
Abstract
Background
Obsessive–compulsive disorder (OCD) is one of the most prevalent comorbidities in anorexia nervosa (AN). As AN is a severe, life-threatening condition, reducing obsessive–compulsive symptomatology is not the primary objective during treatment of AN and, thus, these symptoms may remain unchanged or may even increase in terms of a “symptom shift”.
Methods
In this retrospective analysis, we examined clinical records of 149 adolescents (n = 96, 64%) and adults (n = 53, 36%) with AN (6 males, 4%) who received inpatient treatment and completed the Obsessive–Compulsive Inventory–Revised at admission and discharge.
Results
Obsessive–compulsive symptoms decreased from admission to discharge, irrespective of whether patients had comorbid OCD or not. Within-person decreases in obsessive–compulsive symptoms weakly correlated with increases in body weight.
Conclusions
These results indicate that obsessive–compulsive symptoms decrease during inpatient treatment of AN although they are not primarily targeted during treatment. Furthermore, these improvements seem to be associated with general improvements in AN symptomatology, suggesting the absence of a “symptom shift”. Yet, effect sizes were small and obsessive–compulsive symptoms were still clinically elevated in patients with comorbid OCD at discharge, suggesting that these patients need OCD-specific, psychotherapeutic aftercare.
Plain English summary
This study shows that obsessive–compulsive symptoms decrease during inpatient treatment of anorexia nervosa. That is, there is no “symptom shift”, which refers to the idea that a reduction of anorexia nervosa symptoms may result in an increase in other symptoms. However, obsessive–compulsive symptoms should still be targeted during psychotherapeutic aftercare in patients who show obsessive–compulsive tendencies.
Similar content being viewed by others


Introduction
With a prevalence of about 10–20%, obsessive–compulsive disorder (OCD) is one of the most prevalent comorbidities in anorexia nervosa (AN; [1]). Besides phenomenological overlaps between the two conditions (e.g., ritualized behavior, cognitive rigidity), there is also a substantial shared genetic basis [2, 3]. Yet, as AN is a severe, life-threatening condition, reducing obsessive–compulsive symptomatology is not the primary objective during treatment of AN. Specifically, treatment of AN focuses on weight restoration along with addressing AN symptoms such as restrictive eating, weight and shape concerns, or compulsive exercise [4]. Although less severe cases of AN are treated in out patient or daypatient settings, more severe cases or those who do not respond to these treatments require inpatient treatment [5, 6]. There is a plethora of studies showing that inpatient treatment leads to a substantial gain in body weight and reductions in other AN symptoms in both adolescents and adults (e.g., [7,8,9,10,11]). However, few studies have examined if inpatient treatment also leads to decreases in obsessive–compulsive symptoms, if these symptoms remain unchanged or if they even increase in terms of a “symptom shift” [12].
In a sample with mixed eating disorder diagnoses (that only included 10 AN patients with and 17 AN patients without comorbid OCD), Thiel and colleagues [13] reported that obsessive–compulsive symptoms decreased from psychodynamic inpatient treatment to 30-months follow up only in those with comorbid OCD but not in those without comorbid OCD. The absence of changes in obsessive–compulsive symptoms in the latter group may be explained by the fact that they already had relatively low scores at admission. Furthermore, larger improvements in eating disorder symptoms related to larger improvements in obsessive–compulsive symptoms in this study. In contrast, Mattar and colleagues [14] reported no significant changes in obsessive–compulsive symptoms from admission to discharge in a sample of 24 inpatients with AN. Yet, Lee and colleagues [15] reported significant decreases in obsessive–compulsive symptoms from pre- to post-treatment in a sample with mixed eating disorder diagnoses at a residential treatment facility. Most recently, Pleplé and colleagues [16] reported significant decreases in obsessive–compulsive symptoms from admission to discharge in a large sample (n = 167) of inpatients with AN.
To summarize these four studies, two found that obsessive–compulsive symptoms decreased during treatment, one did not find that obsessive–compulsive symptoms decreased during treatment, and one found that obsessive–compulsive symptoms only decreased in those with comorbid OCD. Thus, although there is some evidence suggesting that obsessive–compulsive symptoms decrease during eating disorder treatment, findings are rather inconsistent. In addition, these findings were derived from different samples (two with AN patients and two with mixed eating disorder diagnoses) and involved different treatments. Furthermore, only one study in a sample with mixed eating diagnoses examined whether changes in obsessive–compulsive symptoms related to changes in eating disorder symptoms. Thus, it is currently unclear if obsessive–compulsive symptoms decrease during inpatient AN treatment, whether they only (or more strongly) change in those with comorbid OCD, and whether changes in obsessive–compulsive symptoms relate to changes in AN symptomatology.
