
Abstract
Background
Self-regulation (SR) as the ability to regulate one’s own physical state, emotions, cognitions, and behavior, is considered to play a pivotal role in the concurrent and subsequent mental and physical health of an individual. Although SR skills encompass numerous sub-facets, previous research has often focused on only one or a few of these sub-facets, and only rarely on adolescence. Therefore, little is known about the development of the sub-facets, their interplay, and their specific contributions to future developmental outcomes, particularly in adolescence. To fill these research gaps, this study aims to prospectively examine (1) the development of SR and (2) their influence on adolescent-specific developmental outcomes in a large community sample.
Methods/design
Based on previously collected data from the Potsdam Intrapersonal Developmental Risk (PIER) study with three measurement points, the present prospective, longitudinal study aims to add a fourth measurement point (PIERYOUTH). We aim to retain at least 1074 participants now between 16 and 23 years of the initially 1657 participants (6–11 years of age at the first measurement point in 2012/2013; 52.2% female). The study will continue to follow a multi-method (questionnaires, physiological assessments, performance-based computer tasks), multi-facet (assessing various domains of SR), and multi-rater (self-, parent-, and teacher-report) approach. In addition, a broad range of adolescent-specific developmental outcomes is considered. In doing so, we will cover the development of SR and relevant outcomes over the period of 10 years. In addition, we intend to conduct a fifth measurement point (given prolonged funding) to investigate development up to young adulthood.
Discussion
With its broad and multimethodological approach, PIERYOUTH aims to contribute to a deeper understanding of the development and role of various SR sub-facets from middle childhood to adolescence. The large sample size and low drop-out rates in the first three measurements points form a sound database for our present prospective research.
Trial registration German Clinical Trials Register, registration number DRKS00030847.
Similar content being viewed by others


Background
Self-regulation (SR) is defined as "…intrinsic processes aimed at adjusting mental and physiological state adaptively to context. [It] encompasses cognitive control, emotion regulation, and top-down and bottom-up processes that alter emotion, behavior, or cognition to attempt to enhance adaptation (or to achieve an explicit or implicit goal or goal state)” (p. 364) [1]. Various constructs are subsumed under this umbrella term [2]. These include basal physiological functions, such as the ability to adaptively regulate physiological responses captured via heart-rate variability (HRV), executive functions (EF) as basal (neuro-)cognitive SR sub-facets, as well as complex, potentially intentional processes, such as regulating one's own behavior or emotions [1, 3]. So far, there is no unifying theory of SR, which impedes scientific progress in this field [4]. In the majority of the proposed conceptual and taxonomic classifications, a hierarchical structure of the SR skills is assumed, with EF viewed as precursors of or basis for more complex SR skills such as planning [1, 4,5,6]. Thus, based on the theoretical assumptions of [1], and acknowledging that SR is a broad concept that encompasses various and also differently complex skills, we divided SR into more basal and more complex SR sub-facets that can be assigned to the regulation of emotion, cognition, behavior, and physiology. In our heuristic conceptualization of SR, we postulate that inhibition or heart rate variability belong to the basal SR sub-facets, whereas we consider delay of gratification or decision making as complex sub-facets. Basal and complex SR sub-facets are conceptualized as forming hierarchical but bidirectional relations (as indicated by the arrows in Fig. 1), and we assume that the influence of basal on complex sub-facets is stronger than vice versa.

The conceptual hierarchical model of SR. The arrows indicate that a reciprocal relationship between basal and complex SR sub-facets is assumed. The line width indicates that the influence of basal on complex sub-facets is assumed to be stronger than vice versa
Commencing in early childhood, SR skills dynamically develop during different stages of life at varying paces. Adolescence (i.e., from puberty till the early twenties; [7]) is a period of extensive changes in the expression, differentiation, and interconnectedness of the various SR competencies [8,9,10,11]. The development of SR from childhood to adolescence shows continuities and discontinuities, and little is known about their causes and predictors to date [12]. Furthermore, individual differences and external influences characterize SR competencies in adolescence [1, 10, 13]. SR is not only shaped by the individuals themselves but also by their social environment (i.e., parents and peers; [14,15,16]. In addition, the SR of an individual also affects the social environment [15], with these transactional person-environment relationships further driving individual development [17, 18].
There is consensus that the degree, differentiation, and interconnectedness of SR skills continue to unfold until young adulthood [8, 9, 11]. Based on our conceptual model, we postulate that during adolescence, complex SR sub-facets successively develop and unfold their potential [3, 10, 19]. This formation process of complex SR essentially builds on the expression of the basal sub-facets. Regulation processes are a fundamental driver of transactional person-environment relations that excel individual development [17, 18]. In adolescence, individual differences in SR become increasingly important as adolescents can choose their environment more independently. Thus, environment and behavior have a reciprocal relationship [18]. Emerging complex SR skills enable adolescents to identify appropriate goals, use planning strategies to achieve goals, and weigh short-term benefits against long-term consequences [4, 20]. Particularly in this age range, however, longitudinal evidence on the typical development of various SR sub-facets and its importance for the accomplishment of adolescent-specific developmental tasks is still scarce [12, 15, 21,22,23,24]. Our longitudinal research will therefore increase our understanding of the development and impact of SR, especially in the previously neglected but vulnerable period from puberty to early adulthood [25].
Research has consistently indicated positive associations between SR and various positive developmental outcomes, such as physical and mental health, well-being, or career success [26,27,28,29,30,31,32]. Consequently, a broad set of well-developed SR skills has been considered critical for adaptive development [33]. Similarly, low SR skills have been discussed as a "generic risk profile" [34,35,36]. That is, at least a certain level of SR skills is considered as a prerequisite of mastering relevant developmental tasks as well as everyday challenges. Adolescence is particularly important because it sets the course for adulthood by progress in social (e.g., the detachment from the parental home, establishment of romantic relationships), personal (e.g., the establishment of a stable identity), and achievement-related (e.g., school graduation, career choice) development [37]. Moreover, in this age range, challenges for SR arise from increasing personal responsibility as well as from the need to cope adequately with developmental tasks. Thus, adolescence is considered a potential turning point for adaptive or maladaptive development [38]: Adverse behaviors occur more frequently but develop very differently with remissions, aggravations, or chronifications (e.g., increased incidence of mental health problems; [39]). Additionally, some adolescents face a high comorbidity of mental health problems and an accumulation of developmental risks [40, 41].
However, a comprehensive meta-analysis on the role of SR in childhood and adolescence [30] has revealed that there is still a paucity of research that considered adolescent samples, as the majority of studies focused on early and middle childhood. Complicating matters further, researchers used different approaches to assess SR (e.g., parent and teacher reports; performance-based assessments), and the type of assessment was the most important moderator of the pooled effect sizes. In addition, many relevant outcomes that are highly relevant in adolescence, such as prosocial behavior, identity development, disordered eating behavior or experience of stigmatization, have not been adequately addressed. Because analyses have often followed an outcome-specific approach (i.e., focusing on single areas, such as aggressive or anxious behavior), little is known about the generic or domain-specific contribution of SR across different developmental outcomes. In addition, the opposite is also true: because analyses have often considered only one or a few sub-facets of SR, little is known about particular powerful sub-facets of SR and their interplay in predicting single or even multiple outcomes. Besides addressing the potential influence of (single and multiple) SR skills on various developmental outcomes, it is also relevant to explore which intra- and interpersonal factors (e.g., influence from significant others) can contribute to the individual level of SR in adolescence. Therefore, a comprehensive approach that concurrently includes multiple SR sub-facets and multiple outcomes over time is needed to analyze the dynamic and bi-directional association of SR with developmental outcomes in adolescence.
We will address these research gaps in the continuation of our prospective PIER-study (“Potsdam Intrapersonal Developmental Risk Study”) that has already captured the development from 6 to 13 years through three measurement points and will be extended to include the critical developmental period of late adolescence (16–21 years). Adding further measurement points will contribute to a comprehensive understanding of SR development from childhood to adolescence and its meaning for other areas of development.
Methods/design
The PIER-study and its continuation as PIERYOUTH is a prospective longitudinal study. Based on the previously collected data on participants in the PIER study (with three measurement points), this study extends collected data by a fourth measurement point which offers new developmental perspectives. To ensure longitudinal comparability while at the same time considering normative developmental changes, the previously applied methods/measures will be continued wherever possible and, if necessary, adjusted to the age of the participants (e.g., self-instead of parent-report). Furthermore, additional measures will be implemented to address additional central aspects of SR that become relevant in adolescence and young adulthood (e.g., planning behavior or risk taking). In short, PIERYOUTH is a prospective, multi-method (encompassing physiological measures, performance-based computer tasks, questionnaires) multi-facet (including measures that assess cognitive, emotional, physiological and behavioral sub-facets of SR) and multi-rater (self- and parent report) approach to study the development and relevance of SR from middle childhood to late adolescence.
Aims of the study
To close the aforementioned research gaps with respect to (1) the developmental course of SR and (2) the contribution of SR to different developmental outcomes in adolescence, PIERYOUTH will address the following research questions:
-
Q1: Developmental trajectories of SR sub-facets.
-
Q1.1: Which continuities and discontinuities emerge for the developmental trajectories of SR skills from middle childhood to adolescence?
-
Q1.2: How can specific developmental patterns of SR be predicted?
-
Q1.3: How do individual SR skills develop in interaction with the level of SR skills in the peer group?
-
Q2: Influence of SR skills on adolescence-specific developmental aspects.
-
Q2.1: How do SR skills in middle childhood affect relevant outcome variables in adolescence?
-
Q2.2: What is the contribution of SR combined with predictors previously established in literature?
-
Q2.3: What is the impact of SR in the context of peer groups (as a social norm) on outcomes?
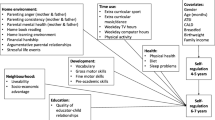
We postulate that developmental processes and outcomes in middle childhood influence SR skills [Q1], which in turn influence outcomes in adolescence [Q1.2; Q2]. Furthermore, we assume bidirectional relations between contextual factors and SR [Q1.3]. With respect to Q2, we hypothesize that SR proves to be a central predictor for relevant developmental outcomes in adolescence. In terms of a cascade model, developmental outcomes can themselves become predictors, and diverse interactions between the predisposing factors in middle childhood are assumed. Figure 2 illustrates the previous and to-be-generated prospective database that can be drawn upon to answer these research questions in PIERyouth.

Exemplary overview of constructs collected longitudinally and research questions
Study participants
The sample is based on the previously conducted PIER study with data from 1657 children (52.1% girls, average age: 8.36, SD = 0.95) at the first measurement point (T1) in 2011/2012. The aim was to recruit entire classes of elementary schools, if possible, to ensure economic data collection (several individuals tested at one location) in comparable social environments. The children were recruited in 120 classes (first to third grade) spread across 33 schools in the federal state of Brandenburg. To obtain a most representative sample, schools located in rural and urban areas and in regions with varying social stratification were included. This sample has been successfully followed-up over three years with only low drop-out rates at the second (T2) and third measurement points (T3; see Table 1). With respect to the forthcoming fourth PIERYOUTH measurement point (T4), it can be assumed that due to the long interval since T3 (8 years) and the probable changes in school and residence that have occurred in the meantime, the drop-out rate will rise to a conservative estimate of around 30%. Therefore, we assume that 1074 adolescents and 750 parents will remain in the sample. Because not all participants aren’t still in school, no further data from teachers are collect at T4. Dependent on further funding, a fifth measurement point is planned three years later, aiming for 1020 participants.
