
Abstract
Background
Immunization is one of the most far-reaching and cost-effective strategies for promoting good health and saving lives. A complex immunization schedule, however, may be burdensome to parents and lead to reduced vaccine compliance and completion. Thus, it is critical to develop combination vaccines to reduce the number of injections and simplify the immunization schedule. This study aimed to investigate the current status of the pentavalent diphtheria-tetanus-acellular pertussis inactivated poliomyelitis and Haemophilus influenzae type B conjugate (DTaP-IPV/Hib) vaccination in Southern China as well as explore the factors in the general population associated with uptake and the differences between urban and rural populations.
Methods
A cross-sectional study was conducted with recently enrolled kindergarten students in Hainan Province between December 2022 and January 2023. The study employed a stratified multistage cluster random sampling method. Information regarding the demographic characteristics and factors that influence decisions were collected from the caregivers of children via an online questionnaire. Multivariate logistic regression was used to determine the factors associated with the status of DTap-IPV/Hib vaccinations.
Results
Of the 4818 valid responses, 95.3% of children were aged 3–4 years, and 2856 (59.3%) held rural hukou. Coverage rates of the DTaP-IPV/Hib vaccine, from 1 to 4 doses, were 24.4%, 20.7%, 18.5%, and 16.0%, respectively. Caregivers who are concerned about vaccine efficacy [adjusted odds ratio (aOR) = 1.53, 95% confidence interval (CI): 1.30–1.79], the manufacturer (aOR = 2.05, 95% CI: 1.69–2.49), and a simple immunization schedule (aOR = 1.26, 95% CI: 1.04–1.54) are factors associated with a higher likelihood of vaccinating children against DTaP-IPV/Hib. In addition, caregivers in urban areas showed more concern about the vaccine price (P = 0.010) and immunization schedule (P = 0.022) in regard to vaccinating children.
Conclusions
The DTaP-IPV/Hib vaccine coverage rate in Hainan Province remains low. Factors such as lower socioeconomic status, cultural beliefs, concerns about vaccine safety, and cost may hinder caregivers from vaccinating their children. Further measures, such as health education campaigns to raise knowledge and awareness, and encouragement of domestic vaccine innovation, which would reduce out-of-pocket costs, could be implemented to improve the coverage of DTap-IPV/Hib vaccination.
Graphical Abstract

Similar content being viewed by others

Background
Early child development (ECD) is an essential element of the Sustainable Development Goals and serves as the foundation of adult health and well-being [1]. Although substantive progress has been made in tackling under-5 mortality, with a reduction in the number of childhood deaths from 5.9 million in 2015 to 5 million in 2021, many children who survive are not able to thrive due to the threat of infectious diseases [2]. Among the five major areas of ECD, the area of health emphasizes childhood immunization. Vaccines annually prevent 2–3 million fatalities and safeguard millions more from disease and disability [3]. As one of the most far-reaching health interventions, immunization is an incredibly cost-effective strategy for promoting good health and saving lives. A study in 94 low- and middle-income countries estimated that every US dollar (USD) 1 invested in immunization generates a return of USD 51.8 in broader societal benefits of people who live longer and healthier lives [4].
The World Health Organization (WHO) developed Immunization Agenda 2030 to reduce mortality and morbidity from vaccine-preventable diseases (VPDs) from the period of 2021 to 2030 [5]. The current National Immunization Program (NIP) in China provides, at no cost, vaccines for eligible-aged children to prevent 12 VPDs and reduce by 99% the incidence of these diseases [6]. In addition, the number of recommended vaccines during childhood has increased significantly. Currently, children can receive ~ 20 injections by the age of 2 years to complete their immunization schedule, although the number of injections may increase in the coming years due to an increasing number of new diseases and vaccines. Evidence suggests, however, that a complex immunization schedule may be burdensome to parents and healthcare providers and can even lead to reduced vaccine compliance and completion [7, 8].
