
Abstract
Background
This study examines associations between psychological distress, intentions to use e-cigarettes, and cigarette smoking, e-cigarette use, and cannabis consumption through e-cigarette use among a diverse sample of U.S. young adults.
Procedures
Young adults (N = 314; 72.5% female) were recruited to complete an online survey during the first few months of the COVID-19 pandemic.
Results
Associations between psychological distress and cigarette smoking, e-cigarette use, cannabis vaping, and intentions to use e-cigarettes were found. Current e-cigarette use (OR = 1.23, 95% CI 1.17, 1.28, p < .001; 7.5%) and cannabis vaping (OR = 2.03, 95% CI 1.88, 2.18, p < .001; 10%) was higher among female, possibly due to the significantly higher psychological distress reported among females. Interactions between intentions to use e-cigarettes and psychological distress variables were found for all smoking and vaping behaviors.
Conclusions
Public health efforts should increase focus on providing psychological services for young adults to improve coping strategies that are alternative to smoking and vaping behaviors.
Similar content being viewed by others

Introduction
E-cigarette use has become a major health concern among young adults. In 2018, the estimated prevalence of young adult (ages 18–24) current electronic cigarette (e-cigarette) users was 7.6% [1]. More than half of e-cigarette users are under the age of 35 [2]. Moreover, the COVID-19 pandemic has placed additional health burdens among cigarette smokers and e-cigarette users. In fact, smokers and e-cigarette users are significantly more likely to report COVID-19 symptoms [3,4,5]. Moreover, the predominant use of—and preference for—e-cigarette products among young adults presents an additional concern due to increased psychological distress during the COVID-19 pandemic [6]. Increased rates of psychological distress during the early COVID-19 pandemic may have facilitated smoking and e-cigarette use as well as intentions to use e-cigarettes. Thus, an examination of the role of psychological distress and intentions to use e-cigarettes as an underlying mechanism of smoking and e-cigarette use among young adults in the U.S. during the early pandemic is needed.
Increased risk of COVID-19 outcomes for smokers and e-cigarette users
Evidence suggests that current cigarette smokers are at an increased risk of COVID-19 outcomes due to enhanced expression of angiotensin-converting enzyme-2 (ACE-2), which is the gene encoding the receptor for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), throughout the human airway tract [7]. Not only are cigarette smokers more likely to report symptoms of COVID-19, but they are also more likely to be hospitalized if they test positive for COVID-19 [4, 5]. For example, heavy smokers (i.e., more than 30 pack-years) have higher odds of hospitalization and death following a COVID-19 diagnosis when compared to non-smokers [8]. Additionally, men who smoke have a higher expression of ACE-2 than women, possibly explaining higher COVID-19 mortality rates among males [9, 10]. Sex differences in ACE-2 expression have also been found for e-cigarettes use [11].
Although not yet extensively studied as cigarette smoking exposure, studies examining e-cigarette use have begun to demonstrate a similar association with COVID-19 risk [12]. Often referred to as “vaping” because many people incorrectly believe e-cigarettes create a vapor that is then inhaled but, in fact, produce an aerosol of tiny particles, e-cigarettes have become a growing public health concern among adolescents and young adults [13,14,15]. Specifically, a greater preference for e-cigarettes among youth [2, 16], which are often perceived to be safer than traditional cigarette products [17, 18], highlights a need for empirical work to explore the use of vaping products during a highly distressing time (i.e., the early COVID-19 pandemic months). In fact, e-cigarette use, or “vaping”, seems to be associated with COVID-19 diagnosis among adolescents and young adults [3].
E-cigarettes, or vaping products, may be used in a variety of methods and for various purposes. For example, some e-cigarette users will concurrently smoke cigarettes or use vaping to consume cannabis products. In fact, a large proportion of e-cigarette users report a preference for “vaping” cannabis as opposed to smoking it [19], particularly among young adults [20]. When examining the risk of COVID-19 diagnosis among cigarette smokers, e-cigarette users, and dual users (i.e., individuals who use both cigarettes and e-cigarettes), COVID-19 diagnosis was five times more likely among exclusive e-cigarettes users and seven times more likely among dual-users [3]. Moreover, some studies have suggested that concurrent use of e-cigarettes and cannabis may be an underlying risk factor of COVID-19 symptomatology and diagnosis, in that, compared to exclusive e-cigarette users, concurrent e-cigarette and cannabis users were more than three times more likely to report COVID-19 symptoms and almost twice as likely to report a COVID-19 diagnosis [21]. Taken together, growing evidence shows an increased risk of COVID-19 outcomes due to cigarette smoke and e-cigarette “vaping”. Furthermore, these associations emphasize a need to illuminate the role of psychological distress in driving the use of cigarette and vaping products during the early COVID-19 pandemic.
Intentions to use e-cigarettes
According to the Theory of Planned Behavior [22, 23], a person’s intentions to engage in a behavior are a major determinant in behavioral engagement. It is well established that intentions to engage in behaviors are important predictors of future smoking behaviors among youth [24, 25], such that intentions to use e-cigarettes are related to current e-cigarette and cigarette use [26]. Moreover, e-cigarette use appears to increase the likelihood of cigarette smoking among youth [27], by way of increasing intentions to smoke cigarettes when youth have used e-cigarettes [28, 29]. Additionally, intentions to quit using e-cigarettes are lower among youth dual users as opposed to exclusive e-cigarette users [30]. Thus, intentions to use e-cigarettes are important determinants of future behaviors which may increase the likelihood of e-cigarette use as well as cigarette smoking behaviors.
Furthermore, the increased risk that COVID-19 poses to smokers, and the increased experiences of psychological distress during the pandemic, may influence behavioral intentions. For example, among a sample of Italian adults during the COVID-19 lockdown in April 2020, most exclusive cigarette smokers reported considering quitting, but most exclusive e-cigarette users had not considered stopping the use of e-cigarettes [31]. Thoughts of quitting appear to differ according to smoking or vaping method and may closely reflect intentions. Indeed, past work has found that more than 10% of youth had intentions to use e-cigarettes and smoke cigarettes [32, 33]. Alternatively, more than half of current e-cigarette young adult users want to quit [34]. Yet, many cigarettes and e-cigarettes users may find it difficult to quit because psychological distress can make it more difficult to succeed [35].
Psychological distress related to smoking and vaping behaviors
The pandemic has led to significant increase in psychological distress (i.e., anxiety, depression, stress) [36]. Among the general U.S. adult population during the spring of 2020, clinically significant levels of anxiety and depression were reported, particularly among young adults [37,38,39]. Persistently elevated psychological distress among U.S. adults spanning from April 2020 through August 2021 in comparison to consistent prevalence rates of 3–4% prior to the onset of the COVID-19 pandemic demonstrate the ongoing impact on mental health [40]. Although several studies have reported a decline or cessation of e-cigarette use among many populations during the pandemic because of factors such as lack of accessibility due to stay-at-home orders and smoke shop closures, some proportion of young adults increased their use of e-cigarettes [41, 42]. For example, since the start of the pandemic, 24% of smokers increased their cigarette use and 28% decreased [43]. Conversely, over 27% of e-cigarette users had increased their e-cigarette use and less than 24% had decreased [43]. Differences in reduction rates between cigarette and e-cigarette use may reflect underlying mechanisms such as age, risk perceptions [44], nicotine dependence [45], and a possible preference for e-cigarette use as a coping strategy for psychological distress among youth. Yet, most studies have not examined the role of psychological distress as a facilitating factor in the use of e-cigarette use among current young adult users since the start of the pandemic.
As smoking behaviors are often precipitated by reports of high anxiety and stress [46,47,48], it may also lead to an increase in smoking and the use of e-cigarettes among young adults during the pandemic. In fact, college students often report using e-cigarettes as a stress management tool [49]. Moreover, among youth, loneliness has been positively associated with smoking [50] and e-cigarette use [51]. Similarly, depression is associated with higher smoking dependence [52] and appears to account for difficulty in smoking cessation efforts as rates remain consistently lower for depressed smokers than for smokers in the general population [53]. However, there is a lack of research examining whether increases in psychological distress of anxiety, depression, loneliness, and stress, during the early months of the COVID-19 pandemic influenced smoking, e-cigarette use, and intentions to use e-cigarettes simultaneously among young adults in the U.S.
