
Abstract
Background
Post-transplant lymphoproliferative disorder is a well-recognized but rare complication of hematopoietic stem cell and solid organ transplant. Due to rarity of this disease, retrospective studies from major transplant centers has been the main source to provide treatment guidelines, which are still in evolution. The sample size of this study is among one of the largest study on PTLD till date reported throughout the world.
Methods
This study was performed at University of Florida which is one of the largest transplant center in South East United States. We performed treatment and survival analysis along with univariate and multivariate analysis to identify prognostic factors.
Results
We reviewed 141 patients diagnosed with PTLD over last 22 years with median follow-up of 2.4 years. The estimated median overall survival of the entire group was 15.0 years. Sub group analysis showed that 5-year overall survival rates of pediatric population were 88% (median not reached). For adults, median OS was 5.35 years while for elderly patients it was 1.32 years. The estimated median OS of patients with monomorphic PTLD was 9.0 years while in polymorphic PTLD was 19.3 years. Univariate analysis identified gender, age at transplant and PTLD diagnosis, performance status, IPI score, allograft type, recipient EBV status, multiple acute rejections prior to PTLD diagnosis, PTLD sub-type, extra-nodal site involvement, immunosuppressive drug regimen at diagnosis, initial treatment best response were statistically significant prognostic factors (p < 0.05). On multivariate analysis, age at PTLD diagnosis, recipient EBV status, bone marrow involvement, and initial best response were statistically significant prognostic factors (p < 0.05). Surprisingly, use of Rituximab alone as upfront therapy had poor hazard ratio in the cumulative group as well less aggressive PTLD subgroup comprising of early lesions and polymorphic PTLD.
Conclusions
Our experience with treatment and analysis of outcomes does challenge current role of Rituximab use in treatment of PTLD. Currently as we define role of immunotherapy in cancer treatment, the role of acute rejections and immunosuppressant in PTLD becomes more relevant as noticed in our study. This study was also able to find new prognostic factors and also verified other known prognostic factors.
Similar content being viewed by others


Background
Post-transplant lymphoproliferative disorder (PTLD) is a well-recognized complication of Hematopoietic Stem Cell Transplant (HSCT) and Solid Organ Transplant (SOT). It was first described in renal transplant recipients in 1968 by Doak et al. [1] and the term PTLD was first introduced in 1984 by Starzl et al. [2]. PTLD was classified as a separate entity for the first time in 2008 World Health Organization (WHO) classification of lymphoma [3].
The reported incidence of PTLD varies in different transplant centers likely secondary to different immunosuppressive regimens, allograft types and patient population characteristics. PTLD following SOT occurs in up to 20% with the highest incidence in intestinal and multi-organ transplants (5–20%), followed by lung and heart transplants (2–10%) and then by renal and liver transplants (1–5%) [4]. Higher incidence of PTLD in heart, lung, intestinal and multi-organ transplants has been attributed to greater immunosuppression necessary to protect allografts in these patients [5,6,7]. In the pediatric population with SOT, PTLD incidence varies from 2.2% in the kidney to 15% in lung transplant recipients [8]. In contrast, PTLD incidence is about 4% after hematopoietic stem cell transplant (HSCT) [9]. Historically, mortality rates in SOT-related PTLD were 50–70% and up to 70–90% in HSCT, although recent data suggests that outcomes have been improving and comparable to SOT [10, 11].
In the updated 2016 WHO lymphoma classification, PTLD has been subclassified as Plasmacytic hyperplasia PTLD, Infectious mononucleosis PTLD, Florid follicular hyperplasia PTLD, Polymorphic PTLD, Monomorphic PTLD (B- and T-/NK-cell types) and Classical Hodgkin lymphoma PTLD [12]. Diffuse large B-cell lymphoma (DLBCL) accounts for the majority of the cases of PTLD. Most PTLD cases are of B-cell origin while 5–10% can be T/NK cell or Hodgkin lymphoma type. About 70% of cases of PTLD is associated with Epstein-Barr virus (EBV), especially in cases which occur early after transplantation. Pathogenesis of the disease is linked to EBV proliferation in the setting of chronic immunosuppression leading to an inhibition of T cells immune function. However, in 30% of EBV-negative PTLD patients, pathogenesis is not clearly understood.