Recruitment strategy
We are contacting all eligible 1590 families (70 families provided at T3 no informed consent for further contact) from the PIER-study via mail to request their renewed participation. Due to the fact, that many former participants will be of legal age and due to the new General Data Protection Regulation (GDPR), it is necessary to obtain renewed written consent. Because the participants were minors at the former measurement points, we only have the address data of the parents. However, the majority of children have presumably not yet finished school or are still in contact with their parents. Therefore, it seems likely that they continue to live at home or can be contacted through their parents. If no valid contact data is available, the residents’ registration office will be contacted to disclose the latest address.
Figure 3 shows an overview of the recruitment strategy. In order to obtain renewed informed consent, a letter including relevant study information and declaration of consent forms (in case of minors, also a parental consent form for their child’s participation) will be sent to the families. In case of no response within two weeks, we will re-contact the families by mail or telephone (if parents’ email addresses and telephone numbers are available). Particularly phone calls are an important means to get in direct contact with the families that also facilitates discussing and addressing potential barriers to renewed participation. Telephone calls will follow the spirit of motivational interviewing that has proven particularly helpful to ensure retention [42]. In case of unavailable mail/phone data or further lack of response after three weeks, the families will receive a reminder in the form of a postcard and, in case of further lack of response, a second invitation letter. We aim to contact all participants at least three times in order to realize a high retention rate. After providing written informed consent, participants will receive a link to arrange an online appointment for testing.

Overview of recruitment strategy. The symbol with the cross mark represents the exclusion from participation
Data collection strategy
In contrast to the initial plan of conducting one longer face-to-face session, data collection had to be adjusted due to contact restrictions following the Covid-19 pandemic. It is now taking place in two separate sessions, a longer online session followed by a short face-to-face onsite session. This procedure deviates from the prior data assessment at T1–T3 that took place face-to-face and in schools (two sessions per person, with a duration of around 50 min each). In PIERYOUTH, the young people will arrange an appointment for an online session with a trained test administrator. This online session will take about 2 h. At the beginning of the online session, the test administrator briefly explains the test instructions. Throughout the session, they are available for questions and activate the experiments (randomized in four blocks). The participants can complete the individual questionnaires and performance-based computer tasks at their own pace. The test administrator can see the participant’s progress, but not their answers or performance. At the end of the online survey, a 30 min face-to-face on site appointment will be arranged. During this session, the procedures that cannot be conducted online (e.g., objective measures, such as heart-rate variability (HRV), anthropomorphic measurements) will be carried out. As compensation, participants will receive a total of 30€. In addition, participants can win up to additional 15€ as part of two experiments (Balloon Analogue Risk Task (BART); distributive behavior task). To increase adherence to the face-to-face on site session, additional vouchers were raffled off for participation. If interested, participants will receive aggregated study results provided after data analysis. Ethical approval was obtained from the institutional review board of the University of Potsdam (8/84th meeting—30.03.2020).
Study measures
The PIER-study already included multiple measures of SR as self-reports, parent- and teacher-reports, and performance-based computer tasks. On a construct level, these assessments and objective measures continue in PIERYOUTH, although sometimes the specific assessment procedure had to be adjusted to the older age of the participants. In the following, not only the assessments at T4 will be described, but also the corresponding assessments at T1–T3 in order to clarify necessary age-dependent adjustments. An overview of the study measures is presented in Table 2. Of note, the questionnaires and performance-based tasks are presented to the participants in a block-randomized sequence in order to control for order effects (4 blocks). The computer tasks were programmed in E-Prime 2.0 Professional (2012 Psychology Software Tools) at T1–T3 and in JATOS/OpenSesame at T4. Online questionnaires were programmed with SoSci Survey (version 3.4).
Self-regulation
As mentioned above, SR skills were divided in basal and complex SR sub-facets.
Basal SR sub-facets
Basal SR sub-facets include inhibition, working-memory updating, cognitive flexibility, heart rate variability (HRV), and emotional reactivity. Inhibition, cognitive flexibility and emotional reactivity are collected online, while the HRV and working-memory updating are collected in the face-to-face on site assessment.
Inhibition
The ability to control, modulate, and plan one’s behavior, to suppress primary behavioral impulses and inappropriate responses, and to resist impulsive behavior was assessed at T1–T3 via parent-ratings with six items from the Inhibitory Control subscale of the Temperament in Middle Childhood Questionnaire [43]. The ability to suppress primary behavioral impulses in favor of a less dominant response was also assessed with a performance-based measure at T1–T3 using an adaptation of the Fruit-Stroop Task [44, 45]. At T4, an age-appropriate computer-based Stroop Task is used [46]. Against a black background, participants see a color word (RED, BLUE, GREEN) printed in different colors (red, blue, green). After the color word appears, the participants have to name the ink-color as quickly as possible. The first 42 trials are performed without response conflicts (words replaced by rows of three to five asterisks), followed by runs with color words. The initial 42 color words are presented with congruent ink, and the following 42 words with incongruent ink, which requires the inhibition of a predominant response (e.g., reading the color word) to correctly name the ink-color. Inhibition capacities are measured via interference scores calculated from reaction times or accuracy in congruent relative to incongruent trials. Preceding the Stroop test at T4, potential color-vision deficiency is assessed via self-report with two self-constructed items: whether the adolescent is struggling with identifying colors and, if applicable, from which color-vision deficiency they are suffering.
Working-memory updating
At T1–T3, the ability to actively monitor and manipulate information in short-term memory was assessed using the Digit Span Backward (ZN-R) subtest of the German version of the Wechsler Intelligence Scale for Children—Fourth Edition (WISC-IV; 6–16 years; [47]). At T4, the corresponding subtest of the Wechsler Adult Intelligence scale—Fourth Edition (WAIS-IV; from 16 years; [48]) as an age-appropriate version is used. The participants hear a series of individual spoken digits and are asked to verbally repeat the digits in reverse order. After a correct repetition, the following series is extended by one digit, and after two incorrect turns, the test is terminated. The measure for updating capacity is the length of the final sequence or the number of sequences repeated correctly in reversed order.
Cognitive flexibility
The ability to adjust the attentional focus to current demands or to flexibly shift between mental sets and demands was assessed via the child-appropriate, performance-based Cognitive Flexibility Task [49] at T1 and T2. From T3 onwards, the age-appropriate performance-based Dimensional Change Card Sorting (DCCS) task is being used [50]: On a computer screen, participants are presented with two geometrical symbols that vary across the two dimensions ‘shape’ and ‘color’ (i.e., a blue box and yellow star). A third symbol with complimentary features (i.e., blue star) must then be matched as quickly as possible to one of the two original shapes via keypress according to a fixed rule indicted by a verbal cue (i.e., ‘shape’ or ‘color’). The 20 trials of the first block establish a dominant rule (i.e., 50% of participants sort by shape or color, respectively). In the second block, trials appear in pseudo-random order: 45 non-switch trials follow the dominant rule and 15 switch trials require the other, non-dominant rule. There is always at least one dominant trial between two non-dominant trials. The costs of switching to the new sorting rule are calculated from reaction times or accuracy in the switch relative to the non-switch trials. High cognitive flexibility comes with low switch costs.
Heart rate variability (HRV)
HRV, as a measure of neurovegetative activity and autonomic function of the heart, characterizes variations in heart rate over a given measurement period. High HRV is considered a biological marker of good self-regulatory capacity [51, 52]. HRV was collected at T1 and T2 using electrodes on the palms of the hands for a period of 3 min using Polar watches (RS800CX, Polar Electro Oy, Kempele) [53]. From T4 onwards, the heart rate is being objectively measured using clamp electrodes applied on the participants’ wrists and the software BioSign HRV-Scanner standard professional version 3.5 [54] for a period of 5 min. Furthermore, a number of external factors that may influence HRV are assessed as self-report. With self-constructed items, adolescents indicate whether they have (1) consumed caffeine in the previous 2 h, (2) consumed other cardioactive substances (such as nicotine, alcohol, other drugs) or undergone intensive physical training during the last 24 h. Moreover, three open questions are used to assess the quality and duration of sleep during the previous night, and the time of the last meal.
Emotional reactivity
The tendency to show strong emotional reactions in general was recorded at T1–T3 with the subscale emotional control of the Behavior Rating Inventory of Executive Function (BRIEF; [55]) via parent-report. From T4 onwards, the same scale is used to assess emotional reactivity via self- and parent-report. The proneness to react with anger in the face of interruption of tasks or hindrance in goal achievement in particular was recorded at T1 and T2 using seven items of the Anger/Frustration subscale of the Temperament in Middle Childhood Questionnaire (TMCQ; [43]) via parent-report. From T4 onwards, anger reactivity is assessed as self-report via six items (as suggested by [56]) of the Anger subscale of the Buss-Perry Aggression Questionnaire (German: [56]).
Complex SR sub-facets
Complex SR sub-facets include emotion regulation strategies, affective decision making, delay of gratification, risk-taking/impulsivity, planning behavior, conscientiousness, and eating-related SR. All these assessments are conducted during the online session.
Emotion regulation strategies
At T1–T3, anger-regulation strategies (dispersion, perseveration, expression, control, external regulation) were recorded via age-appropriately adapted items of the Dealing with Anger subscale of the Questionnaire to Elicit Emotion Regulation in Children and Adolescents (FEEL-KJ; [57]) via self- and parent-reports. Furthermore, at T1 and T2 strategies of dealing with anger were assessed via an adaption of the Emotion Regulation subscale of the Intelligence and Development Scales (IDS; [58]) via self-reports. At T4, the German versions of the Emotion Regulation Questionnaire (ERQ; [59]) and the 27-item version of the Cognitive Emotion Regulation Questionnaire (CERQ; [60]) are used to capture self-reported emotion-regulation strategies, namely cognitive reappraisal and expressive suppression (ERQ) as well as “functional” (e.g., relativizing, refocusing) and “dysfunctional” (e.g., self-blame, rumination) strategies (CERQ).
Affective decision-making
The tendency to make emotion-driven decisions and take risks was assessed at T1–T3 using the computer-based Hungry Donkey Task [61]. At T4, we use an age-appropriate version with a higher number of trials and a more complex pattern of win-loss probabilities [62]. Participants are asked to help a hungry donkey and to collect as many apples as possible by selecting and opening one of four depicted doors in 100 trials. After opening a door, certain numbers of gained (green) and lost (red) apples are displayed (e.g., + 4, − 8). The exact win-loss probability is different for each door and unknown to the participants. Relevant measures are the number of apples obtained (net gain) or the difference of choices for “disadvantageous” door positions (yielding higher immediate gains but long-term losses) versus “advantageous” door positions (yielding lower immediate gains but long-term gains) across trials (e.g., all trials or in learning blocks with several trials each). A preference for disadvantageous doors reflects poorer affective decision making, a preference for immediate rewards, or a stronger insensitivity to negative consequences.