In this retrospective analysis, we analyzed clinical records from 149 inpatients with AN and examined three research questions. First, based on the findings by Pleplé and colleagues [16], we expected that obsessive–compulsive symptoms would decrease from admission to discharge. Second, based on the findings by Thiel and colleagues [13], we hypothesized that decreases in obsessive–compulsive symptoms would be larger in patients with comorbid OCD than in patients without comorbid OCD. Third, based on the findings by Thiel and colleagues [13] who found that larger reductions in obsessive–compulsive symptoms related to related to larger decreases in eating disorder symptoms, we hypothesized that larger reductions in obsessive–compulsive symptoms would also relate to larger weight gain.
Methods
General study description
In this retrospective study, data from patients with AN who received inpatient treatment at the Schoen Clinic Roseneck (Prien am Chiemsee, Germany) between January 2015 and September 2021 and who completed the German version [17] of the Obsessive–Compulsive Inventory–Revised (OCI–R; [18]) at admission and discharge were analyzed. The OCI–R is not part of the routine diagnostic assessment for AN patients but is completed by patients upon request by their therapists if exploratory questions suggest that there might be an obsessive–compulsive symptomatology and, therefore, further evaluation of obsessive–compulsive symptoms is deemed necessary. At the Schoen Clinic Roseneck, data from the diagnostic assessments (e.g., age, sex, body weight and height, length of stay, diagnoses, questionnaire scores) are automatically transferred to a database from which they can be exported without any identifying information (e.g., name, date of birth, place of residence) by authorized employees. Thus, accessing individual patient charts is not necessary. According to the guidelines by the institutional review board of the LMU Munich, retrospective studies conducted on already available, anonymized data are exempt from requiring ethics approval. The data of this study are available at https://osf.io/k2g95.
Treatment description
The inpatient treatment offered at the hospital adheres to the German S3-guidelines for the treatment of AN [5, 19] in terms of admission criteria, treatment elements, and therapy goals. Thus, patients received a cognitive-behavioral therapy-oriented, multimodal AN treatment that included several treatment elements such as individual psychotherapy sessions, group therapy sessions, exercise therapy, meal preparation classes, body image exposure, nutrition counseling, and food intake protocols as well as clinical management of medical complications. The treatment includes a high-calorie refeeding schedule (starting on the first day of treatment) that aims at a weight gain of 0.7–1.0 kg per week for all underweight AN patients. This schedule includes three meals per day, each having approximately 700 kcal and, thus, totaling to a daily caloric intake of approximately 2100 kcal. Meals are supervised by a nurse or therapist in earlier treatment stages. The schedule is individually tailored if patients do not finish their meals or do not show the expected weight gain by increasing portion size, adding snacks between meals, or offering sip feeds. As normalization of eating behavior is one of the therapeutic goals, patients do not receive nasogastric feeding. Patients can choose between vegetarian and non-vegetarian menus; vegan menus are not offered.
Sample description
Between January 2015 and September 2021, 4350 cases with a primary diagnosis of full syndrome AN (ICD–10 code F50.0; n = 3808, 87.5%) or atypical AN (ICD–10 code F50.1; n = 542, 12.5%) were treated at the hospital. Of these, 486 patients (11.2%) were diagnosed with comorbid OCD (ICD–10 code F42) and 3864 patients (88.8%) had no comorbid OCD. For a subset of 149 patients, OCI–R scores were available both at admission and discharge. Of these, 132 patients (88.6%) were diagnosed with full syndrome AN and 17 had atypical AN (11.4%). One-hundred and one patients (67.8%) were diagnosed with comorbid OCD and 48 patients (32.2%) had no comorbid OCD.Footnote 1 Six patients (4.0%) were male. Mean age was 18.6 years (SD = 5.88; 96 adolescents, 64.4%; 53 adults, 35.6%).Footnote 2 Mean body mass index (BMI) was 15.2 kg/m2 (SD = 2.05) at admission and 18.0 kg/m2 (SD = 1.68) at discharge. Mean length of stay was 124 days (SD = 48.5).
OCI–R
The OCI–R assesses obsessive–compulsive symptoms with 18 items. Responses are recorded on a five-point scale from 0 = not at all to 4 = extremely. Higher sum scores indicate higher obsessive–compulsive symptomatology. A score of 21 has been found to optimally discriminate between patients with OCD and persons without OCD [18]. Internal reliability (McDonald’s omega; cf. [20]) was ω = 0.864 at admission and ω = 0.891 at discharge in the current study.
