
Abstract
Background
Adolescence and young adulthood is a high-risk period for the development of eating disorders. In recent years, there has been an increase in use of technology-based interventions (TBIs) for the treatment of eating disorders. The objective of this study was to determine the types of technology used for eating disorder treatment in youth and their effectiveness.
Methods
A scoping review was conducted according to PRISMA-ScR guidelines. Four databases were searched. Eligible articles included: (1) a TBI (2) participants with a mean age between 10- and 25-years and meeting DSM-IV or DSM-5 criteria for any eating disorder and (3) qualitative or quantitative designs. Quantitative and qualitative studies were assessed for quality.
Results
The search identified 1621 articles. After screening of titles and abstracts, 130 articles were read in full and assessed for eligibility by two raters. Forty-nine (29 quantitative and 20 qualitative, observational, or mixed methods studies) met inclusion criteria. Quality ratings indicated that 78% of quantitative studies had a low risk of bias and 22% had a moderate risk. Technologies reviewed in our study included videoconference therapy, mobile applications, and online self-help. We considered interventions used both within sessions with clinicians as well as those used in between sessions by patients alone. Fifteen of 18 (83%) quantitative studies found that TBIs reduce eating disorder symptomatology, with nine of those reporting medium-to-large effect sizes. Qualitative data was of high quality and suggested that virtual interventions are acceptable in this population.
Conclusions
Although identified studies are of high quality, they are limited in number. More research is needed, particularly regarding videoconferencing and mobile applications. Nonetheless, TBIs show promise for the treatment of eating disorders in youth.
Trial registration: Not applicable.
Plain English summary
The use of virtual care to treat adolescents and young adults with eating disorders has increased in recent years. To better understand what types of technologies are being used in virtual care and these technologies’ effectiveness, we systematically reviewed research studies that discussed the use of any technology to treat youth (which was defined as young people aged 25 years or under) with an eating disorder. We found 49 relevant studies. They revealed that videoconference therapy, mobile applications, and online self-help are most frequently used for virtual treatment. Of the 18 studies evaluating the effectiveness of these technologies, 15 found virtual care to be effective for reducing eating disorder symptoms. Studies describing patient experiences with these technologies, of which there were nine, suggested that patients overall were satisfied with receiving virtual care. Although these results are promising, research on virtual treatment is still lacking, especially on videoconferencing therapy and mobile applications.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Eating disorders (EDs) affect individuals of all ages, but adolescents are particularly at risk of developing EDs during this critical period of their development [1]. Evidence-based treatments such as family-based treatment (FBT) and cognitive behavioral therapy (CBT) are effective in reducing ED symptoms and promoting recovery in youth with EDs [2, 3]. However, it has been suggested that many children, adolescents, and young adults (hereafter referred to as “youth”) meeting criteria for an ED may not receive these effective therapies for a number of reasons, including limited treatment seeking behaviour [4,5,6], limited access to specialized care, and stigma surrounding the illness and treatments, among others [7]. More specifically, lack of provider training as well as limited capacity to provide individual and family therapy to comply with the demand of services contribute to limited access to specialized ED care [7].
In recent years, virtual interventions have become increasingly common, albeit mostly in a research context. The types of virtual treatment in place for EDs are varied and include the delivery of therapy remotely in real-time (e.g., videoconferencing), the provision of support between therapy sessions (e.g., email, texting, instant messaging), and self-help and self-monitoring interventions (e.g., internet self-help, internet-based CBT (iCBT), smartphone applications, etc.), each of which can be used alone or in combination [8, 9].
Several reviews have summarized and evaluated the evidence for psychological interventions delivered virtually for the treatment of EDs. A review on Technology-Based Interventions (TBIs) for EDs from 2013 [10] concluded that internet-based treatments are superior to waitlists for reducing ED symptoms. However, these results cannot be generalized to youth and adolescents as only one included study (of 21 studies in total) involved females in this age category. Additionally, no studies on therapy delivered via videoconferencing could be included. Given the increasing ubiquity of this modality, a new review may be warranted. A 2015 review [11] had similar conclusions but similarly included only a limited number of studies carried out exclusively in youth meeting threshold for ED diagnoses.
An updated review published in 2016 [12] suggested that iCBT and guided self-help reduced ED psychopathology, that virtual interventions may help to reach underserved populations and improve access to care, and that smartphone apps are increasingly popular but still have unknown clinical effectiveness. These results may also be somewhat difficult to generalize to youth in particular, as the review does not systematically include and focus on a specific participant age range. Though another informative and more recent paper was published in 2020 [13], studies published during the COVID-19 pandemic have not been reviewed. Furthermore, the 2020 review was not youth-specific and focused solely on RCTs, which are important for understanding effectiveness but may provide limited information about patient experience with TBIs. Additionally, reviews to date do not clearly address the extent to which interventions are delivered in a hybrid or fully online format.
More recently, the COVID-19 pandemic has brought new challenges for individuals with EDs and their care, including difficulties in accessing timely medical and psychological care due to limited services and increased demand [14]. The new constraints have led to a rapid shift to virtual care for many ED treatment programs [15, 16] and forced clinicians to rapidly adapt their methods to maintain services. The first few studies describing online adaptations made to ED care in the context of the COVID pandemic indicated general acceptability by individuals with EDs and their families as well as the overall usefulness of telemedicine [15,16,17,18]. This transition has shed new light on the use of TBIs and their potential benefits for ED treatment [15, 18], including increasing access to treatment, which will remain pertinent even after the COVID-19 pandemic.
Given the rapid changes and improvements made to virtual care modalities for EDs in the past decade, there is a pressing need for current and comprehensive studies to guide and inform clinicians in the adoption of TBIs for youth with EDs. The aim of the present study was to update existing reviews [10,11,12,13] by presenting a scoping review of research on TBIs for youth with EDs. Specifically, the objectives of this scoping review were to describe the extent to which different types of technologies have been implemented in the treatment of individuals meeting clinical diagnostic criteria for EDs, including hybrid and fully online treatments and to review the effectiveness of such interventions.
Methods
Search strategy
A protocol was developed but was not registered. A literature search was conducted between June 18, 2021 and February 9, 2022 using the following databases: Medline, PubMed, PsychINFO, and Google Scholar. The reference lists of relevant articles were also examined to extract additional articles. We designed and conducted the searches on the above-mentioned databases for the last 10 years (2011–2021, used as a filter). This specific time frame was chosen with the rationale that technology used before 2011 might not be representative of what is available and commonly used in more recent years and other studies [10, 11] have already reviewed the literature published before this date. Searches consisted of a combination of keywords grouped into four categories which were combined with the “AND” function: (1) telemedicine OR telehealth OR telecare OR ehealth OR e-therapy OR internet-based OR online OR web-based OR smartphone OR text messaging OR mobile OR videoconferencing; (2) eating disorder OR anorexia OR bulimia; (3) adolescen* OR child* OR young adult* and; (4) intervention OR program OR trial OR therapy OR treatment OR psychotherapy OR self-help. Note that the search engines expanded the term “eating disorder” to all related feeding and eating disorders subtopics. All fields (e.g., titles, keywords, abstracts) were searched.
Selection process
We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA-ScR) guidelines for scoping reviews [19].
Screening 1: titles
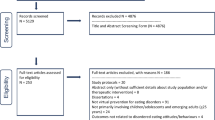
Once the records were generated from each database search, they were combined to remove duplicates. Two reviewers (RD and KN) then each screened half of the records using the titles only to determine if they were relevant or not. Titles that hinted at online interventions for EDs were retained and, to be conservative, titles that were vague were automatically moved to the next round of screening (abstract screening) (Fig. 1).

Search flow diagram
Screening 2: abstracts
To allow for further narrowing of the generated search records, a second screening based on abstracts was done using articles retained from screening 1. Two reviewers (RD and KN) then each screened half of the records based on their abstract. Abstracts that mentioned relevant elements of the eligibility criteria were retained for full-text review (Fig. 1).
Eligibility
The full texts of the remaining articles were extracted. To assess eligibility, the full text articles were independently read and rated on each of the criteria by the joint first authors of the paper (RD and KN). Discrepancies were discussed between the two reviewers. If consensus could not be reached, the two senior authors (NC and LB) made a final decision. This happened on five instances (e.g., study describing a new technology that is very different from other studies found).
