Res. 2019;273:325–30.
Emilsson M, Berndtsson I, Gustafsson PA, Horne R, Marteinsdottir I. Reliability and validation of Swedish translation of beliefs about Medication Specific (BMQ-Specific) and brief illness perception questionnaire (B-IPQ) for use in adolescents with attention-deficit hyperactivity disorder. Nord J Psychiatry. 2020;74(2):89–95.
Garcia RR, Alvarado VS, Agraz FP, Barreto FR. Assesment of drug attitudes in patients with schizophrenia: psychometric properties of the DAI Spanish version. Actas Esp De Psiquiatria. 2004;32(3):138–42.
Niemeyer L, Schumm L, Mechler K, Jennen-Steinmetz C, Dittmann RW, Hage A. When I stop my medication, everything goes wrong: content analysis of interviews with adolescent patients treated with psychotropic medication. J Child Adolesc Psychopharmacol. 2018;28(9):655–62.
Bukstein OG, Arnold LE, Landgraf JM, Hodgkins P. Does switching from oral extended-release methylphenidate to the methylphenidate transdermal system affect health-related quality-of-life and medication satisfaction for children with attention-deficit/hyperactivity disorder? Child & Adolescent Psychiatry & Mental Health [Electronic Resource]. 2009;3(1):39.
Manos M, Frazier TW, Landgraf JM, Weiss M, Hodgkins P. HRQL and medication satisfaction in children with ADHD treated with the methylphenidate transdermal system. Curr Med Res Opin. 2009;25(12):3001–10.
Ninan A, Stewart SL, Theall L, King G, Evans R, Baiden P, et al. Psychotropic medication monitoring checklists: use and utility for children in residential care. Journal of the Canadian Academy of Child and Adolescent Psychiatry /. et de l’adolescent. 2014;23(1):38–47. Journal de l’Academie canadienne de psychiatrie de l’enfant.
Rofail D, Gray R, Gournay K. The development and internal consistency of the satisfaction with Antipsychotic Medication scale. Psychol Med. 2005;35(7):1063–72.
Gortz-Dorten A, Breuer D, Hautmann C, Rothenberger A, Dopfner M. What contributes to patient and parent satisfaction with medication in the treatment of children with ADHD? A report on the development of a new rating scale. Eur Child Adolesc Psychiatry. 2011;20(Suppl 2):S297–307.
Harpur RA, Thompson M, Daley D, Abikoff H, Sonuga-Barke EJ. The attention-deficit/hyperactivity disorder medication-related attitudes of patients and their parents. J Child Adolesc Psychopharmacol. 2008;18(5):461–73.
Steffenak AKM, Wilde-Larsson B, Hartz I, Nordström G. Experience of psychotropic drug use among young people with mental health problems. Nordic J Nurs Res. 2015;35(4):241–8.
Cuenca J, Glazebrook C, Kendall T, Hedderly T, Heyman I, Jackson G, et al. Perceptions of treatment for tics among young people with Tourette syndrome and their parents: a mixed methods study. BMC Psychiatry. 2015;15:46.
Meaux JB, Hester C, Smith B, Shoptaw A. Stimulant medications: a trade-off? The lived experience of adolescents with ADHD. J Spec Pediatr Nurs. 2006;11(4):214–26.
Kranke DA, Floersch J, Kranke BO, Munson MR. A qualitative investigation of self-stigma among adolescents taking psychiatric medication. Psychiatr Serv. 2011;62(8):893–9.
Murphy AL, Gardner DM, Kisely S, Cooke C, Kutcher SP, Hughes J. A qualitative study of antipsychotic medication experiences of Youth. J Can Acad Child Adolesc Psychiatry. 2015;24(1):61–9.
Floersch J, Longhofer JL, Kranke D, Townsend L, Integrating, Thematic. Grounded theory and narrative analysis:a case study of adolescent psychotropic treatment. Qualitative Social Work. 2010;9(3):407–25.
Floersch J, Townsend L, Longhofer J, Munson M, Winbush V, Kranke D, et al. Adolescent experience of psychotropic treatment. Transcult Psychiatry. 2009;46(1):157–79.
McMillan SS, Stewart V, Wheeler AJ, Kelly F, Stapleton H. Medication management in the context of mental illness: an exploratory study of young people living in Australia. BMC Public Health. 2020;20(1):1188.
Moses T. Adolescents’ commitment to continuing psychotropic medication: a preliminary investigation of considerations, contradictions, and correlates. Child Psychiatry Hum Dev. 2011;42(1):93–117.
Häge A, Weymann L, Bliznak L, Märker V, Mechler K, Dittmann RW. Non-adherence to psychotropic medication among adolescents - a systematic review of the literature. Z Kinder Jugendpsychiatr Psychother. 2018;46(1):69–78.
Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17.
Srimongkon P, Aslani P, Chen TF. Consumer-related factors influencing antidepressant adherence in unipolar depression: a qualitative study. Patient Prefer Adherence. 2018;12:1863–73.
