
Abstract
Background
Few studies have investigated factors associated with anxiety and depression among patients with erectile dysfunction (ED). This study aimed to investigate associated factors and the prevalence of anxiety and depression in this special group in China.
Methods
Data from 511 patients with ED aged 18–60 years were collected between July 2021 and April 2022. The 5-item International Index of Erectile Function (IIEF-5) questionnaire, self-rating anxiety scale (SAS) and self-rating depression scale (SDS) were used to evaluate erectile function, anxiety and depression, respectively. Univariate analysis and multivariate linear regression analyses were used to explore the associated factors of depression and anxiety.
Results
The prevalence of anxiety and depression among ED patients was 38.16% and 64.97%, respectively. The mean anxiety index score was 47.37 ± 6.69 points, and the mean depression index was 54.72 ± 9.10 points. Multiple linear regression analysis showed that worse ED, low education level, and smoking were positively associated with increased risk of anxiety and depression. In addition, younger age, longer onset time, and irregular sleep were positively associated with high risk of anxiety, and irregular exercise was associated with severe depression.
Conclusions
The prevalence of depression and anxiety in ED patients is high, and the severity of ED, age, education level, smoking, onset time, regular sleep, and exercise were associated with anxiety or depression. Reversible risk factors should be avoided and individualized psychological support services are necessary for ED patients.
Similar content being viewed by others


Introduction
Erectile dysfunction (ED) is defined as the inability to achieve and maintain sufficient erection to allow for satisfactory sexual performance [1]. Epidemiological data have shown that ED is highly prevalence worldwide and is currently one of the most common sexual dysfunctions in men [2]. A previous study showed that the prevalence of ED varied from 37.2 to 48.6% in eight high burden countries [3]. In New Zealand, it was found that nearly a third of men aged 40–70 had ED but only 16% of them received a medical diagnosis and 22% are treated [4]. ED is described as a disrupted bio-psycho-social process involving the psychological, endocrine, vascular and nervous systems [5], which can significantly affect an individual's psychological well-being [6]. This suggests that the mental health of ED patients should be investigated and closely monitored.
Psychiatric disorder is strongly associated with erectile dysfunction, and their relationship seems to be bidirectional but not thoroughly studied [7,8,9]. A meta-analysis showed that depression increases the risk of ED and that ED also increases the risk of depression [10]. Sexual failure can lead to anxiety, increased fear, loss of confidence in sex, and lead to avoidance of sex, ultimately increasing the likelihood of future failure and creating a vicious circle [11]. A study in Greek found that 63.1% of ED patients had detectable mental illness, including 25.2% of depression [12]. They also found a positive correlation between the severity of depressive symptoms and the tendency of patients to discuss sex, but no significant correlation with the severity and duration of ED. Understanding the factors influencing the psychological response of ED patients can help identify high-risk groups of psychological disorders and formulate early individualized interventions.
Although some clinical studies have investigated the subject of sexual dysfunction, the association between psychiatric disorders and ED is not well characterized [13,14,15], especially no studies on the influencing factors. In addition, studies on ED may in terms of regions, periods, and measurement methods, thus it is necessary to analyze ED patients under different cultural, ethnic and socio-economic backgrounds.
Therefore, this research sought to investigate the associated factors and prevalence of anxiety and depression among ED patients in China. The findings will help to intervene reversible risk factors and formulate early individualized treatment for high-risk ED patients.
Methods
Study design
This was a questionnaire-based cross-sectional survey conducted in the andrology center of the Third Xiangya Hospital of Central South University in Hunan, China from July 2021 to April 2022. Using the PASS 15 software and with a confidence level of 0.95, an estimated prevalence rate of 30%, and error not exceeding 4%, sample size was calculated to be 502.
Participants
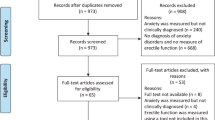
Patients who complained of erectile dysfunction and visited the outpatient department were consecutively enrolled, and all participants were required to complete the questionnaire independently in a separate room after obtaining informed consent. Consultation was allowed when confused about any options, and the completed questionnaire would be checked by staff. A total of 550 respondents were recruited during this period, and 511 participants who met inclusion and did not meet the exclusion criteria were included in the study. The inclusion criteria were as follows: (1) men aged 18–60; (2) sexual life history over 6 months; (3) scores of the 5-item International Index of Erectile Function (IIEF-5) questionnaire are between 5 and 21. The exclusion criteria were as follows: (1) cognitive or communication disorders; (2) previous serious mental illness; (3) history of severe chronic diseases. All participants gave informed consent and could withdraw or interrupt from the study at any time. This study was approved by the IRB of The Third Xiangya Hospital of Central South University (date: 24/04/2019; number: 2019-S252) and registered in the Chinese Clinical Trial Registry (date: 05/09/2019; number: ChiCTR1900025700).