Delay of gratification
The ability to forgo an immediate reward and to control impulses in favor of a larger or higher value in the future was assessed at T1–T3 using four decision questions [63]. Children needed to decide whether they wanted to obtain a smaller amount of real incentives (2 sweets, 2 toys) immediately or a larger amount some time later. At T4, the German Delay Discounting Test (DDT; [64, 65]) is used. In 27 items, participants are asked to imagine they would receive money from the test administrator, and they must choose between a smaller, immediate amount of money or a larger amount of money to be received later. The derived discount rate informs on how much a person devalues a future reward (referred to as delay discounting). The discount rate depends, among other variables, on the value of the immediately available reward and the delay interval. A low devaluation of future rewards speaks for higher delay-of-gratification ability.
Behavioral control/impulsivity
At T4, this facet is assessed via self- and parent-reports, using a short version of the UPPS Impulsive Behavior Scale (UPPS; adapted from [66] and [67]; 10 items on four subscales: lack of premediation, urgency, sensation seeking, and (lack of) perseverance) and the Self-Regulation Scale (SRS, 10 items; [68]). The SRS captures the ability to sustain difficult actions even when attention or motivation is impaired. Furthermore, at T4, risk-taking is assessed using the computer-based Balloon Analogue Risk Task [69] as a behavioral measure with 20 trials. The task consists of inflating a balloon displayed on a computer screen by pressing a button repeatedly, with each press yielding a small monetary reward (0.5 Cent) that the participants actually receive after the test session. After each key press, participants have to decide either to continue inflating the balloon and thus increase their monetary reward, or to stop inflating it. With further inflation, participants increase the risk that the balloon will burst (in which case all money of this trial is lost), whereas termination secures the money earned in this trial. As dependent variable the so-called adjusted average pumps, i.e., pumps on the balloons which did not explode, will be calculated.
Planning behavior
At T1–T3, the child’s ability to deal with tasks that have to be mastered now or in the future was measured via teacher-reports with the Plan/Organize subscale of the BRIEF [55]. At T4, this subscale is included as a self- and parent-report. Additionally, planning behavior is assessed with the two Intention-items of the UPPS (adapted from [66, 67]) described above. Furthermore, five items of the Impulsivity subscale from the German version of the Barratt Impulsiveness Scale (BIS) (German: [70]) are assessed via self-report.
Conscientiousness
Conscientiousness, one of the personality dimensions of the Big Five, is considered as self-regulatory competence in personality psychology [71]. Conscientiousness refers to the tendency to be disciplined, perform well, and be reliable. At T4, it is assessed using parsimonious subscale of a short version the Big Five Inventory-SOEP (BFI-S; [72]) via self-report (3 items).
Eating-related SR
SR competencies associated with eating behavior that are regarded as contributing to weight status were assessed at T1–T3. The emotional overeating, emotional undereating, food responsiveness, and satiety responsiveness subscales of the Children’s Eating Behavior Questionnaire were assessed via parent-report (CEBQ; [73]). Moreover, at T3, a short version of the restrictive eating behavior subscale of the Dutch Eating Behavior Questionnaire for children (DEBQ; [74]) and six items of the Eating Behavior Disturbance Questionnaire [75] assessing emotional eating were used (self-reports). Furthermore, the subscale external eating behavior of the DEBQ [75] was assessed via parent-report. At T4, the CEBQ is assessed via parent-report, and the German version of the Adult Eating Behavior Questionnaire (AEBQ; [76, 77]) is applied as self-report. An age-appropriate version of the DEBQ is used to assess restrictive eating behavior via self-report and external eating behavior via parent-report [78]. Furthermore, the survey is assessing food self-regulation via self-report. On two self-constructed slider scales, the participants are indicating their determination of losing weight and changing eating behaviors in the near future.
Outcome measures and predictors
Outcome measures and predictors encompass multiple measures that are of importance in adolescence, amongst others weight status, body dissatisfaction, stigma, prosocial behavior, moral identity, emotional and behavioral problems, as well as social information processing.
Weight status
Children’s weight status was measured at T1–T3 using parent-reports and objective anthropometric measurements of height and weight (dressed but without jacket/shoes). Body weight was assessed with the personal floor scale Kern MPB 300K100, and the Stadiometer seca 217 measured the participants’ body height. To ensure privacy, measurement and weighing were performed individually and, if necessary, behind a folding screen. At T4, this standardized protocol is implemented during the on-site session. Self-reported weight is additionally collected with one self-constructed item in the online survey.
Body dissatisfaction
Body dissatisfaction was assessed at T1–T3 using child-specific body silhouettes [79]: Children were asked to indicate their current and their desired body figure using seven sex-specific body silhouettes with ascending degrees of relative fat mass. The difference between the two selected silhouettes can be used as indicator of body dissatisfaction [80]. In order to account for physical changes during adolescence, nine sex-specific silhouettes of Thompson and Gray [81] are applied at T4. To also cover aspects relevant for body images among males, nine additional silhouettes from Lynch and Zellner [82] are applied to map muscularity. The attitude subscale of the German Drive for Muscularity Scale [83] is assessing the muscularity related dissatisfaction of male and female participants. In addition, at T1–T4 single items are assessing the participants’ weight satisfaction and relevance of weight and one self-constructed item rates the current estimation of one’s own weight status (reaching from “very underweight” to “very overweight) as self-report.
Internalized weight stigma
At T3, internalized weight stigma was assessed using the child-adapted version of the Weight Bias Internalization Scale (WBIS-C; [84]). This scale is also used atT4.
Stigma
At T1–T3, perceptions of being teased by others about one’s weight were assessed via self-report using an abbreviated version of the appearance-related subscale of the Perception of Teasing Scale (POTS; [85]). Additionally, it was assessed from which persons (groups) the stigmatizations originated. At T3–T4, weight-related and performance-related teasing is being measured via the POTS; with additional items assessing suffering caused by each teasing form (POTS; [85]). Furthermore, at T4 the two subscales exclusion and parental encouragement of the appearance-related social pressure questionnaire (FASD; [86]) are used with four items each.
Self-esteem
The positive view of oneself was recorded at T1 and T2 with the Self-Esteem subscale of the health-related quality of life questionnaire (KINDL; [87]) and at T3 with the Self-Esteem subscale of the Child Health Questionnaire (CHQ; [88, 89]). At T4, the three-item Rosenberg’s self-esteem scale [90] is used.
Prosocial behavior
At T1–T3, prosocial behavior was measured via parent- and teacher reports via the accordant subscale of the Strengths and Difficulties Questionnaire (SDQ) (five items; [91, 92]). At T4, it is continued as a self- and parent report. In addition, prosocial behavior will be additionally assessed in an age-appropriate experiment with a particular focus on distributive behavior. In line with previous research in adult samples [93, 94], participants are requested to distribute a constant amount of money (7 Euro) between themselves and other participants under three conditions (dictator game, ultimatum game, third-person punishment scenario). Participants receive the actual money that they have kept for themselves from one randomly selected condition together with the money for the study participation. Finally, we assess prosocial behavior via four items asking about the adolescents’ actual prosocial behavior in everyday situations [95].
Moral identity
Following procedures in adolescence [96] and adulthood [97] at T4, participants are being asked to rate the personal importance of 18 positive, partially morality-related traits (e.g., being honest, fair) to assess the relative importance of moral traits [98].
Justice sensitivity
At T4, sensitivity to injustice from the victim’s, observer’s, and perpetrator’s perspective will be assessed via self-reports with five congruently worded items per scale from the Justice Sensitivity Inventory for Children and Adolescents (JSI-CA 5; [99]).
Loss of control eating and binge eating (BE)
At T1–T3, the SCOFF (5 items; [100]), allowing for a categorical (conspicuous/inconspicuous) and a dimensional view of abnormal eating behavior, was used as a screening instrument to detect conspicuous eating behavior as self- and parent-report. For specific consideration of eating behaviors associated with Binge Eating (BE), an age-adapted version of the Questionnaire of Eating and Weight Patterns (QEWP; [101, 102]) was used. At T4, these survey instruments are continued as self-reports, together with the SCOFF as a parent version. Furthermore, binge eating and compensatory behaviors as key behavioral features of eating disorders are assessed via self-report with six items of the German version of the Eating Disorder Examination Questionnaire (EDE-Q; [103]). Based on these answers, branching items of the EDE-Q assess the frequency of binge eating and compensatory behaviors. The Loss of Control Over Eating scale (LOCES; [104, 105]) with seven items is also included.
Emotional and behavioral problems
At T1–T3, we used the Strengths and Difficulties Questionnaire (SDQ; [91, 92]) with the four subscales emotional problems, conduct problems, hyperactivity, and peer problems (parent- and teacher-report). Further, the SDQ encompasses the potential impairment caused by symptoms. At T4, the age-appropriate version SDQ-18+ is implemented as a self-report measure. In addition, the parent-report of the SDQ is also applied to allow for continuity in reporting, while also controlling for informant effects. The SDQ can be evaluated as a total problems scale and at subscale level.
Depressive symptoms
Using the diagnostic classification systems for mental disorders in childhood and adolescence of the ICD-10 and DSM-IV (DISYPS-KJ; [106]), children rated four dichotomous items (yes/no) on depressive symptoms at T1 and T2. At T3, depressiveness was assessed with six items of the Depression Test for Children of Elementary School Age (DTGA; [107]). From T4 onwards, the Patient Health Questionnaire, PHQ-8 (i.e., PHQ-9 without the item on suicidality; [108, 109] is used (self-report). The PHQ-8 includes eight items that map the diagnostic criteria of depression according to the DSM and thus the presence and severity of depressive symptoms [109].
Anxiety symptoms
At T1 and T2, anxiety was assessed using 11 items of the Mannheim Adolescent Questionnaire (MJF; [110]) and at T3 using six items of the Child Anxiety Test 2 (KAT-II; [111]). At T4, the Generalized Anxiety Disorder Screener (GAD-7; [112]), a seven-item instrument for assessing symptoms of generalized anxiety disorder according to the DSM, is used (self-report).
Social information processing (SIP)
At T4, individual specifics of the cognitive processing of social information (in different processing steps) are assessed with an adapted version of the Scenes for Social Information Processing in Adolescence (SSIPA; [113]) survey. Adolescents are given three age-appropriate descriptions of potentially provocative social situations, each followed by two questions indicating the participant’s interpretation of each situation (likelihood of hostility/neutral intention on the part of the protagonist), five items assessing triggered emotions (e.g., anger, sadness, embarrassment), their evaluation of four possible responses (assertiveness, passivity, overt/relational aggression) with five items each assessing likelihood of choosing each of the responses. From this, scores are calculated for specific processing styles for different SIP steps.