Data analyses
Changes in OCI–R scores from admission to discharge were tested with a paired samples t-test. Changes in OCI–R scores from admission to discharge as a function of comorbid OCD were tested with analysis of variance for repeated measures with the factors time (admission vs. discharge) and group (comorbid vs. no comorbid OCD). The within-person association between changes in OCI–R scores from admission to discharge and changes in BMI from admission to discharge was tested by computing a repeated measures correlation coefficient with the R-package rmcorr [21].
Results
Changes in obsessive−compulsive symptoms from admission to discharge
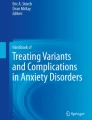
OCI−R scores decreased from admission (M = 26.4, SD = 13.5) to discharge (M = 24.4, SD = 14.1; t(148) = 3.20, p = 0.002, d = 0.26; Fig. 1).

Mean sum scores of the Obsessive–Compulsive Inventory–Revised at admission and discharge in the total sample and as a function of comorbid and no comorbid obsessive–compulsive disorder (OCD). Error bars indicate standard errors of the mean. The black dotted line indicates the cut-off score of 21 that has been found to optimally discriminate between persons with and without obsessive–compulsive disorder in the study by Foa and colleagues [18]
Changes in obsessive−compulsive symptoms from admission to discharge as a function of comorbid OCD
The interaction group × time was not significant (F(1,147) = 0.72, p = 0.397, ηp2 = 0.005), indicating that the size of changes in OCI−R scores from admission to discharge did not differ between groups (Fig. 1). Of note, although scores decreased in both groups, they were still above the cut-off score of 21 in those with comorbid OCD at discharge (Fig. 1).
Within-person association between body weight and obsessive−compulsive symptoms across admission and discharge
The repeated measures correlation between BMI and OCI–R scores was rrm = − 0.266 (p = 0.001, 95%CI[− 0.109; − 0.410]; Fig. 2), indicating that within-person weight gain was associated with decreases in obsessive–compulsive symptoms.

Rmcorr plot depicting within-person associations across admission and discharge between body mass index and scores of the Obsessive–Compulsive Inventory–Revised. Note that, in rmcorr, separate parallel lines are fit to the data from each person and the sign of the rmcorr coefficient is indicated by the direction of the common regression slope. In the rmcorr plot, each patient’s data and corresponding line are shown in different color. This is done because rmcorr can capture strong intra-individual relationships (here: between body weight and obsessive–compulsive symptoms across the two measurement time points) that are missed by using averaged data. As can be seen by the negative rmcorr coefficient (rrm = − .27) and the negative slopes of the individual fit lines, larger weight gain was associated with decreases in obsessive–compulsive symptoms
Discussion
Summary of findings
In this retrospective analysis, obsessive–compulsive symptoms significantly decreased during inpatient treatment of AN. The magnitude of this decrease was small and was similar in patients with and without comorbid OCD. Although obsessive–compulsive symptoms decreased, average scores were still clinically elevated in those with comorbid OCD at discharge. Larger decreases in obsessive–compulsive symptoms related to larger weight gain with a small effect size, suggesting that decreases in AN symptomatology do not result in a “symptom shift”, that is, do not facilitate obsessive–compulsive symptomatology.
Clinical implications
The finding that obsessive–compulsive symptoms decrease during AN treatment and relate to general changes in AN symptoms may be partially explained by overlapping features of both conditions. For example, both AN and OCD share several phenotypic, epidemiological, and neuropsychological characteristics such as excessive habit formation, cognitive rigidity, and repetitive and ritualistic behaviors [22, 23]. Thus, treating AN symptoms may also generalize to alter obsessive–compulsive symptoms that are not related to food, eating, and body weight because of their close phenomenological—but maybe also etiological—connection [2, 3].
Intervention techniques that target these central, overlapping features of both conditions may be particularly effective in the treatment of AN. Indeed, cognitive remediation therapy—originally developed as a treatment for schizophrenia—has been adapted for eating disorders as an add-on treatment element [24]. Amongst others, it addresses cognitive rigidity by using cognitive exercises to increase set-shifting abilities (i.e., increase cognitive flexibility) and to promote a more global information processing (i.e., decrease extreme attention to details). While some pilot studies found beneficial effects of cognitive remediation therapy in patients with AN, however, overall findings have been mixed [25]. In fact, two recent randomized controlled trials did not find that cognitive remediation therapy as an add-on to treatment as usual improved clinical and cognitive outcomes when compared to an active control condition [22, 26]. Thus, further research is necessary that examines if targeting obsessive–compulsive features of AN with cognitive remediation therapy has actual benefits over and above traditional psychotherapeutic approaches such as cognitive-behavioral therapy.