To address these concerns, many international organizations recommend that countries develop combination vaccines, which can be produced by grouping multiple antigens into one injection [9, 10]. In 2010, the Chinese National Medical Products Administration approved the pentavalent diphtheria-tetanus-acellular pertussis inactivated poliomyelitis and Haemophilus influenzae type B conjugate vaccine (DTaP-IPV/Hib) (Pentaxim®, Sanofi Pasteur Limited, Marcy l’Etoile, France), which can prevent more than five high incidences of morbidity and mortality diseases [11]. Until now, it was the highest degree of combination vaccines available in China. Numerous studies have demonstrated the good immunogenicity and safety profile of the DTaP-IPV/Hib combination vaccine, which is equal to the separately administered vaccine components [12, 13]. The DTaP-IPV/Hib combination vaccine offers a safe and effective alternative for reducing the number of injections from 12 to 4, which can reduce pain and discomfort and prevent potential side effects for children, save time and money, and reduce the loss of productivity for caregivers [14, 15]. Notably, China, as the sole WHO member country that has not incorporated the Hib vaccine into its NIP, exhibits a relatively low national coverage rate of only 33%, thereby experiencing a significant residual burden of Hib disease [16]. The use of the DTaP-IPV/Hib combination vaccine could contribute to enhancing Hib coverage, which allows for better and wider protection against infectious diseases and decreases the cost of disease management [17].
The DTap-IPV/Hib vaccination rates in many developed countries are far higher and were 94.4% in England and over 93.7% in Canada [18, 19]. The vaccine is imported, optional, and self-paid (Category 2), and the DTap-IPV/Hib vaccination rate in China significantly varies across different regions, but the overall rates are low. According to previous studies, the DTap-IPV/Hib vaccine coverage exhibited variations, with rates that range from 18.51% in Hangzhou during 2017 to 6.28% in Chongqing during 2015 [20, 21]. Considering the financial responsibility of caregivers in China to fully cover the cost of the DTap-IPV/Hib vaccine through out-of-pocket payments, it becomes imperative to assess the actual immunization status and the factors that influence DTap-IPV/Hib vaccine uptake within the country. Nevertheless, it is unfortunate that there is a lack of comprehensive information available about the utilization of the DTap-IPV/Hib vaccine and the factors that influence its uptake within the Chinese context.
In 2018, the Chinese government made the strategic decision to establish Hainan Province as the nation’s inaugural free trade port, operating under the socialist system. To facilitate the importation of pharmaceuticals and sanitary equipment, Hainan Free Trade Port (HFTP) has implemented a range of convenient and preferential laws and policies. This development is expected to enhance the accessibility of imported vaccines for local residents [22]. Hence, this study aimed to investigate the current status of DTap-IPV/Hib vaccination in Hainan Province as an example and explore the potential influencing factors in the general population as well as the differences between urban and rural populations. The study also sought to provide recommendations for increasing the vaccination rate, including tailored preparation to address hesitancy, and build vaccine literacy in China.
Methods
Study design and ethic
This study is part of a larger cross-sectional survey on the intervention strategies for ECD, which includes, among others, immunization, responsive caregiving, and early learning. The survey was conducted with a population of newly enrolled kindergarteners in Hainan Province from December 12, 2022, to January 8, 2023. Although it is mandatory for all 3-year-old children who reside in Hainan Province to enroll in kindergarten, there may be variations in the actual age at which they are enrolled (95% of the children were 3–4 years old, but there were a few children who were 2 or 5 years old). Ethics approval was obtained from the Research Ethics Board of the Hainan Women and Children’s Medical Center (2020-002). This paper includes data only from vaccination surveys and uses components of the cross-sectional questionnaire relevant to the aims of this paper.
Study participants and randomization
Newly enrolled kindergarteners in Hainan Province in 2022 were recruited, and those who had foreign nationality or studied in special education schools were excluded. A stratified multistage cluster random sampling approach was employed for the cross-sectional study. First, primary sampling units (PSUs) were set at the county-level administrative region. There are a total of 3 groups and 24 categories of PSUs, including 8 municipal districts, 6 county-level cities, and 10 counties/autonomous counties. Half of the units in each group were randomly selected.
We then defined secondary sampling units (SSUs) based on the kindergarten’s ownership (public or private) and level (provincial/demonstration level; first, second, or third level in city/county; and unrated level). There are a total of 120 categories of SSUs. In each SSU, one or two kindergartens were randomly selected, and all the enrolled children in the junior grade were invited to participate in the survey (Fig. 1). Random sampling was conducted, using a list of random numbers, by an individual epidemiologist who was not involved in any other research activities of this survey. A total of 8478 children from 180 kindergartens were randomly selected as participants. All caregivers of children who participated in the study were informed about the intention of the study and gave their electronic informed consent at the beginning of the online survey.