Aggressive and antisocial behavior
At T1–T3, antisocial behavior was assessed using the delinquent behavior subscale of the Child Behavior Checklist (CBCL/4–18; [114, 115]) via parent-report. At T4, parents rate their child’s antisocial behavior with 17 items from the Adult Behavior Checklist (ABCL; [116, 117]) and two items from the CBCL [114, 118]. Adolescents self-report on antisocial behavior with the items from the Adult Self-Report (ASR; [116, 117]) and one additional item from the Youth Self-Report (YSR; [114, 118]). Forms (physical, relational, verbal) and functions (proactive, reactive) of aggressive behavior were assessed at T1–T3 via teacher-reports and at T3 via self-reports, using seven and six items from the Children’s Social Behavior Scale (CSBS-T; [119]) and the Instrument for Reactive and Proactive Aggression (IRPA; [120]), respectively. At T4, both questionnaires on aggressive behavior are used as self- and parent-reports.
Other variables
In addition, a number of variables are assessed that may be included in the analyses as grouping or control variables.
Sociodemographic variables
Age and gender of the participants are recorded in the self- and parent-reports. At T4, the gender category “diverse” is added to “male” and “female”.
Socioeconomic status (SES) and education
At T1–T3, SES was estimated using the educational attainment of the mother and father, on a scale from 1 (missing middle school degree) to 6 (university degree). At T3, the occupation of both parents, the household size, and the monthly household income were additionally recorded. At T4, subjectively perceived social status is assessed as self-report with the McArthur Scale [121], because the subjective assessment of relative status has proven to be a particularly good indicator of social position. Adolescents are indicating on a “ladder” where they locate their social position relative to others. Furthermore, they report their current occupation (student, trainee, etc.). In addition, parents provide information on the Winkler-Index [122] which reflects the educational, occupational, and financial background of the families.
Contact with parents
At T4, parents are asked whether their child still lives with them (or already moved out) and how often they are in contact with their child.
Migration background
At T4, to determine migration background, the adolescents report about the language spoken at home, as well as their and their parents’ country of birth.
Pubertal status
At T4, two self-constructed items are used to assess sex-specific bodily changes during puberty. Adolescents rate the concurrency of their body changes in comparison to their peers on a 5-point Likert-scale ranging from significantly earlier to significantly later. Additionally, females indicate whether they have experienced their first menstruation, and males whether their voice has changed already.
Cognitive theory of mind
The ability to infer action intentions and beliefs of others was assessed at T1 and T2 with six items of a cartoon task [123]. At T3 and T4, the computer-based Belief-Desire Reasoning Task [124] is applied. In this task with 30 trials, participants receive information about another person’s preferences (e.g., she likes/does not like apples) and assumptions about the state of reality (e.g., she thinks that the apples are in the blue/yellow box) and are then asked to choose which of the two boxes that person will open.
Affective theory of mind
The ability to recognize the emotional states of others was assessed at T1 and T2 with six items of a cartoon task [123]. From T3 onwards, the German version of the computer-based Facial Scale of the Cambridge Mindreading Face-Voice Battery [125] is applied. Participants watch 5.5 s long, silent movie clips in which actors portray various complex emotions (e.g., pensive, confused). Subsequently, participants are asked to select (by pressing a key) one adjective that best describes the emotion from four adjectives presented on the screen. At T4, 14 of the videos show adult actors, and six videos show adolescent actors.
Cognitive processing speed
Due to strong overlaps with some cognitively anchored self-regulatory competencies, cognitive processing speed was measured using the Digit Symbol Coding Test (ZST) of the German version of the Wechsler Intelligence Scale for Children—Fourth Edition (WISC-IV; 6–16 years; [47]) at T1–T3. At T4, the corresponding subtest of the Wechsler Adult Intelligence scale—Fourth Edition (WAIS-IV; from 16 years; [48]) as an age-appropriate version is used. Participants are asked to assign abstract symbols to a series of numbers using a given coding key. The number of correct matches produced in a limited time (120 s) is measured.
Family risk factors
At T2 and T3, the Family Adversity Index (FAI; German adaptation after [126]) was used to record various critical life events of the child over the entire life span via parent reports with dichotomous items (yes/no) (e.g., including massive partnership conflicts of the parents, mental disorder of a parent). At T4, these questions are expanded by further critical life events, and parents are asked to rate them separately concerning different life phases of their child (until the 6th birthday and in in the last five years).
Current burdens
T4 takes place during the COVID-19 pandemic and the war in Ukraine, both of which are associated with increased psychosocial stress for children, adolescents and their families [127, 128]. Therefore, the perceived extent of corona-related stress as well as the stress caused by the current global political situation are assessed via self-report on a 7-point Likert-scale ranging from ‘not burdensome at all’ to ‘extremely burdensome’.
Use of mental health services
At T4, a self-constructed item explores adolescents’ utilization of therapy until T4 (self- and parent-report). If applicable, more specific information is requested (e.g., type of therapy, reasons for therapy, duration of therapy).
Level of personality functioning
At T4, the Operationalized Psychodynamic Diagnosis—Structure Questionnaire Short Version (OPD-SQS; [129]) assesses the level of personality functioning in terms of perception, control, communication and attachment (self-report).
Social media use
At T1–T4, parents and children/adolescents rate the child’s/adolescents’ time spent on average on physical activity, watching television, and using a computer (items adapted from the KiGGS-study (a cohort longitudinal study on the health of children, adolescents and young adults in Germany; [130, 131]). At T4, additional self-report items are assessing the adolescents’ usage of social media (frequency and duration of series consumption; active and passive social media use according to [132]; type of media used). Another two self-report items of the Sociocultural Attitudes Towards Appearance Questionnaire-IV (SATAQ‐IV-R [133]; German Version: [134]) are assessing media pressure experienced by the adolescents.
Academic achievement
At T1–T3, teachers rated a child’s abilities regarding grammar, concentration, memory, reading, spelling, numeracy and reasoning (on a scale of 1–6 corresponding to school grades) using the Potsdam Teacher Questionnaire [135]. Additionally, parents indicated their child’s grades in German reading and spelling (T1–T3) and mathematics (T3). At T4, adolescents indicate how they perceive their academic accomplishments relative to their peers based on a 10-point visual analog scale in the form of a hierarchical ladder (from 0 “on a par with people with the worst performances” to 10 “on a par with people with the best performance”).
Social desirability
At T4, the short version of the scale for Detecting Test Manipulation through Faking Good and Social Desirability Bias (SEA-K; [136]) is included in the self-report questionnaire.
Parental weight status
At T1–T3, parents were asked to report their height and weight to calculate their body mass index (BMI; [137]).
Statistical analyses
Before testing specific hypotheses, several methodological challenges have to be considered. Firstly, this concerns the age-appropriate operationalization of constructs while maintaining conceptual equivalence (e.g., adolescence-specific content adjustments or change of measures; the transition from parent- to self-report). Secondly, the concepts itself can change (e.g., the dimensional structure of SR becomes more complex with increasing age). To deal with these problems, we use multiple statistical approaches like confirmatory factor analysis for measurement invariance testing, developmental scaling, approximate invariance testing, or directly including the change of structure in the model.
Thirdly, methodological challenges arise from the integration of multiple indicators of the same construct due to the comprehensive multi-method and multi-rater assessment of the SR skills. The comprehensive and concurrent examinations of the SR-sub-facets (including self-report, proxy-report (parents, teachers), and behavioral data) will form the basis of the data-driven synthesis of the different assessment methods [138]. This way, latent factors of individual SR competencies with ratings from different sources can be identified. In addition, whenever possible, we will model method factors in latent analyses to account for rater effects. Fourthly, the inclusion of several related constructs may lead to multicollinearity between SR-sub-facets. We will address this problem via various established approaches. One is exploratory factor analyses to analyze the empirical relations between variables and to reduce the number of variables (Eisenberg et al. [138]). As another approach, we will apply a data-driven focus after testing for multicollinearity, in case no theoretical or evidence-based assumptions integrating the different sub-facets can be derived from the literature. Additionally, effect sizes provide information on the strength of the relations, which facilitates interpreting the clinical significance of the findings. Furthermore, we will conduct subgroup analyses (e.g., age; gender; pubertal status, see [139]) to make statements about the generalizability of the findings. For further hypotheses testing, we will apply different structural equation models (e.g., cross-lagged analyses, latent-growth modelling). If possible, the analyses will be performed at the latent level. School class membership will be accounted for when necessary and possible. The calculations will be carried out with SPSS, R, and Mplus.
Power analysis
Because the present study bases on existing prospective data, a power calculation can only examine whether the existing (N = 1657) and expected samples (N = 1074 for T4, N = 1020 for T5) are sufficient for the intended analyses. A Monte Carlo simulation supported the sufficient size of the expected sample by indicating that cross-lagged models from the first to the fourth assessment can meaningfully test effects with a strength of r = 0.09, and mediation models can test indirect effects with a strength of r = 0.01 and a power of 0.95. For latent-growth models, the power exceeds 0.99 for the identification of predictors for the slope with an effect size of 0.15 [140]).
Discussion
The PIERYOUTH-study is a prospective longitudinal study covering a period of 10 years and an age range from 6 to 20 years. The focus lies on the role of SR as a central resource for accomplishing different developmental tasks [1, 3]. The study enables to investigate the complex single and conjoint development of multiple SR skills from middle childhood to adolescence, thus including adolescence as a period that has not yet been sufficiently addressed in SR research [30] despite the numerous changes relevant to SR development (such as increasing autonomy or the development of more complex SR strategies). The study will also examine potential overlapping or differential prospective association patterns of single and conjoint SR skills with a broad range of outcome variables (e.g., prosocial behavior, delinquency, emotional problems, eating-related behaviors) that are highly relevant in this age range.
A particular strength of this study is the multi-method and multi-rater assessment of multiple SR sub-facets (e.g., delay of gratification, HRV, impulsivity, emotion regulation). Adoption of this multi-faceted battery facilitates complex data analyses on developmental trajectories of SR, other skills, or the interplay between SR sub-facets. Furthermore, the specific contribution of individual SR sub-facets to a broad range of adolescence-specific outcomes can be examined. This multifaceted assessment allows for not only examining developmental trajectories of SR and their influencing factors, but also the influence of SR on specific aspects (e.g., aggressiveness, delinquency) and their specific vs. generic relevance (i.e., whether the level and/or profile of SR sub-facets is predictive for different mental health problems). Consequently, implications for the development of theory-based and evidence-based, possibly outcome-specific SR interventions can be derived.