Current study
The current study aims to examine rates of cigarette smoking, e-cigarette use, dual usage, and cannabis vaping during the early months of the COVID-19 pandemic, well as the influence of intentions to use e-cigarettes and psychological distress (i.e., anxiety, depression, loneliness, and stress) on smoking and vaping behaviors among young adults. Due to the increase in popularity of electronic devices for smoking [2], this study primarily focused on the intentions and use of e-cigarettes. However, cigarette smoking was also assessed as an outcome. Moreover, due to marked differences in smoking behaviors between men and women [54], associations were examined separately for gender. Four hypotheses were proposed: (H1) Current cigarette smoking prevalence will be lower than e-cigarette use rates among young adults, but both rates will be higher among men than women. (H2) Intentions to use e-cigarettes in the future will be higher among dual cigarette and e-cigarette users as well as those who use e-cigarettes to vape cannabis in comparison to current exclusive cigarette or exclusive e-cigarette users. (H3) Moreover, intentions to use e-cigarettes will be positively associated with cigarette smoking, e-cigarette use, and the use of e-cigarettes to consume cannabis among both men and women. Last, (H4) psychological distress, including anxiety, depression, loneliness, and stress will be positively associated with current cigarette smoking, e-cigarette use, dual use, and consumption of cannabis through e-cigarettes by interacting with intentions to use e-cigarettes.
Methods
Participants
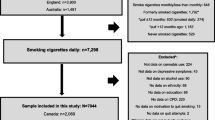
Participants for this study were recruited between September 2019 to December 2020 and included 405 emerging adults (M age = 20.35; SD = 2.71) from the greater Los Angeles area. Analyses for this study included respondents who participated from March 23, 2020 to November 25, 2020 (N = 314; M age = 20.56, SD = 2.97; 73% females), after the World Health Organization (WHO) declared COVID-19 a global pandemic on March 11, 2020. Respondents collected prior to the pandemic from September 14, 2019 to December 2, 2019 (n = 91) were excluded from analyses as this study focused on processes during the pandemic. Seventy-two percent of the sample were current college students. The sample was diverse in racial/ethnic background (22% Asian; 4.2% Black; 11.9% Latina/o; 1.5% Pacific Islander; 1.7% Other; 45.7% White; 13% Multiracial), but predominantly identified as female (72.5%). Most participants identified as Heterosexual (70%), followed by Bisexual (17%), Gay/Lesbian (7%), Queer (1.7%), and Other/Prefer not to say (4.3%). The median household income was between 80,000 to 89,999 per year. Over 30% of participants reported their parents’ (both mother and father) education attainment to be a 4-year college degree.
Measures
Item questions and statements for variables measured can be found in Table 1.
Cigarette smoking and e-cigarette use
Current cigarette smoking was assessed using a single item (see Table 1 for item questions and statements) responses on a 4-point scale (1 = “No, I never was a smoker”; 2 = “No, I am an ex-smoker”; 3 = “Yes, occasionally but not every day”; 4 = “Yes, I smoke every day”). Participants who reported occasional and frequent current use of cigarettes were combined and dichotomized (0 = “No”, 1 = “Yes”) to estimate the prevalence of overall current cigarette smokers across usage levels. Prevalence of ever having used an e-cigarette was measured using a single question regarding knowledge of e-cigarettes responses (1 = “No, I have never read anything about it and nobody told me about it”; 2 = “Yes, I read a bit about it or someone told me about it”; 3 = “Yes, I am informed on the e-cigarette, but I have never used it”; 4 = “Yes, and I have already used an e-cigarette”). Participants who responded “Yes, and I have already used an e-cigarette” were used to calculate the prevalence of ever e-cigarette use. Current e-cigarette use was assessed using a single item responses on a 5-point scale (1 = “No, I have never used it”; 2 = “No, but I have used it in the past”; 3 = “Yes, occasionally”; 4 = “Yes, I use it frequently but not daily”; 5 = “Yes, I use it every day”). Occasional, frequent, and daily current use of e-cigarettes were combined and dichotomized (0 = “No”, 1 = “Yes”) to estimate the prevalence of overall current users of e-cigarettes across usage levels.
Dual users of cigarettes and e-cigarettes were identified by coding (1 = exclusive cigarette user; 2 = exclusive e-cigarette user; 3 = dual user) based on responses to both items of current e-cigarette use and current cigarette smoking who responded with any of the affirmative answers to both questions (i.e., “Yes, occasionally”; “Yes, I use it frequently but not daily”; “Yes, I use it every day”).
Cannabis consumption
Cannabis consumption and use of e-cigarettes to consume cannabis products were each assessed using single items. Recent cannabis consumption was measured using the frequency of cannabis consumption in the last month, in which participants entered a numerical response to indicate the number of days cannabis was consumed in the last 30 days. Responses were dichotomized to indicate whether the participant was a current cannabis user (0 = “no use in the past 30 days”, 1 = “at least one day of use in the last 30 days”). The use of e-cigarettes to consume cannabis was measured as a discrete response to a single item question. Participants chose from various substances in their response including cannabis, cocaine, heroin, amphetamines, ecstasy, benzodiazepines/barbiturates, nicotine, and other. Participants who selected cannabis, regardless of their use of additional non-cannabis substances, were coded to indicate use of e-cigarettes to consume cannabis (0 = non-cannabis use of e-cigarettes; 1 = cannabis use of e-cigarettes).
E-cigarette intentions
Participants’ intentions to use e-cigarettes in the future, regardless of current and past e-cigarette use, were assessed using a single item on a 4-point response scale (1 = “I have no intention at all to use an e-cigarette”; 2 = “I don’t have plans to use or abstain from using an e-cigarette”; 3 = “I plan to use an e-cigarette”; 4 = “I strongly want to use an electronic cigarette”). Among current and past e-cigarette users, intentions to continue use of e-cigarettes was assessed using an additional single item about the length of time they intended to continue using e-cigarettes. Responses were on a 11-point scale (1 = “0 days”; 2 = “1 to 6 days”; 3 = “1 week”; 4 = “2 weeks”; 5 = “3 weeks”; 6 = “4 weeks”; 7 = “2 months”; 8 = “3 months”; 9 = “6 months”; 10 = “1 year”; 11 = “More than 1 year”).
Psychological distress
Anxiety, depression, loneliness, and stress were separately assessed as single item measures of psychological distress. Previous work has supported the use of single item measures of self-rated mental health to be highly associated with multi-item measures of health [55]. Perceived anxiety, depression, loneliness, and stress were assessed using single items of each variable as reported for symptoms in the past month. Responses for all psychological distress measures were on a 5-point scale (1 = “Never”; 2 = “Rarely”; 3 = “Sometimes”; 4 = “Often”; 5 = “Always”). Additionally, two items were used to measure the use of e-cigarettes to relieve anxiety and stress. Responses for the use of e-cigarettes to relieve anxiety were on a 6-point scale (1 = “Not applicable, I don’t experience nervousness, anxiety”; 2 = “No”; 3 = “Maybe”; 4 = “Yes, somewhat”; 5 = “Yes, a lot”; 6 = “Yes, definitely”) and responses for the use of e-cigarettes to relieve stress were on a 4-point scale of agreement (1 = “Not at all true”; 2 = “Not very true”; 3 = “Somewhat true”; 4 = “Very true”).
Procedure
Participants completed an online survey through Qualtrics. The survey included questions on psychosocial determinants (e.g., attitudes, beliefs, other non-tobacco substance use, family history of smoking, peer influence, cultural influence, psychological distress, use to relieve anxiety and stress, weight and stress control), structural factors (e.g., age of initiation, attempts to quit, cost, modification of e-cigarette, flavor preferences, “vaping tricks”, social media vaping viewership, accessibility), and outcomes (i.e., oral and respiratory health such as coughing, throat irritation) of cigarette and e-cigarette use. Informed consent from all participants and IRB approval for the study was obtained through the Human Subjects Committee at Occidental College prior to data collection.
Participant recruitment for the survey was conducted across the 2019–2020 academic year and was open to all young adults over the age of 18. Fall 2019 data collection was completed by December 3 2019, prior to the World Health Organization (WHO) initial report of COVID-19 on December 31, 2019. Spring 2020 data collection began March 23, 2020 after the WHO declared COVID-19 a global pandemic on March 11, 2020. Thus, time of survey completion was used to determine inclusion for analyses (i.e., data collected prior to the WHO declaring COVID-19 a pandemic were excluded), with Spring survey responses used for data analyses.