Stratified sample units of kindergartens of different levels in Hainan. There are 4 prefecture-level cities, 5 county-level cities, and 10 counties/autonomous counties in the Hainan administrative division. Among the 4 prefecture-level cities, there are 4 municipal districts each in Haikou and Sanya Cities. Danzhou City is taken as a county-level city, as it governs only streets and towns. We deleted Sansha City due to underpopulation. Thus, there is a total of 3 groups and 24 categories of primary sampling units, including 8 municipal districts, 6 county-level cities, and 10 counties/autonomous counties
Sample size and power analysis
The sample size was calculated with the following formula based on an error α = 0.05, \(Z_{1 - \alpha /2}\) = 1.96, and allowance error δ = 0.02: \(n = \left( {\frac{{Z_{1 - \alpha /2} }}{\delta }} \right)^{2} \times p \times \left( {1 - p} \right)\). Based on the whole ECD study, we adopted the early Human Capability Index to more comprehensively assess the development of children. In accordance with our preliminary pilot study, the estimated risk of poor development was found to be 18%, which is slightly lower than the average rate of 20%, observed within the Chinese population [23]. Assuming a conservative estimate of 20% for the risks of poor development in Hainan, we determined that the calculated sample size required was 1537. After estimating 70% valid data, the total number of participants was expected to be 2196.
Data collection and quality control
Based on a review of the literature, we developed a structured questionnaire to collect data on demographic characteristics and factors that influence the choices of the DTaP-IPV/Hib vaccine. We implemented expert consultation to ensure the scientific validity and rationale of the questionnaire. We then conducted a pilot study with a random sample of 128 caregivers in two kindergartens to ensure the comprehension of the questionnaire. After the pilot study, a few modifications were made to ensure that the questions were comprehensible and interpreted as intended. The results of the pilot study were not included in the main study.
The data collection was carried out by the Maternal and Children Health Care System in Hainan Province, China. At the beginning of the survey, we provided standard training for the head of each PSU, who then provided training and guidance to the kindergartens within their jurisdiction to ensure that they carried out this survey, following the uniform process. The kindergarten representatives were responsible for checking the children’s personal information and guiding parents or caregivers to finish the online survey within two weeks.
In addition, a web-based questionnaire and research management platform were set up. The selected kindergartens were requested to upload the properly formatted information about their children (including name, gender, kindergarten, class, and date of birth) to the questionnaire platform, and the questionnaire platform generated a unique login code for each child [24]. Both the link to the research and the unique login code were distributed to parents through the Maternal and Children Health Care System and kindergarten teachers. The questionnaire collection process is strictly quality controlled by various levels of regulatory systems. Using the login code, all parents accessed the online questionnaire to double-check the child’s personal information and gave informed consent to participate in the survey.
After collecting questionnaires, we excluded those with missing important and obvious logical errors. Valid data with complete basic information and DTaP-IPV/Hib vaccination status were included in the analysis.
Measures
Using the researcher-designed questionnaire, we obtained the general demographic characteristics of the participants, including children’s age, gender, hukou (the location of registered residency of the child), and ethnic group; administrative division, rank, and type of kindergartens; premature delivery, basic medical insurance, commercial medical insurance, number of children in the family, and previous vaccination status in NIP; caregivers’ relationship with the children, education level, and employment status; and annual household income.
Acceptance of vaccination is an outcome behavior that results from a complex decision-making process that can be potentially influenced by a wide range of factors. As caregivers play a key role in vaccination, we also assessed their influence using the “3Cs” model, which was first proposed to the WHO EURO Vaccine Communications Working Group in 2011. The “3Cs” model is a professionally validated theoretical framework for vaccination determinants, comprised of confidence, convenience, and complacency factors [25]. We designed eight questions that were incorporated into the 3Cs in our study. To make subsequent analysis clearer, we categorized responses into two categories: “Yes” or “No.”
Statistical analysis
All variables were categorical and represented as frequencies with percentages. The characteristics of participants who had previously been vaccinated for DTaP-IPV/Hib and those who had not were compared using a chi-square test.
The relationship between the explanatory variables (demographic characteristics of caregivers and children) and the outcome variable (vaccinating their children against DTaP-IPV/Hib) was examined by multivariate logistic regression. The outcome variable was dichotomized into “Vaccinated” (at least 1 dose) and “Unvaccinated.” An adjusted odds ratio (aOR) with a 95% confidence interval (CI) for each variable were calculated.