The primary goal of PTLD treatment is cure while retaining allograft function. Historically, reduction in immunosuppression (RIS) has been the primary mode of treatment. Current guidelines recommend RIS at lowest tolerated levels based on PTLD type, stage, critical illness and allograft risk and then monitoring closely for response and escalation of therapy in the case that RIS alone is not sufficient [13]. Efficacy of this modality depends on PTLD sub-types, disease extent and other prognostic markers [14]. Furthermore, the durability of response by RIS alone is maintained only in about 10% of the patients [2, 15].
Choquet et al. conducted the first prospective (Phase II) trial of single-agent rituximab in SOT-related PTLD after the failure of RI [16]. At 1 year, the Overall Response Rate (ORR) was 34%, and Overall Survival (OS) rate was 67%. When applicable, single agent rituximab is now considered as the first option in low-risk or patients failing RIS. The initial response to rituximab alone as induction therapy is also noted to be a prognostic factor for PTLD [17]. Due to the toxicity of chemotherapy, it is usually reserved for patients with high-risk, aggressive disease or who failed modalities above including RIS and/or single agent rituximab [17, 18]. In adults, anthracycline-based chemotherapy regimens have shown good success for PTLD, and R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone) is currently the preferred regimen for B-cell PTLD with ORR up to 90% [19, 20]. In the pediatric population, the chemotherapy regimen RCP (rituximab, cyclophosphamide, and prednisone) has shown a good response and is preferred regimen [21, 22].
Due to the rarity of this disease, different transplant centers have reported incidence and outcomes and have identified several factors affecting prognosis. As University of Florida (UF) is one of the largest transplant centers in the southeastern United States, we here report our experience with PTLD which we expect will help in better understanding of this rare entity.
Methods
Study population and data collection
The study population was identified mainly from the patient database at UF Health using ICD 9/10 codes and also from United Network for Organ Sharing (UNOS). The studied patient population comprised of all patients including both pediatric and adults, with pathologically confirmed PTLD after SOT or HSCT.
The primary source of data collection was individual chart review by the study team, and no patient was contacted directly or indirectly for data collection. Data were collected in a Health Insurance Portability and Accountability Act (HIPAA) compliant data tool, Research Electronic Data Capture (REDCap) provided by UF. Data was collected for demographics, transplant and immunosuppression history, EBV and CMV serostatus, diagnosis, treatment and outcomes of PTLD.
Data interpretation and statistical analysis
Data were analyzed using SAS software 9.4 (SAS Institute, Cary, NC.) with the help of the UF department of biostatistics. Our primary outcome was overall survival (OS). A secondary analysis was then performed to identify factors affecting OS. The hazard ratio (HR) was calculated, and univariate and multivariate analysis was done. Disease outcome was measured as complete remission (CR), partial remission (PR), stable disease (SD) and progressive disease (PD). Disease control rate (DCR) and overall response rates (ORR) were also calculated. DCR was defined as the sum of CR, PR, and SD while ORR was defined as the sum of CR and PR.
Results
A total of 151 patients were identified as per study inclusion criteria. Patients with very limited records were excluded (n = 10), and so 141 patients were included for final analysis. These patients were diagnosed with PTLD over a period of 22.2 years ranging from September 1994 to December 2016. These patients were transplanted as early as November 1988 to as late as May 2016. Data were collected up to Jan 31, 2017, of all eligible patients. Median follow up time from PTLD diagnosis was 2.4 years.
Estimated overall survival, univariate and multivariate analysis
The estimated median OS of the entire group was 15.0 years (CI 5.83–19.33), see Fig. 1. For pediatric population median was not reached but 5 year survival rates were 88%, in adults estimated median OS was 5.35 years (CI 1.33–18.15) while for elderly patients estimated median OS was 1.32 years (CI 0.34–2.84). The estimated median OS in patients who achieved CR was 19.3 (CI 18.15–19.33) years while the estimated median OS in patients who achieved PR was 5.4 years (CI 0.17–5.35). The estimated median OS of patients with monomorphic PTLD was 9.0 years (CI 2.52–NR) while in polymorphic PTLD was 19.3 years (CI 1.32–19.32).