Statistical analysis
Prevalence of cigarette and e-cigarette use as well as psychological distress differences between gender were examined using chi-square and independent samples t tests, respectively. Differences in psychological distress and intentions to use e-cigarettes across exclusive cigarette (70% female; M age = 20.89, SD = 1.62), exclusive e-cigarette users (85.7% female; M age = 21.50, SD = 4.88), dual users (56.3% female; M age = 21.81, SD = 8.42), and cannabis vapers (76.7% female; M age = 20.53, SD = 2.06) were examined using ANCOVAs. Logistic regressions were used to examine associations between major variables of interests with dichotomous outcomes, represented as odds ratios. Linear regressions were used for continuous outcomes, represented as beta coefficients. Age, race/ethnicity, household income, and parental (mother and father) educational attainment levels were controlled for in all regression analyses. Analyses that examined associations among the total sample additionally controlled for gender. All analyses were performed using weights to adjust for differential representation in the gender population in the sample.
Results
Prevalence and descriptive data for all major variables of interest are provided in Table 2. Gender differences for major variables can be seen in Table 3.
Smoking and e-cigarette use
Among the analytical sample of participants recruited after WHO declared COVID-19 a pandemic (n = 314), 20.4% (18.4% females, 29.3% males) reported being a current or past cigarette smoker, 11% reported being a current smoker (i.e., “occasionally” and “daily”), 39.2% (39.5% females, 42.7% males) reported having ever used an e-cigarette, 11% reported current use of e-cigarettes (i.e., “occasionally”, “frequently”, and “daily”), and 77.7% reported currently being an abstainer from all cigarette and e-cigarette behaviors. Chi-square analyses show that the prevalence of ever having used e-cigarettes was significantly higher than the prevalence of ever having smoked a cigarette (χ2 = 6074.0, df = 1, p < 0.001). A multinomial logistic regression was used to estimate the likelihood of exclusive cigarette, e-cigarette, and dual usage based on gender. Males were more likely to report current cigarette use (OR = 1.26, S.E. = 0.10, 95% CI = 1.03, 1.54), less likely to be current e-cigarette users (OR = 0.44, S.E. = 0.05, 95% CI = 0.40, 0.48), and more than twice as likely to be dual cigarette and e-cigarette users (OR = 2.27, S.E. = 0.09, 95% CI = 1.91, 2.70) than their female counterparts. See Table 2 for details of cigarette and e-cigarette prevalence among males and females and Table 3 for t test results of gender differences.
Intentions to use e-cigarettes
Over 6% of participants, regardless of smoking and e-cigarette use experience, indicated that they planned or wanted to use an e-cigarette in the future (“I plan to use an e-cigarette” = 5.5%; “I strongly want to use an e-cigarette” = 1.6%), with females reporting significantly higher intentions (see Table 3). An ANCOVA among all current cigarette and/or e-cigarette users show that exclusive cigarette users’ intentions to use e-cigarettes (M = 1.75, SD = 0.58) were significantly lower than exclusive e-cigarette users’ (M = 2.38, SD = 0.62) and dual users’ intentions (M = 2.76, SD = 0.83), but dual users’ intentions to use e-cigarettes were not significantly different from exclusive e-cigarette users’ intentions (F (1, 3) = 10,300.45, p < 0.001).
The largest proportion of participants (16%) reported no intentions to use e-cigarettes (0 days), followed by 2 weeks and 1 year (8% each). Among all current cigarette and e-cigarette users, intended length of time for future e-cigarette use significantly differed between females (see Table 3), with males reporting longer timeline intentions to use e-cigarettes. ANCOVA results showed that intended length of time for future use of e-cigarettes was significantly different among exclusive cigarette smokers (M = 1.43, SD = 1.05), exclusive e-cigarette users (M = 5.44, SD = 3.50), and dual users (M = 6.11, SD = 3.08), with cigarette users having the shortest intended length of use between 0 days and less than 1 week (F (2, 5) = 325.76, p < 0.001).
Logistic regressions were used to test associations between intentions to use e-cigarettes and current cigarette and e-cigarette use among females and males. Females were more likely to be current cigarette smokers if they reported intentions to use e-cigarettes (OR = 1.26, S.E. = 0.11, 95% CI = 1.02, 1.55), but the intended length of time for future e-cigarette use did not predict current cigarette usage (OR = 0.99, S.E. = 0.03, 95% CI = 0.94, 1.06). Conversely, intentions to use e-cigarettes did not predict current e-cigarette use (OR = 0.91, S.E. = 0.06, 95% CI = 0.80, 1.03) among females, yet the intended length of time for future e-cigarettes use predicted a higher likelihood of being a current e-cigarette user (OR = 2.87, S.E. = 0.03, 95% CI = 2.70, 3.04). Both intentions to use e-cigarettes (OR = 0.02, S.E. = 0.60, 95% CI = 0.01, 0.04) and intended length of time for future e-cigarettes use (OR = 1.76, S.E. = 0.11, 95% CI = 1.43, 2.16) predicted dual usage of cigarette and e-cigarettes among females. Among males neither type of intentions for e-cigarette use predicted current cigarette use nor e-cigarette use (p > 0.90).
Cannabis use
Over 41% of participants, regardless of smoking and e-cigarette use experience, reported using cannabis in the past month for an average of 9 days (M = 9.47; SD = 10.71) and over 9% reported using e-cigarettes to consume cannabis (see Table 2). Also, males reported a significantly greater number of days consuming cannabis than females (see Table 3). In addition to a higher likelihood of e-cigarette use among females (OR = 1.23, S.E. = 0.02, 95% CI = 1.17, 1.28), chi-square results indicated that a larger prevalence of females reported using e-cigarettes to consume cannabis (χ2 = 261.59, df = 1, p < 0.001) than males. Specifically, a logistic regression revealed that females (10%) were more than twice as likely to report using e-cigarettes to consume cannabis (OR = 2.03, S.E. = 0.04, 95% CI = 1.88, 2.18) than males (7.5%).
Over 7% of cannabis users (cannabis use in the last 30 days ≥ 1 day) reported intentions to use e-cigarettes (“I plan to use e-cigarettes” = 5.8%; “I strongly want to use e-cigarettes” = 1.9%) and 2% reported intentions for long-term future use of e-cigarettes (i.e., more than 1 year). Among the overall sample, recent cannabis users (i.e., at least 1 day of cannabis use in the last 30 days) reported significantly higher intentions to use e-cigarettes (M = 1.48, SD = 0.69; t = − 18, 65, df = 15,037.11, p < 0.001) and lower intentions for the length of time to use e-cigarettes in the future (M = 2.36, SD = 2.76; t = 8.51, df = 1286.07, p < 0.001) in comparison to participants who had not used cannabis recently or at all (M intentions to use e-cigarettes = 1.33, SD = 0.59; M intended length of time for future e-cigarette use = 3.35, SD = 3.81). Males who use cannabis reported significantly higher intentions to use e-cigarettes, but females reported longer intentions of future e-cigarette use than males (see Table 3). MANCOVA results show that participants who use e-cigarettes to consume cannabis significantly differed in their intentions to use e-cigarettes (M = 2.40, S.E. = 0.04; F (4, 13,408) = 1798.85, p < 0.001) and the intended length of time for future e-cigarette use (M = 2.82, S.E. = 0.05; F (4, 13,408) = 1266.98, p < 0.001) than those who did not use cigarettes or e-cigarettes (MD = 0.74, S.E. = 0.01), exclusively used cigarettes (MD = 0.35, S.E. = 0.06), exclusively use e-cigarettes (MD = − 0.25, S.E. = 0.02), and dual users (MD = − 0.63, S.E. = 0.04; see Table 2 for descriptive data of intentions variables across groups).