Study questionnaire
The paper questionnaire consisted of three parts, and all scales in this study were Chinese version. The first part collected general information including living habits, age, education level, body mass index (BMI), occupation, sexual behavior among others. The second part contained the IIEF-5 questionnaire for evaluating erectile function, and the third part included self-rating anxiety scale (SAS) and self-rating depression scale (SDS) for anxiety and depression.
The IIEF-5 questionnaire is an effective tool used to detect the existence and severity of ED and has been linguistically validated in multilingual languages [16,17,18]. The Chinese version of IIEF-5 scale has been validated and extensively applied [19, 20]. Based on the Chinese version of IIEF-5 scale scores, the severity categories of ED was classified as follows: no ED (22–25 points), mild (17–21 points), mild to moderate (12–16 points), moderate (8–11 points) and severe (5–7 points).
SAS and SDS scales are standard assessment tools, whose validity and reliability have been examined in several studies [21, 22]. The SAS is a self-report measurement psychological scale developed by Zung in 1971 to evaluate anxiety [23]. It includes twenty items, five of which are reverse scores, and each item can be scored 1 to 4 points according the following options: 1 (no score or very limited score time), 2 (A small amount of time), 3 (for a long time) and 4 (most or all of the time). A SAS index score is the raw scores of all items multiplied by 1.25 to obtain the integer, which can be divided as follows: severe anxiety (≥ 70 points), moderate anxiety (60–69 points), mild anxiety (50–59 points) and no anxiety (< 50 points).
The SDS is a psychological scale established by Zung in 1965 to evaluate depression [24]. Similar to SAS, it also has 20 items, 10 of which are reverse scores. In the Chinese version of the SDS scales, a cut-off score of 53 points (a raw score of 42) has been recommended in the Chinese population [25], which has since been adopted by several Chinese studies [26, 27]. The SDS index score can be divided as follows: severe depression (≥ 73 points), moderate depression (63–72 points), mild depression (53–62 points) and no depression (< 53 points).
Statistical analysis
Data were analyzed using the Statistical Product and Service Solutions (SPSS, version 26.0, IBM, Armonk, NY, USA). Frequencies were used to describe categorical variables, and means ± standard deviation (SD) were used to represent scale scores. The Kolmogorov–Smirnov test was used to test normal distribution. Independent sample t-test or single-factor analysis of variance (ANOVA) was used to compare the scores of depression and anxiety scales among different groups and multivariate linear regression analysis was used to identify associated factors of depression and anxiety. Categorical variables (hobbies and occupations) in the multivariate regression analysis were encoded as dummy variables. P < 0.05 was statistically significant.
Results
Demographic characteristics
A total of 550 respondents were recruited where 28 did not meet inclusion criteria and 11 met exclusion criteria. Finally, 511 males with ED were enrolled. The Cronbach alpha coefficient of the IIEF-5 questionnaire we used was 0.81, the SDS scale was 0.77, and the SAS scale was 0.66, showing sufficient internal consistency. Baseline characteristics of ED patients are detailed in Table 1. The mean age and IIEF-5 score was 33.79 ± 8.20 years and 12.76 ± 4.45 points, respectively. Approximately 35.23% had sought treatment for ED and 22.7% had different sexual partner, 49.51% were smokers, 35.62% were alcohol consumers, 58.32% had irregular sleep and 40.31% had no regular exercise. According to the IIEF-5 score, 14.29% of patients had severe ED, 27.40% had moderate ED, 35.81% had mild to moderate ED and 22.50% had mild ED.
Anxiety and depression
The severity categories of depression and anxiety are shown in Table 2. The prevalence of anxiety was 38.16% and the mean anxiety index score was 47.37 ± 6.69 points. The prevalence of depression was 64.97% and the mean depression index score was 54.72 ± 9.10 points. About 31.51% of ED patients had both anxiety and depression.