A comprehensive non-responder analysis was conducted. The available data from the Hainan Women and Children’s Medical Center system were used to conduct an analysis of non-response to evaluate whether the non-responders differed systematically from the responders of the survey. Then, a subgroup analysis was performed, which examined differences in the variables among the groups. All statistics were managed by Microsoft Excel version 2010 (Microsoft Corporation, Redmond, WA, USA) and analyzed using SPSS version 24.0 (SPSS Inc., Chicago, IL, USA). Two-sided P-values < 0.05 were considered significant.
Results
Demographic characteristics of respondents
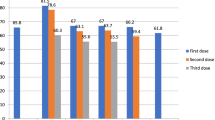
A total of 4818 valid questionnaires were analyzed in this study, for a valid response rate of 56.8% (Fig. 2). Of the 4818 responses, most were aged ≤ 3 years (75.2%), the majority were from the Han population (80.4%), and 2856 (59.3%) held rural hukou. Almost two-thirds of the families had more than one child (66.1%), and the vast majority (92.5%) of children completed the immunization program of Hainan Province at the target age. Among the respondents, mothers predominated (75.3%), 70.0% of the caregivers were employed, and 31.6% had a 4-year college or associate’s degree. With regard to non-NIP vaccine determinants, the safety (51.0%) and efficacy (44.1%) of the vaccine are the two core issues with which caregivers have always been concerned, and more than one-third (39.3%) of caregivers depend heavily on doctors’ vaccination advice. Details are provided in Table 1.

Flowchart of sample selection
Factors associated with DTaP-IPV/Hib vaccination
The immunization coverage rates of the DTaP-IPV/Hib vaccine, from 1 to 4 doses, were 24.4%, 20.7%, 18.5%, and 16.0%, respectively, in Hainan Province. In the multivariate regression model, DTaP-IPV/Hib vaccination status differed significantly in terms of the children’s hukou (P < 0.001), and ethnic group (P < 0.001); administrative division (P < 0.001) and rank of kindergartens (P < 0.001); basic medical insurance (P < 0.004), commercial medical insurance (P < 0.001), and previous vaccination status in NIP (P < 0.001); caregivers’ education level (P < 0.001) and employment status (P < 0.045); and annual household income (P < 0.003). We then adjusted all socioeconomic and demographic characteristics of respondents. Caregivers who feel positively toward vaccine efficacy (aOR = 1.53, 95% CI: 1.30–1.79), the manufacturer (aOR = 2.05, 95% CI: 1.69–2.49), and immunization schedule (aOR = 1.26, 95% CI: 1.04–1.54) are more likely to vaccinate their children against DTaP-IPV/Hib. Those who are more concerned about vaccine safety (aOR = 0.58, 95% CI: 0.50–0.68) and price (aOR = 0.73, 95% CI: 0.60–0.88) are less likely to vaccinate their children against DTaP-IPV/Hib (Table 2).
Assessing non-response bias
The analyses showed that responders (n = 4818) were comparable to non-responders (n = 3660) with regard to gender and age. Responders, however, were significantly more often of Han ethnicity and were county or autonomous county-, provincial-, or demonstration-level kindergarteners, or public kindergarteners compared to non-responders (P < 0.001) (Table 3). The subgroup analysis results for variables with differences are displayed in Additional file 1: Tables S1–S4.
Factors associated with DTaP-IPV/Hib vaccination in urban and rural areas
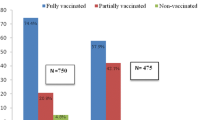
In China, hukou represents the location of the registered residency of the children, which is approximately equal to the living residence. Our results showed that caregivers in both urban and rural groups are concerned about vaccine safety, efficacy, and the manufacturer (P < 0.001). Disparities were observed, however, in terms of the convenience dimension related to vaccine price and immunization schedule. Specifically, the urban group exhibited greater concerns regarding vaccine price (P = 0.010) and adherence to the immunization schedule (P = 0.022) in terms of vaccination against DTaP-IPV/Hib (Fig. 3).