KM estimate of overall survival of cumulative group
On univariate analysis for OS, we found that patient gender, age at transplant and PTLD diagnosis, performance status, IPI score, allograft type, recipient EBV status, multiple acute rejections prior to PTLD diagnosis, PTLD sub-type, extra-nodal site, immunosuppressive drug regimen at diagnosis, initial treatment best response were statistically significant prognostic factors (p < 0.05). On multivariate analysis age at diagnosis, recipient EBV status, bone marrow involvement, and initial best response were statistically significant prognostic factors (p < 0.05). Figures 2 and 3 shows KM analysis of other significant prognostic markers.

KM estimate based on significant factors

KM estimate based on significant factors
Demographics
Demographic profile of these 141 patients showed that 62.4% were males (n = 88) and 37.6% were females (n = 53). Racial distribution showed that 71.6% were Whites (n = 101) followed by 17.7% of Blacks or African Americans (n = 25) and rest others. 12.8% (n = 18) had a past medical history of malignancy before transplant. The median age at the time of PTLD diagnosis was 41.6 years (Range 1.8–79.4 years). Of these, the pediatric (< 18 years) population consisted of 38.3% (n = 54) while 61.7% (n = 87) were adults. Of the 141 patients, 16.3% patients (n = 23) were aged 65 years or above.
Prognostic impact
Our study revealed female gender as a better prognostic marker with HR of 0.553 (p: 0.0427, CI 0.311–0.981) while race and ethnicity were not statistically significant. A past medical history of malignancy showed a trend towards poorer prognostic marker but was not statistically significant.
Age at PTLD diagnosis was also statistically significant with pediatric patients having HR of 0.241 (p < 0.0001, CI 0.123–0.473) and elderly patients with HR of 3.543 (p < 0.0001, CI 1.894–6.628).
Transplant history
Median age at transplant was 33.3 years (range 1 month to 68 years). Median time from transplant to PTLD diagnosis was 4.1 years (range 1 month to 18.4 years). Type of organ transplant distribution is as detailed in Table 1. Of 17 lung transplant patients 64.7% (n = 11) had single lung transplant while rest 35.3% (n = 6) patients had a double lung transplant.
Prognostic impact
Age at the time of transplant showed pediatric population has a better prognosis with HR: 0.207 (p < 0.0001 CI 0.105–0.407). Among adults, patients between 18–64 years had HR of 3.316 (p < 0.0001, CI 1.836–5.990) while elderly patients above 65 years of age had HR of 2.573 (p 2.573, CI 1.012–6.545).
Allograft type was also a statistically significant prognostic marker with lung transplant recipients having HR of 4.380 (p < 0.0001, CI 2.327–8.245) and liver transplant recipients had HR of 0.357 (p: 0.0023, CI 0.184–0.693) as compared to the rest of group. BMT patients also did poorly with HR of 2.197 (p: 0.0746, CI 0.925–5.219).
EBV and CMV status
At the time of transplant, out of 141 transplant recipients, 58.2% (n = 82) were EBV seropositive while by the time of PTLD diagnosis 72.3% (n = 102) patients were seropositive for EBV. EBV serostatus of donors was mostly unavailable in records. Pathologic evaluation of tumor specimen for EBV showed, 56.0% (n = 79) were positive for EBV, 34.0% (n = 48) were negative and in 9.9% (n = 14) this information was not available. Epstein-Barr encoding region (EBER) in situ hybridization technique was used to identify EBV in the tissue specimen.
At time of transplant, CMV serostatus of recipients was positive for 39.7% (n = 56), negative for 52.5% (n = 74) and unknown for 7.8% (n = 11). CMV serostatus of donor was positive in 48.2% (n = 68), negative in 29.8% (n = 42) and was unknown for 22.0% (n = 31) patients.
Prognostic impact
The only significant poor prognostic factor was positive recipient EBV status with HR of 2.666 (p: 0.0127, CI 1.233–5.765). CMV status of either recipient or donor and the tumor EBER status were not significant.
