
Abstract
Background
Many studies have reported specific adaptations to high altitude, but few studies have focused on physiological variations in high-altitude adaptation in Andean highlanders. This study aimed to investigate the relationships between SpO2 and related factors, including individual variations and sex differences, in Andean highlanders.
Methods
The participants were community-dwelling people in La Paz, Bolivia, aged 20 years and over (age range 20–34 years). A total of 50 men and 50 women participated in this study. Height, weight, SpO2, hemoglobin concentration, finger temperature, heart rate, and blood pressure were measured. Information about lifestyle was also obtained by interview.
Results
There were individual variations of SpO2 both in men (mean 89.9%, range 84.0–95.0%) and women (mean 91.0%, range 84.0–96.0%). On Student’s t test, men had significantly lower heart rate (p = 0.046) and SpO2 (p = 0.030) than women. On the other hand, men had significantly higher SBP (p < 0.001), hemoglobin (p < 0.001), and finger temperature (p = 0.004). In men, multiple stepwise regression analysis showed that a higher SpO2 was correlated with a lower heart rate (β = − 0.089, p = 0.007) and a higher finger temperature (β = 0.308, p = 0.030) (r2 for model = 0.18). In women, a higher SpO2 was significantly correlated with a higher finger temperature (β = 0.391, p = 0.015) (r2 for model = 0.12). A higher SpO2 was related to a higher finger temperature (β = 0.286, p = 0.014) and a lower heart rate (β = − 0.052, p = 0.029) in all participants (r2 for model = 0.21). Residual analysis showed that individual SpO2 values were randomly plotted.
Conclusion
Random plots of SpO2 on residual analysis indicated that these variations were random error, such as biological variation. A higher SpO2 was related to a lower heart rate and finger temperature in men, but a higher SpO2 was related to finger temperature in women. These results suggest that there are individual variations and sex differences in the hemodynamic responses of high-altitude adaptation in Andean highlanders.
Similar content being viewed by others

Background
Studies of adaptation to high altitude started over 100 years ago, and they focused on increased hemoglobin (Hb) concentrations in Andean highlanders or sojourners in high-mountain areas [1, 2]. This Hb increase is the typical physiological response of humans at high altitude [2,3,4]. Hb carries less oxygen with increasing altitude because the partial pressure of oxygen in the lung is decreased, and there is decreased oxygen available for diffusion into the blood [5]. This percentage of arterial Hb with oxygen is evaluated by measuring percutaneous arterial oxygen saturation (SpO2), and SpO2 indicates the oxygen level in the body. A lower SpO2 occurs in acute mountain sickness, which can include various severe symptoms [6, 7]. Therefore, to maintain oxygen levels, people who stay at high altitude and Andean highlanders have increased Hb concentrations or SpO2.
Although early studies focused on the Andean type of physiological adaptation, such as high Hb and slightly lower SpO2 [5, 8, 9], recent studies reported population differences in high-altitude adaptation and suggested that there are different physiological responses to hypobaric hypoxia despite similar levels of hypoxic stress. Interestingly, Tibetan highlanders have lower Hb and SpO2 levels than Andean highlanders [10,11,12].
Previous studies also reported physiological variations and sex differences in highlanders. In Andean highlanders, Beall et al. [5] reported that SpO2 was higher in men than in women. Furthermore, higher SpO2 was associated with higher Hb concentrations in Ethiopian women [13]. In Tibetans of Nepal, lower SpO2 was associated with lower glycosylated hemoglobin (HbA1c) [14]. In other studies, SpO2 was an important index for acute mountain sickness (AMS) in Andean highlanders [8], and there were individual variations of SpO2 in lowlanders exposed to hypobaric hypoxia [15]. These results suggest that there are individual variations and sex differences in high-altitude adaptation, and SpO2 is an important physiological index for evaluating adaptability to high altitude.
Although some studies have reported the Tibetan type of high-altitude adaptation in recent years [1, 4, 14, 16], studies of the Andean type are limited; in particular, few studies have focused on physiological variations from the perspective of physiological anthropology [5, 8]. Therefore, this study aimed to investigate the relationships between SpO2 and related factors, including individual variations and sex differences, in Andean highlanders.
Methods
The participants were community-dwelling people aged 20 years and over (20–34 years old) in La Paz, Bolivia (altitude 3700–4000 m), who were invited to participate in this study in 2016. All participants were born and raised around La Paz. A total of 50 men and 50 women (university students) participated in this study. All participants gave their written, informed consent before the examination. This study was approved by the Ethics Committee of Nagasaki University Graduate School of Biomedical Sciences (No. 16072995).
After an explanation of the experiment and obtaining written, informed consent (30 min), each participant’s height, weight, SpO2, hemoglobin concentration, finger temperature, heart rate, and blood pressure were measured. All parameters were measured at a room temperature of 23 to 25 °C, participants stayed in the room for up to 2 h, and they wore normal clothes (not controlled).
SpO2 was measured by a finger pulse oximeter (Masimo Radical V 5.0, Masimo Corp., Irvine, CA, USA). Hb concentration and finger temperature on the inner surface of the index finger were measured by an ASTRIM FIT health monitoring analyzer (Sysmex, Kobe, Japan). After measuring SpO2, Hb, and finger temperature at the right hand, systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate were measured in the left arm in the resting condition by a digital automatic blood pressure monitor (OMRON Model, HEM-7210, Kyoto, Japan). These physiological measurements were measured within 1 h of entering the room. Height (m) and weight (kg) were measured with light clothing and without shoes, and the body mass index (BMI) was calculated as weight/height squared (kg/m2). Keeping vertical at each point, height was measured to the nearest 0.1 cm from the top of the head to the heel using a tape measure (0 to 200 cm) attached to the wall. Information about physical activity (walking or doing any equivalent amount of exercise activity more than 30 min a day (yes/no)), current smoking (having one or more cigarettes per day (yes/no)), and alcohol drinking (some alcohol consumption one or more days per week (yes/no)) was obtained by interview. However, physical activity, smoking, and alcohol drinking were not controlled before the measurements.
Statistical analysis
Variables are presented as means with SD. Student’s t test and Fisher’s exact test were used for comparisons between men and women. Pearson’s correlation analysis was used to assess correlations between SpO2 and other parameters for all participants, for men, and for women. Multiple stepwise regression analysis was used to assess correlations between SpO2 and related parameters (sex, height, weight, BMI, hemoglobin, heart rate, SBP, DBP, finger temperature, current smoking, alcohol drinking, and physical activity) for all participants, for men, and women. To assess the individual variations of SpO2, residual analysis was performed using a multiple stepwise regression model in both sexes. The estimated values of SpO2 were plotted on the X-axis, and the residuals between the measured and estimated values of SpO2 were plotted on the Y-axis. The 95% confidence interval (CI) of the residuals was calculated as the limits of agreement.
A p value of less than 0.05 was considered significant. The data were analyzed using the Statistical Analysis System software package version 9.4 (SAS Institute, Cary, NC, USA).
Results
There were individual variations of SpO2 in both men (mean 89.9%, range 84.0–95.0%) and women (mean 91.0%, range 84.0–96.0%). Table 1 summarizes the characteristics of the 100 participants. Men had significantly higher height and weight than women, but there was no significant difference in BMI. On physiological measurements, men had significantly lower heart rate and SpO2 than women. On the other hand, men had significantly higher SBP, hemoglobin, and finger temperature. In other factors, men had significantly higher rates of alcohol drinking and physical activity.
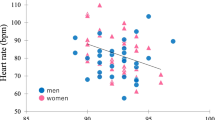
In men, SpO2 was negatively correlated with heart rate and DBP (Fig. 1, Table 2). In women, SpO2 was positively correlated with finger temperature and showed a trend to having a negative correlation with DBP (Table 2).