Eligibility criteria were the following: (1) quantitative, qualitative, or descriptive studies published in English, French, Spanish, German, or Dutch; (2) including participants with a mean age between 10 and 25 years; (3) meeting DSM-IV or DSM-5 (or equivalent) criteria for any eating disorder, including diagnoses made using patient interviews or self-report questionnaires; (4) primarily examining TBIs (corresponding to online therapy, online support, or online self-help), and; (5) relevant to the research questions. The age cut-off of 25 years-old was based on clinical recommendations and treatment guidelines showing that the 18- to 25-year-old age group is distinct developmentally from older adults and present health disparities due to the transition from pediatric to adult health services that is often experienced during this period [20, 21]. Additionally, there is considerably less research focusing on the 10–18 years old group (n = 18 of 49 studies). Articles were excluded if: (1) they were published before 2011; (2) they constituted commentaries, editorials, or reviews and book chapters of studies already included, or: (3) they examined interventions addressing obesity or preventive interventions (e.g., in youth without a formal ED diagnosis). The decision to exclude studies evaluating early interventions in youth with pre-clinical/pre-diagnostic symptoms was made to facilitate the generalizability of our findings to clinical ED programs providing care to youth with a confirmed ED diagnosis. For studies using the same study sample, all relevant papers that met all criteria were retained in the full article count and Table 1, with only one being included in the quality assessment results. This was done to ensure full representation of the work done in this research area. Additionally, we made the decision a priori to include research protocols to provide the fullest understanding of the types of technology-based interventions used in the treatment of EDs in youth. This allowed us to potentially review and discuss new modalities for which no evidence yet exists but may be the object of future research.
Charting the data
The data charting process was carried out independently by the joint first authors of the paper (RD and KN), who each read and extracted information from half of the eligible articles. The reviewers each inputted data into a separate, dedicated spreadsheet which included the following categories: (1) sample characteristics, including: number of participants, age (mean, range, and standard deviation), race, ethnicity, socioeconomic status, and recruitment details; (2) study design; (3) a description of the intervention; (4) mode of delivery of the described intervention; (5) type of provider (e.g., psychiatrist, therapist, etc.); (6) outcome measures described in the article; (7) results, including primary and secondary outcomes in empirical studies and highlights from qualitative and descriptive studies, and; (8) key takeaways and conclusions from the study. When any of the above-mentioned information was not included in the publication, except when non-applicable due to the nature of the article/study, the corresponding author of the study was contacted by email for clarifications or to obtain the necessary results.
Quality assessment
A critical appraisal was carried out for quantitative and qualitative studies in order to describe the quality of the evidence included in the review. Quality ratings were not used as an eligibility criterion, as the goal of the review was to describe the widest array of studies on this topic and studies were discussed narratively. For quantitative studies, a 19-item tool adapted from Greenhalgh and Brown [67] and Higgins et al. [68] was used because it fit best with the heterogeneity of methods described in the studies. Two unblinded reviewers (RD and KN) independently assessed the articles on each item using “yes”, “no”, “not reported”, or “non-applicable”. For qualitative studies, the 10-item Critical Appraisal Skills Programme [69] checklist was used. The same unblinded reviewers independently assessed the articles on each item using “yes,” “no,” or “can’t tell.” For both the quantitative and qualitative studies, disagreements were discussed between the two reviewers until consensus was reached (see Additional file 1: Fig. S1 and Additional file 2: Fig. S2 for final ratings). Note that we did not conduct a quality assessment for observational/descriptive studies, as there was too much variability in their methodology.
Synthesis of results
Data pertaining to articles describing intervention trials with quantitative results were compiled and placed into a table for data presentation. Those articles were analyzed based on mode of delivery of the intervention and virtual versus hybrid (in-person and virtual) delivery to answer the main research questions, using available data measures such as effect sizes. The remaining articles were categorized into qualitative/mixed-methods studies, descriptions of adaptations to the COVID-19 pandemic, and new technologies that could potentially be used in the future in the treatment of EDs.
Results
Identification of studies and quality assessment
The searches from the four electronic databases and reference lists led to a total of 2173 records (Medline: 491, Pubmed: 732, PsychINFO: 291, Google Scholar: 625), which was then reduced to 1621 records after removal of duplicates. A total of 130 articles were retrieved in full-text and assessed for eligibility (see Fig. 1). Finally, 49 articles met full inclusion criteria and were included in the scoping review. Of these, 29 articles used quantitative methodologies to evaluate interventions, and these were prioritized for analysis of effectiveness. The remaining 20 studies, of which 12 were observational or descriptive and eight were mixed methods or qualitative studies, were described separately (see Table 1). Overall, most qualitative and mixed methods studies (7/8) can be considered of high quality (i.e., meeting at least 8/10 criteria) according to the critical appraisal checklist (see Additional file 2: Fig. S2). The remaining study met 6/10 criteria.
Of the quantitative articles describing intervention trials (n = 29), 18 included results, while 11 consisted of study protocols only. Note that we included these protocols on the basis that they had the potential of having a sample age that fit our inclusion criteria considering their target population. The 18 quantitative papers covered results from 14 intervention trials, with a few papers analyzing different results from the same trial. Overall, 78% (n = 14) of the 18 quantitative studies were qualified as high quality/low risk of bias, meaning that more than 10 out of 19 quality assessment criteria were met (i.e., “yes” or “partially yes”), and 22% (n = 4) were qualified as moderate to low quality/moderate to high risk of bias, meaning that fewer than 10 out of 19 criteria were met (see Additional file 1: Fig. S1). Of those four articles, only one study met fewer than seven criteria.
Virtual modalities were generally used to deliver primary (vs. adjunctive) treatment. We considered interventions used both within sessions with clinicians as well as those used in between sessions by patients alone. Our review found therapy delivered via videoconference, mobile applications, and internet self-help to be the most used and each of these, in addition to other technologies, are discussed separately below. However, these modalities have also been used as adjunct interventions to increase points of contact with therapists in between appointments via email, instant-messaging, text message, telephone, or automated messages. Of the 29 intervention studies reviewed and discussed in more detail below, 20 studies (69%) provided some type of supplemental virtual support. Email contact (or asynchronous messages within applications) was most frequent (n = 15 studies), followed by instant-messaging support (n = 5 studies), automated support (n = 5 studies), videoconference support (n = 2 studies), and text message support (n = 1 study).
Another important component of TBIs and treatment for EDs is whether the intervention was delivered fully online or was supplemented by in-person appointments, in what could be described as hybrid interventions. Table 2 summarizes evidence for hybrid and fully online interventions by modality. Overall, there are fewer interventions that are considered hybrid. Almost all internet self-help interventions (11/12) were fully online and most mobile app interventions were hybrid (5/7). Effect sizes were largest for fully online videoconferencing interventions.
Modes of delivery: quantitative studies
TBIs are reviewed below, based on the mode of delivery described in the study.
Videoconference platforms for delivery of therapy
Our search identified four articles [25, 29, 31, 56] on the use of videoconference technology for ED treatment. This included a pair of articles by Anderson et al. discussing an experimental protocol [56] and its subsequent results [25]. In all articles, the therapy provided via videoconference constituted the primary treatment, but there was variation in terms of the addition or not of in-person therapy sessions and in-person medical follow-ups.
Two of the studies [25, 31, 56] evaluated the use of videoconference for delivering FBT for individuals with anorexia nervosa (AN). One of these was a pilot, multicenter, randomized controlled trial (RCT) [31] comparing two methods for delivering FBT in a sample of 40 participants with AN (aged 12–18 years, mean 14.88 years), either via a videoconferencing platform, in which case the whole family of the adolescent participated, or via an online guided self-help program, in which case only the parents of adolescents participated. At the end of treatment, there was an overall improvement, regardless of treatment group, in ED psychopathology measured using the Eating Disorder Examination (EDE) interview Global score with a large effect size (d = 1.04). The change was similar in both treatment groups (videoconference: d = 1.03; guided self-help: d = 1.01). The second was an uncontrolled trial [25, 56] targeting adolescents (n = 10) aged 13–18 years (mean age = 16.1 years) with typical or atypical AN, consisting of 20 sessions of family-based treatment given over 6 months, during which time the therapist maintained contact with the treating pediatrician, who evaluated participants in-person. Participant weight (d = 0.53) and self-reported ED symptoms (d = 1.06) improved from baseline to end-of-treatment and moderate to large effect sizes were maintained at 6-month follow-up [25].
A third article described an uncontrolled trial by Giel et al. [29], evaluating a videoconference relapse prevention program based on the Maudsley Model of AN Treatment was evaluated. The intervention included an initial and final in-person therapy session and eight videoconference therapy sessions, given over a period of 4 months to participants (n = 16) with a mean age of 21.7 years (SD = 4.3) and a diagnosis of AN. Participants who completed the intervention (n = 12) showed significantly lower scores on the eating concerns subscale of the standardized eating disorder examination questionnaire (EDE-Q) post-intervention as compared to before. Though not statistically significant, effect sizes for BMI change (r = 0.50), body shape concerns subscale (r = 0.43), weight concerns subscale (r = 0.36), and global EDE-Q scores (r = 0.41) were medium to large.