Limitations
Several factors limit interpretation of the current findings. As this was a retrospective analysis of clinical records, diagnoses were not confirmed by a structured clinical interview, which may be more precise than clinical diagnoses. However, the prevalence of comorbid OCD diagnoses (11%) matches well with prevalence rates that have been recently reported in a recent meta-analytic investigation [1], suggesting that OCD diagnoses were not under- or overestimated in the current study. Further, OCI–R scores were primarily available for those with comorbid OCD, which may have introduced a bias as the current sample was not representative of all treated cases with AN (i.e., although only 11% of all AN cases had comorbid OCD, 68% of all analyzed cases with available OCI–R scores had comorbid OCD). Finally, the current sample included both full syndrome and atypical AN patients as well as both males and females but the subgroups of atypical AN patients and males were too small to allow for testing whether changes in obsessive–compulsive symptoms differed between these groups. Yet, at least for the differentiation between full syndrome and atypical AN, it has been previously been reported that these groups do not show substantial differences in obsessive–compulsive symptoms [27].
Conclusion
The current study shows that obsessive–compulsive symptoms decrease during inpatient treatment of AN (although these are not a primary treatment target) and these decreases are associated with increases in body weight. Of note, effect sizes were small and patients with comorbid OCD still had clinically elevated obsessive–compulsive symptomatology at discharge, suggesting that obsessive–compulsive symptoms should be targeted with OCD-specific treatment elements in psychotherapeutic aftercare.
Availability of data and materials
The data of this study are available at https://osf.io/k2g95.
Notes
Note that patients with and without comorbid OCD did not differ in age (t(147) = 1.16, p = .246, d = 0.20) and length of stay (t(147) = 0.55, p = .585, d = 0.10). Groups also did not differ in BMI (main effect of group: F(1,147) = 0.03, p = .866, ηp2 < .001) and changes in BMI from admission to discharge (group × time interaction: F(1,147) = 0.04, p = .835, ηp2 < .001). Similarly, BMI was uncorrelated with OCI–R scores at admission (r = .076, p = .357).
Note that adolescents and adults did not differ in OCI–R scores (main effect of group: F(1,147) = 0.72, p = .396, ηp2 = .005) and changes of OCI–R scores from admission to discharge (group × time interaction: F(1,147) < 0.01, p = .963, ηp2 < .001). Similarly, age was uncorrelated with OCI–R scores at admission (r = .055, p = .504).
References
Drakes DH, Fawcett EJ, Rose JP, Carter-Major JC, Fawcett JM. Comorbid obsessive-compulsive disorder in individuals with eating disorders: an epidemiological meta-analysis. J Psychiatr Res. 2021;141:176–91.
Cederlöf M, Thornton LM, Baker J, Lichtenstein P, Larsson H, Rück C, et al. Etiological overlap between obsessive-compulsive disorder and anorexia nervosa: a longitudinal cohort, multigenerational family and twin study. World Psychiatr. 2015;14:333–8.
Yilmaz Z, Halvorsen M, Bryois J, Yu D, Thornton LM, Zerwas S, et al. Examination of the shared genetic basis of anorexia nervosa and obsessive–compulsive disorder. Mol Psychiatr. 2020;25:2036–46.
Byrne S, Wade T, Hay P, Touyz S, Fairburn CG, Treasure J, et al. A randomised controlled trial of three psychological treatments for anorexia nervosa. Psychol Med. 2017;47(16):2823–33.
Resmark G, Herpertz S, Herpertz-Dahlmann B, Zeeck A. Treatment of anorexia nervosa—new evidence-based guidelines. J Clin Med. 2019;8(2):153.
Anderson LK, Reilly EE, Berner L, Wierenga CE, Jones MD, Brown TA, et al. Treating eating disorders at higher levels of care: overview and challenges. Curr Psychiatr Rep. 2017;19(8):48.
Meule A, Schrambke D, Furst Loredo A, Schlegl S, Naab S, Voderholzer U. Inpatient treatment of anorexia nervosa in adolescents: a one-year follow up study. Eur Eat Disord Rev. 2021;29:165–77.
Schlegl S, Diedrich A, Neumayr C, Fumi M, Naab S, Voderholzer U. Inpatient treatment for adolescents with anorexia nervosa: clinical significance and predictors of treatment outcome. Eur Eat Disord Rev. 2016;24:214–22.
Schlegl S, Quadflieg N, Löwe B, Cuntz U, Voderholzer U. Specialized inpatient treatment of adult anorexia nervosa: effectiveness and clinical significance of changes. BMC Psychiatr. 2014;14(258):1–12.