Some limitations also deserve attention: The PIERYOUTH study includes a sample with an above-average educated family background in the German federal state Brandenburg, which is not representative of all German children and adolescents in that age group. Additionally, the survey had to strike a balance between the time burden on participants and the desired breadth of constructs. Therefore, we decided to use short versions of established instruments whenever possible. These short versions are time-efficient but have the potential disadvantage of lower reliabilities. Performing statistical analyses at the latent level can reduce this problem. Of note, due to the COVID-19 pandemic with access restrictions for researchers (e.g., at schools), the larger part of assessments at T4 are conduct online—in contrast to the previous face-to-face tests at schools. However, this also facilitates the recruitment of eligible individuals who no longer live in the region. Due to the extensive training of the test administrators, a high level of data quality can be ensured.
To sum up, there has been an increased interest to address questions on the development and effects of SR in a developmental framework covering an age range from middle childhood to adolescence. Prospective data over a longer time span are essential to foster our understanding of the emergence and role of self-regulation for a positive youth development. The PIERYOUTH-study aims to contribute to our understanding of the complex interplay of different SR sub-facets and their influence on child and adolescent development.
Availability of data and materials
Data generated in the course of the study will be available from the corresponding author on reasonable request and after a moratorium of five years following the completion of the study.
Abbreviations
- ABCL:
-
Adult behavior checklist
- AEBQ:
-
Adult eating behavior questionnaire
- ASR:
-
Adult self-report
- BART:
-
Balloon analogue risk task
- BE:
-
Binge eating
- BFI-S:
-
Big five inventory-SOEP
- BIS:
-
Barratt impulsiveness scale
- BMI:
-
Body mass index
- BRIEF:
-
Behavior rating inventory of executive function
- CBCL:
-
Child behavior checklist
- CEBQ:
-
Children’s eating behavior questionnaire
- CERQ:
-
Cognitive emotion regulation questionnaire
- CHQ:
-
Child health questionnaire
- CSBS-T:
-
Children’s social behavior scale-teacher version
- DCCS:
-
Dimensional change card sorting task
- DDT:
-
German delay discounting test
- DEBQ:
-
Dutch eating behavior questionnaire for children
- DISYPS-KJ:
-
Diagnostik-system für psychische Störungen im Kindes-und Jugendalter; diagnostic system of mental disorders in children and adolescents
- DTGA:
-
Depressionstest für Kinder im Grundschulalter; depression test for children of elementary school age
- EDE-Q:
-
Eating disorder examination questionnaire
- EF:
-
Executive functions
- ERQ:
-
Emotion regulation questionnaire
- FAI:
-
Family adversity index
- FASD:
-
Fragebogen zum aussehensbezogenen druck; appearance-related social pressure questionnaire
- FEEL-KJ:
-
Fragebogen zur Erhebung der Emotionsregulation bei Kindern und Jugendlichen; questionnaire to elicit emotion regulation in children and adolescents
- FIML:
-
Full information maximum likelihood procedure
- GAD-7:
-
Generalized anxiety disorder assessment
- GDPR:
-
General data protection regulation
- HRV:
-
Heart rate variability
- IDS:
-
Intelligence and development scales
- IRPA:
-
Instrument for reactive and proactive aggression
- JSI-CA:
-
Justice sensitivity inventory for children and adolescents
- LOCES:
-
The loss of control over eating scale
- MJF:
-
Mannheimer Jugendlichen-Fragebogen; Mannheim adolescent questionnaire
- O:
-
Objective measures
- OPD-SQS:
-
Operationalised psychodynamic diagnostic-structural questionnaire short version
- P:
-
Parent-report
- PB:
-
Performance-based computer task
- PHQ-8:
-
Patient health questionnaire without item suicidality
- PHQ-9:
-
Patient health questionnaire
- PIER:
-
Potsdamer Internale Entwicklungs-Risiken; engl. Potsdam intrapersonal developmental risk study
- POTS:
-
Perception of teasing scale
- QEWP:
-
Questionnaire of eating and weight patterns
- S:
-
Self-report
- SATAQ‐IV-R:
-
Sociocultural attitudes towards appearance questionnaire-IV revised
- SDQ:
-
Strengths and difficulties questionnaire
- SEA-K:
-
Skala zur Erfassung von Testverfälschung durch positive Selbstdarstellung und sozial erwünschte Antworttendenzen; scale for detecting test manipulation through faking good and social desirability bias
- SES:
-
Socioeconomic status
- SIP:
-
Social information processing
- SPSS:
-
Statistical package for the social sciences
- SR:
-
Self-regulation
- SRS:
-
Self-regulation scale
- SSIPA:
-
Social information processing in adolescence
- T:
-
Teacher-report
- T1/T2/T3/T4:
-
First/second/third/fourth measurement point
- TMCQ:
-
Temperament in middle childhood questionnaire
- UPPS:
-
UPPS impulsive behavior scale with subscales urgency, premeditation, perseverance, sensation seeking, and positive urgency
- WAIS-IV:
-
Wechsler adult intelligence scale-fourth edition
- WBIS-C:
-
Weight bias internalization scale for children
- WISC-IV:
-
Wechsler intelligence scale for children-fourth edition
- YSR:
-
Youth self-report
- ZN-R:
-
Zahlen nachsprechen-rückwärts; German version of the digit span backwards subtest oft he WISC-IV
- ZST:
-
Zahlensymboltest; symbol digit modalities test (SDMT)
References
Nigg JT. Annual research review: on the relations among self-regulation, self-control, executive functioning, effortful control, cognitive control, impulsivity, risk-taking, and inhibition for developmental psychopathology. J Child Psychol Psychiatr. 2017;58:361–83. https://doi.org/10.1111/jcpp.12675.
Burman JT, Green CD, Shanker S. On the meanings of self-regulation: digital humanities in service of conceptual clarity. Child Dev. 2015;86:1507–21. https://doi.org/10.1111/cdev.12395.
McClelland MM, Geldhof GJ, Morrison F, Gestsdottir S, Cameron C, Bowers E, et al. Self-regulation. In: Halfon N, Forrest CB, Lerner RM, Faustman EM, editors., et al., Handbook of life course health development. Cham: CH; 2018. p. 275–98.
Bailey R, Jones SM. An integrated model of regulation for applied settings. Clin Child Fam Psychol Rev. 2019;22:2–23. https://doi.org/10.1007/s10567-019-00288-y.
Gettens KM, Gorin AA. Executive function in weight loss and weight loss maintenance: a conceptual review and novel neuropsychological model of weight control. J Behav Med. 2017;40:687–701. https://doi.org/10.1007/s10865-017-9831-5.
Miller AL, Lo SL, Bauer KW, Fredericks EM. Developmentally informed behaviour change techniques to enhance self-regulation in a health promotion context: a conceptual review. Health Psychol Rev. 2020;14:116–31. https://doi.org/10.1080/17437199.2020.1718530.
Goossens L. Adolescent development: putting Europe on the map. In: Jackson S, Goossens L, editors. Handbook of adolescent development. New York: Psychology Press; 2006. p. 1–10.
Friedman NP, Miyake A. Unity and diversity of executive functions: Individual differences as a window on cognitive structure. Cortex. 2017;86:186–204. https://doi.org/10.1016/j.cortex.2016.04.023.
Karr JE, Areshenkoff CN, Rast P, Hofer SM, Iverson GL, Garcia-Barrera MA. The unity and diversity of executive functions: a systematic review and re-analysis of latent variable studies. Psychol Bull. 2018;144:1147–85. https://doi.org/10.1037/bul0000160.
Steinberg L, Icenogle G, Shulman EP, Breiner K, Chein J, Bacchini D, et al. Around the world, adolescence is a time of heightened sensation seeking and immature self-regulation. Dev Sci. 2018;21:1–13. https://doi.org/10.1111/desc.12532.
Wang C, Hu Y, Weng J, Chen F, Liu H. Modular segregation of task-dependent brain networks contributes to the development of executive function in children. Neuroimage. 2020;206:116334. https://doi.org/10.1016/j.neuroimage.2019.116334.
Rutter M. Adolescence: biology, epidemiology, and process considerations. In: Oettingen G, Gollwitzer PM, editors. Self-regulation in adolescence. Cambridge: Cambridge University Press; 2015. p. 123–46.
Hauser MD. Patience! How to assess and strengthen self-control. Front Educ. 2019;4:25. https://doi.org/10.3389/feduc.2019.00025.
Bridgett DJ, Burt NM, Edwards ES, Deater-Deckard K. Intergenerational transmission of self-regulation: a multidisciplinary review and integrative conceptual framework. Psychol Bull. 2015;141:602–54. https://doi.org/10.1037/a0038662.
Blair C. The development of executive functions and self-regulation: a bidirectional psychobiological model. In: Vohs KD, Baumeister RF, editors. Handbook of self-regulation: research, theory, and applications. 3rd ed. New York: Guilford Press; 2016. p. 417–39.
Farley JP, Kim-Spoon J. The development of adolescent self-regulation: reviewing the role of parent, peer, friend, and romantic relationships. J Adolesc. 2014;37:433–40. https://doi.org/10.1016/j.adolescence.2014.03.009.
Denissen JJA, van Aken MAG, Penke L, Wood D. Self-regulation underlies temperament and personality: an integrative developmental framework. Child Dev Perspect. 2013;7:255–60. https://doi.org/10.1111/cdep.12050.
Sameroff A. The transactional model. In: Sameroff AJ, editor. The transactional model of development: how children and contexts shape each other. 1st ed. Washington, DC: American Psychological Association; 2009. p. 3–21.
Silvers JA. Adolescence as a pivotal period for emotion regulation development. Curr Opin Psychol. 2022;44:258–63. https://doi.org/10.1016/j.copsyc.2021.09.023.
Gestsdottir S, Lerner RM. Positive development in adolescence: the development and role of intentional self-regulation. Hum Dev. 2008;51:202–24. https://doi.org/10.1159/000135757.
Eisenberg N. Self-regulation: conceptual issues and relations to developmental outcomes in childhood and adolescence. In: Oettingen G, Gollwitzer PM, editors. Self-regulation in adolescence. Cambridge: Cambridge University Press; 2015. p. 57–77.
Oettingen G, Gollwitzer PM. Self-regulation: principles and tools. In: Oettingen G, Gollwitzer PM, editors. Self-regulation in adolescence. Cambridge: Cambridge University Press; 2015. p. 3–29.
Steinberg L. The neural underpinnings of adolescent risk-taking: the roles of reward-seeking, impulse-control, and peers. In: Oettingen G, Gollwitzer PM, editors. Self-regulation in adolescence. Cambridge: Cambridge University Press; 2015. p. 3–29.
McClelland MM, Geldhof GJ, Cameron CE, Wanless SB. Development and self-regulation. In: Lerner RM, editor. Handbook of child psychology and developmental science. 7th ed. Hoboken, NJ: John Wiley & Sons; 2015. p. 1–43.
Atherton OE. Typical and atypical self-regulation in adolescence: the importance of studying change over time. Social Pers Psych Compass. 2020;14:155. https://doi.org/10.1111/spc3.12514.
de Ridder DTD, Lensvelt-Mulders G, Finkenauer C, Stok FM, Baumeister RF. Taking stock of self-control: a meta-analysis of how trait self-control relates to a wide range of behaviors. Pers Soc Psychol Rev. 2012;16:76–99. https://doi.org/10.1177/1088868311418749.