Mobile apps
Mobile apps can be used in multiple ways for mental health interventions including as a supplement to treatment, as a self-help tool between appointments, or as a monitoring device following inpatient treatment [70]. We identified two studies which aimed to test the effectiveness of different app-based interventions.
One article described the TCApp mobile app. This app consists of features including self-records, food records, and thought records, monitoring, and instant messaging with the therapist. Anastasiadou et al. [24] conducted a multicentre RCT to compare the effectiveness of standard CBT augmented with TCApp to treatment as usual in participants with any ED diagnosis (n = 106, mean age = 18.06 years). The authors found no significant difference between the two groups on the EDE-Q global scale and subscales over time. Regardless of the treatment group, CBT reduced overall symptom severity with medium to large effect sizes (r range = 0.46–0.63) [24].
A second article described Recovery Record, an app which features self-monitoring, a thoughts and feelings journal, coping strategies, personalized goals, and contact with a clinician as the central elements. In a pilot RCT by Neumayr et al. [33] treatment combining the use of Recovery Record with treatment as usual was compared to treatment as usual alone in participants with AN (n = 40, age range = 15–36 years). The authors found no significant differences between baseline and post-intervention for BMI or EDE-Q, and non-significant between-group differences with moderate effect sizes for EDE-Q global scores (d = 0.56) and subscales (ranging from d = 0.33 to 0.64), and a small effect size for BMI (d = − 0.24), in favor of the intervention group.
Internet self-help
Seven manuscripts described an intervention that offered online self-help modules and these varied substantially in content and therapeutic approach.
We identified four trials testing internet-based self-help programs utilizing CBT principles such as self-monitoring, stimulus control, operant conditioning methods, exposure treatment, and cognitive restructuring [26, 27, 34, 36]. The following studies may differ in terms of the amount of internet self-help modules used and their specific content. An RCT [27, 28] focused on a 9-month web-based relapse prevention program for AN (n = 258, mean age = 23.8 years) following inpatient treatment with a subsequent 9-month follow-up study [28]. Participants who completed the intervention gained significantly more weight (0.62 BMI points) than those who received treatment as usual, corresponding to a small to medium effect size (mean d = 0.22). At 9-month follow-up from the end of treatment, weight gain remained greater in the intervention group, though the between-group difference was no longer significant [28]. Notably, while eating disorder symptoms increased in both conditions, the internet self-help group showed a lower increase in ED symptoms [27]. Another RCT by Wagner et al. [36] compared the effectiveness of CBT-based internet self-help to bibliotherapy in both adolescents and adults with binge/purge type EDs (n = 126, age range = 16–21 years). They found that both interventions were effective and led to significant improvement on primary outcomes, (i.e., monthly binge eating, vomiting, and fasting). Additionally, 46.5% of the participants reported being abstinent from binging for 7 months following both interventions [36]. Similarly, one RCT testing the effectiveness of iCBT-based self-help with email support in 76 participants (mean age = 23.9 years) with BN found a greater reduction in EDE global scores in the iCBT group (d = 1.28, corresponding to a large effect size) than in the waitlist control group (d = 0.52, medium effect size) [34]. Finally, an uncontrolled trial by Carrard et al. [26] examining iCBT self-help in 127 women (mean age = 24.68 years) with bulimia nervosa (BN) found that 45% of participants had clinically improved following the intervention, with significant improvements on outcomes such as binge episodes, self-induced vomiting, and over-exercising, as measured by the Eating Disorder Inventory-2.
One RCT tested the effectiveness of an internet self-help psychoeducation intervention called “Featback” [22], modeled on psychoeducation principles and including elements such as freedom to choose modules, automated messages, and feedback on monitoring and reflective exercises. The authors evaluated effectiveness and experiences of this intervention in a sample of 354 female participants (mean age = 24.2 years) with any ED in four conditions: Featback alone, Featback with low intensity therapist email support, Featback with high intensity therapist support, and waitlist control. They found that Featback with or without added support was superior to waitlist for bulimic symptoms (d = 0.16) and for ED-related quality of life at 3-month follow-up (d = 0.22) but was similar to waitlist for symptoms of AN. Although additional therapist support did not have an impact on treatment effectiveness, it did significantly increase participants' level of satisfaction with the program [22].
The remaining two articles examined diverse types of online self-help programs for young people with EDs. Wilksch et al. [71] conducted an RCT comparing Media Smart-Targeted, an online program that addresses known ED risk factors, to receiving a one-off email with tips for fostering a positive body image for participants with any ED (n = 316, age range = 18–25 years). The researchers found that participants who received Media Smart-Targeted were 75% less likely than those who received tips for body image to meet diagnostic criteria for an ED 12 months after the intervention [71]. In a non-randomized study in participants with AN, the authors [30] examined the effectiveness of treatment as usual when supplemented by videos on ED recovery (i.e., self-help component), daily text messages, and one weekly in-person meeting (n = 22, mean age = 25 years). Results showed significant reductions in participants’ global (∆η2 = 0.59, corresponding to a large effect size) and subscale (∆η2 range = 0.41–0.60, corresponding to large effect sizes) scores on the EDE-Q [30].
Registered protocols
The review identified several recently registered protocols outlining studies that fit our inclusion criteria but did not yet have published results. There were two protocols outlining RCTs to evaluate the smartphone apps, Recovery Record [65] and Jourvie Research app [62, 63] for participants with AN. A third study proposed an RCT evaluating a CBT-based self-help program, with and without therapist support, for participants with BN [57]. A fourth RCT proposed to evaluate the fully automated, online psychoeducation program Featback, comparing groups with and without expert patient support [64]. A fifth study proposed an uncontrolled trial to evaluate the transferability of FBT for adolescents with AN to a videoconference platform [60].
The review also identified several registered protocols with RCT methodologies evaluating self-help interventions, that met inclusion criteria despite published results no longer meeting criteria, for example, in the case that protocols targeted individuals potentially in the age range of interest, but eventual recruitment led to a mean participant age greater than 25 years [58, 59, 61, 66]. Nonetheless, similarly rigorous methodologies evaluating self-help in youth would contribute to evidence on this type of intervention.
Modes of delivery: qualitative and mixed-methods studies:
The qualitative and mixed-methods studies described below give insight into participant perspectives on the use of virtual modalities of care and on the transition to virtual treatment during the COVID-19 pandemic.
Mobile phone applications
Four studies explored participant perspectives on the use of four different smartphone applications, Recovery Record [46, 50], TCApp [48], and a recently developed unnamed app [51]. Two studies describing the development of new smartphone applications for EDs were also identified (no data was collected) [40, 72].
During initial application development for Recovery Record, acceptability data was collected in a naturalistic manner through a survey that was available to any individual who downloaded Recovery Record from the app store. Over a 2-year period, 97% of those who rated the app (n = 2503) gave it at least a 4/5 rating [46]. Using a naturalistic and cross-sectional study, Lindgreen et al. [50] described the experiences of participants with either AN or BN (n = 41, mean age = 24 years) using the Recovery Record self-monitoring app in addition to treatment as usual, which was either weekly family therapy or group/individual sessions. Rating of three key app features, namely meal logs, phone notifications (i.e., meal reminders and positive affirmations), and data sharing with clinicians varied across participants and ranged from supportive to obstructive of daily life. Furthermore, the authors found that participants' experiences were mixed and depended on several variables including their appreciation of app features, the frequency of app usage, and the context in which the app was used (e.g., home vs. school).
Anastasiadou et al. [48] used group discussions with stakeholders, including participants (n = 9, mean age = 15 years) who were drawn from an RCT evaluating the effectiveness of the TCApp smartphone app plus treatment as usual vs. treatment as usual alone in participants with any type of ED, over a 12-week period (National Library of Medicine, NCT03197519). All participants reported that they found the app practical and easy to use, despite some problems with the design of the app, particularly the over-quantification of symptoms and the lack of personalization. Six of nine participants rated the content appropriate, explaining that the app helped gain better understanding of problematic behavior and was a good companion during recovery. There were limited privacy and anonymity concerns (three out of nine) and some (three out of nine) found the contact with therapists in the app limited and impersonalized.
Preliminary acceptability of Space from Body and Eating Concerns Program, a mobile phone and desktop application using CBT principles for the treatment of any ED in adolescents (n = 44, age = 14–17 years), was described [41]. Overall, more than half of participants provided positive feedback relating to perceptions that the app would have a positive impact on ED recovery and would be useful as compared with in-person treatment. Negative or constructive feedback included suggestions for improving app content and design and adding gamification features.