Dalle Grave R, Calugi S, El Ghoch M, Conti M, Fairburn CG. Inpatient cognitive behavior therapy for adolescents with anorexia nervosa: immediate and longer-term effects. Front Psych. 2014;5:14.
Dalle Grave R, Conti M, Calugi S. Effectiveness of intensive cognitive behavioral therapy in adolescents and adults with anorexia nervosa. Int J Eat Disord. 2020;53:1428–38.
Garke M, Sörman K, Jayaram-Lindström N, Hellner C, Birgegård A. Symptom shifting and associations with mental illness: a transdiagnostic approach applied to eating disorders. J Abnorm Psychol. 2019;128:585–95.
Thiel A, Züger M, Jacoby GE, Schüßler G. Thirty-month outcome in patients with anorexia or bulimia nervosa and concomitant obsessive-compulsive disorder. Am J Psychiatr. 1998;155(2):244–9.
Mattar L, Thiébaud M-R, Huas C, Cebula C, Godart N. Depression, anxiety and obsessive–compulsive symptoms in relation to nutritional status and outcome in severe anorexia nervosa. Psychiatr Res. 2012;200(2):513–7.
Lee EB, Barney JL, Twohig MP, Lensegrav-Benson T, Quakenbush B. Obsessive compulsive disorder and thought action fusion: relationships with eating disorder outcomes. Eat Behav. 2020;37: 101386.
Pleplé A, Lalanne C, Huas C, Mattar L, Hanachi M, Flament MF, et al. Nutritional status and anxious and depressive symptoms in anorexia nervosa: a prospective study. Sci Rep. 2021;11(1):771.
Gönner S, Leonhart R, Ecker W. Das Zwangsinventar OCI-R - die deutsche version des obsessive-compulsive inventory-revised. Psychother Psychosom Med Psychol. 2007;57:395–404.
Foa EB, Huppert JD, Leiberg S, Langner R, Kichic R, Hajcak G, et al. The obsessive-compulsive inventory: development and validation of a short version. Psychol Assess. 2002;14:485–96.
Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften. S3-Leitlinie Diagnostik und Behandlung der Essstörungen. Berlin: AWMF; 2020.
Hayes AF, Coutts JJ. Use omega rather than Cronbach’s alpha for estimating reliability. But…. Commun Methods Meas. 2020;14(1):1–24.
Bakdash JZ, Marusich LR. Repeated measures correlation. Front Psychol. 2017;8:456.
van Passel B, Danner UN, Dingemans AE, Aarts E, Sternheim LC, Becker ES, et al. Cognitive remediation therapy does not enhance treatment effect in obsessive-compulsive disorder and anorexia nervosa: a randomized controlled trial. Psychother Psychosom. 2020;89(4):228–41.
Serpell L, Livingstone A, Neiderman M, Lask B. Anorexia nervosa: Obsessive–compulsive disorder, obsessive–compulsive personality disorder, or neither? Clin Psychol Rev. 2002;22(5):647–69.
Tchanturia K, Lock J. Cognitive remediation therapy for eating disorders: development, refinement and future directions. In: Adan RAH, Kaye WH, editors. Behavioral neurobiology of eating disorders. Berlin, Heidelberg: Springer; 2011. p. 269–87.
Hagan KE, Christensen KA, Forbush KT. A preliminary systematic review and meta-analysis of randomized-controlled trials of cognitive remediation therapy for anorexia nervosa. Eat Behav. 2020;37: 101391.
Brockmeyer T, Schmidt H, Leiteritz-Rausch A, Zimmermann J, Wünsch-Leiteritz W, Leiteritz A, et al. Cognitive remediation therapy in anorexia nervosa—a randomized clinical trial. J Consult Clin Psychol. 2021;89(10):805–15.
Levinson CA, Brosof LC, Ram SS, Pruitt A, Russell S, Lenze EJ. Obsessions are strongly related to eating disorder symptoms in anorexia nervosa and atypical anorexia nervosa. Eat Behav. 2019;34: 101298.
Acknowledgements
Not applicable.
Funding
Open Access funding enabled and organized by Projekt DEAL. No funding was received for this study.
Author information
Authors and Affiliations
Contributions
AM prepared and analyzed the data and wrote the first draft of the manuscript. UV conceptualized the study and revised the manuscript for content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
According to the guidelines by the institutional review board of the LMU Munich, retrospective studies conducted on already available, anonymized data are exempt from requiring ethics approval.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Meule, A., Voderholzer, U. Changes in obsessive–compulsive symptoms during inpatient treatment of anorexia nervosa. J Eat Disord 10, 106 (2022). https://doi.org/10.1186/s40337-022-00629-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40337-022-00629-3