Factors associated with DTaP-IPV/Hib vaccination in urban and rural areas. We adjusted the socioeconomic and demographic characteristics of respondents. aOR adjusted odds ratio; CI confidence interval
Discussion
The vaccination of children, the main target population, can have far-reaching effects on general health and well-being, cognitive development, and economic productivity. More than 70 vaccines are available for use, and many more are expected to protect against multiple diseases, which will further increase the number of injections and office visits [8, 26]. Complex immunization schedules can result in missed or delayed dosing, especially for children under 2 years old. Thus, it is essential to develop combination vaccines to simplify the vaccine schedule. Although the DTaP-IPV/Hib vaccine is the highest degree of combination vaccines available in China, the coverage rates of this vaccine are still low. It is, thus, critical to explore the factors that affect the vaccination rate of DTaP-IPV/Hib. To our knowledge, this is the first large sample investigation of the immunization status and the influencing factors of the DTap-IPV/Hib vaccine in Hainan Province, which includes more than ten million permanent residents. Our findings show that the cumulative coverage rates of the DTap-IPV/Hib vaccine from 1 to 4 doses were 24.4%, 20.7%, 18.5%, and 16.0%, respectively, in Hainan Province, which was higher than other areas in China [20, 21].
Consistent with other studies, Voo et al. found that caregivers with higher economic and cultural levels are more likely to vaccinate their children against DTap-IPV/Hib [27]. This could be explained by research that shows that caregivers with higher economic and cultural levels are inclined to accurately process the evidence regarding vaccination and to have access to more healthcare resources, such as choosing self-paid vaccines [28]. The cost of an imported DTaP-IPV/Hib vaccine per fully immunized child is estimated to be 2488 Chinese Yuan (CNY), and it is paid out-of-pocket, without any subsidy or insurance coverage. This higher cost may impose a financial burden on families with a lower income, potentially limiting their access to the vaccine and reducing the likelihood of full compliance and completion (Additional file 1: Table S5). Previous research in China and Japan has found that a subsidy would reduce the out-of-pocket price and increase the coverage of vaccination [29, 30].
Currently, the advancement of combined vaccines in China is impeded by numerous technical challenges. These include the absence of the crucial component IPV in the market and the presence of thiomersal in the co-purification process utilized for manufacturing DTaP vaccines, which can adversely affect the immunogenicity of the IPV antigen [31]. To address these concerns, the government should not only develop innovative vaccine pricing mechanisms and increase financing options but also provide an incentive for domestic manufacturers to research and develop DTap-IPV/Hib vaccines. Moreover, region-specific strategies should be developed based on their disease burden and fiscal capacity [32].
Our findings reveal that the efficacy and safety of the DTap-IPV/Hib vaccine have played a significant role in influencing its uptake within the general population. Studies in five countries in South America have revealed that safety and efficacy were the two most important factors for caregivers to decide whether to vaccinate their children [33]. Accurate information about vaccines is vital for caregivers, as they often lack a complete understanding of how vaccines function and struggle to make well-informed decisions about vaccination. Research conducted by Boerner et al. has shown that insufficient information about vaccination or conflicting information from various sources can decrease an individual’s willingness to vaccinate [34]. Therefore, it is of the utmost importance to communicate information about vaccines in a clear and easily comprehensible manner to overcome barriers to vaccination [35]. Healthcare providers play a crucial role as trusted sources of information for caregivers, enabling them to enhance their understanding and awareness. France’s implementation experience highlights the effectiveness of health education campaigns led by reputable medical institutions. These campaigns serve as valuable strategies to provide credible and reliable information about the safety and efficacy of vaccines. The ultimate goal is to empower individuals to make informed decisions regarding vaccination and ensure accessible and comprehensive vaccine information and knowledge [36].
The findings of this study demonstrated a notable disparity in vaccination rates between urban (35.7%) and rural populations (16.6%). In addition, the study revealed that caregivers who expressed concerns about the immunization schedule were more inclined to vaccinate their children against DTaP-IPV/Hib, particularly among those who resided in urban areas. As a combination vaccine, the DTap-IPV/Hib vaccine could simplify the immunization schedule and reduce the total number of required office visits [37]. Our preliminary research found that the Hib vaccination coverage rate in Hainan Province is 39.7%. Among children who received the Hib vaccine, 61.5% opted for direct vaccination with the DTap-IPV/Hib vaccine (data have not been published). Due to conflicts between routine vaccination times and parents’ working hours, parents in urban areas prefer to pay higher fees to buy time. Time loss related to the number of office visits may prevent parents from completing the immunization schedule on time and result in missed or delayed dosing. Pellissier et al. provided evidence that reducing the number of office visits can lead to time savings and potentially lower indirect costs associated with parental work loss [15]. Overall, although combination vaccines may cost slightly more than the total cost of their component vaccines, the benefits of vaccination timeliness and compliance and a simplified schedule may outweigh the cost.