Finally, one study examined user experience of a new smartphone app for adolescents with AN [51]. The app has an unguided self-help program based on psychoeducation, CBT, and motivational interviewing. In their study, the authors recruited 8 female adolescents between 12- and 18-years-old (mean age = 15.5 years) as well as clinicians to participate in semi-structured focus groups. Qualitative data showed that the app was viewed positively by both patients and clinicians, although concerns were raised surrounding novelty, dependability, and efficiency. Overall, the psychoeducation portion was deemed important by both patients and clinicians [51].
Internet self-help
Participant views on an internet-based cognitive behavioral self-help treatment with email support from a therapist were described by Sanchez-Ortiz et al. [52]. Purposive sampling was used to select individuals with diverse fields of study in university, with a diagnosis of BN or Eating Disorder Not Otherwise Specified (EDNOS), and who had completed between four and eight sessions of the intervention from among a larger group of 76 women participating in an RCT testing the effectiveness of iCBT compared to a delayed treatment control for EDNOS or BN [52]. Nine participants took part in semi-structured interviews while 31 of the 64 RCT participants who completed at least one session responded to an online questionnaire. All participants mentioned that the treatment improved symptoms and eating patterns in some way. Treatment flexibility was considered important, participants felt supported in their treatment, and the internet-based self-help program was user-friendly and relevant. However, 68% of participants expressed lack of privacy as the biggest problem with being able to access treatment when they wanted to.
Transition to virtual treatment during the COVID-19 pandemic
Several articles describe the transition to virtual care during the pandemic [15, 16, 18, 39, 44, 45, 47, 49, 53]. Many ED clinics were able to transfer most of their services online [15, 16, 18, 39, 44, 45, 47, 49]. Parents seemed to be the most appreciative of having appointments virtually. On the other hand, patients and staff often preferred face-to-face compared to online contact [43, 49, 53] and most patients reported wanting to return to in-person appointments for most components of treatment when pandemic-related restrictions would be lifted [15, 44, 49, 53]. Shaw [43], for example, described the transition of an art psychotherapy program for adolescents with AN to videoconference format, overall, as feasible but hindering connectedness and communication, as occasionally facilitating participant disengagement, and as potentially causing difficulties for participants with AN who struggle with seeing themself and being seen on camera as it may perpetuate negative thoughts related to EDs. Nonetheless, in several cases, patients found virtual treatment to be a positive experience [45, 49, 53] and rated the impact of technology on their treatment experience as low [53]. There may also be additional advantages to online care, such as providing opportunities for exposure to triggers in the home environment and allowing patients on bed restrictions to participate in group therapy at a distance [15]. In addition, emerging observational data suggests that the transition from face-to-face to telehealth treatment can be associated with a decrease in ED symptoms, comparable to historic benchmarks for in-person treatment [45]. Shaw et al. [53] found that there were more referrals accepted and an increase in telemedicine appointments offered in 2020 compared to 2019.
Case studies
One case study (n = 2, ages 15 and 20 years) describing a multidisciplinary intervention including FBT for youth with AN delivered via videoconference and unlimited instant messaging support online found that the participants gained 1.9 and 2.9 kg and their ED symptoms decreased (7 and 12-point decrease on the EDE-Q) [54]. Another case study [73] describing the provision of CBT via videoconferencing for one 14-year-old female participant with EDNOS found that the intervention, which included one of twelve sessions in-person, was acceptable to the participant and her family and resulted in increased food intake and normalization of the participant’s growth trajectory.
Other technologies
Marco et al. [32] compared CBT with and without an adjunct virtual reality therapy component targeting body image disturbance in an RCT (n = 34 females, mean age = 21.82 years). The VR component consisted of an adaptation [74] of an in-person CBT for body image program [75] that combined group sessions and individual psychotherapy sessions which immerse participants in environments and exercises that are intended to help them become aware of and change their body image [32]. All participants, regardless of treatment group, experienced significant improvements in body image (η2 = 0.35, corresponding to a large effect size) and ED psychopathology (η2 = 0.70, corresponding to a large effect size) post-treatment and at 1-year follow-up, although participants receiving the VR intervention showed greater improvement. An RCT examined the effectiveness of having text messages as additional support to in-person CBT treatment [35]. Ten females (mean age = 21.5 years) who met diagnostic criteria for AN were exposed to both treatment conditions, either receiving or not receiving motivational text-messages in a randomized order, using a replicated single-case alternating treatment design. The authors found no significant main effect of additionally receiving text messages on caloric intake or dietary restraint [35].
Discussion
Main findings
This scoping review aimed to describe how technology is currently being included in interventions to treat youth with EDs, to categorize interventions in terms of hybrid versus fully online programs, and to evaluate the effectiveness of such interventions. We reviewed both quantitative and qualitative/mixed-methods/observational data in addition to published protocols. The number of studies for each specific treatment modality was limited, but the majority of quantitative and qualitative studies were considered of high quality based on our systematic quality assessments.
Overall, most TBIs described in the included studies were used as primary treatments, although supplementary support was also available in most studies. The modalities, especially videoconferencing, appeared to have been used to deliver evidence-based therapies (e.g., FBT). Additionally, TBIs were more often used to deliver therapy rather than medical or other health services. Finally, most of the interventions included were completely online, as opposed to hybrid interventions.
Our review identified few studies evaluating the use of videoconferencing to deliver psychotherapy for youth with EDs. This is a clear gap in the literature given the ease with which in-person therapy can be adapted for this medium and the rapid shift to this modality during the COVID-19 pandemic. Indeed, studies describing the transition to online services during the pandemic revealed that most ED outpatient programs and eventually day programs were able to move entirely online quickly and efficiently and that most patients and families see some important benefits with videoconferencing [15, 16, 18, 39, 44, 49, 53]. Though shown to be acceptable, studies on patient experience of virtual care provide nuance on how the accessibility and flexibility of virtual care must be balanced with the decreased connection patients and clinicians may report experiencing in exclusively online treatment. Some studies pointed to the necessity of face-to-face meetings early in treatment to build rapport while others, specifically referencing the COVID-19 period, prioritized those with the highest psychological needs for in-person care. Still, these services may be useful to other groups including those with reduced mobility or living in more remote areas and can be used according to the desires of individual patients, families, and clinician teams, within a hybrid framework that may become an essential part of the post-pandemic landscape.
It should be noted that in all three of the empirical studies on videoconferencing, the modality was new, but the specific type of therapy used already has a good evidence base when delivered in-person. Thus, FBT, a well-established treatment for adolescents with AN, may be effective for weight gain (in those who are underweight) and for decreasing ED symptoms in adolescents with AN when delivered virtually. However, these findings are drawn from only one case study and two quantitative studies, neither of which use in-person therapy as a control group comparison. Interestingly, available data of one study suggest that FBT delivered virtually may be as effective as online guided self-help FBT for decreasing ED symptoms [31]. This could point to the transferability of FBT to various modalities, which could increase treatment options for patients and improve accessibility, though these findings are preliminary. Though more rigorous studies are needed to fully substantiate the effectiveness of videoconferencing therapy for youth with EDs, especially in other populations than youth with AN, these initial findings are in line with studies that show videoconference therapy to be effective for other mental disorders, including depression and obsessive–compulsive disorders [76, 77].
The limited number of studies identified in this review evaluating mobile applications as treatment modalities for youth with EDs did not find statistically significant effects of this intervention on eating-disorder related outcomes. This is in agreement with literature on the topic which found that while mobile apps are generally acceptable to patients, they have limited effects on ED psychopathology [78]. This could represent a true lack of effect or could represent an inability to detect the specific contributions of the app to recovery given that patients in both interventions discussed here continued to receive therapy as usual in addition to using the app. The small number of studies evaluating mobile applications in youth is also somewhat surprising considering the many different mobile applications available for ED care [79, 80] and considering that youth, especially females, are amongst the biggest users of mobile phones and applications [81]. Given this context, future research may consider the impacts of unexamined use of mobile apps for EDs, especially because mobile apps which track calories have been associated with increased ED symptomatology [82,83,84].
Clinicians and patients agree that mobile apps are useful in early stages of the disease [51] and features such as psychoeducation and self-monitoring can be relevant at these points. The ease with which they can be implemented [80] also means that there is high potential to providing these interventions early in the course of treatment. Patient experiences with mobile apps suggest that the option to personalize features in the app is critical and emerging research suggests that multimedia features and the possibility to easily link to resources are the most engaging to youth patients [51, 85]. Beyond this, the use of apps and their specific features should be discussed on a case-by-case basis that takes into account patient and clinician preferences and capacities, as these can vary greatly between individuals [50].