Immunosuppression and rejection episodes
Induction immunosuppression for transplant were used in 30.5% (n = 43) patients. Prior to diagnosis of PTLD, 44.0% (n = 62) had history of acute allograft rejection and 16.3% (n = 23) had more than 1 episode of rejection. Chronic allograft rejection was noted in 9.2% (n = 13) patients. At the time of PTLD diagnosis, tacrolimus was the most common immunosuppressant used either alone or in combination (63.1%, n = 89).
Prognostic impact: Patient with history of single or multiple episodes of acute rejections were noted to have HR of 1.58 (p: 0.0961, CI 0.922–2.708) while patients with multiple episodes of acute rejections had statistically significant HR of 2.2 (p = 0.0073, CI 1.244–4.046). Chronic rejection had a trend of poor prognosis but was not statistically significant. Induction immunosuppression was not found to be significantly associated with OS.
Use of tacrolimus at the time of diagnosis either alone or in combination with other immunosuppression for maintenance immunosuppression had a good prognostic impact with HR of 0.476 (p: 0.0068, CI 0.278–0.815). Similarly, use of azathioprine showed good prognostic impact with a p-value of 0.0558, almost statistically significant (HR 1.719, CI 0.987–2.994).
Presenting characteristics
Median time from transplant to the diagnosis of PTLD was 4.1 years (range: 32 days–18.4 years). Early PTLD, defined as diagnosed within 1 year was noted in 24.8% (n = 35) patients while late-onset PTLD, which is defined as occurring after 1 year, was noted in 75.2% (n = 106) patients.
B-symptoms were present in 48.2% patients (n = 68) and fever was the most common B symptom noted in 39.0% (n = 55) patients. 90.8% (n = 128) had Eastern Cooperative Oncology Group (ECOG) performance status of equal or less than two.
CD20 status was positive in 73.8% (n = 104). Extra-nodal site was involved in 69.5% (n = 98) and most common extra nodal site GI tract (27.0%, n = 38). More than one extra-nodal site was involved in 22.7% (n = 32) and bulky disease (> 10 cm) was noted in 14.2% (n = 20) patients.
Prognostic impact: Early or late PTLD onset did not impact OS. The presence of B-symptoms was also not significant as well. Good performance status of ECOG 0–2 was a good prognostic factor with HR of 0.183 (p < 0.0001, CI 0.091–0.368). Bone marrow involvement had a poor prognosis with HR of 2.184 (p: 0.0423, CI 1.027–4.643). No other extra nodal site including CNS or allograft was found to have statistically significant hazard ratio. Other factors including serum LDH and albumin, CD20 status and bulky disease were also not significant.
IPI score
IPI score was calculated in all 141 patients, but few patients did not have all required information to calculate IPI. Since missing information could have impacted actual IPI score, we excluded 16 patients where 1 or more item was missing from calculating the exact score. Of the remaining 125 patients, median IP score was 2 (Range 0–5).
Prognostic impact: Higher IPI score of 3–5 was found to have statistically significant HR of 1.843 (p: 0.0422, CI 1.022–3.324).
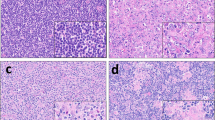
Pathology
Table 2 shows the detailed pathologic distribution of study population along with HR of each sub-groups. DLBCL was noted to be the most common sub-type (42.6%, n = 60).
Prognostic impact: Monomorphic PTLD had HR of 2.309 (p: 0.0177, CI 1.156–4.609). T cell PTLD or DLBCL did not have statistically significant impact on OS.
Treatment
Out of 141 patients, 4.3% (n = 6) patients did not receive any treatment as either patient declined treatment or were not considered to be candidates for therapy. Immunosuppression was reduced (RIS) in 77.3% (n = 109) patients, as the only measure or in combination with other treatment modalities. The upfront treatment approach is outlined in Table 3.