Univariate analysis
Univariate analysis was performed to assess the association between depression and anxiety and demographic variables, including age, BMI, education level, occupation, hobbies, smoking, alcohol drinking, coffee drinking, regular sleep, regular exercise, treatment history, regular sexual partner, onset time, frequency of intercourse, and severity of ED (Table 1). The factors associated with depression and anxiety are not always the same. The results revealed that age (p < 0.001), education level (p < 0.001), occupation (p = 0.031), hobbies (p = 0.011), smoking (p < 0.001), regular sleep (p < 0.001), treatment history (p < 0.001), regular sexual partner (p = 0.005), onset time (p < 0.001), and severity of ED (p < 0.001) were significantly associated with anxiety, whereas education level (p < 0.001), occupation (p < 0.001), hobbies (p = 0.039), smoking (p < 0.001), coffee drinking (p = 0.007), regular exercise (p < 0.001), treatment history (p = 0.032), and severity of ED (p = 0.032) were significantly associated with depression.
Multiple linear regression analysis
Factors with statistical significance in the univariate analysis were used as independent variables and anxiety or depression index scores were used as dependent variables for multivariate analysis. Results showed that a worsening ED (49.68 ± 6.66), low education level (49.52 ± 6.52), smoking (48.42 ± 6.13), younger age (50.03 ± 7.99), longer onset time (48.44 ± 6.93), and irregular sleep (48.24 ± 6.78) were positively associated with a high risk of anxiety (Table 3R2 = 0.17). In addition, worse ED (56.56 ± 8.26), low education level (58.84 ± 7.01), smoking (56.69 ± 8.05), and irregular exercise (56.80 ± 8.82) was associated with increased risk of depression (Table 4R2 = 0.169).
Discussion
This research identified factors associated with anxiety and depression among ED patients in China. About 38.16% and 64.97% of ED patients had anxiety and depression respectively, whereas 31.51% of ED patients had both anxiety and depression; and most of the symptoms were mild. The prevalence of anxiety and depression is higher than that reported in a previous study in Greece (anxiety disorders in 11.7% and depressive disorders in 25.2%) and Japan (anxiety was 7.7% -29.1% and depression was 13.6% -32.1% in different age groups) [12, 28]. This difference may be caused by geographical, cultural or socio-economic differences, especially given that it was conducted after the COVID-19 disease outbreak. Anxiety symptoms in the general population have nearly doubled to 24% compared to before the COVID-19 outbreak [29]; anxiety and depression have been reported to be major psychological challenges during the COVID-19 pandemic [30,31,32].
In our study, more than a third of ED patients had moderate or severe ED, and multivariate linear regression analysis demonstrated that anxiety and depression were significantly positively associated with ED severity. Patients with worse ED (a lower IIEF-5 score) are more likely to develop anxiety or depression. This is similar to findings from some previous studies [33, 34], but differs from one European report [12]. The latter study found that depressive symptoms were not associated with ED severity, although they enrolled a small sample size. Moreover, the mechanism linking ED and psychological problems has not been well studied. ED patients tend to have low positive emotions and negative expectations about their sexual performance. This mental state distracts their attention from erotic signals, leading to inhibition of genital arousal. As a consequence, some men will avoid sex, which worsens their initial negative sex-related effect [35]. Therefore, we speculate that men with severe ED will experience higher stigma, weakness, and fear, all of which negatively affect their sexual function, but the causality of this relationship needs further investigation.
Educational level has been shown to protect against psychological disorders development in the general population [36, 37]. In line with these results, our study found that educational levels were significantly negatively associated with depression and anxiety in ED patients. This reinforces the findings of existing literature and support the hypothesis that higher levels of education can be a protective factor against depression and anxiety in ED patients. This finding can be attributed to the fact that education precedes and influences other socio-economic indicators, such as family status and income [37], and can make patients more receptive to disease status or understand its expected therapeutic outcomes.
Although age can influence anxiety and depression, this varies with the content. For example, prevalence of depression and anxiety increases with age under conflict settings [38], while the severity of depression and anxiety decreases with age among breast cancer patients [39]. Our data demonstrated that younger age was associated with higher levels of anxiety symptoms. Younger patients find it more difficulty to cope with ED, and may be more anxious due to their multiple social roles and sensitive family roles. Therefore, the psychological burden is heavier among young ED patients.