While there has been no systematic evaluation of self-help interventions specifically for adolescents and young adults, early reviews that included mixed age populations [10,11,12,13] found that these interventions were superior to wait-list for reducing ED psychopathology, especially for participants with binge-type symptoms (vs. restrictive-type symptoms). However, these reviews recommended that more RCTs should be carried out to confirm the effectiveness of such interventions, especially in adolescents. More recently, Ahmadiankalati et al. [13] maintained that evidence for both acceptability and effectiveness of internet-based interventions was limited and that there is a lack of studies in adolescents, among other groups.
Similarly, we found that all self-help interventions were targeted towards older adolescents (> 16 years) and young adults. The pertinence, effectiveness and safety of this modality for younger adolescents, thus, remains unknown. Evidence for the use of self-help for patients with AN is also limited, based on our study though there may be some benefits in terms of weight gain [27, 28, 31]. As for restrictive ED symptoms, findings were mixed, ranging from a decrease to no change or even an increase in restrictive symptoms from baseline to end of treatment [22, 28, 30, 71]. It is noteworthy to mention the studies in which symptoms decreased were either uncontrolled or used a passive placebo group.
Effectiveness of internet self-help, and internet CBT in particular, for patients with BN and other purgative type EDs is promising but still needs to be verified as compared to active control interventions. The one study that compared internet self-help to an active control found that [34, 35] internet CBT was effective but had similar outcomes as the control intervention. When compared to waitlist control, we identified studies that confirmed effectiveness, but this was true, with large effect sizes and clinical improvements, in under half of study participants.
Finally, it should be noted that many of the studies examining internet self-help intervention were published between 2011 and 2013, which may lead us to question the current pertinence of this modality for individuals with EDs. Despite this, we did identify two protocols for internet self-help published in 2020 and 2021. Further, a smaller number of self-help studies, published over the last 6 years, were identified. Thus, this modality appears still relevant but has most likely been overshadowed by the development of new mobile apps and the increase of videoconferencing use since the beginning of the pandemic. Nevertheless, it may be an important option for those who would not seek in-person care. With regards to internet self-help of all types, design may be an important feature and interventions incorporating multimedia elements, that is, a combination of audio, text, video, etc., are associated with the greatest ED symptom reduction in treatment groups [85]. Though technology design was not a key element of our research, interventions explicitly described as interactive and/or multimedia in manuscripts were effective [22, 30, 71]. Even so, results should be interpreted cautiously as the improvements seen in the study by Kim [30] cannot be attributed to the multimedia intervention alone, as patients continued to receive TAU and weekly in-person guidance for technology usage.
The five protocols with unpublished results identified in this review target various modalities of intervention including two protocols on mobile applications, two on internet-based self-help programs, and one on videoconference therapy, with the majority (4/5) using rigorous RCT methodology. Future studies may build on the methodologies and interventions described. Additionally, the four published protocols with results not meeting our review inclusion criteria are informative and may be of interest to researchers and clinicians in that all use RCT methodology and most use active control groups, which can be applied to the population of interest.
Overall, the current findings align with previous reviews [10,11,12,13] that have found promising results for TBIs. Similar to what was described in these reviews, there seems to be few studies evaluating mobile application effectiveness while videoconferencing and internet self-help have been evaluated in a variety of contexts. Our review adds to previous work in that we reported on TBI use during the COVID-19 pandemic, showed the lack of studies on adolescents and youth, and brought to light the lack of hybrid intervention models.
Strengths and limitations
This scoping review has several strengths. First, the review has a rigorous methodological procedure, including a quality assessment for both quantitative and qualitative studies to provide key information on the studies included. Second, contrary to a previous review of TBIs [11], our age criteria allowed us to review the literature in youth and emerging adults in the most extensive way without including studies that are not pertinent. Nevertheless, we had to compromise on age specificity in some cases where the age range extended beyond 25 years. There was a need for such information as this population is particularly at risk for EDs and has distinct developmental characteristics. Further, the present review included literature from before and during the pandemic and studies were categorized in terms of modes of delivery as well as described in terms of being hybrid versus fully online interventions.
Several limitations need to be considered. First, no cross-coding was carried out during the title and abstract screening phase, which may have had an impact on initial article selection for the study. However, we used a conservative approach to screening, which should have mitigated this impact. Second, the inclusion criteria were relatively strict in terms of age and diagnosis, which led to exclusion of studies that could potentially be relevant for researchers and clinicians interested in subclinical and/or older adult populations. However, our use of an inclusion criteria based on average participant age (between 10 and 25 years) also means that studies including individuals outside this range may also be included. Third, only results from the last 10 years were included based on the rationale that older studies may not have up to date technologies. It is possible that some studies prior to 2011 had similar methodologies and interventions to the ones we included, however, these were likely included in earlier reviews of virtual interventions, such as Aardoom et al. [10]. Fourth, several included studies had a relatively small sample size and lacked a control group, which could make the generalization of findings difficult. Fifth, evaluating dropout rates, which are highly variable (4.7–84.8%) in studies evaluating TBIs for EDs [11], warrants further investigation. Finally, as the number of studies for each treatment modality was relatively small and individual studies were highly heterogeneous, we did not further quantify overall results by using meta-analytic procedures. Such an approach would be useful once more empirical studies become available.
This review identified several areas for future research. Studies are needed on videoconference therapy to better understand if common in-person treatment approaches, such as FBT and CBT, can be reasonably transferred online without compromising effectiveness. This is necessary considering this modality was used most frequently when transitioning to online treatment during the COVID-19 pandemic. In our review, mobile phone applications were not associated with improved treatment outcomes in youth when added to treatment as usual. The limited number of studies in clinical populations overall makes it difficult to draw clear conclusions on the pertinence of this modality for treatment. It is possible that the features provided in current mobile phone apps (mostly self-monitoring and food logs) may not be of benefit in a clinical youth population and that other features may need to be proposed. There was also a concern regarding the lack of individualization of available apps, which may make their use less appealing to patients. Self-help was useful in all cases but its effectiveness in comparison to active treatment modalities remains unclear, and more studies need to be conducted to determine the level of support (high vs. low intensity) that is required for effectiveness and the type of support that is the most helpful (automated vs. clinician vs. technician). Additionally, there is a lack of systematic studies on hybrid treatments, which warrants further investigation considering patients’ expressed needs/desires for in-person support when receiving virtual care. The combination of in-person and virtual components of treatment may offer patients the opportunity to benefit from the best elements of each approach. However, evidence-based guidelines on providing hybrid care are lacking [86] and no firm conclusions can be made based on our review as most of the studies reviewed were fully online.
Conclusions
This review has found evidence supporting the use of TBIs for the treatment of EDs in youth. In particular, internet self-help guides were useful for decreasing ED symptomatology and the evidence to support this finding was of high quality. Though qualitative studies suggest that some form of therapist support is an essential element of treatment, future studies could investigate the impact of therapist support on ED outcomes in self-help programs. In addition, more controlled trials with larger samples are required to evaluate the effectiveness of videoconference therapy. However, videoconferencing has been shown to be feasible and acceptable during the COVID-19 pandemic. Limited evidence was found on the use of mobile phone applications in the clinical youth population. More controlled trials of mobile phone applications in clinical populations are required to conclude on their effectiveness. Considering that youth are particularly at risk for EDs, there is a lack of high-quality RCTs testing virtual care and hybrid interventions in this population. Filling this important research gap could lead to significant improvements in ED care in a rapidly evolving landscape of ED treatment in youth.
Availability of data and materials
As no new data were generated in this study, data sharing is not applicable to this article.
Abbreviations
- AN:
-
Anorexia nervosa
- BMI:
-
Body mass index
- BN:
-
Bulimia nervosa
- CBT:
-
Cognitive behavioral therapy
- DSM-IV:
-
Diagnostic and statistical manual of mental disorders fourth edition
- DSM-5:
-
Diagnostic and statistical manual of mental disorders fifth edition
- ED:
-
Eating disorder
- EDE:
-
Eating disorder examination
- EDE-Q:
-
Eating disorder examination-questionnaire
- EDNOS:
-
Eating disorder not otherwise specified
- FBT:
-
Family-based treatment
- RCT:
-
Randomized controlled trial
- TAU:
-
Treatment as usual
- TBI:
-
Technology-based interventions
References
Treasure J, Duarte TA, Schmidt U. Eating disorders. Lancet. 2020;395(10227):899–911. https://doi.org/10.1016/S0140-6736(20)30059-3.
Linardon J, Wade TD, de la Piedad Garcia X, Brennan L. The efficacy of cognitive-behavioral therapy for eating disorders: a systematic review and meta-analysis. J Consult Clin Psychol. 2017;85(11):1080–94. https://doi.org/10.1037/ccp0000245.