Among females, linear regressions revealed that intentions to use e-cigarettes (β = 0.44, S.E. = 0.19, p < 0.001) and intended length of time for future e-cigarette use (β = 0.19, S.E. = 0.05, p < 0.001) predicted recent cannabis use (i.e., the last 30 days). Logistic regression indicated that intentions to use e-cigarettes predicted using e-cigarettes to consume cannabis (OR = 2.09, S.E. = 0.04, 95% CI = 1.33, 1.44), but intended length of time for future e-cigarette use did not predict using e-cigarettes to consume cannabis (p = 0.23). Among males, linear regressions revealed that intentions to use e-cigarettes (β = 0.35, S.E. = 0.39, p < 0.001) and intended length of time for future e-cigarette use (β = − 0.50, S.E. = 0.09, p < 0.001) predicted recent cannabis use. Also, a logistic regression demonstrated that intentions to use e-cigarettes (OR = 5006.81, S.E. = 0.58, 95% CI = 1590.28, 15,763.30) and intended length of time for future e-cigarette use (OR = 0.20, S.E. = 0.15, 95% CI = 0.15, 0.27) predicted the use of e-cigarettes to consume cannabis.
Psychological distress
Over 90% of the total sample reported experiencing some level (i.e., “rarely”, “sometimes”, “often”, or “always”) of one or more type of psychological distress (i.e., anxiety, depression, loneliness, or stress). The highest frequency reported was for stress with 30% of participants reporting “sometimes”, 44% of participants reporting “often” and 15% “always”. Independent samples t test (see Table 3) results demonstrate that females reported significantly higher levels of anxiety, depression, loneliness, and stress than males.
A paired samples t test was used to compare levels of psychological distress. Among the overall sample, frequency of reported anxiety (M = 3.31, SD = 1.08) was significantly higher than frequency of depression symptoms (M = 2.94, SD = 0.96) in the last 30 days (t = 111.56, df = 71,337, p < 0.001). Anxiety (M = 3.31, SD = 1.09) was significantly higher than loneliness (M = 2.93, SD = 1.02; t = 97.26, df = 71,605, p < 0.001). Stress (M = 3.65, SD = 0.88) was significantly higher than anxiety (M = 3.31, SD = 1.09; t = − 106.66, df = 71,873, p < 0.001), depression (M = 2.94, SD = 0.96; t = − 224.99, df = 71,337, p < 0.001), and loneliness (M = 2.93, SD = 1.01; t =—202.58, df = 71,605, p < 0.001). Depression (M = 2.94, SD = 0.96) and loneliness (M = 2.93, SD = 1.01) were not significantly different from one another (t = 1.36, df = 71,609, p = 0.17). An ANOVA was used to assess differences in psychological distress between cigarette smokers, e-cigarette users, dual users, and cannabis vapers to individuals who did not engage in any of the behaviors. Participants who did not engage in any of the smoking or vaping behaviors reported significantly lower anxiety (M = 3.29, SD = 1.08; F(1,71,873) = 447.74, p < 0.001), depression (M = 2.91, SD = 0.96; F(1,71,605) = 631.13, p < 0.001), loneliness (M = 2.91, SD = 1.00; F (1, 71,605) = 260.26, p < 0.001), and stress (M = 3.65, SD = 0.88; F (1, 71,873) = 40.67, p < 0.001) than cigarette smokers (M anxiety = 3.40, SD = 0.92; M depression = 3.10, SD = 0.70; M loneliness = 2.90, SD = 1.05; M stress = 3.70, SD = 0.78), e-cigarette users (M anxiety = 3.86, SD = 1.13; M depression = 3.43, SD = 0.82; M loneliness = 3.36, SD = 1.11; M stress = 3.86, SD = 0.83), cannabis vapers (M anxiety = 3.31, SD = 1.02; M depression = 3.07, SD = 0.79; M loneliness = 2.85, SD = 1.14; M stress = 3.64, SD = 0.94), and dual cigarette and e-cigarette users (M anxiety = 3.53, SD = 0.89; M depression = 3.20, SD = 0.75; M loneliness = 3.13, SD = 0.96; M stress = 3.53, SD = 0.72). Logistic regressions were used to examine whether anxiety, depression, loneliness, and stress predict current cigarette use, e-cigarette use, dual usage of cigarette and e-cigarettes, as well as e-cigarettes to consume cannabis. Among females, anxiety (OR = 1.22, S.E. = 0.06, 95% CI = 1.09, 1.36), depression (OR = 1.32, S.E. = 0.06, 95% CI = 1.16, 1.49), loneliness (OR = 1.22, S.E. = 0.05, 95% CI = 1.10, 1.36) and stress (OR = 0.61, S.E. = 0.06, 95% CI = 0.54, 0.69) were significant predictors of current cigarette smoking. Anxiety (OR = 1.52, S.E. = 0.02, 95% CI = 1.45, 1.59), depression (OR = 1.46, S.E. = 0.0395% CI = 1.38, 1.54), loneliness (B = 0.87, S.E. = 0.02, 95% CI = 0.83, 0.91), and stress (OR = 0.64, S.E. = 0.03, 95% CI = 0.61, 0.68) were predictors of e-cigarette use. None of the psychological distress variables significantly predicted dual usage of cigarettes and e-cigarettes among females (p > 0.05). Anxiety (OR = 1.05, S.E. = 0.02, 95% CI = 1.01, 1.09), depression (OR = 1.92, S.E. = 0.03, 95% CI = 1.83, 2.02), loneliness (OR = 0.68, S.E. = 0.02, 95% CI = 0.65, 0.71) and stress (OR = 0.66, S.E. = 0.02, 95% CI = 0.63, 0.69) were significant predictors of using e-cigarettes to consume cannabis.
Among males, anxiety (OR = 1.41, S.E. = 0.08, 95% CI = 1.21, 1.64), depression (OR = 1.34, S.E. = 0.08, 95% CI = 1.14, 1.57), loneliness (OR = 1.26, S.E. = 0.06, 95% CI = 1.11, 1.42) and stress (OR = 0.76, S.E. = 0.09, 95% CI = 0.65, 0.91) were significant predictors of current cigarette smoking. Depression (OR = 3.05, S.E. = 0.07, 95% CI = 2.67, 3.48), loneliness (OR = 2.49, S.E. = 0.07, 95% CI = 2.19, 2.83) and stress (OR = 1.27, S.E. = 0.08, 95% CI = 1.10, 1.47) were significant predictors of current e-cigarette use. None of the psychological distress variables predicted dual usage among males. Anxiety (OR = 0.45, S.E. = 0.05, 95% CI = 0.40, 0.49), loneliness (OR = 0.90, S.E. = 0.05, 95% CI = 0.82, 0.99) and stress (OR = 5.46, S.E. = 0.06, 95% CI = 4.82, 6.17) were significant predictors of using e-cigarettes to consume cannabis.
Independent samples t test used to examine gender differences in the use of e-cigarettes to relieve anxiety and stress (see Table 3) revealed that endorsement of using e-cigarettes to relieve anxiety was significantly higher among males than females. Conversely, endorsement of using e-cigarettes to deal with stress was higher among females than males.
Psychological distress and intentions to use e-cigarettes
Linear regressions were used to test whether psychological distress predicted intentions to use e-cigarettes. Among females, anxiety (β = 0.07, S.E. = 0.01, p < 0.001), depression (β = 0.11, S.E. = 0.01, p < 0.001), loneliness (β = − 0.20, S.E. = 0.01, p < 0.001), and stress (β = 0.04, S.E. = 0.01, p < 0.001) predicted intentions to use e-cigarettes. Also, anxiety (β = − 0.10, S.E. = 0.03, p < 0.001), depression (β = 0.09, S.E. = 0.04, p < 0.001), loneliness (β = − 0.24, S.E. = 0.04, p < 0.001), and stress (β = − 0.10, S.E. = 0.04, p < 0.001) predicted intended length of time for future e-cigarette use. Among males, anxiety (β = − 0.17, S.E. = 0.01, p < 0.001), depression (β = 0.10, S.E. = 0.01, p < 0.001), loneliness (β = 0.04, S.E. = 0.01, p < 0.001), and stress (β = 0.18, S.E. = 0.01, p < 0.001) predicted intentions to use e-cigarettes. Anxiety (β = 0.64, S.E. = 0.10, p < 0.001), depression (β = − 0.46, S.E. = 0.08, p < 0.001), loneliness (β = 0.68, S.E. = 0.08, p < 0.001), and stress (β = − 0.74, S.E. = 0.08, p < 0.001) predicted intended length of time for e-cigarette use.