Furthermore, emerging evidence from previous studies has linked the onset and symptoms of mental disorders in the general population to healthy “lifestyle factors”, which refers to healthy behaviors such as physical activity, diet, smoking, and sleep [40]. For example, a meta-review showed that smoking was a causal factor contributing to the occurrence of severe and moderate mental illness. Moreover, the use of physical activity in specific situations and poor sleep quality were risk factor for mental illness [41]. In our study, we found that healthy lifestyles such as non-smoking, regular sleep, and regular exercise can reduce anxiety or depression symptoms, but anxiety or depression is not always affected by the same factors, with regular sleep only affects anxiety and regular exercise only associated with depression. This may be attributed to the characteristics of ED population or to different mechanisms of anxiety and depression. Anxiety is characterized by worry, feelings of apprehension, and prominent tension, while depression is manifested as slow thinking, depressive mood, and loss of interest [42]. Moreover, although regular sexual partner, treatment history, occupation, hobbies, and coffee drinking were statistically significant in univariate analysis, and a previous study showed that partnered with women with female sexual dysfunction can increase risk of erectile dysfunction [43], they were not in multivariate analysis, thus further research is needed.
Our current findings are important today, it provides insights into the associated factors and prevalence of anxiety and depression, as well as coping strategies among ED patients. Anxiety and depression among patients with ED represent a major public health problem, and a large number of ED patients have both diseases. For ED patients with anxiety or depression, psychosocial interventions including cognitive and behavioral therapy, and different modalities (e.g., marital therapy, sexual skills training, psychosexual education) are recommended (2). In addition, counselling for partner is also recommended [43]. In clinical practice, most Chinese doctors lack the psychological disease diagnosis and treatment background and do not evaluate psychological situation before treatment, which may affect the treatment outcomes of ED. Therefore, in-depth analysis of the psychological state of ED patients and its associated factors may help to explore the association of depression and anxiety with ED to develop individualized treatment options.
Limitations
First, since this is a cross-sectional design, it was difficult to infer the causality between ED and psychological diseases. Second, all participants were recruited from the men’s outpatient department, and most of the patients were from Hunan province and a few from other provinces, so ample biasness was inevitable, and multicenter or large sample study is necessary. Third, our study lacks patients with severe anxiety and depression, this could be because people with severe symptoms cannot complete the questionnaire independently. Therefore, future studies should be conducted with large sample size.
Conclusions
In summary, this study demonstrated the prevalence and associated factors of anxiety and depression among patients with ED in China. The prevalence of anxiety and depression in ED patients is high, and the severity of ED, education level, age, smoking, onset time, regular sleep, and exercise were associated with anxiety or depression symptoms. Clinicians should not ignore the psychological problems of ED patients, and they should work more closely with psychiatrists to help patients find reversible risk factors such as unhealthy “lifestyle factors” and administer individualized treatment in a timely manner.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due individual privacy but are available from the corresponding author on reasonable request.
Abbreviations
- ED:
-
Erectile dysfunction
- IIEF-5:
-
5-Item international index of erectile function
- SAS:
-
Self-rating anxiety scale
- SDS:
-
Self-rating depression scale
- BMI:
-
Body mass index
- PASS:
-
Power analysis and sample size
- IRB:
-
Institutional review board
- SPSS:
-
Statistical product service solutions
- SD:
-
Standard deviation
- ANOVA:
-
Analysis of variance
References
NIH Consensus Conference. NIH consensus development panel on impotence. JAMA. 1993;270(1):83–90.
Salonia A, Bettocchi C, Boeri L, Capogrosso P, Carvalho J, Cilesiz NC, et al. European association of urology guidelines on sexual and reproductive health-2021 update: male sexual dysfunction. Eur Urol. 2021;80(3):333–57.
Goldstein I, Goren A, Li VW, Tang WY, Hassan TA. Epidemiology update of erectile dysfunction in eight countries with high burden. Sex Med Rev. 2020;8(1):48–58.
Quilter M, Hodges L, von Hurst P, Borman B, Coad J. Male Sexual function in New Zealand: a population-based cross-sectional survey of the prevalence of erectile dysfunction in men aged 40–70 years. J Sex Med. 2017;14(7):928–36.