Stiles-Shields C, Hoste RR, Doyle PM, Le Grange D. A review of family-based treatment for adolescents with eating disorders. Rev Recent Clin Trials. 2012;7(2):133–40. https://doi.org/10.2174/157488712800100242.
Bohrer BK, Carroll IA, Forbush KT, Chen P-Y. Treatment seeking for eating disorders: results from a nationally representative study. Int J Eat Disord. 2017;50(12):1341–9. https://doi.org/10.1002/eat.22785.
Forrest LN, Smith AR, Swanson SA. Characteristics of seeking treatment among U.S. adolescents with eating disorders. Int J Eat Disord. 2017;50(7):826–33. https://doi.org/10.1002/eat.22702.
McLean SA, Caldwell B, Roberton M. Reach out and recover: intentions to seek treatment in individuals using online support for eating disorders. Int J Eat Disord. 2019;52(10):1137–49. https://doi.org/10.1002/eat.23133.
Thompson C, Park S. Barriers to access and utilization of eating disorder treatment among women. Arch Womens Ment Health. 2016;19(5):753–60. https://doi.org/10.1007/s00737-016-0618-4.
Lindefors N, Andersson G, editors. Guided internet-based treatments in psychiatry. Berlin: Springer; 2016. https://doi.org/10.1007/978-3-319-06083-5.
Sadeh-Sharvit S. Use of technology in the assessment and treatment of eating disorders in youth. Child Adolesc Psychiatr Clin N Am. 2019;28(4):653–61. https://doi.org/10.1016/j.chc.2019.05.011.
Aardoom JJ, Dingemans AE, Spinhoven P, Van Furth EF. Treating eating disorders over the internet: a systematic review and future research directions. Int J Eat Disord. 2013;46(6):539–52. https://doi.org/10.1002/eat.22135.
Schlegl S, Bürger C, Schmidt L, Herbst N, Voderholzer U. The potential of technology-based psychological interventions for anorexia and bulimia nervosa: a systematic review and recommendations for future research. J Med Internet Res. 2015;17(3):e85. https://doi.org/10.2196/jmir.3554.
Aardoom JJ, Dingemans AE, Van Furth EF. E-health interventions for eating disorders: emerging findings, issues, and opportunities. Curr Psychiatry Rep. 2016;18(4):42. https://doi.org/10.1007/s11920-016-0673-6.
Ahmadiankalati M, Steins-Loeber S, Paslakis G. Review of randomized controlled trials using e-health interventions for patients with eating disorders. Front Psychiatry. 2020;11:568. https://doi.org/10.3389/fpsyt.2020.00568.
Chadi N, Spinoso-Di Piano C, Osmanlliu E, Gravel J, Drouin O. Mental health-related emergency department visits in adolescents before and during the COVID-19 pandemic: a multicentric retrospective study. J Adolesc Health. 2021;69(5):847–50. https://doi.org/10.1016/j.jadohealth.2021.07.036.
Datta N, Derenne J, Sanders M, Lock JD. Telehealth transition in a comprehensive care unit for eating disorders: challenges and long-term benefits. Int J Eat Disord. 2020;53(11):1774–9. https://doi.org/10.1002/eat.23348.
Davis C, Ng KC, Oh JY, Baeg A, Rajasegaran K, Chew CSE. Caring for children and adolescents with eating disorders in the current Coronavirus 19 pandemic: Singapore perspective. J Adolesc Health. 2020;67(1):131–4. https://doi.org/10.1016/j.jadohealth.2020.03.037.
Branley-Bell D, Talbot CV. Exploring the impact of the COVID-19 pandemic and UK lockdown on individuals with experience of eating disorders. J Eat Disord. 2020;8(1):44. https://doi.org/10.1186/s40337-020-00319-y.
Barney A, Buckelew S, Mesheriakova V, Raymond-Flesch M. The COVID-19 pandemic and rapid implementation of adolescent and young adult telemedicine: challenges and opportunities for innovation. J Adolesc Health. 2020;67(2):164–71. https://doi.org/10.1016/j.jadohealth.2020.05.006.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMAScR): checklist and explanation. Ann Intern Med. 2018;169:467–73. https://doi.org/10.7326/M18-0850.
Couturier J, Pellegrini D, Miller C, Bhatnagar N, Boachie A, Bourret K, Brouwers M, Coelho JS, Dimitropoulos G, Findlay S, Ford C, Geller J, Grewal S, Gusella J, Isserlin L, Jericho M, Johnson N, Katzman DK, Kimber M, Lafrance A, Leclerc A, Loewen R, Loewen T, McVey G, Norris M, Pilon D, Preskow W, Spettigue W, Steinegger C, Waite E, Webb C. The COVID-19 pandemic and eating disorders in children, adolescents, and emerging adults: virtual care recommendations from the Canadian consensus panel during COVID-19 and beyond. J Eat Disord. 2021;9(1):46. https://doi.org/10.1186/s40337-021-00394-9.
Society for Adolescent Health and Medicine, Golden NH, Katzman DK, Sawyer SM, Ornstein RM, Rome ES, Garber AK, Kohn M, Kreipe RE. Position paper of the society for adolescent health and medicine: medical management of restrictive eating disorders in adolescents and young adults. J Adolesc Health. 2015;56(1):121–5. https://doi.org/10.1016/j.jadohealth.2014.10.259.
Aardoom JJ, Dingemans AE, Spinhoven P, van Ginkel JR, de Rooij M, van Furth EF. Web-based fully automated self-help with different levels of therapist support for individuals with eating disorder symptoms: a randomized controlled trial. J Med Internet Res. 2016;18(6):e159. https://doi.org/10.2196/jmir.5709.
Aardoom JJ, Dingemans AE, Fokkema M, Spinhove P, Van Furth EF. Moderators of change in an internet-based intervention for eating disorders with different levels of therapist support: What works for whom?. Behav Res Therapy. 2017;89:66–74. https://doi.org/10.1016/j.brat.2016.11.012.
Anastasiadou D, Folkvord F, Brugnera A, Cañas Vinader L, Serrano Troncoso E, Carretero Jardí C, Linares Bertolin R, Muñoz Rodríguez R, Martínez Nuñez B, Graell Berna M, Torralbas-Ortega J, Torrent-Solà L, Puntí-Vidal J, Carrera Ferrer M, Muñoz Domenjó A, Diaz Marsa M, Gunnard K, Cusido J, Arcal Cunillera J, Lupiañez-Villanueva F. An mHealth intervention for the treatment of patients with an eating disorder: a multicenter randomized controlled trial. Int J Eat Disord. 2020;53(7):1120–31. https://doi.org/10.1002/eat.2328.
Anderson KE, Byrne CE, Crosby RD, Le Grange D. Utilizing telehealth to deliver family-based treatment for adolescent anorexia nervosa. Int J Eat Disord. 2017;50(10):1235–8. https://doi.org/10.1002/eat.22759.
Carrard I, Fernandez-Aranda F, Lam T, Nevonen L, Liwowsky I, Volkart AC, Rouget P, Golay A, Van der Linden M, Norring C. Evaluation of a guided internet self-treatment programme for bulimia nervosa in several European countries. Eur Eat Disord Rev. 2011;19(2):138–49. https://doi.org/10.1002/erv.1043.
Fichter MM, Quadflieg N, Nisslmüller K, Lindner S, Osen B, Huber T, Wünsch-Leiteritz W. Does internet-based prevention reduce the risk of relapse for anorexia nervosa? Behav Res Ther. 2012;50(3):180–90. https://doi.org/10.1016/j.brat.2011.12.003.
Fichter MM, Quadflieg N, Lindner S. Internet-based relapse prevention for anorexia nervosa: nine-month follow-up. J Eat Disord. 2013;1:23. https://doi.org/10.1186/2050-2974-1-23.
Giel KE, Leehr EJ, Becker S, Herzog W, Junne F, Schmidt U, Zipfel S. Relapse prevention via videoconference for anorexia nervosa—findings from the RESTART pilot study. Psychother Psychosom. 2015;84(6):381–3. https://doi.org/10.1159/000431044.
Kim Y-R, Cardi V, Lee GY, An S, Kim J, Kwon G, Kim JW, Eom J-S, Treasure J. Mobile self-help interventions as augmentation therapy for patients with Anorexia Nervosa. Telemed E-Health. 2019;25(8):740–7. https://doi.org/10.1089/tmj.2018.0180.
Lock J, Couturier J, Matheson BE, Datta N, Citron K, Sami S, Welch H, Webb C, Doxtdator K, John-Carson N. Feasibility of conducting a randomized controlled trial comparing family-based treatment via videoconferencing and online guided self-help family-based treatment for adolescent anorexia nervosa. Int J Eat Disord. 2021;54(11):1998–2008. https://doi.org/10.1002/eat.23611.