Gestsdottir S, Geldhof GJ, Lerner JV, Lerner RM. What drives positive youth development? Assessing intentional self-regulation as a central adolescent asset. Int J Dev Sci. 2017;11:69–79. https://doi.org/10.3233/DEV-160207.
Howard SJ, Williams KE. Early self-regulation, early self-regulatory change, and their longitudinal relations to adolescents’ academic, health, and mental well-being outcomes. J Dev Behav Pediatr. 2018;39:489–96. https://doi.org/10.1097/DBP.0000000000000578.
De Ridder D, Adriaanse M, Fujita K. Self-control in health and well-being. Concepts, theories, and central issues. In: De Ridder D, Adriaanse M, Fujita K, editors. The Routledge international handbook of self-control in health and well-being. London: Routledge; 2018. p. 1–7.
Robson DA, Allen MS, Howard SJ. Self-regulation in childhood as a predictor of future outcomes: a meta-analytic review. Psychol Bull. 2020;146:324–54. https://doi.org/10.1037/bul0000227.
Vohs KD, Baumeister RF. Understanding self-regulation. An introduction. In: Vohs KD, Baumeister RF, editors. Handbook of self-regulation: research, theory, and applications. New York: Guilford Press; 2004. p. 1–9.
Baumeister RF, Vohs KD. Strength model of self-regulation as limited resource. In: Olson JM, Zanna MP, editors. Advances in experimental social psychology. Amsterdam: Elsevier; 2016. p. 67–127. https://doi.org/10.1016/bs.aesp.2016.04.001.
Poulton R, Moffitt TE, Silva PA. The Dunedin multidisciplinary health and development study: overview of the first 40 years, with an eye to the future. Soc Psychiatr Psychiatr Epidemiol. 2015;50:679–93. https://doi.org/10.1007/s00127-015-1048-8.
Deutz MHF, Shi Q, Vossen HGM, Huijding J, Prinzie P, Deković M, et al. Evaluation of the strengths and difficulties questionnaire-dysregulation profile (SDQ-DP). Psychol Assess. 2018;30:1174–85. https://doi.org/10.1037/pas0000564.
Deutz MHF, Vossen HGM, de Haan AD, Deković M, van Baar AL, Prinzie P. Normative development of the child behavior checklist dysregulation profile from early childhood to adolescence: associations with personality pathology. Dev Psychopathol. 2018;30:437–47. https://doi.org/10.1017/S0954579417000955.
Haltigan JD, Aitken M, Skilling T, Henderson J, Hawke L, Battaglia M, et al. “P” and “DP:” Examining symptom-level bifactor models of psychopathology and dysregulation in clinically referred children and adolescents. J Am Acad Child Adolesc Psychiatr. 2018;57:384–96. https://doi.org/10.1016/j.jaac.2018.03.010.
Moffitt TE, Arseneault L, Belsky D, Dickson N, Hancox RJ, Harrington H, et al. A gradient of childhood self-control predicts health, wealth, and public safety. Proc Natl Acad Sci U S A. 2011;108:2693–8. https://doi.org/10.1073/pnas.1010076108.
Buitelaar JK. Adolescence as a turning point: for better and worse. Eur Child Adolesc Psychiatr. 2012;21:357–9. https://doi.org/10.1007/s00787-012-0296-3.
Rapee RM, Oar EL, Johnco CJ, Forbes MK, Fardouly J, Magson NR, Richardson CE. Adolescent development and risk for the onset of social-emotional disorders: a review and conceptual model. Behav Res Ther. 2019;123:103501. https://doi.org/10.1016/j.brat.2019.103501.
Angold A, Costello EJ, Erkanli A. Comorbidity. J Child Psychol Psychiatr. 1999;40:57–87. https://doi.org/10.1111/1469-7610.00424.
Ravens-Sieberer U, Otto C, Kriston L, Rothenberger A, Döpfner M, Herpertz-Dahlmann B, et al. The longitudinal BELLA study: design, methods and first results on the course of mental health problems. Eur Child Adolesc Psychiatr. 2015;24:651–63. https://doi.org/10.1007/s00787-014-0638-4.
Sayegh CS, Huey SJ, Barnett E, Spruijt-Metz D. Motivational Interviewing to prevent dropout from an education and employment program for young adults: a randomized controlled trial. J Adolesc. 2017;58:1–11. https://doi.org/10.1016/j.adolescence.2017.04.004.
Simonds J, Kieras JE, Rueda MR, Rothbart MK. Effortful control, executive attention, and emotional regulation in 7–10-year-old children. Cogn Dev. 2007;22:474–88. https://doi.org/10.1016/j.cogdev.2007.08.009.
Roebers CM, Röthlisberger M, Cimeli P, Michel E, Neuenschwander R. School enrolment and executive functioning: a longitudinal perspective on developmental changes, the influence of learning context, and the prediction of pre-academic skills. Eur J Dev Psychol. 2011;8:526–40. https://doi.org/10.1080/17405629.2011.571841.
Archibald SJ, Kerns KA. Identification and description of new tests of executive functioning in children. Child Neuropsychol. 1999;5:115–29. https://doi.org/10.1076/chin.5.2.115.3167.
Friedman NP, Miyake A, Altamirano LJ, Corley RP, Young SE, Rhea SA, Hewitt JK. Stability and change in executive function abilities from late adolescence to early adulthood: a longitudinal twin study. Dev Psychol. 2016;52:326–40. https://doi.org/10.1037/dev0000075.
Petermann F, Petermann U. Hamburg-Wechsler-Intelligenztest für Kinder IV (HAWIK-IV). [Hamburg-Wechsler-Intelligence-Scale for Children IV (HAWIK-IV)]. Bern: Huber; 2008.
Petermann F. Wechsler Adult Intelligence Scale-(WAIS-IV): Manual zur Durchführung und Auswertung; deutsche Übersetzung und Adaptation der WAIS-IV von David Drechsler. [Manual for implementation and evaluation; German translation and adaptation of the WAIS-IV]. Frankfurt: Pearson; 2012.
Roebers CM, Kauer M. Motor and cognitive control in a normative sample of 7-year-olds. Dev Sci. 2009;12:175–81. https://doi.org/10.1111/j.1467-7687.2008.00755.x.
Qu L, Low JJW, Chong PS, Lim DWL, Keren-Happuch, FFE. Task switching in English-Chinese bilinguals: A life span approach. In: Kashima Y, Kashima ES & Beatson R, editors. Steering the cultural dynamics: Selected papers from the 2010 Congress of the International Association for Cross-Cultural Psychology; 2013. p. 76–84.
Holzman JB, Bridgett DJ. Heart rate variability indices as bio-markers of top-down self-regulatory mechanisms: a meta-analytic review. Neurosci Biobehav Rev. 2017;74:233–55. https://doi.org/10.1016/j.neubiorev.2016.12.032.
Zahn D, Adams J, Krohn J, Wenzel M, Mann CG, Gomille LK, et al. Heart rate variability and self-control: a meta-analysis. Biol Psychol. 2016;115:9–26. https://doi.org/10.1016/j.biopsycho.2015.12.007.
Koch A, Pollatos O. Cardiac sensitivity in children: sex differences and its relationship to parameters of emotional processing. Psychophysiology. 2014;51:932–41. https://doi.org/10.1111/psyp.12233.
Appelhans BM, Luecken LJ. Heart rate variability as an index of regulated emotional responding. Rev Gen Psychol. 2006;10:229–40. https://doi.org/10.1037/1089-2680.10.3.229.
Gioia GA, Isquith PK, Guy SC, Kenworthy L. Behavior rating inventory of executive function. Child Neuropsychol. 2000;6:235–8. https://doi.org/10.1076/chin.6.3.235.3152.
Herzberg PY. Faktorstruktur, Gütekriterien und Konstruktvalidität der deutschen Übersetzung des Aggressionsfragebogens von Buss und Perry. [Factor structure, quality criteria, and construct validity of the German translation of the Buss and Perry Aggression Questionnaire]. ZDDP. 2003;24:311–23. https://doi.org/10.1024/0170-1789.24.4.311.
Grob A, Smolenski C. FEEL-KJ: manual und Fragebogen zur Erhebung der Emotionsregulation bei Kindern und Jugendlichen. [FEEL-KJ: Manual and questionnaire for the assessment of emotion regulation in children and adolescents]. Bern: Huber; 2005.
Grob A, Meyer CS, Hagmann-von AP. IDS: Intelligence and Development Scales: Intelligenz-und Entwicklungsskalen für Kinder von 5–10 Jahren. [IDS: Intelligence and Development Scales: intelligence and development scales for children 5–10 years old]. Bern: Huber; 2009.
Abler B, Kessler H. Emotion regulation questionnaire—Eine deutschsprachige Fassung des ERQ von Gross und John. [Emotion regulation questionnaire: a German language version of the ERQ by Gross and John]. Diagnostica. 2009;55:144–52. https://doi.org/10.1026/0012-1924.55.3.144.
Loch N, Hiller W, Witthöft M. Der cognitive emotion regulation questionnaire (CERQ). ZPPP. 2011;40:94–106. https://doi.org/10.1026/1616-3443/a000079.
Crone EA, Bunge SA, Latenstein H, van der Molen MW. Characterization of children’s decision making: sensitivity to punishment frequency, not task complexity. Child Neuropsychol. 2005;11:245–63. https://doi.org/10.1080/092970490911261.
Crone EA, van der Molen MW. Developmental changes in real life decision making: performance on a gambling task previously shown to depend on the ventromedial prefrontal cortex. Dev Neuropsychol. 2004;25:251–79. https://doi.org/10.1207/s15326942dn2503_2.
Wulfert E, Block JA, Santa Ana E, Rodriguez ML, Colsman M. Delay of gratification: impulsive choices and problem behaviors in early and late adolescence. J Pers. 2002;70:533–52. https://doi.org/10.1111/1467-6494.05013.
Forstmeier S, Maercker A. Selbstkontrolle im höheren Erwachsenenalter: Eine deutsche Version des Delay Discounting Tests von Kirby. [Self-control in older adulthood: a German version of the delay discounting test by Kirby]. Psychother Psychosom Med Psychol. 2011;61:e19-33. https://doi.org/10.1055/s-0031-1277169.
Göllner LM, Ballhausen N, Kliegel M, Forstmeier S. Delay of gratification, delay discounting and their associations with age, episodic future thinking, and future time perspective. Front Psychol. 2018;8:2304. https://doi.org/10.3389/fpsyg.2017.02304.
Kovaleva A, Beierlein C, Kemper CJ, Rammstedt B. Eine Kurzskala zur Messung von Impulsivität nach dem UPPS-Ansatz: Die Skala Impulsives-Verhalten-8 (I-8). [A short scale for measuring impulsivity according to the UPPS approach: the impulsive behavior-8 scale (I-8)]. Köln: GESIS; 2012.