Delman J, Clark JA, Eisen SV, Parker VA. Facilitators and barriers to the active participation of clients with serious mental illnesses in medication decision making: the perceptions of young adult clients. J Behav Health Serv Res. 2015;42(2):238–53.
Charach A, Yeung E, Volpe T, Goodale T, dosReis S. Exploring stimulant treatment in ADHD: narratives of young adolescents and their parents. BMC Psychiatry. 2014;14(1):110.
Dikec G, Kardelen C, Gonzalez LP, Mohammadzadeh M, Bilac O, Stock C. Perceptions and experiences of adolescents with Mental disorders and their parents about psychotropic medications in Turkey: a qualitative study. Int J Environ Res Public Health. 2022;19(15).
Sibeoni J, Orri M, Manolios E, Spodenkiewicz M, Labey M, Verneuil L, et al. Early-treatment stage for adolescents with depression and their parents: an IPSE qualitative study. European Child & Adolescent Psychiatry; 2022.
Skudal KE, Holmboe O. Resultater fra nasjonal brukererfaringsundersøkelse blant foresatte til barn og unge innen psykisk helsevern (BUP) i 2017 [Results following a national user experience survey among primary caregivers with mental health care for children and adolescents in 2017]. Oslo Folkehelseinstituttet. 2019.; 2019.
Fry A, Mitchell SA, Wiener L. Considerations for conducting and reporting digitally supported cognitive interviews with children and adults. J Patient Rep Outcomes. 2021;5(1):131.
Phillippi J, Lauderdale J. A guide to Field Notes for qualitative research: Context and Conversation. Qual Health Res. 2018;28(3):381–8.
Tessier S. From field notes, to transcripts, to tape recordings: evolution or combination? Int J Qualitative Methods. 2012;11(4):446–60.
Lindgren B-M, Lundman B, Graneheim UH. Abstraction and interpretation during the qualitative content analysis process. Int J Nurs Stud. 2020;108:103632.
Bengtsson M. How to plan and perform a qualitative study using content analysis. NursingPlus Open. 2016;2:8–14.
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–12.
Edgcomb JB, Zima B. Medication adherence among children and adolescents with severe Mental illness: a systematic review and Meta-analysis. J Child Adolesc Psychopharmacol. 2018;28(8):508–20.
Verma S, Agrawal R. Psychotropic medication adherence in children and adolescents. South Med J. 2021;114(7):388–94.
Murphy AL, Gardner DM, Kisely S, Cooke CA, Kutcher SP, Hughes J. System struggles and substitutes: a qualitative study of general practitioner and psychiatrist experiences of prescribing antipsychotics to children and adolescents. Clin Child Psychol Psychiatry. 2016;21(4):634–48.
Moses T. Parents’ conceptualization of adolescents’ mental health problems: who adopts a psychiatric perspective and does it make a difference? Community Ment Health J. 2011;47(1):67–81.
Carter N, Bryant-Lukosius D, DiCenso A, Blythe J, Neville AJ. The use of triangulation in qualitative research. Oncol Nurs Forum. 2014;41(5):545–7.
Hartz I, Skurtveit S, Steffenak AKM, Karlstad O, Handal M. Psychotropic drug use among 0–17 year olds during 2004–2014: a nationwide prescription database study. BMC Psychiatry. 2016;16.
Acknowledgements
The authors want to thank the adolescents and parents who participated and shared their experience. We want to thank Olaf Holmboe for conducting interviews, data collection, coding of data and preliminary analysis.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. This study was supported by the Norwegian Health Directorate and the Norwegian Institute of Public Health.
Open access funding provided by Norwegian Institute of Public Health (FHI)
Author information
Authors and Affiliations
Contributions
Investigation and project administration: AS. Conceptualization: All authors. Data analysis: AS, Methodology: All authors. Writing - original draft: AS and HHI. Writing - review & editing: AS and HHI.
Corresponding author
Ethics declarations
Ethical approval
This study has been approved by the Institutional Review Board at the Norwegian Institute of Public Health.
Informed consent statement
Written informed consent to participate in this study was provided by the adolescents and their parents. All study participants were informed of their right to refuse participation and to end the interview at any time.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Conflict of interest
The authors declare that there is no conflict of interest in this work. We used OpenAI’s ChatGPT, a large language model, to assist in editing drafts. ChatGPT’s involved primarily feedback on text style, spelling and grammar. Furthermore, the responses were carefully reviewed, and critically assessed by the researchers to ensure accuracy and relevance. The inclusion of AI-generated feedback was a complement to, rather than a replacement for, traditional research methodologies. We report according to the 32-item checklist of consolidated criteria for reporting qualitative studies (COREQ), see Additional File 3.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Steiro, A.K., Iversen, H.H. Important aspects of experiences from patients and parents related to medications in Child and Adolescents Mental Health Services (CAMHS) - a qualitative study. BMC Psychol 12, 458 (2024). https://doi.org/10.1186/s40359-024-01962-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-024-01962-9