Melman A, Gingell JC. The epidemiology and pathophysiology of erectile dysfunction. J Urol. 1999;161(1):5–11.
Nguyen HMT, Gabrielson AT, Hellstrom WJG. Erectile dysfunction in young men-a review of the prevalence and risk factors. Sex Med Rev. 2017;5(4):508–20.
Shiri R, Koskimaki J, Tammela TL, Hakkinen J, Auvinen A, Hakama M. Bidirectional relationship between depression and erectile dysfunction. J Urol. 2007;177(2):669–73.
Rajkumar RP, Kumaran AK. Depression and anxiety in men with sexual dysfunction: a retrospective study. Compr Psychiatry. 2015;60:114–8.
McCabe MP, Althof SE. A systematic review of the psychosocial outcomes associated with erectile dysfunction: does the impact of erectile dysfunction extend beyond a man’s inability to have sex? J Sex Med. 2014;11(2):347–63.
Liu Q, Zhang Y, Wang J, Li S, Cheng Y, Guo J, et al. Erectile dysfunction and depression: a systematic review and meta-analysis. J Sex Med. 2018;15(8):1073–82.
Yafi FA, Jenkins L, Albersen M, Corona G, Isidori AM, Goldfarb S, et al. Erectile dysfunction. Nat Rev Dis Primers. 2016;2:16003.
Mallis D, Moysidis K, Nakopoulou E, Papaharitou S, Hatzimouratidis K, Hatzichristou D. Psychiatric morbidity is frequently undetected in patients with erectile dysfunction. J Urol. 2005;174(5):1913–6.
Dubin JM, Bennett NE, Halpern JA. The adverse impact of COVID-19 on men’s health. Curr Opin Urol. 2022;32(2):146–51.
Pennanen-Iire C, Prereira-Lourenco M, Padoa A, Ribeirinho A, Samico A, Gressler M, et al. Sexual health implications of COVID-19 pandemic. Sex Med Rev. 2021;9(1):3–14.
Shamloul R, Ghanem H. Erectile dysfunction. The Lancet. 2013;381(9861):153–65.
Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Peña BM. Development and evaluation of an abridged, 5-item version of the international index of erectile function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11(6):319–26.
Utomo E, Blok BF, Pastoor H, Bangma CH, Korfage IJ. The measurement properties of the five-item international index of erectile function (IIEF-5): a Dutch validation study. Andrology. 2015;3(6):1154–9.
Vallejo-Medina P, Saffon JP, Alvarez-Muelas A. Colombian clinical validation of the international index of erectile function (IIEF-5). Sex Med. 2022;10(1): 100461.
Yang B, Xu P, Shi Y, Xu J, Zheng L, Li H, et al. Erectile dysfunction and associated risk factors in Chinese males of infertile couples. J Sex Med. 2018;15(5):671–7.
Tang Z, Li D, Zhang X, Yi L, Zhu X, Zeng X, et al. Comparison of the simplified international index of erectile function (IIEF-5) in patients of erectile dysfunction with different pathophysiologies. BMC Urol. 2014;14:52.
Dunstan DA, Scott N, Todd AK. Screening for anxiety and depression: reassessing the utility of the Zung scales. BMC Psychiatry. 2017;17(1):329.
Dunstan DA, Scott N. Norms for Zung’s self-rating anxiety scale. BMC Psychiatry. 2020;20(1):90.
Zung WWK. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–9.
Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70.
Wang CF, Cai ZH, Xu Q. Self-rating depression scale - evaluation analysis of SDS in 1,340 normal persons. Chin J Nervous Mental Dis. 1986;05:267–8.
Feng Q, Zhang QL, Du Y, Ye YL, He QQ. Associations of physical activity, screen time with depression, anxiety and sleep quality among Chinese college freshmen. PLoS ONE. 2014;9(6): e100914.
Dunstan DA, Scott N. Clarification of the cut-off score for Zung’s self-rating depression scale. BMC Psychiatry. 2019;19(1):177.
Sugimori H, Yoshida K, Tanaka T, Baba K, Nishida T, Nakazawa R, et al. Relationships between erectile dysfunction, depression, and anxiety in Japanese subjects. J Sex Med. 2005;2(3):390–6.