After initial or upfront therapy, 32.6% (n = 46) patients needed 2nd line therapy, and another 9.2% (n = 13) needed third line therapy. Subsequent therapy was needed for patients who either progressed or relapsed after first line therapy and rarely for intolerance. At the end of the study, 60.3% (n = 85) eventually needed chemotherapy with or without rituximab as part of either first line, second line, or third line therapy. CHOP (± R) was the most common regimen used and was used in 28.4% (n = 40) of overall patients. Figure 4 shows patients in different groups needing second-line therapy as compared to the cumulative. 48.5% of patients treated with RIS alone as the first option needed further therapy. Similarly of all patients with monomorphic PTLD and treated with RIS alone, 37.1% of them needed further therapy. Table 4 shows distribution of different chemotherapeutic regimens as first, second and third line therapy. Figure 5 shows patient distribution needing 2nd line treatment based on pathology type and initial treatment choice.

Comparison of patients needing further lines of therapy

Flow chart showing need of 2nd line treatment based on pathology type and initial treatment choice
Prognostic impact: Surprisingly, patients treated with Rituximab alone as front line therapy with or without RIS did poorly with HR of 1.930 (p: 0.0309, CI 1.062–3.505). On subgroup analysis, this was again statistically significant in less aggressive PTLD group comprising of early lesions and polymorphic types of PTLD with HR of 3.765 (p: 0.0498, CI 1.001–14.161), but was not significant for monomorphic PTLD group.
Use of rituximab anytime during treatment either alone or with chemotherapy did not have statistically significant impact on OS and similarly use of CHOP any time during treatment was not statistically significant for OS, as compared to the rest of group.
Response
At the end of the study, 62.4% (n = 88) had complete response while 18.4% (n = 26) had progressive disease. ORR was 68.1% (n = 96) while DCR was 74.5% (n = 105). Table 5 shows patient outcomes at the end of the study.
57.4% (n = 81) patients were still alive at the end of study. Of these, 48.9% (n = 69) are alive without PTLD while 8.5% (n = 12) are alive with PTLD. 39.7% (n = 56) patients are deceased and status of 2.8% (n = 4) is unknown. Of deceased patients, 17.7% (n = 25) died due to PTLD or treatment related complications, 14.2% (n = 20) died of unrelated reasons while cause of death in 7.8% (n = 11) in not available.
Prognostic impact
After any kind of first-line therapy, patients who achieved CR had HR of 0.356 (p: 0.0006, CI 0.198–0.641) while patients who had PD had HR of 6.130 (p < 0.0001, CI 3.354–11.204).
Outcome based on PTLD subtypes
Figure 6 shows distribution of final outcomes of different PTLD types as compared to cumulative group.

Shows final outcome of different PTLD types as compared to cumulative
Graft outcome
After PTLD diagnosis, grafts survived in 82.3% (n = 116) and failed in 11.3% (n = 16) patients. During PTLD treatment 18.4% (n = 26) experienced treatment related graft rejection which led to graft failure in 4.3% (n = 6) patients while graft in 14.2% (n = 20) patient was able to be salvaged.
Prognostic impact
Rejection episodes during PTLD treatment did not impact OS.
Discussion
This retrospective study from a regional transplant center of South-East USA has a good sample size which is among one of the largest reported studies so far throughout the world. Our study identified multiple statistically significant prognostic factors which do impact overall survival and can help in establishing guidelines for further therapy of this rare disease. Table 6 shows comparative results of prognostic factors identified in previous major studies. We compared our results with findings of these studies.
Certain prognostic factors are well known including age, performance status, extra-nodal site involvement, low albumin and IPI score. These findings represent age, extent and nutritional status which is expected to impact survival. In contrast to these known factors, albumin was not significant in our study.
We found that female gender to have statistically significant better prognosis which was also noted by Jain et al. but was not statistically significant in that study [24]. The advanced stage of PTLD was not significant, but in PTLD types monomorphic PTLD did perform poorly which is known to be an aggressive form of PTLD with poor prognosis. T-cell PTLD was found to do poorly in some studies but not in our study [23, 30].
The role of EBV is very well known in the pathogenesis of PTLD, but its impact on survival is still not clear. EBV positivity was reported to be a poor prognostic factor by Oton et al. [27] while non-EBV PTLD was seen as poor prognostic by Leblond et al. [23] and Kinch et al. [30]. Our study did find that EBV recipients tend to do poorly, but EBER positive PTLD had no significant impact on survival. These findings do support the role of EBV in the pathogenesis of PTLD, but its impact on survival needs to be studied further.