Subsequently, interactions between intentions to use e-cigarettes and psychological distress factors were used to predict smoking and vaping behaviors. Among females, interactions between intentions to use e-cigarettes and anxiety (OR = 1.08, S.E. = 0.04, 95% CI = 1.00, 1.16) significantly predicted current cigarette smoking. Interactions between intentions to use e-cigarettes and anxiety (OR = 1.30, S.E. = 0.01, 95% CI = 1.26, 1.33) and depression (OR = 1.12, S.E. = 0.01, 95% CI = 1.09, 1.15) significantly predicted e-cigarette use. Interactions between intentions to use e-cigarettes and anxiety (OR = 1.06, S.E. = 0.01, 95% CI = 1.04, 1.09) and depression (OR = 1.07, S.E. = 0.01, 95% CI = 1.04, 1.10) significantly predicted using e-cigarettes to consume cannabis. Interactions with length of time for future intentions to use e-cigarettes with anxiety (OR = 2.09, S.E. = 0.09, 95% CI = 1.74, 2.51), depression (OR = 0.83, S.E. = 0.03, 95% CI = 0.78, 0.87), and loneliness (OR = 0.79, S.E. = 0.05, 95% CI = 0.73, 0.87) significantly predicted cigarette use. Interactions with length of time for future intentions to use e-cigarettes with anxiety (OR = 0.65, S.E. = 0.04, 95% CI = 0.60, 0.70), depression (OR = 1.33, S.E. = 0.02, 95% CI = 1.28, 1.38), and loneliness (OR = 1.25, S.E. = 0.03, 95% CI = 1.18, 1.32) significantly predicted e-cigarette use. Interactions with length of time for future intentions to use e-cigarettes with anxiety (OR = 1.72, S.E. = 0.03, 95% CI = 1.61, 1.83) and loneliness (OR = 0.84, S.E. = 0.02, 95% CI = 0.81, 0.86) significantly predicted e-cigarettes to consume cannabis.
Among males, no psychological distress variables significantly interacted with intentions to use e-cigarettes to predict cigarette smoking. Interactions between intentions to use e-cigarettes and anxiety (OR = 1.45, S.E. = 0.17, 95% CI = 1.04, 2.03) and depression (OR = 0.77, S.E. = 0.11, 95% CI = 0.62, 0.96) significantly predicted current e-cigarette use. Anxiety (OR = 0.61, S.E. = 0.03, 95% CI = 0.57, 0.65), and depression (OR = 5.33, S.E. = 0.06, 95% CI = 4.74, 6.0) interactions with intentions to use e-cigarettes significantly predicted using e-cigarettes to consume cannabis. Interactions between intended length of time for future e-cigarette use and anxiety (OR = 0.14, S.E. = 0.18, 95% CI = 0.10, 0.19), depression (OR = 3.74, S.E. = 0.16, 95% CI = 2.74, 5.1), and loneliness (OR = 0.37, S.E. = 0.09, 95% CI = 0.31, 0.44) to predict current cigarette use. No interactions between psychological distress factors and intended length of time for future e-cigarette use predicted e-cigarette use. Depression (OR = 0.15, S.E. = 0.55, 95% CI = 0.05, 0.45) significantly interacted with intended length of time for future e-cigarette use in predicting e-cigarette use to consume cannabis.
Discussion
The overarching aim of this paper was to illuminate the role of intentions and psychological distress (i.e., anxiety, depression, loneliness, and stress) on cigarette and e-cigarette use during the beginning of the COVID-19 pandemic. Specifically, this study examined associations between intentions to use e-cigarettes, psychological distress, and cigarette use, e-cigarette use, and the use of e-cigarettes to consume cannabis among young adults.
H1
E-cigarette use will be higher than cigarette use, and both will be highest among men.
Results provide partial support for hypothesis 1. Prevalence of ever having smoked a cigarette was significantly lower than the prevalence of ever having used an e-cigarette among the overall sample. However, current use of cigarettes and e-cigarettes were equal in prevalence. Additionally, consistent with hypothesis 1, cigarette smoking and dual usage of e-cigarettes and cigarettes among males was significantly higher than females. Yet, contrary to previous reports of higher prevalence of e-cigarette use among male youth [56, 57], e-cigarette use was higher among females. Gender differences in e-cigarette use are often driven by various factors such as perceived stress, in that, the association of perceived stress with tobacco product use is higher among females than males [58]. The role of stress as an underlying mechanism of e-cigarette use among females is particularly relevant to this study as female participants reported significantly higher stress than males. Psychological distress differences, along with other factors (e.g., reinforcement of e-cigarette use among females through sensory appeal of flavor preferences [59]) may partially explain the higher prevalence of e-cigarette use among females during the early pandemic timeline.
H2
Intentions to use e-cigarettes will be highest among dual users and cannabis vapers.
Results partially supported hypothesis 2. Although dual users did not significantly differ in their intentions to use e-cigarettes from exclusive e-cigarette users, both groups as well as cannabis vapers reported higher intentions to use e-cigarettes than exclusive cigarette users. Perhaps cigarette and e-cigarette users have established their preferred method of smoking or vaping with no inclination to switch methods. For example, some e-cigarette users have reported a difficult adjustment period when switching from smoking to vaping due to various barriers (i.e., lack of knowledge regarding the technical aspects of vaping products) [60], which may dissuade switching methods. More importantly, dual users of cigarettes and e-cigarettes report significantly longer-term intentions to use e-cigarettes in the future, suggesting they are the least likely to attempt to quit in the near future. This is a particular concern during the COVID-19 pandemic as dual users may be the most vulnerable to negative outcomes from COVID-19 exposure [3].
Although cannabis consumption facilitates e-cigarette use it does not appear to be the strongest correlate of e-cigarette use. This may be because cannabis vapers had higher intentions to use e-cigarettes than cigarette smokers and abstainers, but lower intentions than exclusive e-cigarette and dual users. Perhaps the various options available for cannabis consumption (i.e., inhalation, oral ingestion, topical) influence intentions of vaping cannabis among cannabis consumers and may reflect preferences in the method of cannabis consumption. In fact, cannabis delivery method preferences among young adults are wide ranging (e.g., hollowed-out cigars filled with marijuana known as a “blunt” [61], bongs, vaporizers, and edibles [62]). Despite not having the highest intentions to use e-cigarettes, cannabis users are still a major population of concern during the pandemic because cannabis use has been correlated with COVID-19 hospitalization due to shared genetic underpinnings [63].
H3
E-cigarette use intentions will be associated with cigarette and vaping behaviors.
Results provide support for hypothesis 3. Intentions were significant predictors of cigarette, e-cigarette, and dual usage among females. Previous studies have found an association between e-cigarette use and cigarette smoking [27,28,29]. This study findings demonstrate this association through the underlying mechanism of intentions. Moreover, both intentions to use e-cigarettes and intended length of time for future e-cigarette use predicted dual usage of cigarette and e-cigarettes among females. Previous research has indicated that e-cigarette users who are non-cigarette smokers report high intentions to smoke cigarettes compared with their counterparts who had never used e-cigarettes [64], suggesting an association between e-cigarette use and cigarette smoking. Results from this study further illuminate the role of intentions, specific to e-cigarettes, which appear to influence cigarette smoking behaviors as well. Intentions to use e-cigarettes, as well as factors that encourage these intentions, may increase the risk of both e-cigarette use and cigarette smoking among young adults who are not current cigarette smokers. Although intentions did not significantly predict e-cigarette use among males, other facets of intentions not studied here may influence e-cigarette use among this population (e.g., intentions regarding the frequency or type of e-cigarette). It is important to understand how different facets of intentions to use e-cigarettes (i.e., intentions to use, length of time, frequency) predict e-cigarette and cigarette use as it may help identify youth who are the most vulnerable to vaping and smoking behaviors.
Furthermore, intentions to use e-cigarettes predicted cannabis vaping among females. Among males, intentions to use e-cigarettes and length of time for future intention to use e-cigarettes predicted cannabis vaping. These results clarify the gender differences in specific types of intentions that influence e-cigarette use for cannabis consumption. In line with previous research that shows females and males differ in their primary forms of cannabis use (e.g., edibles, blunts) [62], these results clarify the nuanced gender differences in factors that influence e-cigarette use for cannabis consumption. The link between cannabis use, vaping, and COVID-19 outcomes [21] may suggest a need for emphasis on cannabis vaping individuals and those with intentions to use e-cigarettes to be identified as high risk for negative COVID-19 outcomes.