Kwong ASF, Pearson RM, Adams MJ, Northstone K, Tilling K, Smith D, et al. Mental health before and during the COVID-19 pandemic in two longitudinal UK population cohorts. Br J Psychiatry. 2021;218(6):334–43.
Slomski A. Pediatric depression and anxiety doubled during the pandemic. JAMA. 2021;326(13):1246.
Gloster AT, Lamnisos D, Lubenko J, Presti G, Squatrito V, Constantinou M, et al. Impact of COVID-19 pandemic on mental health: an international study. PLoS ONE. 2020;15(12): e0244809.
Zhou Q, Hu Z, Bian G, Yu H, Li X, Lu Y, et al. Mental health and psychosocial function of general population during the COVID-19 epidemic in China. Clin Transl Med. 2020;10(2): e103.
Yang Y, Song Y, Lu Y, Xu Y, Liu L, Liu X. Associations between erectile dysfunction and psychological disorders (depression and anxiety): a cross-sectional study in a Chinese population. Andrologia. 2019;51(10): e13395.
Gao J, Zhang X, Su P, Liu J, Shi K, Hao Z, et al. Relationship between sexual dysfunction and psychological burden in men with infertility: a large observational study in China. J Sex Med. 2013;10(8):1935–42.
Dewitte M, Bettocchi C, Carvalho J, Corona G, Flink I, Limoncin E, et al. A psychosocial approach to erectile dysfunction: position statements from the European society of sexual medicine (ESSM). Sex Med. 2021;9(6): 100434.
Shi Z, Qin Y, Chair SY, Liu Y, Tian Y, Li X, et al. Anxiety and depression levels of the general population during the rapid progressing stage in the coronavirus disease 2019 outbreak: a cross-sectional online investigation in China. BMJ Open. 2021;11(5): e050084.
Bjelland I, Krokstad S, Mykletun A, Dahl AA, Tell GS, Tambs K. Does a higher educational level protect against anxiety and depression? The HUNT Stud Soc Sci Med. 2008;66(6):1334–45.
Charlson F, van Ommeren M, Flaxman A, Cornett J, Whiteford H, Saxena S. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. The Lancet. 2019;394(10194):240–8.
Yang H, Brand JS, Fang F, Chiesa F, Johansson AL, Hall P, et al. Time-dependent risk of depression, anxiety, and stress-related disorders in patients with invasive and in situ breast cancer. Int J Cancer. 2017;140(4):841–52.
Lianov L, Johnson M. Physician competencies for prescribing lifestyle medicine. JAMA. 2010;304(2):202–3.
Firth J, Solmi M, Wootton RE, Vancampfort D, Schuch FB, Hoare E, et al. A meta-review of “lifestyle psychiatry”: the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. 2020;19(3):360–80.
Robinson OJ, Overstreet C, Letkiewicz A, Grillon C. Depressed mood enhances anxiety to unpredictable threat. Psychol Med. 2012;42(7):1397–407.
Chew PY, Choy CL, Sidi HB, Abdullah N, Che Roos NA, Salleh Sahimi HM, et al. The association between female sexual dysfunction and sexual dysfunction in the male partner: a systematic review and meta-analysis. J Sex Med. 2021;18(1):99–112.
Acknowledgements
The authors would like to thank the Third Xiangya Hospital of Central South University for its support.
Funding
This work was supported by the Research Foundation from Hunan Provincial Health Commission (202204054996).
Author information
Authors and Affiliations
Contributions
YX, TX, JY contributed to the conception and design of the study. YX, JY performed the statistical analysis and wrote the article. TX, JP, JL contributed to data collection. JP contributed to research registration. XZ, MY, HZ contributed to manuscript revision. All authors contributed to the article and approved the submitted version. All authors read and approved by the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the IRB of The Third Xiangya Hospital of Central South University (date: 24/04/2019; number: 2019-S252) and registered in the Chinese Clinical Trial Registry (date: 05/09/2019; number: ChiCTR1900025700). Written informed consent to participate in this study was provided by the participants, and the study was conducted in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xiao, Y., Xie, T., Peng, J. et al. Factors associated with anxiety and depression in patients with erectile dysfunction: a cross-sectional study. BMC Psychol 11, 36 (2023). https://doi.org/10.1186/s40359-023-01074-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-023-01074-w