Marco JH, Perpiñá C, Botella C. Effectiveness of cognitive behavioral therapy supported by virtual reality in the treatment of body image in eating disorders: one year follow-up. Psychiatry Res. 2013;209(3):619–25. https://doi.org/10.1016/j.psychres.2013.02.023.
Neumayr C, Voderholzer U, Tregarthen J, Schlegl S. Improving aftercare with technology for anorexia nervosa after intensive inpatient treatment: a pilot randomized controlled trial with a therapist-guided smartphone app. Int J Eat Disord. 2019;52(10):1191–201. https://doi.org/10.1002/eat.23152.
Sánchez-Ortiz VC, Munro C, Stahl D, House J, Startup H, Treasure J, Williams C, Schmidt U. A randomized controlled trial of internet-based cognitive-behavioural therapy for bulimia nervosa or related disorders in a student population. Psychol Med. 2011;41(2):407–17. https://doi.org/10.1017/S0033291710000711.
Shingleton RM, Pratt EM, Gorman B, Barlow DH, Palfai TP, Thompson-Brenner H. Motivational text message intervention for eating disorders: a single-case alternating treatment design using ecological momentary assessment. Behav Ther. 2016;47(3):325–38. https://doi.org/10.1016/j.beth.2016.01.005.
Wagner G, Penelo E, Wanner C, Gwinner P, Trofaier M-L, Imgart H, Waldherr K, Wöber-Bingöl C, Karwautz AFK. Internet-delivered cognitive-behavioural therapy vs. conventional guided self-help for bulimia nervosa: long-term evaluation of a randomised controlled trial. Br J Psychiatry. 2013;202:135–41. https://doi.org/10.1192/bjp.bp.111.098582.
Wagner G, Penelo E, Nobis G, Mayrhofer A, Wanner C, Schau J, Spitzer M, Gwinner P, Trofaier ML, Imgart H, Fernandez-Aranda F, Karwautz A. Predictors of good therapeutic outcome and drop-out in technology assisted guided self-help in the treatmennt of bulimia nervosa and bulimia like phenotype. Eur Eat Disorders Rev. 2015;23:163–9. https://doi.org/10.1002/erv.2336.
Wilksch SM, O'Shea A, Wade TD. Media Smart-Targeted: Diagnostic outcomes from a two-country pragmatic online eating disorder risk reduction trial for young adults. Int J Eat Disord. 2017;51:270–4. https://doi.org/10.1002/eat.22825.
Carretier E, Guessoum SB, Radjack R, Mao S-F, Minassian S, Blanchet C, Moro MR, Lachal J. Adjustment of healthcare and telemedicine in times of lockdown and COVID-19 pandemic: feedback from a “Maison des adolescents” (Teenager’s House). Neuropsychiatr Enfance Adolesc. 2021;69(3):132–7. https://doi.org/10.1016/j.neurenf.2021.02.001.
Criquillion S. A mobile application for people with anorexia and bulimia. Soins Psychiatrie. 2017;38(311):40–3. https://doi.org/10.1016/j.spsy.2017.04.012.
Kasson E, Vázquez MM, Doroshenko C, Fitzsimmons-Craft EE, Wilfley DE, Taylor CB, Cavazos-Rehg PA. Exploring social media recruitment strategies and preliminary acceptability of an mHealth tool for teens with eating disorders. Int J Environ Res Public Health. 2021;18(15):7979. https://doi.org/10.3390/ijerph18157979.
Rajankar P, Milind Patki S. Eat Well: Smart Intervention Plan for Bulimia in the Indian Context. J Psychosocial Res. 2019;14(2):335-344. https://doi.org/10.32381/JPR.2019.14.02.11.
Shaw L. ‘Don’t look!’ an online art therapy group for adolescents with Anorexia Nervosa. Int J Art Ther. 2020;25(4):211–7. https://doi.org/10.1080/17454832.2020.1845757.
Stewart C, Konstantellou A, Kassamali F, McLaughlin N, Cutinha D, Bryant-Waugh R, Simic M, Eisler I, Baudinet J. Is this the “new normal”? A mixed method investigation of young person, parent and clinician experience of online eating disorder treatment during the COVID-19 pandemic. J Eat Disord. 2021;9(1):78. https://doi.org/10.1186/s40337-021-00429-1.
Raykos BC, Erceg-Hurn DM, Hill J, Campbell B, McEvoy PM. Positive outcomes from integrating telehealth into routine clinical practice for eating disorders during COVID-19. Int J Eat Disord. 2021;54(9):1689–95. https://doi.org/10.1002/eat.23574.
Tregarthen JP, Lock J, Darcy AM. Development of a smartphone application for eating disorder self-monitoring. Int J Eat Disord. 2015;48(7):972–82. https://doi.org/10.1002/eat.22386.
Yaffa S, Adi EL, Itai P, Marit JM, Doron G, Daniel S. Treatment of eating disorders in adolescents during the COVID-19 pandemic: a case series. J Eat Disord. 2021;9(1):17. https://doi.org/10.1186/s40337-021-00374-z.
Anastasiadou D, Folkvord F, Serrano-Troncoso E, Lupiañez-Villanueva F. Mobile health adoption in mental health: user experience of a mobile health app for patients with an eating disorder. JMIR MHealth UHealth. 2019;7(6):e12920. https://doi.org/10.2196/12920.
Brothwood PL, Baudinet J, Stewart CS, Simic M. Moving online: young people and parents’ experiences of adolescent eating disorder day programme treatment during the COVID-19 pandemic. J Eat Disord. 2021;9(1):62. https://doi.org/10.1186/s40337-021-00418-4.
Lindgreen P, Lomborg K, Clausen L. Patient experiences using a self-monitoring app in eating disorder treatment: qualitative study. JMIR MHealth UHealth. 2018;6(6):e10253. https://doi.org/10.2196/10253.
Naccache B, Mesquida L, Raynaud J-P, Revet A. Smartphone application for adolescents with anorexia nervosa: an initial acceptability and user experience evaluation. BMC Psychiatry. 2021;21(1):467. https://doi.org/10.1186/s12888-021-03478-7.
Sánchez-Ortiz VC, House J, Munro C, Treasure J, Startup H, Williams C, Schmidt U. “A computer isn’t gonna judge you”: a qualitative study of users’ views of an internet-based cognitive behavioural guided self-care treatment package for bulimia nervosa and related disorders. Eat Weight Disord. 2011;16(2):e93–101. https://doi.org/10.1007/BF03325314.
Shaw H, Robertson S, Ranceva N. What was the impact of a global pandemic (COVID-19) lockdown period on experiences within an eating disorder service? A service evaluation of the views of patients, parents/carers and staff. J Eat Disord. 2021;9(1):14. https://doi.org/10.1186/s40337-021-00368-x.
Hellner M, Bohon C, Kolander S, Parks E. Virtually delivered family-based eating disorder treatment using an enhanced multidisciplinary care team: a case study. Clin Case Rep. 2021;9(6):e04173. https://doi.org/10.1002/ccr3.4173.
Duncan AB, Velasquez SE, Nelson EL. Using videoconferencing to provide psychological services to rural children and adolescents: A review and case example. J Clin Child Ado Psychol. 2014;43(1):115–27. https://doi.org/10.1080/15374416.2013.836452.
Anderson KE, Byrne C, Goodyear A, Reichel R, Le Grange D. Telemedicine of family-based treatment for adolescent anorexia nervosa: a protocol of a treatment development study. J Eat Disord. 2015;3:25. https://doi.org/10.1186/s40337-015-0063-1.
Barakat S, Touyz S, Maloney D, Russell J, Hay P, Cunich M, Lymer S, Kim M, Madden S, Miskovic-Wheatley J, Maguire S. Supported online cognitive behavioural therapy for bulimia nervosa: a study protocol of a randomised controlled trial. J Eat Disord. 2021;9:126. https://doi.org/10.1186/s40337-021-00482-w.
Bulik CM, Marcus MD, Zerwas S, Levine MD, Hofmeier S, Trace SE, Hamer RM, Zimmer B, Moessner M, Kordy H. CBT4BN versus CBTF2F: comparison of online versus face-to-face treatment for bulimia nervosa. Contemp Clin Trials. 2012;33(5):1056–64. https://doi.org/10.1016/j.cct.2012.05.008.
de Zwaan M, Herpertz S, Zipfel S, Tuschen-Caffier B, Friederich H-C, Schmidt F, Gefeller O, Mayr A, Lam T, Schade-Brittinger C, Hilbert A. INTERBED: internet-based guided self-help for overweight and obese patients with full or subsyndromal binge eating disorder. A multicenter randomized controlled trial. Trials. 2012;13:220. https://doi.org/10.1186/1745-6215-13-220.