As seen in our study, the initial response to treatment has been seen as a prognostic value in studies done by Ghobrial et al. [25] and Maecker et al. [26]. This does show that patients who do not respond with early treatment options should be managed considering that they may have poor survival as compared to the rest of group.
Patients who were on tacrolimus and azathioprine for maintenance immunosuppression at the time of PTLD diagnosis performed better in this study and similar finding for tacrolimus was noted by Jain et al. [24], although interestingly previous studies have also shown increased incidence of PTLD with tacrolimus use [7, 34]. The significance of allograft rejection episodes in PTLD incidence is well known [35, 36] but we also noticed that patients who had acute rejections, especially multiple rejections performed poorly, and similar findings were noted by Kremers et al. [35]. Transplant recipients who experience episodes of rejection often get increased immune-suppression for allograft protection. Our study findings signify the role of chronic immunomodulation over the years for these patients and need to be considered while selecting chronic immune suppressants and during rejection treatments. As noted in our study, patients who experience rejections and later on develop PTLD will tend to do poorly. We do recommend close follow up with immunologists or transplant teams who can navigate these patients through these complexities of immunosuppression management.
Rituximab use was seen statistically significant related with good prognosis by Oton et al. [27] and Evens et al. [29]. but not in other studies [25, 32]. In our study rituximab use was not associated with improved survival as compared to the rest of group. Strikingly in our study, we noticed that isolated use of Rituximab as upfront therapy had poor hazard ratio in the cumulative group as well less aggressive subgroup comprising early lesion and polymorphic PTLD. We could not identify any factor which could explain this finding as patients who received Rituximab alone had comparable performance status and disease status to rest of group. They had a poor initial response which in itself is a poor prognostic finding in our study. These findings support further studies looking into the role of rituximab in PTLD, especially isolated use without other chemotherapeutic agents. Although CHOP (± R) was noted to be the most common regimen used, we did not find any statistically significant results of CHOP use.
Study limitations
This study was done as a retrospective study, and the main aim of this study was to identify new and validate previously known prognostic factors. Authors do acknowledge the inherent limitations of a retrospective study, but we do feel that good sample size of this study acquired over prolonged period does make results reliable. Most of the PTLD treatment guidelines are derived from retrospective studies from different transplant centers, like our study and with contribution from limited prospective trials due to the rarity of this disease [16, 20]. Treatment regimens and dosages used to treat PTLD were as per the current guidelines as per discretion of treating physicians. This study goes back over a prolonged period when EBV PCR was not routinely available or monitored as the standard of care. This value was not available for many patients, especially in the adult population. Also, this study was not focused on epidemiology or incidence of PTLD.
Conclusion
This study, which is one of the largest studies done so far has validated some of the long-established prognostic factors while identifying some new factors and challenging others. We hope this study will further help physicians in making treatment choices based on these prognostic factors.
Abbreviations
- PTLD:
-
post-transplant lymphoproliferative disorder
- IRB:
-
institutional review board
- WHO:
-
World Health Organization
- SOT:
-
solid organ transplant
- HSCT:
-
hematopoietic stem cell transplant
- DLBCL:
-
diffuse large B cell lymphoma
- EBV:
-
Epstein-Barr virus
- RIS:
-
reduced Immunosuppression
- UF:
-
University of Florida
- R-CHOP:
-
rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone
- RCP:
-
rituximab, cyclophosphamide, and prednisone
- OS:
-
overall survival
- CR:
-
complete remission
- PR:
-
partial remission
- SD:
-
stable disease
- PD:
-
progressive disease
- DCR:
-
disease control rate
- ORR:
-
overall response rates
- ECOG:
-
Eastern Cooperative Oncology Group
- CMV:
-
cyto-megalo virus
- HR:
-
hazard ratio
- EBER:
-
epstein-barr encoding region
References
Michonneau D, Suarez F, Lambert J, et al. Late-onset post-transplantation lymphoproliferative disorders after kidney transplantation: a monocentric study over three decades. Nephrol Dial Transplant. 2013;28:471–8.
Starzl TE, Nalesnik MA, Porter KA, et al. Reversibility of lymphomas and lymphoproliferative lesions developing under cyclosporin-steroid therapy. Lancet. 1984;1:583–7.