H4
Psychological distress will be positively associated with smoking, e-cigarette use, and cannabis vaping by interacting with intentions.
Rates of cigarette and e-cigarette use at the beginning of the pandemic appear to be, at least partially, influenced by psychological distress. Anxiety, depression, loneliness, and stress predicted intentions to use e-cigarettes as well as intended length of time for future e-cigarette use. Among other factors, psychological distress is positively associated with cigarette and e-cigarette use [65,66,67,68]. Findings from this study reveal that the influence of psychological distress applies to cannabis vaping as well as cigarette and e-cigarette use by way of intentions to use e-cigarettes. These findings may clarify reports that most young adults did not decrease their substance use (i.e., marijuana use) amid the pandemic [69], perhaps, in part, because of higher psychological distress. The association between psychological distress and e-cigarette use found in this study are further supported by the higher prevalence of anxiety, depression, loneliness, and stress reported among smokers and e-cigarette users than abstainers. Also, results revealed that females are more likely to report using e-cigarettes as well as using e-cigarettes to consume cannabis than their male counterparts. Gender differences in psychological distress may partially explain the higher likelihood of e-cigarette and cannabis vaping among females as they also reported significantly higher levels of psychological distress than males.
Previous work along with this study’s results suggest a bi-directional, and harmful, relationship between psychological distress and cannabis vaping. For example, results in this study reveal that depression is associated with e-cigarette use to consume cannabis. Moreover, past studies indicate that the use of cannabis, vaping, or other tetrahydrocannabinol (THC) products may carry unique risks for those “self-medicating” and make depression worse [70]. Thus, psychological distress may both facilitate cannabis vaping behaviors and exacerbate the use of e-cigarettes to consume cannabis. Furthermore, most young adult cannabis vapers did not change use during the early pandemic [71]. A lack of change in cannabis vaping may be due to psychological distress as suggested by this study’s results.
Finally, intentions related to e-cigarette use significantly interacted with psychological distress factors, and subsequently related to a higher likelihood of cigarette smoking, vaping and cannabis vaping. Intentions to use e-cigarettes appears to strengthen the association between psychological distress and smoking and vaping behaviors, particularly among females. In fact, cigarette smokers, e-cigarette users, dual users, and cannabis vapers reported higher anxiety, depression, stress, and loneliness than their abstaining counterparts. Smokers with psychological distress have previously been found to report higher intentions to switch to electronic cigarettes as a method to quit smoking [72]. The results of this study further clarify this relationship by demonstrating that psychological distress interacts with various types of intentions to use e-cigarettes which may not be directly related to smoking cessation. Moreover, psychological distress may increase the likelihood of vaping cannabis which may subsequently increase risk of negative COVID-19 outcomes. Also, the results of this study suggest that intentions to use e-cigarettes are related to a higher likelihood of cigarette smoking. Thus, psychological distress among non-current cigarette smokers may place them at higher risk to begin cigarette smoking if they have intentions to use vaping products. This is a particular concern as the pandemic’s impact continues and facilitates persistent elevated symptoms of psychological distress (e.g., depression [73]) which may continue to influence smoking and vaping behaviors.
The influence of psychological distress on smoking and vaping behaviors may not be unique to the pandemic. However, this study’s results show that this association is significantly present for young adults during the early months of the pandemic. Moreover, the influence of psychological distress on smoking and vaping behaviors is likely to interact with intentions to use e-cigarettes. Thus, individuals who have intentions to use e-cigarettes or to continue using e-cigarettes for a longer period of time if already using them are more likely to use e-cigarettes and possibly cigarettes as well when experiencing various types of psychological distress, including anxiety, depression, loneliness, and stress. In addition to typical negative outcome concerns of smoking and vaping behaviors (e.g., exposure to harmful carcinogens and other cancer inducing chemicals), the ongoing COVID-19 pandemic makes these individuals more vulnerable to negative health outcomes.
Limitations
Although two types of intentions for e-cigarette use (i.e., intentions to use and length of time for future use) were examined, intentions for smoking cigarettes were not measured and, therefore, comparisons of intentions for cigarette and e-cigarette use could not be conducted. Additionally, psychological distress measures were single-item assessments which does not allow assessment of the severity. Also, psychological distress measures were not specific to the COVID-19 pandemic, nor did the study measure the use of e-cigarettes to relieve depression and loneliness. This limits the ability to assess whether psychological distress was directly related to concerns of the pandemic and whether e-cigarette use was intended for the relief of all psychological distress factors. It is unclear if documented increase in psychological distress [74,75,76] experienced by U.S. young adults is directly related to the pandemic and if there is an underlying mechanism of fear for COVID-19 risk among those who smoke cigarettes or use e-cigarettes.
Future research
Future research should examine multiple types of intentions for substance use such as frequency and purpose (e.g., to quit other substance use behaviors or to self-medicate against psychological distress). Examining behavioral intentions as a multi-faceted factor of substance use can clarify the underlying mechanisms of smoking and vaping behaviors as well as better identify at-risk individuals. Also, future work should endeavor to examine whether intentions influence various forms of cannabis consumption that do not rely on e-cigarettes to clarify whether this association is based on cannabis use itself or the delivery method.
Smoking relapse rates among young adults and those who recently have attempted to abstain is typically high [77]. Reduced availability of cessation programming (e.g., access to helplines, cessation clinics, face-to-face support, and appointments with general practitioners) during the pandemic may have further hindered efforts and success at smoking cessation [78]. Future work should examine if increased psychological distress experienced during the pandemic has influenced relapse rates.
Conclusions
Reducing smoking and vaping behaviors has become more important than ever since the pandemic began due to the increased risk of COVID-19 outcomes. According to results from this study, two factors that may provide guidance for better targeting interventions are psychological distress and intentions. In fact, a significant change in intentions can lead to behavioral change [79]. In addition, providing better mental health support among young adults may subsequently reduce cigarette and e-cigarette use. Yet, the pandemic led to reduced availability of resources for smoking cessation efforts [78] and healthier options for coping with psychological distress. Public health efforts that provide alternative positive coping strategies such as exercise and meditation may help decrease reliance on e-cigarettes for psychological distress management. Increased public resources for psychological services and smoking cessation should focus on young adult populations.
Finally, curbing excessive cannabis use may mitigate the impact of COVID-19. Intervention efforts aimed at reducing cannabis vaping behaviors may partially result in a reduction of cannabis use. However, because cannabis is often used to deal with psychological distress, reducing availability of cannabis may unintentionally result in other negative coping strategies such as cigarette smoking. Thus, efforts to reduce vaping and smoking behaviors must balance the need for interventions that help young people develop healthy and effective coping skills that do not unintentionally have negative impact on other psychosocial outcomes such as psychological distress.
Availability of data and materials
The datasets generated during the current study are not publicly available due to concerns of confidentiality concerns and the sensitive nature of information collected but are available from the corresponding author on reasonable request.
References
Creamer MR, Wang TW, Babb S, Cullen KA, Day H, Willis G, Jamal A, Neff L. Tobacco product use and cessation indicators among adults—United States, 2018. Morb Mortal Wkly Rep. 2019;68(45):1013.
Mirbolouk M, Charkhchi P, Kianoush S, Uddin SI, Orimoloye OA, Jaber R, Bhatnagar A, Benjamin EJ, Hall ME, DeFilippis AP, Maziak W. Prevalence and distribution of e-cigarette use among US adults: behavioral risk factor surveillance system, 2016. Ann Intern Med. 2018;169(7):429–38.
Gaiha SM, Cheng J, Halpern-Felsher B. Association between youth smoking, electronic cigarette use, and COVID-19. J Adolesc Health. 2020;67(4):519–23.
Hopkinson NS, Rossi N, El-Sayed Moustafa J, Laverty AA, Quint JK, Freidin M, Visconti A, Murray B, Modat M, Ourselin S, Small K. Current smoking and COVID-19 risk: results from a population symptom app in over 2.4 million people. Thorax. 2021;76(7):714–22.
Neira DP, Watts A, Seashore J, Polychronopoulou E, Kuo YF, Sharma G. Smoking and risk of COVID-19 hospitalization. Respir Med. 2021;1(182): 106414.