Partsch MV, Danner D. Measuring self-control in international large-scale surveys. Eur J Psychol Assess. 2021;37:409–18. https://doi.org/10.1027/1015-5759/a000618.
Schwarzer R. Selbstregulation (REG). [Self-regulation (REG)]. In: Schwarzer R, Jerusalem M, editors. Skalen zur Erfassung von Lehrer-und Schülermerkmalen. Dokumentation der psychometrischen Verfahren im Rahmen der wissenschaftlichen Begleitung des Modellversuchs Selbstwirksame Schulen. Berlin: Freie Universität Berlin; 1999. p. 92–3.
Lejuez CW, Read JP, Kahler CW, Richards JB, Ramsey SE, Stuart GL, et al. Evaluation of a behavioral measure of risk taking: the balloon analogue risk task (BART). J Exp Psychol Appl. 2002;8:75–84. https://doi.org/10.1037/1076-898x.8.2.75.
Meule A, Vögele C, Kübler A. Psychometrische evaluation der deutschen Barratt Impulsiveness Scale—Kurzversion (BIS-15). [Psychometric evaluation of the German Barratt Impulsiveness Scale—Short Version (BIS-15)]. Diagnostica. 2011;57:126–33. https://doi.org/10.1026/0012-1924/a000042.
Hampson SE, Edmonds GW, Barckley M, Goldberg LR, Dubanoski JP, Hillier TA. A big five approach to self-regulation: personality traits and health trajectories in the Hawaii longitudinal study of personality and health. Psychol Health Med. 2016;21:152–62. https://doi.org/10.1080/13548506.2015.1061676.
Schupp J, Gerlitz J-Y. Big Five Inventory-SEOP (BFI-S): Zusammenstellung sozialwissenschaftlicher Items und Skalen (ZIS). [BIG Five Inventory-SOEP (BFI-S). Compilation of social science items and scales (CIS)]: ZIS-GESIS Leibniz Institute for the Social Sciences; 2008.
Wardle J, Gutherie CA, Sanderson S, Rapoport L. Development of the children’s eating behaviour questionnaire. J Child Psychol Psychiatr. 2001;42:963–70. https://doi.org/10.1111/1469-7610.00792.
Franzen F. Der Dutch Eating Behavior Questionnaire für Kinder (DEBQ-K)—Ein Fragebogen zur Erfassung gezügelten Essverhaltens [The Dutch eating behavior questionnaire for children (DEBQ-K)-a questionnaire to assess restrained eating behavior]. Kindheit und Entwicklung. 1997;6:116–22.
Warschburger P, Petermann F. Adipositas. Göttingen: Hogrefe; 2007.
Hunot C, Fildes A, Croker H, Llewellyn CH, Wardle J, Beeken RJ. Appetitive traits and relationships with BMI in adults: development of the adult eating behaviour questionnaire. Appetite. 2016;105:356–63. https://doi.org/10.1016/j.appet.2016.05.024.
Hunot-Alexander C, Beeken RJ, Goodman W, Fildes A, Croker H, Llewellyn C, Steinsbekk S. Confirmation of the factor structure and reliability of the ‘adult eating behavior questionnaire’ in an adolescent sample. Front Psychol. 2019;10:1991. https://doi.org/10.3389/fpsyg.2019.01991.
Nagl M, Hilbert A, de Zwaan M, Braehler E, Kersting A. The German version of the Dutch eating behavior questionnaire: psychometric properties, measurement invariance, and population-based norms. PLoS ONE. 2016;11:e0162510. https://doi.org/10.1371/journal.pone.0162510.
Collins ME. Body figure perceptions and preferences among preadolescent children. Int J Eat Disord. 1991;10:199–208. https://doi.org/10.1002/1098-108X(199103)10:2%3c199::AID-EAT2260100209%3e3.0.CO;2-D.
Zitzmann J, Warschburger P. Psychometric properties of figure rating scales in children: the impact of figure ordering. J Pers Assess. 2020;102:259–68. https://doi.org/10.1080/00223891.2018.1505731.
Thompson MA, Gray JJ. Development and validation of a new body-image assessment scale. J Pers Assess. 1995;64:258–69. https://doi.org/10.1207/s15327752jpa6402_6.
Lynch SM, Zellner DA. Figure preferences in two generations of men: the use of figure drawings illustrating differences in muscle mass. Sex Roles. 1999;40:833–43. https://doi.org/10.1023/A:1018868904239.
Mohnke S, Warschburger P. Körperunzufriedenheit bei weiblichen und männlichen Jugendlichen: Eine geschlechtervergleichende Betrachtung von Verbreitung, Prädiktoren und Folgen. [Body dissatisfaction among female and male adolescents: comparing prevalence, predictors, and consequences between the sexes]. Prax Kinderpsychol Kinderpsychiatr. 2011;60:285–303. https://doi.org/10.13109/prkk.2011.60.4.285.
Zuba A, Warschburger P. Weight bias internalization across weight categories among school-aged children. Validation of the weight bias internalization scale for children. Body Image. 2018;25:56–65. https://doi.org/10.1016/j.bodyim.2018.02.008.
Thompson JK, Cattarin J, Fowler B, Fisher E. The perception of teasing scale (POTS): a revision and extension of the physical appearance related teasing scale (PARTS). J Pers Assess. 1995;65:146–57. https://doi.org/10.1207/s15327752jpa6501_11.
Helfert S, Warschburger P. Fragebogen zum aussehensbezogenen sozialen Druck [Questionnaire on appearance-related social pressure]. Klinische Diagnostik und Evaluation. 2009;3:207–21.
Ravens-Sieberer U. Der KINDL-R Fragebogen zur Erfassung der gesundheitsbezogenen Lebensqualität bei Kindern und Jugendlichen—Revidierte form. [The KINDL-R Questionnaire for the assessment of health-related quality of life in children and adolescents-revised form]. In: Schumacher J, Klaiberg A, Brähler E, editors. Diagnostische Verfahren zu Lebensqualität und Wohlbefinden. Göttingen: Hogrefe; 2003. p. 184–8.
Landgraf JM, Maunsell E, Speechley KN, Bullinger M, Campbell S, Abetz L, Ware JE. Canadian-French, German and UK versions of the Child Health Questionnaire: methodology and preliminary item scaling results. Qual Life Res. 1998;7:433–45. https://doi.org/10.1023/A:1008810004694.
Warschburger P, Landgraf JM, Petermann F, Freidel K. Health-related quality of life in children assessed by their parents: evaluation of the psychometric properties of the CHQ-PF50 in two German clinical samples. Qual Life Res. 2003;12:291–301. https://doi.org/10.1023/A:1023233308653.
Thönnissen C, Wilhelm B, Alt P, Fiedrich S, Walper S. Parfaim scales and instruments manual, release 12.0. Köln: GESIS Data Archive; 2021.
Goodman R. Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry. 2001;40:1337–45. https://doi.org/10.1097/00004583-200111000-00015.
Woerner W, Becker A, Friedrich C, Klasen H, Goodman R, Rothenberger A. Normierung und Evaluation der deutschen Elternversion des Strengths and Difficulties Questionnaire (SDQ): Ergebnisse einer repräsentativen Felderhebung. [Normative data and evaluation of the German parent-rated Strengths and Difficulties Questionnaire (SDQ): Results of a representative field study]. Z Kinder Jugendpsychiatr Psychother. 2002;30:105–12. https://doi.org/10.1024//1422-4917.30.2.105.
Baumert A, Schlösser T, Schmitt M. Economic games. A performance-based assessment of fairness and altruism. Eur J Psychol Assess. 2014. https://doi.org/10.1027/1015-5759/a000183.
Fetchenhauer D, Huang X. Justice sensitivity and distributive decisions in experimental games. Pers Individ Dif. 2004;36:1015–29. https://doi.org/10.1016/S0191-8869(03)00197-1.
Ritgens C, Bondü R. Everyday prosocial behavior scale. Psychologische Hochschule Berlin; unpublished.
Hardy SA, Walker LJ, Olsen JA, Woodbury RD, Hickman JR. Moral identity as moral ideal self: links to adolescent outcomes. Dev Psychol. 2014;50:45–57. https://doi.org/10.1037/a0033598.
Arnold ML. The place of morality in the adolescent self. Diss Abstr Int Sect B Sci Eng. 1994;54:5407.
Blasi A. Moral cognition and moral action: a theoretical perspective. Dev Rev. 1983;3:178–210. https://doi.org/10.1016/0273-2297(83)90029-1.
Bondü R, Elsner B. Justice sensitivity in childhood and adolescence. Soc Dev. 2015;24:420–41. https://doi.org/10.1111/sode.12098.
Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: a new screening tool for eating disorders. West J Med. 2000;172:164–5. https://doi.org/10.1136/bmj.319.7223.1467.
Johnson WG, Grieve FG, Adams CD, Sandy J. Measuring binge eating in adolescents: adolescent and parent versions of the questionnaire of eating and weight patterns. Int J Eat Disord. 1999;26:301–14. https://doi.org/10.1002/(SICI)1098-108X(199911)26:3%3c301::AID-EAT8%3e3.0.CO;2-M.
Warschburger P, Kröller K. Adipositas im Kindes-und Jugendalter: Was sind Risikofaktoren für die Entstehung einer Binge Eating Disorder? [Obesity in childhood and adolescence: What are the risk factors for the development of a Binge Eating Disorder?]. 2005;13:69–78. https://doi.org/10.1026/0943-8149.13.2.69.
Hilbert A, Tuschen-Caffier B. Eating disorder examination-questionnaire: Deutschsprachige Übersetzung [Eating disorder examination-questionnaire: German translation]. 2nd ed. Tübingen: Dgvt Verlag; 2016.
Latner JD, Mond JM, Kelly MC, Haynes SN, Hay PJ. The loss of control over eating scale: development and psychometric evaluation. Int J Eat Disord. 2014;47:647–59. https://doi.org/10.1002/eat.22296.
Peitz D, Schulze J, Warschburger P. Getting a deeper understanding of mindfulness in the context of eating behavior: development and validation of the mindful eating inventory. Appetite. 2021;159:105039. https://doi.org/10.1016/j.appet.2020.105039.
Döpfner M, Lehmkuhl G. DISYPS-KJ: Diagnostik-System für psychische Störungen im Kindes-und Jugendalter nach ICD-10 und DSM-IV. [DISYPS-KJ: Diagnostic system for mental disorders in childhood and adolescence]. Bern: Hans Huber; 2000.
Esser G, Laucht M, Drews S, Ihle WDTGA. Depressionstest für Kinder im Grundschulalter. [DTGA Depression test for children of primary school age]. Göttingen: Hogrefe; 2013.
Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. 2002;32:509–15. https://doi.org/10.3928/0048-5713-20020901-06.
Löwe B, Spitzer RL, Zipfel S, Herzog W. PHQ-D: Gesundheitsfragebogen für Patienten: Manual Komplettversion und Kurzform. [PHQ-D: Patient Health Questionnaire: Manual Complete Version and Short Form]. 2nd ed. Karlsruhe: Pfizer; 2002.