Campo E, Swerdlow SH, Harris NL, et al. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. Blood. 2011;117:5019–32.
Petrara MR, Giunco S, Serraino D, et al. Post-transplant lymphoproliferative disorders: from epidemiology to pathogenesis-driven treatment. Cancer Lett. 2015;369:37–44.
Opelz G, Henderson R. Incidence of non-Hodgkin lymphoma in kidney and heart transplant recipients. Lancet. 1993;342:1514–6.
Cockfield SM. Identifying the patient at risk for post-transplant lymphoproliferative disorder. Transpl Infect Dis. 2001;3:70–8.
Opelz G, Döhler B. Lymphomas after solid organ transplantation: a collaborative transplant study report. Am J Transplant. 2004;4:222–30.
Wistinghausen B, Gross TG, Bollard C. Post-transplant lymphoproliferative disease in pediatric solid organ transplant recipients. Pediatr Hematol Oncol. 2013;30:520–31.
Uhlin M, Wikell H, Sundin M, et al. Risk factors for epstein-barr virus-related post-transplant lymphoproliferative disease after allogeneic hematopoietic stem cell transplantation. Haematologica. 2014;99:346–52.
Nakanishi C, Kawagishi N, Sekiguchi S, et al. Post-transplantation lymphoproliferative disorder in living-donor liver transplantation: a single-center experience. Surg Today. 2012;42:741–51.
Styczynski J, Gil L, Tridello G, et al. Response to rituximab-based therapy and risk factor analysis in epstein barr virus-related lymphoproliferative disorder after hematopoietic stem cell transplant in children and adults: a study from the infectious diseases working party of the European Group for blood and marrow transplantation. Clin Infect Dis. 2013;57:794–802.
Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375–90.
Parker A, Bowles K, Bradley JA, et al. Management of post-transplant lymphoproliferative disorder in adult solid organ transplant recipients—BCSH and BTS guidelines. Br J Haematol. 2010;149:693–705.
Tsai DE, Hardy CL, Tomaszewski JE, et al. Reduction in immunosuppression as initial therapy for posttransplant lymphoproliferative disorder: analysis of prognostic variables and long-term follow-up of 42 adult patients. Transplantation. 2001;71:1076–88.
Ghobrial IM, Habermann TM, Ristow KM, et al. Prognostic factors in patients with post-transplant lymphoproliferative disorders (PTLD) in the rituximab era. Leuk Lymphoma. 2005;46:191–6.
Choquet S, Leblond V, Herbrecht R, et al. Efficacy and safety of rituximab in B-cell post-transplantation lymphoproliferative disorders: results of a prospective multicenter phase 2 study. Blood. 2006;107(8):3053–7.
Trappe RU, Dierickx D, Zimmermann H, et al. Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful stratification into rituximab or R-chop consolidation in an international, prospective, multicenter phase II trial. J Clin Oncol 2016;JCO2016693564.
Dharnidharka VR, Webster AC, Martinez OM, et al. Post-transplant lymphoproliferative disorders. Nat Rev Dis Primers. 2016;2:15088.
Choquet S, Trappe R, Leblond V, et al. CHOP-21 for the treatment of post-transplant lymphoproliferative disorders (PTLD) following solid organ transplantation. Haematologica. 2007;92:273–4.
Trappe R, Oertel S, Leblond V, et al. Sequential treatment with rituximab followed by CHOP chemotherapy in adult B-cell post-transplant lymphoproliferative disorder (PTLD): the prospective international multicentre phase 2 PTLD-1 trial. Lancet Oncol. 2012;13:196–206.
Mynarek M, Schober T, Behrends U, et al. Posttransplant lymphoproliferative disease after pediatric solid organ transplantation. J Immunol Res. 2013;2013:814973.
Gross TG, Orjuela MA, Perkins SL, et al. Low-dose chemotherapy and rituximab for post-transplant lymphoproliferative disease (PTLD): a Children’s Oncology Group report. Am J Transplant. 2012;12:3069–75.
Leblond V, Dhedin N, Mamzer Bruneel MF, et al. Identification of prognostic factors in 61 patients with posttransplantation lymphoproliferative disorders. J Clin Oncol. 2001;19:772–8.