This study has several limitations. First, there is a non-response bias in the study results due to the lower response rate. Responders and non-responders may differ in their vaccination status. Thus, we collected the available data to conduct an analysis of non-responders and then conducted a subgroup analysis. Second, the confirmation of vaccination status was based on the caregivers’ self‐reports, which rely on memory rather than medical records. Hence, the information may not accurately reflect the DTaP-IPV/Hib vaccine coverage rate and may be subject to recall bias. Because the newly enrolled children are required to provide vaccination records upon admission to kindergarten in September, however, the probability is less that their parents do not remember or are uncertain about the DTaP-IPV/Hib vaccination status. Third, the sample was selected from one geographic area. The specific context of Hainan Province, which might not represent the whole population in China, could limit the generalizability of the findings. Further research should be undertaken to extend the scope to widely evaluate the vaccination rate and influencing factors in China. Despite the above limitations, this study provides important evidence by which to evaluate the vaccination status and popularization proposals of the DTaP-IPV/Hib vaccine in China.
Conclusions
Our study provides important evidence of the prevalence and determining factors of the DTaP-IPV/Hib vaccination in Hainan Province, China. The coverage rate of the DTaP-IPV/Hib vaccine in Hainan Province remains at a low level but is slightly higher than that found in previous studies conducted in China. Caregivers may be hesitant to vaccinate their children against DTaP-IPV/Hib due to concerns about the vaccine’s safety and price. Thus, more effective health education campaigns should be conducted to publicize and promote access to DTaP-IPV/Hib vaccine knowledge and awareness. Further, the government should provide an incentive for domestic manufacturers to research and develop DTap-IPV/Hib vaccines as well as provide innovative vaccine pricing mechanisms and increase financing options to address the cost concern.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ECD:
-
Early child development
- US dollars:
-
USD
- WHO:
-
World Health Organization
- VPDs:
-
Vaccine-preventable diseases
- NIP:
-
National Immunization Program
- DTaP-IPV/Hib:
-
Diphtheria-tetanus-acellular pertussis inactivated poliomyelitis and Haemophilus influenzae type B
- HFTP:
-
Hainan Free Trade Port
- PSUs:
-
Primary sampling units
- SSUs:
-
Secondary sampling units
- aOR :
-
Adjusted odd ratio
- CI :
-
Confidential interval
- CNY:
-
Chinese Yuan
References
Black MM, Walker SP, Fernald LCH, Andersen CT, DiGirolamo AM, Lu C, et al. Early childhood development coming of age: science through the life course. Lancet. 2017;389(10064):77–90.
You D, Hug L, Ejdemyr S, Idele P, Hogan D, Mathers C, et al. Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet. 2015;386(10010):2275–86.
GAVI. Sustainable Development Goals. https://www.gavi.org/our-alliance/global-health-development/sustainable-development-goals. Accessed 13 Apr 2023.
Sim SY, Watts E, Constenla D, Brenzel L, Patenaude BN. Return on investment from immunization against 10 pathogens in 94 low- and middle-income countries, 2011–30. Health Aff (Millwood). 2020;39(8):1343–53.
WHO. Immunization Agenda 2030: A Global Strategy to Leave No One Behind 2021. https://www.who.int/publications/m/item/immunization-agenda-2030-a-global-strategy-to-leave-no-one-behind. Accessed 20 Apr 2023.
Pan J, Wang Y, Cao L, Wang Y, Zhao Q, Tang S, et al. Impact of immunization programs on 11 childhood vaccine-preventable diseases in China: 1950–2018. Innovation (Camb). 2021;2(2): 100113.
Li H, Tan Y, Zeng H, Zeng F, Xu X, Liao Y, et al. Co-administration of multiple childhood vaccines—Guangdong Province, 2019. China CDC Weekly. 2020;2(1):13–5.
Wallace AS, Mantel C, Mayers G, Mansoor O, Gindler JS, Hyde TB. Experiences with provider and parental attitudes and practices regarding the administration of multiple injections during infant vaccination visits: lessons for vaccine introduction. Vaccine. 2014;32(41):5301–10.