Esser G. Mannheimer Jugendlichenfragebogen MJF für 12-16-Jährige [Mannheim Youth Questionnaire MJF for 12–16 year olds]. In: BVKJ, editor. Gesundheitscheckheft des BVKJ. Köln: BVKJ; 2006. p. 19–20.
Thurner F, Tewes U. Der Kinder-Angst-Test II (KAT II): Drei Fragebögen zur Erfassung der Ängstlichkeit und von Zustandsängsten bei Kindern ab 9 Jahren. [The Child Anxiety Test II (KAT II): Three questionnaires to assess anxiety and state fears in children aged 9 years and older.]. Göttingen: Hogrefe; 2000.
Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092–7. https://doi.org/10.1001/archinte.166.10.1092.
Vagos P, Rijo D, Santos IM. Scenes for social information processing in adolescence: item and factor analytic procedures for psychometric appraisal. Psychol Assess. 2016;28:416–28. https://doi.org/10.1037/pas0000194.
Döpfner M, Plück J, Kinnen C. Manual deutsche Schulalter-Formen der Child Behavior Checklist von Thomas M. Achenbach: Elternfragebogen über das Verhalten von Kindern und Jugendlichen, (CBCL/6-18R), Lehrerfragebogen über das Verhalten von Kindern und Jugendlichen (TRF/6-18R), Fragebogen für Jugendliche (YSR/11-18R). [Manual German school-age forms of the Child Behavior Checklist by Thomas M. Achenbach: Parent Questionnaire on Child and Adolescent Behavior, (CBCL/6-18R), Teacher Questionnaire on Child and Adolescent Behavior (TRF/6-18R), Adolescent Questionnaire (YSR/11-18R).]. Göttingen: Hogrefe; 2014.
Achenbach TM. The child behavior checklist and related instruments. In: Maruish ME, editor. The use of psychological testing for treatment planning and outcomes assessment. 2nd ed. Hillsdale New Jersey: Lawrence Erlbaum Associates Publishers; 1999. p. 429–66.
Achenbach TM, Rescorla LA. Manual for the ASEBA Adult Forms & Profiles. Fragebögen zur Erfassung psychischer Probleme bei Erwachsenen. Deutschsprachige Fassungen des Adult Self-Report for Ages 18–59 und der Adult Behavior Checklist for Ages 18–59. [Manual for the ASEBA adult forms & profiles. Questionnaires to assess mental health problems in adults. German-language versions of the Adult Self-Report for Ages 18–59 and the Adult Behavior Checklist for Ages 18–59.]. 1st ed. Burlington, VT: University of Vermont, Research Center for Children; 2014.
Achenbach TM, Rescorla LA. Manual for the ASEBA adult forms & profiles: an integrated system of multi-informant assessment. Burlington, VT: University of Vermont, Research center for children, youth & families; 2001.
Achenbach TM, Rescorla LA. Manual for the ASEBA school-age forms & profiles: child behavior checklist for ages 6–18, Teacher’s Report Form, Youth Self-Report. Burlington, VT: ASEBA; 2001.
Crick NR. The role of overt aggression, relational aggression, and prosocial behavior in the prediction of children’s future social adjustment. Child Dev. 1996;67:2317–27. https://doi.org/10.1111/j.1467-8624.1996.tb01859.x.
Polman J. Hot-headed or cold-blooded? Towards a clear distinction between reactive and proactive aggression in youth. Niederlande: Prins Partners Ipskamp; 2008.
Euteneuer F, Süssenbach P, Schäfer SJ, Rief W. Subjektiver sozialer Status. MacArthur-Skalen zur Erfassung des wahrgenommenen sozialen Status im sozialen Umfeld (SSS-U) und in Deutschland (SSS-D). [Subjective social status. MacArthur Scales for the Assessment of Perceived Social Status in the Social Environment (SSS-U) and in Germany (SSS-D)]. Verhaltenstherapie. 2015;25:229–32. https://doi.org/10.1159/000371558.
Winkler J, Stolzenberg H. Der Sozialschichtindex im Bundes-Gesundheitssurvey. Das Gesundheitswesen. 1999;61:178–83.
Sebastian CL, Fontaine NMG, Bird G, Blakemore S-J, de Brito SA, McCrory EJP, Viding E. Neural processing associated with cognitive and affective theory of mind in adolescents and adults. Soc Cogn Affect Neurosci. 2012;7:53–63. https://doi.org/10.1093/scan/nsr023.
Apperly IA, Warren F, Andrews BJ, Grant J, Todd S. Developmental continuity in theory of mind: speed and accuracy of belief-desire reasoning in children and adults. Child Dev. 2011;82:1691–703. https://doi.org/10.1111/j.1467-8624.2011.01635.x.
Vetter NC, Weigelt S, Döhnel K, Smolka MN, Kliegel M. Ongoing neural development of affective theory of mind in adolescence. Soc Cogn Affect Neurosci. 2014;9:1022–9. https://doi.org/10.1093/scan/nst081.
Voll R, Allehoff W. Widrige familiäre und soziale Bedingungen und psychiatrische Auffälligkeiten bei Achtjährigen [Adverse family and social conditions and psychiatric abnormalities in eight-year-olds]. Z Kinder Jugendpsychiatr Psychother. 1982;10:100–9.
Riad A, Drobov A, Krobot M, Antalová N, Alkasaby MA, Peřina A, Koščík M. Mental health burden of the Russian-Ukrainian war 2022 (RUW-22): Anxiety and depression levels among young adults in Central Europe. Int J Environ Res Public Health. 2022;19:8418. https://doi.org/10.3390/ijerph19148418.
Stavridou A, Stergiopoulou A-A, Panagouli E, Mesiris G, Thirios A, Mougiakos T, et al. Psychosocial consequences of COVID-19 in children, adolescents and young adults: a systematic review. Psychiatr Clin Neurosci. 2020;74:615–6. https://doi.org/10.1111/pcn.13134.
Ehrenthal JC, Dinger U, Schauenburg H, Horsch L, Dahlbender RW, Gierk B. Entwicklung einer Zwölf-Item-Version des OPD-Strukturfragebogens (OPD-SFK). [Development of a 12-item version of the OPD-Structure Questionnaire (OPD-SQS)]. Z Psychosom Med Psychother. 2015;61:262–74. https://doi.org/10.13109/zptm.2015.61.3.262.
Lampert T, Sygusch R, Schlack R. Nutzung elektronischer Medien im Jugendalter. Ergebnisse des Kinder-und Jugendgesundheitssurveys (KiGGS). [Use of electronic media in adolescence. Results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS)]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2007;50:643–52. https://doi.org/10.1007/s00103-007-0225-7.
Hölling H, Schlack R, Kamtsiuris P, Butschalowsky H, Schlaud M, Kurth BM. Die KiGGS-Studie. Bundesweit repräsentative Längs-und Querschnittstudie zur Gesundheit von Kindern und Jugendlichen im Rahmen des Gesundheitsmonitorings am Robert Koch-Institut. [The KiGGS study. Nationwide representative longitudinal and cross-sectional study on the health of children and adolescents within the framework of health monitoring at the Robert Koch Institute]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2012;55:836–42. https://doi.org/10.1007/s00103-012-1486-3.
Frison E, Eggermont S. Exploring the relationships between different types of facebook use, perceived online social support, and adolescents’ depressed mood. Soc Sci Comput Rev. 2016;34:153–71. https://doi.org/10.1177/0894439314567449.
Schaefer LM, Harriger JA, Heinberg LJ, Soderberg T, Thompson JK. Development and validation of the sociocultural attitudes towards appearance questionnaire-4-revised (SATAQ-4R). Int J Eat Disord. 2017;50:104–17. https://doi.org/10.1002/eat.22590.
Hoffmann S, Warschburger P. SATAQ-4R Deutsche Version. University of Potsdam; unpublished.
Esser, G., Kohn, J. & Wyschkon, A. Potsdamer Lehrerfragebogen (PLF). University of Potsdam; 2005, unpublished.
Satow L. Skala zur Erfassung von Testverfälschung durch positive Selbstdarstellung und sozial erwünschte Antworttendenzen (SEA). [Scale to detect test bias due to positive self-representation and socially desirable response tendencies (SEA)]: ZPID (Leibniz Institute for Psychology Information); 2012.
World Health Organization (WHO). Obesity-preventing and managing the global epidemic: report on a WHO consultation. Geneva: World Health Organization; 2000.
Eisenberg IW, Bissett PG, Zeynep Enkavi A, Li J, MacKinnon DP, Marsch LA, Poldrack RA. Uncovering the structure of self-regulation through data-driven ontology discovery. Nat Commun. 2019;10:2319. https://doi.org/10.1038/s41467-019-10301-1.
Campbell J, Ehlert U. Acute psychosocial stress: Does the emotional stress response correspond with physiological responses? Psychoneuroendocrinology. 2012;37:1111–34. https://doi.org/10.1016/j.psyneuen.2011.12.010.
Muthén LK, Muthén BO. How to use a Monte Carlo study to decide on sample size and determine power. Struct Equ Modeling. 2002;9:599–620. https://doi.org/10.1207/S15328007SEM0904_8.
Acknowledgements
We would like to thank all participating children and adolescents, parents, teachers, and schools of the PIER-study for their support. In addition, special thanks to all the PhD students and postdoc researchers as well as the student experimenters of the former and the current assessments, and to Theresa Zickert for her support in compiling the relevant information for the study protocol.
Funding
Open Access funding enabled and organized by Projekt DEAL. The PIERYOUTH-study is funded by the German Research Foundation (DFG) as a research group (FOR 5034; 426314138) including the realization of the data collection and the coordination (WA 1143/16-1; 17-1) and six individual projects (BO 4482/5-1; 6-1; EL 253/10-1; KL 2338/2-1; WA 1143/15-17/1; RB 3253/1-1). The first three measurement points (T1–T3) were also funded by the DFG as part of the research training group GRK 1668. Publication of the study protocol was funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – Projektnummer 491466077.
Author information
Authors and Affiliations
Contributions
RBO, BE, AMK, RB and PW designed the study. PW and MSG drafted the manuscript, all authors reviewed and contributed to the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study will be conducted in accordance with the principles of Good Clinical Practice, the Declaration of Helsinki (https://www.wma.net/wpcontent/uploads/2016/11/DoH-Oct2008.pdf), and current ethical standards. Written informed consent is obtained from each participant. Depending on the age of the participant, informed consent from the legal representative or guardian will also be required. The ethical approval of the Ethics Committee of Potsdam University was obtained (request numbers 2/2010, 28-33/2011, 3-10/2012, 21/2012, 32/2014, 18/2020, 10/2022 and 37/2022).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Warschburger, P., Gmeiner, M.S., Bondü, R. et al. Self-regulation as a resource for coping with developmental challenges during middle childhood and adolescence: the prospective longitudinal PIERYOUTH-study. BMC Psychol 11, 97 (2023). https://doi.org/10.1186/s40359-023-01140-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-023-01140-3