Breslau J, Finucane ML, Locker AR, Baird MD, Roth EA, Collins RL. A longitudinal study of psychological distress in the United States before and during the COVID-19 pandemic. Prev Med. 2021;1(143):106362.
Zhang H, Rostami MR, Leopold PL, Mezey JG, O’Beirne SL, Strulovici-Barel Y, Crystal RG. Expression of the SARS-CoV-2 ACE2 receptor in the human airway epithelium. Am J Respir Crit Care Med. 2020;202(2):219–29.
Lowe KE, Zein J, Hatipoğlu U, Attaway A. Association of smoking and cumulative pack-year exposure with COVID-19 outcomes in the Cleveland Clinic COVID-19 Registry. JAMA Intern Med. 2021;181(5):709–11.
Gebhard C, Regitz-Zagrosek V, Neuhauser HK, Morgan R, Klein SL. Impact of sex and gender on COVID-19 outcomes in Europe. Biol Sex Differ. 2020;11(1):1–3.
Gomez JM, Du-Fay-de-Lavallaz JM, Fugar S, Sarau A, Simmons JA, Clark B, Sanghani RM, Aggarwal NT, Williams KA, Doukky R, Volgman AS. Sex differences in COVID-19 hospitalization and mortality. J Womens Health. 2021;30(5):646–53.
Naidu V, Zeki AA, Sharma P. Sex differences in the induction of angiotensin converting enzyme 2 (ACE-2) in mouse lungs after e-cigarette vapor exposure and its relevance to COVID-19. J Investig Med. 2021;69(5):954–61.
Galiatsatos P. Johns Hopkins Medicine [Internet]. [cited 2021, July 16]. Coronavirus: smoking, vaping, wildfire smoke and air pollution. https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-smoking-vaping-wildfire-smoke-and-air-pollution
King BA, Jones CM, Baldwin GT, Briss PA. The EVALI and youth vaping epidemics—implications for public health. N Engl J Med. 2020;382(8):689–91.
Murthy VH. E-cigarette use among youth and young adults: a major public health concern. JAMA Pediatr. 2017;171(3):209–10.
Walley SC, Wilson KM, Winickoff JP, Groner J. A public health crisis: electronic cigarettes, vape, and JUUL. Pediatrics. 2019;143(6):e20182741.
Thatcher A. E-cigarettes more popular than tobacco among youth. Can Med Assoc J. 2015;187:6.
Choi K, Fabian L, Mottey N, Corbett A, Forster J. Young adults’ favorable perceptions of snus, dissolvable tobacco products, and electronic cigarettes: findings from a focus group study. Am J Public Health. 2012;102(11):2088–93.
Hecht SS. Lung carcinogenesis by tobacco smoke. Int J Cancer. 2012;131(12):2724–32.
Morean ME, Lipshie N, Josephson M, Foster D. Predictors of adult e-cigarette users vaporizing cannabis using e-cigarettes and vape-pens. Subst Use Misuse. 2017;52(8):974–81.
Jones CB, Hill ML, Pardini DA, Meier MH. Prevalence and correlates of vaping cannabis in a sample of young adults. Psychol Addict Behav. 2016;30(8):915.
Merianos AL, Russell AM, Mahabee-Gittens EM, Barry AE, Yang M, Lin HC. Concurrent use of e-cigarettes and cannabis and associated COVID-19 symptoms, testing, and diagnosis among student e-cigarette users at four US Universities. Addict Behav. 2022;1(126):107170.
Ajzen I. From intentions to actions: a theory of planned behavior. In: Action control 1985. Berlin: Springer; 1985. p. 11–39.
Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211.
Rise J, Kovac V, Kraft P, Moan IS. Predicting the intention to quit smoking and quitting behaviour: extending the theory of planned behaviour. Br J Health Psychol. 2008;13(2):291–310.
Wakefield M, Kloska DD, O’Malley PM, Johnston LD, Chaloupka F, Pierce J, Giovino G, Ruel E, Flay BR. The role of smoking intentions in predicting future smoking among youth: findings from monitoring the future data. Addiction. 2004;99(7):914–22.
Alber JM, Ganjooi K, Gibbs S, Almeida R, Jackson LD. E-cigarette beliefs and intentions among US adults before and after EVALI outbreak. Am J Health Promot. 2021;35(8):1071–7.
Owotomo O, Stritzel H, McCabe SE, Boyd CJ, Maslowsky J. Smoking intention and progression from e-cigarette use to cigarette smoking. Pediatrics. 2020;146(6):e2020002881.
Moore GF, Littlecott HJ, Moore L, Ahmed N, Holliday J. E-cigarette use and intentions to smoke among 10–11-year-old never-smokers in Wales. Tob Control. 2016;25(2):147–52.
Zhong J, Cao S, Gong W, Fei F, Wang M. Electronic cigarettes use and intention to cigarette smoking among never-smoking adolescents and young adults: a meta-analysis. Int J Environ Res Public Health. 2016;13(5):465.
Dai H. Prevalence and factors associated with youth vaping cessation intention and quit attempts. Pediatrics. 2021;148(3):e2021050164.
Caponnetto P, Inguscio L, Saitta C, Maglia M, Benfatto F, Polosa R. Smoking behavior and psychological dynamics during COVID-19 social distancing and stay-at-home policies: a survey. Health psychology research. 2020;8(1).
Dunn M. College student's behavior, health beliefs, norms, and intentions to use e-cigarettes. Am J Health Stud. 2015;30(3). https://doi.org/10.47779/ajhs.2015.176
Patiño-Masó J, Font-Mayolas S, Salamó A, Arboix M, Sullman MJ, Gras ME. Predictors of intentions to use cigarettes and electronic-cigarettes among high school students. J Multidiscip Healthc. 2019;12:591.
Cuccia AF, Patel M, Amato MS, Stephens DK, Yoon SN, Vallone DM. Quitting e-cigarettes: Quit attempts and quit intentions among youth and young adults. Preventive medicine reports. 2021;1(21): 101287.
Siegel A, Korbman M, Erblich J. Direct and indirect effects of psychological distress on stress-induced smoking. J Stud Alcohol Drugs. 2017;78(6):930–7.
Czeisler MÉ, Lane RI, Petrosky E, Wiley JF, Christensen A, Njai R, Weaver MD, Robbins R, Facer-Childs ER, Barger LK, Czeisler CA. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic—United States, June 24–30, 2020. Morb Mortal Wkly Rep. 2020;69(32):1049.
Twenge JM, Joiner TE. Mental distress among US adults during the COVID-19 pandemic. J Clin Psychol. 2020;76(12):2170–82.
Finch LE, Hawkley L, Krummenacher CI, Stripp S, Sterrett D, Smith TW. Age differences in mental health from May through August 2020 among US adults: trajectories and the role of pandemic, lifestyle, and social factors. Aging Ment Health. 2022;11:1–9.
Guerrini CJ, Schneider SC, Guzick AG, Amos Nwankwo GN, Canfield I, Fedson S, Gutierrez AM, Sheu JC, Song AY, Villagran AM, McGuire AL. Psychological distress among the US general population during the COVID-19 pandemic. Front Psychiatry. 2021;22(12):810.
McGinty EE, Presskreischer R, Han H, Barry CL. Trends in psychological distress among us adults during different phases of the COVID-19 pandemic. JAMA Netw Open. 2022;5(1):e2144776.
Gaiha SM, Lempert LK, Halpern-Felsher B. Underage youth and young adult e-cigarette use and access before and during the coronavirus disease 2019 pandemic. JAMA Netw Open. 2020;3(12):e2027572.
Park-Lee E, Ren C, Sawdey MD, Gentzke AS, Cornelius M, Jamal A, Cullen KA. Notes from the field: e-cigarette use among middle and high school students—National Youth Tobacco Survey, United States, 2021. Morb Mortal Wkly Rep. 2021;70(39):1387.
White AM, Li D, Snell LM, O’Connor R, Hoetger C, Croft D, Lester RC, McIntosh S, Underwood M, Schneller L, Breland A. Perceptions of tobacco product-specific COVID-19 risk and changes in tobacco use behaviors among smokers, e-cigarette users, and dual users. Nicotine Tob Res. 2021;23(9):1617–22.
Kreslake JM, Diaz MC, Shinaba M, Vallone DM, Hair EC. Youth and young adult risk perceptions and behaviours in response to an outbreak of e-cigarette/vaping-associated lung injury (EVALI) in the USA. Tob Control. 2022;31(1):88–97.