General recommendations on immunization—recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2011;60(2):1–64.
Lu C, Michaud CM, Gakidou E, Khan K, Murray CJ. Effect of the global alliance for vaccines and immunisation on diphtheria, tetanus, and pertussis vaccine coverage: an independent assessment. Lancet. 2006;368(9541):1088–95.
Dhillon S, Keam SJ. DTaP-IPV/Hib vaccine (Pentacel). Paediatr Drugs. 2008;10(6):405–16.
Nakayama T, Vidor E, Tsuzuki D, Nishina S, Sasaki T, Ishii Y, et al. Immunogenicity and safety of a DTaP-IPV/Hib pentavalent vaccine given as primary and booster vaccinations in healthy infants and toddlers in Japan. J Infect Chemother. 2020;26(7):651–9.
Li Z, Xu J, Tan H, Zhang C, Chen J, Ni L, et al. Safety of pentavalent DTaP-IPV/Hib combination vaccine in post-marketing surveillance in Guangzhou, China, from 2011 to 2017. Int J Infect Dis. 2020;99:149–55.
Lieu TA, Black SB, Ray GT, Martin KE, Shinefield HR, Weniger BG. The hidden costs of infant vaccination. Vaccine. 2000;19(1):33–41.
Pellissier JM, Coplan PM, Jackson LA, May JE. The effect of additional shots on the vaccine administration process: results of a time-motion study in 2 settings. Am J Manag Care. 2000;6(9):1038–44.
Zhang H, Garcia C, Yu W, Knoll MD, Lai X, Xu T, et al. National and provincial impact and cost-effectiveness of Haemophilus influenzae type B conjugate vaccine in China: a modeling analysis. BMC Med. 2021;19(1):181.
Romanenko V, Osipova I, Galustyan A, Scherbakov M, Baudson N, Farhi D, et al. Immunogenicity and safety of a combined DTaP-IPV/Hib vaccine administered as a three-dose primary vaccination course and a booster dose in healthy children in Russia: a phase III, non-randomized, open-label study. Human Vacc Immunother. 2020;16(9):2265–73.
Public Health Agency of Canada. Immunization coverage against invasive pneumococcal disease among children in the capital health region of Alberta. https://www.canada.ca/en/public-health/services/reports-publications/canada-communicable-disease-report-ccdr/monthly-issue/2005-31/immunization-coverage-against-invasive-pneumococcal-disease-among-children-capital-health-region-alberta.html. Accessed 20 Apr 2023.
NHS Digital. Statistics published for all routine childhood vaccinations in England in 2021–22: statistical press release. https://digital.nhs.uk/news/2022/childhood-vaccinations-2021-22. Accessed 20 Apr 2023.
Yang J, Mao Y, Zhang Y, Zhang W. Immunization of category B vaccine and its influencing factors among children aged 0 to 6 in Hangzhou. Prev Med. 2018;30(06):574–7.
Hang L, Li T, Shao J, Yan Y, Zhang Y, Liu H, et al. Coverage status of category B vaccines and its influencing factors among preschoolers in Shapingba District, Chongqing City. Pract Prev Med. 2016;23(04):419–22.
Qi F, Wu Y, Wang J, Wang Q. China’s Hainan free trade port: medical laws and policy reform. Front Public Health. 2021;9: 764977.
Zhang Y, Kang L, Zhao J, Song PY, Jiang PF, Lu C. Assessing the inequality of early child development in China—a population-based study. Lancet Reg Health West Pac. 2021;14: 100221.
Wang X, Zhang Y, Zhao J, Shan W, Zhang Z, Wang G, et al. Cohort Profile: The Shanghai children’s health, education and lifestyle evaluation, preschool (SCHEDULE-P) study. Int J Epidemiol. 2021;50(2):391–9.
MacDonald NE. Hesitancy SWGoV. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4.
Shukla VV, Shah RC. Vaccinations in primary care. Indian J Pediatr. 2018;85(12):1118–27.
Voo JYH, Lean QY, Ming LC, Md Hanafiah NH, Al-Worafi YM, Ibrahim B. Vaccine knowledge, awareness and hesitancy: a cross sectional survey among parents residing at Sandakan District, Sabah. Vaccines (Basel). 2021;9(11):1348.
Charron J, Gautier A, Jestin C. Influence of information sources on vaccine hesitancy and practices. Med Maladies Infect. 2020;50(8):727–33.