Jain A, Nalesnik M, Reyes J, et al. Posttransplant lymphoproliferative disorders in liver transplantation: a 20-year experience. Ann Surg. 2002;236:429–36 (discussion 436–7).
Ghobrial IM, Habermann TM, Maurer MJ, et al. Prognostic analysis for survival in adult solid organ transplant recipients with post-transplantation lymphoproliferative disorders. J Clin Oncol. 2005;23:7574–82.
Maecker B, Jack T, Zimmermann M, et al. CNS or bone marrow involvement as risk factors for poor survival in post-transplantation lymphoproliferative disorders in children after solid organ transplantation. J Clin Oncol. 2007;25:4902–8.
Oton AB, Wang H, Leleu X, et al. Clinical and pathological prognostic markers for survival in adult patients with post-transplant lymphoproliferative disorders in solid transplant. Leuk Lymphoma. 2008;49:1738–44.
Knight JS, Tsodikov A, Cibrik DM, et al. Lymphoma after solid organ transplantation: risk, response to therapy, and survival at a transplantation center. J Clin Oncol. 2009;27:3354–62.
Evens AM, David KA, Helenowski I, et al. Multicenter analysis of 80 solid organ transplantation recipients with post-transplantation lymphoproliferative disease: outcomes and prognostic factors in the modern era. J Clin Oncol. 2010;28:1038–46.
Kinch A, Baecklund E, Backlin C, et al. A population-based study of 135 lymphomas after solid organ transplantation: the role of epstein-barr virus, hepatitis C and diffuse large B-cell lymphoma subtype in clinical presentation and survival. Acta Oncol. 2014;53:669–79.
Dierickx D, Tousseyn T, Sagaert X, et al. Single-center analysis of biopsy-confirmed posttransplant lymphoproliferative disorder: incidence, clinicopathological characteristics and prognostic factors. Leuk Lymphoma. 2013;54:2433–40.
Montanari F, Radeski D, Seshan V, et al. Recursive partitioning analysis of prognostic factors in post-transplant lymphoproliferative disorders (PTLD): a 120 case single institution series. Br J Haematol. 2015;171:491–500.
Luskin MR, Heil DS, Tan KS, et al. The impact of EBV status on characteristics and outcomes of posttransplantation lymphoproliferative disorder. Am J Transplant. 2015;15:2665–73.
Caillard S, Dharnidharka V, Agodoa L, et al. Posttransplant lymphoproliferative disorders after renal transplantation in the United States in era of modern immunosuppression. Transplantation. 2005;80:1233–43.
Kremers WK, Devarbhavi HC, Wiesner RH, et al. Post-transplant lymphoproliferative disorders following liver transplantation: incidence, risk factors and survival. Am J Transplant. 2006;6:1017–24.
Gao SZ, Chaparro SV, Perlroth M, et al. Post-transplantation lymphoproliferative disease in heart and heart-lung transplant recipients: 30-year experience at Stanford University. J Heart Lung Transplant. 2003;22:505–14.
Authors’ contributions
ND, WBS and RB designed study and ND is principal investigator and mentor author. RB, RBj, AF, WPS and NP were involved in data collection. YW and FZ provided statistical data. RB was a major contributor in writing manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets during and/or analyzed during the current study available from the corresponding author on reasonable request.
Consent to publication
Not applicable. Manuscript does not contain any individual person’s data.
Ethics approval and consent to participate
This study was approved by Institution Review Board (IRB) at University of Florida, Gainesville FL and all standard ethical guidelines were followed. Full waiver of informed consent was obtained (IRB201300065).
Funding
No grant or other monetary sources were used to conduct this study. Data was collected using Redcaps provided by the UF CTSI, which is funded in part by the National Institutes of Health Clinical and Translational Science Award program, Grants UL1TR001427, KL2TR001429, and TL1TR001428.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Bishnoi, R., Bajwa, R., Franke, A.J. et al. Post-transplant lymphoproliferative disorder (PTLD): single institutional experience of 141 patients. Exp Hematol Oncol 6, 26 (2017). https://doi.org/10.1186/s40164-017-0087-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40164-017-0087-0