Hambleton A, Le Grange D, Miskovic-Wheatley J, Touyz S, Cunich M, Maguire S. Translating evidence-based treatment for digital health delivery: a protocol for family-based treatment for anorexia nervosa using telemedicine. J Eat Disord. 2020;8:50. https://doi.org/10.1186/s40337-020-00328-x.
Jenkins PE, Luck A, Burrows A, Boughton N. Comparison of face-to-face versus email guided self-help for binge eating: study protocol for a randomised controlled trial. Trials. 2014;15:181. https://doi.org/10.1186/1745-6215-15-181.
Kolar D, Hammerle F, Jenetzky E, Karabasheva E, Huss M. Bridging the gap: smartphone-based support between sessions for adolescent outpatients with Anorexia nervosa—a randomized controlled trial protocol (The SELTIAN study). In: Paper presented at the 4th eating disorders international conference, London, United Kingdom. 2016.
Kolar DR, Hammerle F, Jenetzky E, Huss M. Smartphone-enhanced low-threshold intervention for adolescents with anorexia nervosa (SELTIAN) waiting for outpatient psychotherapy: study protocol of a randomised controlled trial. BMJ Open. 2017;7(10):e018049. https://doi.org/10.1136/bmjopen-2017-018049.
Rohrbach PJ, Dingemans AE, Spinhoven P, Van den Akker-Van Marle E, Van Ginkel JR, Fokkema M, Moessner M, Bauer S, Van Furth EF. A randomized controlled trial of an internet-based intervention for eating disorders and the added value of expert-patient support: study protocol. Trials. 2019;20(1):509. https://doi.org/10.1186/s13063-019-3574-2.
Schlegl S, Neumayr C, Voderholzer U. Therapist-guided smartphone-based aftercare for inpatients with severe anorexia nervosa (SMART-AN): study protocol of a randomized controlled trial. Int J Eat Disord. 2020;53(10):1739–45. https://doi.org/10.1002/eat.23357.
ter Huurne ED, Postel MG, de Haan HA, DeJong CAJ. Effectiveness of a web-based treatment program using intensive therapeutic support for female patients with bulimia nervosa, binge eating disorder and eating disorders not otherwise specified: study protocol of a randomized controlled trial. BMC Psychiatry. 2013;13:310. https://doi.org/10.1186/1471-244X-13-310.
Greenhalgh J, Brown T. Quality assessment: Where do I begin? In: Boland A, Cherry G, Dickson R, editors. Doing a systematic review: a student’s guide. Liverpool: Sage; 2013. p. 61–83.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savović J, Schulz KF, Weeks L, Sterne JAC. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. https://doi.org/10.1136/bmj.d5928.
Critical Appraisal Skills Programme. CASP (Qualitative Studies Checklist) [online] . (2022). Available at: https://casp-uk.b-cdn.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf. Accessed 13 Sept 2022.
Greenhalgh T, Wherton J, Papoutsi C, Lynch J, Hughes G, A’Court C, Hinder S, Fahy N, Procter R, Shaw S. Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Medical Internet Res. 2017;19(11):e8775. https://doi.org/10.2196/jmir.8775.
Wilksch SM, O’Shea A, Wade TD. Media smart-targeted: diagnostic outcomes from a two-country pragmatic online eating disorder risk reduction trial for young adults. Int J Eat Disord. 2018;51(3):270–4. https://doi.org/10.1002/eat.22825.
Rajankar P, Patki S. Eat well: smart intervention plan for bulimia in the Indian context. J Psychosoc Res. 2020;14:335–44. https://doi.org/10.32381/JPR.2019.14.02.11.
Duncan AB, Velasquez SE, Nelson E-L. Using videoconferencing to provide psychological services to rural children and adolescents: a review and case example. J Clin Child Adolesc Psychol. 2014;43(1):115–27. https://doi.org/10.1080/15374416.2013.836452.
Perpina C, Botella C, Banos RM. Imagen corporal en los trastornos alimentarios. Evaluacion y tratamiento por medio de realidad virtual. Valencia: Promo-libro; 2000.
Butters JW, Cash TF. Cognitive-behavioral treatment of women’s body-image dissatisfaction. J Consult Clin Psychol. 1987;55(6):889–97. https://doi.org/10.1037/0022-006X.55.6.889.
Luo C, Sanger N, Singhal N, Pattrick K, Shams I, Shahid H, Hoang P, Schmidt J, Lee J, Haber S, Puckering M, Buchanan N, Lee P, Ng K, Sun S, Kheyson S, Chung DC-Y, Sanger S, Thabane L, Samaan Z. A comparison of electronically-delivered and face to face cognitive behavioural therapies in depressive disorders: a systematic review and meta-analysis. EClinicalMedicine. 2020;24:100442. https://doi.org/10.1016/j.eclinm.2020.100442.
Wootton BM. Remote cognitive–behavior therapy for obsessive–compulsive symptoms: a meta-analysis. Clin Psychol Rev. 2016;43:103–13. https://doi.org/10.1016/j.cpr.2015.10.001.
Anastasiadou D, Folkvord F, Lupiañez-Villanueva F. A systematic review of mHealth interventions for the support of eating disorders. Eur Eat Disord Rev. 2018;26(5):394–416. https://doi.org/10.1002/erv.2609.
Fairburn CG, Rothwell ER. Apps and eating disorders: a systematic clinical appraisal. Int J Eat Disord. 2015;48(7):1038–46. https://doi.org/10.1002/eat.22398.
Juarascio AS, Manasse SM, Goldstein SP, Forman EM, Butryn ML. Review of smartphone applications for the treatment of eating disorders. Eur Eat Disord Rev. 2015;23(1):1–11. https://doi.org/10.1002/erv.2327.
Andone I, Błaszkiewicz K, Eibes M, Trendafilov B, Montag C, Markowetz A. How age and gender affect smartphone usage. In: Proceedings of the 2016 ACM international joint conference on pervasive and ubiquitous computing: adjunct; 2016 Sep 12–16; Heidelberg: Association for Computing Machinery; 2016. p. 9–12. https://doi.org/10.1145/2968219.2971451.
Levinson CA, Fewell L, Brosof LC. My fitness pal calorie tracker usage in the eating disorders. Eat Behav. 2017;27:14–6. https://doi.org/10.1016/j.eatbeh.2017.08.003.
Simpson CC, Mazzeo SE. Calorie counting and fitness tracking technology: associations with eating disorder symptomatology. Eat Behav. 2017;26:89–92. https://doi.org/10.1016/j.eatbeh.2017.02.002.
Messer M, McClure Z, Norton B, Smart M, Linardon J. Using an app to count calories: motives, perceptions, and connections to thinness-and muscularity-oriented disordered eating. Eat Behav. 2021;43:101568. https://doi.org/10.1016/j.eatbeh.2021.101568.
Barakat S, Maguire S, Smith KE, Mason TB, Crosby RD, Touyz S. Evaluating the role of digital intervention design in treatment outcomes and adherence to eTherapy programs for eating disorders: a systematic review and meta-analysis. Int J Eat Disord. 2019;52(10):1077–94. https://doi.org/10.1002/eat.23131.
Smith K, Ostinelli E, Macdonald O, Cipriani A. COVID-19 and telepsychiatry: development of evidence-based guidance for clinicians. JMIR Ment Health. 2020;7(8):e21108. https://doi.org/10.2196/21108.
Acknowledgements
Not applicable.
Funding
RD is supported by a Master-level research award from the Social Sciences and Humanities Research Council. KN is supported by a Master-level research award from the Canadian Institutes of Health Research. LP is supported by a grant from the Bell Let’s Talk Foundation. NC is supported by a clinical scholar award from Fonds de Recherche du Québec—Santé (clinicien-chercheur boursier junior 1). LB is supported by a scholar award from Fonds de Recherche du Québec—Santé (chercheur boursier senior).
Author information
Authors and Affiliations
Contributions
RD and KN designed the study, conducted the search, reviewed the articles, and drafted the initial manuscript. LP reviewed the manuscript for important intellectual content. NC and LB provided supervision, contributed to study design, and reviewed the manuscript for important intellectual content. All authors revised and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Fig. S1.
Quality assessment of quantitative studies.
Additional file 2: Fig. S2.
Quality assessment of qualitative studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Dufour, R., Novack, K., Picard, L. et al. The use of technology in the treatment of youth with eating disorders: A scoping review. J Eat Disord 10, 182 (2022). https://doi.org/10.1186/s40337-022-00697-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40337-022-00697-5