Zhou L, Su Q, Xu Z, Feng A, Jin H, Wang S, et al. Seasonal influenza vaccination coverage rate of target groups in selected cities and provinces in China by season (2009/10 to 2011/12). PLoS ONE. 2013;8(9): e73724.
Kondo M, Yamamura M, Hoshi SL, Okubo I. Demand for pneumococcal vaccination under subsidy program for the elderly in Japan. BMC Health Serv Res. 2012;12:313.
Yang XM. A review of combined immunization: current research situation and its promising future. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(1):120–6 (In Chinese).
Hou Z, Jie C, Yue D, Fang H, Meng Q, Zhang Y. Determinants of willingness to pay for self-paid vaccines in China. Vaccine. 2014;32(35):4471–7.
Gonzalez-Block MA, Gutierrez-Calderon E, Pelcastre-Villafuerte BE, Arroyo-Laguna J, Comes Y, Crocco P, et al. Influenza vaccination hesitancy in five countries of South America. Confidence, complacency and convenience as determinants of immunization rates. PLoS ONE. 2020;15(12):e0243833.
Boerner F, Keelan J, Winton L, Jardine C, Driedger SM. Understanding the interplay of factors informing vaccination behavior in three Canadian provinces. Hum Vacc Immunother. 2013;9(7):1477–84.
Truong J, Bakshi S, Wasim A, Ahmad M, Majid U. What factors promote vaccine hesitancy or acceptance during pandemics? A systematic review and thematic analysis. Health Promot Int. 2022;37(1):daab105.
Pulcini C, Massin S, Launay O, Verger P. Factors associated with vaccination for hepatitis B, pertussis, seasonal and pandemic influenza among French general practitioners: a 2010 survey. Vaccine. 2013;31(37):3943–9.
Maman K, Zollner Y, Greco D, Duru G, Sendyona S, Remy V. The value of childhood combination vaccines: from beliefs to evidence. Hum Vacc Immunother. 2015;11(9):2132–41.
Acknowledgements
The author appreciates all participants for their time and involvement in this study. The work reported in this publication was supported by the Bill & Melinda Gates Foundation (INV-049539). Under the grant conditions of the Foundation, a Creative Commons Attribution 4.0 Generic License has been assigned to the author-accepted manuscript version that might arise from this submission. The funder did not play any role in the study design, data analysis, data interpretation, writing of the paper, or submission for this publication. The content in this paper is solely the responsibility of the authors and does not represent any view of the funder.
Funding
This work was supported by the Bill & Melinda Gates Foundation (Grant No. INV-049539); the Key Research and Development Program of Hainan Province (Grant No. ZDYF2020210); the Project of the National Social Science Fund of China (Grant No. 20BGL264); and the Shanghai Public Health System Construction Three‐Year Action Plan (Grant No. GWVI-11.1-48).
Author information
Authors and Affiliations
Contributions
YC, GL, and FJ designed and conceptualized the study. JX and YC drafted the first manuscript and contributed to the interpretation of the results. JX and CH were involved in data cleaning and data analysis. CH and YD collected the data and supervised the project administration. LF, GL, and FJ contributed to the revision of the manuscript and approved the final version. YC, LF, and FJ obtained funding. All the authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethics approval has been obtained from the Research Ethics Board of the Hainan Women and Children’s Medical Center (2020-002). All participants in the study were informed about the intention of the study and gave their electronic informed consent at the beginning of the online survey.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Supplementary Information
Additional file 1:
Table S1. Multivariate analysis of the potential factors that influence the DTaP-IPV/Hib vaccination by ethnicity. Table S2. Multivariate analysis of the potential factors that influence the DTaP-IPV/Hib vaccination by kindergarten rank. Table S3. Multivariate analysis of the potential factors that influence the DTaP-IPV/Hib vaccination by type of kindergarten. Table S4. Multivariate analysis of the potential factors that influence the DTaP-IPV/Hib vaccination by county-level administrative region. Table S5. Multivariate analysis of the potential factors that influence the full-course DTaP-IPV/Hib vaccination (N = 1174).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xu, J., Cui, Y., Huang, C. et al. Prevalence and factors associated with pentavalent vaccination: a cross-sectional study in Southern China. Infect Dis Poverty 12, 84 (2023). https://doi.org/10.1186/s40249-023-01134-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40249-023-01134-8