Lin H, Chen M, Yun Q, Zhang L, Chang C. Tobacco dependence affects determinants related to quitting intention and behaviour. Sci Rep. 2021;11(1):1–8.
Gallo LC, Roesch SC, Fortmann AL, Carnethon MR, Penedo FJ, Perreira K, Birnbaum-Weitzman O, Wassertheil-Smoller S, Castañeda SF, Talavera GA, Sotres-Alvarez D. Associations of chronic stress burden, perceived stress, and traumatic stress with cardiovascular disease prevalence and risk factors in the HCHS/SOL Sociocultural Ancillary Study. Psychosom Med. 2014;76(6):468.
Long D. Smoking as a coping strategy. Nurs Times. 2003;99(33):50–3.
Slopen N, Kontos EZ, Ryff CD, Ayanian JZ, Albert MA, Williams DR. Psychosocial stress and cigarette smoking persistence, cessation, and relapse over 9–10 years: a prospective study of middle-aged adults in the United States. Cancer Causes Control. 2013;24(10):1849–63.
Napolitano MA, Lynch SB, Stanton CA. Young adult e-cigarette users: perceptions of stress, body image, and weight control. Eat Weight Disord Stud Anorex Bulim Obes. 2020;25(2):487–95.
Dyal SR, Valente TW. A systematic review of loneliness and smoking: small effects, big implications. Subst Use Misuse. 2015;50(13):1697–716.
Gentina E, Kilic D, Dancoine PF. Distinctive role of opinion leaders in the social networks of school adolescents: an investigation of e-cigarette use. Public Health. 2017;1(144):109–16.
Piirtola M, Kaprio J, Baker TB, Piasecki TM, Piper ME, Korhonen T. The associations of smoking dependence motives with depression among daily smokers. Addiction. 2021;116(8):2162–74.
Mathew AR, Hogarth L, Leventhal AM, Cook JW, Hitsman B. Cigarette smoking and depression comorbidity: systematic review and proposed theoretical model. Addiction. 2017;112(3):401–12.
National Institute on Drug Abuse (NIDA) [Internet] [cited 2021, April 12). Are there gender differences in tobacco smoking? https://www.drugabuse.gov/publications/research-reports/tobacco-nicotine-e-cigarettes/are-there-gender-differences-in-tobacco-smoking on 2021, December 4
Ahmad F, Jhajj AK, Stewart DE, Burghardt M, Bierman AS. Single item measures of self-rated mental health: a scoping review. BMC Health Serv Res. 2014;14(1):1–1.
Kong G, Kuguru KE, Krishnan-Sarin S. Gender differences in US adolescent e-cigarette use. Curr Addict Rep. 2017;4(4):422–30.
Ramo DE, Young-Wolff KC, Prochaska JJ. Prevalence and correlates of electronic-cigarette use in young adults: findings from three studies over five years. Addict Behav. 2015;1(41):142–7.
Leventhal AM, Urman R, Barrington-Trimis JL, Goldenson NI, Gallegos K, Chou CP, Wang K, Berhane K, Cruz TB, Pentz MA, Unger J. Perceived stress and poly-tobacco product use across adolescence: Patterns of association and gender differences. J Psychiatr Res. 2017;1(94):172–9.
Pang RD, Goldenson NI, Kirkpatrick M, Barrington-Trimis JL, Cho J, Leventhal AM. Sex differences in the appeal of flavored e-cigarettes among young adult e-cigarette users. Psychol Addict Behav. 2020;34(2):303.
Morphett K, Weier M, Borland R, Yong HH, Gartner C. Barriers and facilitators to switching from smoking to vaping: Advice from vapers. Drug Alcohol Rev. 2019;38(3):234–43.
Lee JP, Battle RS, Lipton R, Soller B. ‘Smoking’: use of cigarettes, cigars and blunts among Southeast Asian American youth and young adults. Health Educ Res. 2010;25(1):83–96.
Huffer MC, Cservenka A. Effects of age and sex on primary form and method of cannabis use. J Subst Use. 2021;26(5):505–10.
Hatoum AS, Morrison CL, Colbert SM, Winiger EA, Johnson EC, Agrawal A, Bogdan R. Genetic liability to cannabis use disorder and COVID-19 hospitalization. Biological psychiatry global open science. 2021;1(4):317–23.
Park JY, Seo DC, Lin HC. E-cigarette use and intention to initiate or quit smoking among US youths. Am J Public Health. 2016;106(4):672–8.
Hwang J, Yun ZS. Mechanism of psychological distress-driven smoking addiction behavior. J Bus Res. 2015;68(10):2189–97.
Kiviniemi MT, Orom H, Giovino GA. Psychological distress and smoking behavior: the nature of the relation differs by race/ethnicity. Nicotine Tob Res. 2011;13(2):113–9.
McGinty EE, Presskreischer R, Han H, Barry CL. Psychological distress and loneliness reported by US adults in 2018 and April 2020. JAMA. 2020;324(1):93–4.
Park SH, Lee L, Shearston JA, Weitzman M. Patterns of electronic cigarette use and level of psychological distress. PLoS ONE. 2017;12(3):e0173625.
Clendennen SL, Case KR, Sumbe A, Mantey DS, Mason EJ, Harrell MB. Stress, Dependence, and COVID-19–related Changes in past 30-day Marijuana, electronic cigarette, and cigarette use among youth and young adults. Tobacco Use Insights. 2021. https://doi.org/10.1177/1179173X211067439.
Saeed OB, Chavan B, Haile ZT. Association between e-cigarette use and depression in US adults. J Addict Med. 2020;14(5):393–400.
Nguyen N, Gaiha SM, Halpern-Felsher B. Self-reported changes in cannabis vaping among US adolescents and young adults early in the COVID-19 pandemic. Prev Med Rep. 2021;1(24):101654.
Yang B, Spears CA, Popova L. Psychological distress and responses to comparative risk messages about electronic and combusted cigarettes. Addict Behav. 2019;1(91):141–8.
Ettman CK, Cohen GH, Abdalla SM, Sampson L, Trinquart L, Castrucci BC, Bork RH, Clark MA, Wilson I, Vivier PM, Galea S. Persistent depressive symptoms during COVID-19: a national, population-representative, longitudinal study of US adults. Lancet Reg Health Am. 2022;1(5):100091.
Kikuchi H, Machida M, Nakamura I, Saito R, Odagiri Y, Kojima T, Watanabe H, Fukui K, Inoue S. Changes in psychological distress during the COVID-19 pandemic in Japan: a longitudinal study. J Epidemiol. 2020;30(11):522–8.
Lorant V, Smith P, Van den Broeck K, Nicaise P. Psychological distress associated with the COVID-19 pandemic and suppression measures during the first wave in Belgium. BMC Psychiatry. 2021;21(1):1.
Wang Y, Fu P, Li J, Jing Z, Wang Q, Zhao D, Zhou C. Changes in psychological distress before and during the COVID-19 pandemic among older adults: the contribution of frailty transitions and multimorbidity. Age Ageing. 2021;50(4):1011–8.
Alboksmaty A, Agaku IT, Odani S, Filippidis FT. Prevalence and determinants of cigarette smoking relapse among US adult smokers: a longitudinal study. BMJ Open. 2019;9(11):e031676.
Cessat TP. Pandemic fans the flames of smoking and health inequity. Tob Induc Dis. 2021;19:9.
Webb TL, Sheeran P. Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychol Bull. 2006;132(2):249.
Acknowledgements
Not applicable.
Funding
This study has no funding to report.
Author information
Authors and Affiliations
Contributions
The sole author was the principal investigator of the study, analyzed, and wrote all portions of the manuscript.The author read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Approval for the study was obtained prior to data collection from Occidental College’s Human Subjects Research Review Committee (HSRRC-IRB). Federalwide Assurance (FWA) number is: FWA00005302. Informed consent was obtained from all participants at the start of the study. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The author has no competing interests to report.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cabral, P. E-cigarette use and intentions related to psychological distress among cigarette, e-cigarette, and cannabis vape users during the start of the COVID-19 pandemic. BMC Psychol 10, 201 (2022). https://doi.org/10.1186/s40359-022-00910-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-022-00910-9