Scatter plot of SpO2 and heart rate in Andean highlanders. SpO2 is negatively correlated with heart rate (r = − 0.307, p = 0.030) in men. The solid line indicates the trend for men
In men, multiple stepwise regression analysis showed that a higher SpO2 was significantly correlated with a lower heart rate and a higher finger temperature (Table 3). On the other hand, in women, a higher SpO2 was significantly correlated with a higher finger temperature (Table 3). A higher SpO2 was related to a higher finger temperature and a lower heart rate in all participants (Table 3).
Residual analysis showed that individual values were randomly plotted in both sexes (Figs. 3 and 4). There were no significant correlations between the estimated value and the residual in men (r = − 0.001, p = 0.994) and in women (r = − 0.00004, p = 0.999). The 95% limits of agreement was − 4.26 to 4.35 in men and − 4.91 to 4.89 in women.
Discussion
Many previous studies indicated the specific type of high-altitude adaptation of various populations, such as Tibetans, Andeans, and Ethiopians [1, 5, 8,9,10,11,12,13, 17,18,19]. On the other hand, studies focusing on variations or sex differences in Andean highlanders have been limited [5, 8]. In the present study, the data for the hemodynamic parameters, focusing primarily on SpO2 of young Andean highlanders, are presented.
In the present study, men had significantly lower SpO2 than women (Table 1). Although this difference was small and its clinical relevance was unclear, men had higher hemoglobin, which might be enough to deliver the oxygen with lower SpO2 compared to women. However, Beall et al. [5] reported that men had higher SpO2 than women in Andean people (La Paz, Bolivia). The reason for this inconsistency was not clear, but it might depend on the difference in participants’ smoking habits. Their participants smoked more (62.3% in men and 39.7% in women) [8], and SpO2 was overestimated in smokers [20,21,22]. It is thought that these factors may be related to the inconsistency between the present data and Beall’s data. However, further studies are needed to compare the SpO2 between smokers and non-smokers in highlanders.
Hemoglobin and SBP were significantly higher and heart rate was lower in men than women (Table 1). Typically, men have higher hemoglobin and blood pressure and a lower heart rate than women in a sea level environment [23,24,25], and the present result for hemoglobin is consistent with the previous study of Andean highlanders [8]. These results suggest that the sex differences of hemoglobin, heart rate, and SBP are common in both lowlanders and highlanders.
Men had significantly higher finger temperature than women (Table 1), consistent with previous studies that reported that men had a higher skin temperature and peripheral blood flow in a thermoneutral environment among lowlanders [26, 27].
There was a significant negative correlation between SpO2 and heart rate in men, but not in women (Fig. 1, Table 2). In men, multiple regression analysis showed that a lower SpO2 was correlated with a higher heart rate after adjusting covariates (Table 3). Although it has been reported that heart rate was decreased after long-term high-altitude exposure [28], the present results indicated that lower SpO2 evoked a higher heart rate for higher oxygen delivery. These physiological states were similar to those of lowlanders. The results might depend on sex differences in the sensitivity of the oxygen receptor or the relatively higher heart rate of women compared to men.
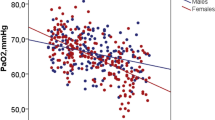
Beall et al. [8] reported a negative correlation between SpO2 and hemoglobin in women and suggested sex differences in hemodynamics in Andean highlanders, whereas SpO2 was not correlated with hemoglobin in both sexes in the present study (Fig. 2, Table 2).

Scatter plot of SpO2 and hemoglobin in Andean highlanders.
In the present study, a lower SpO2 was related to or tended to be associated with higher DBP in both sexes (Table 2). Multiple stepwise regression analysis showed that a lower SpO2 was significantly correlated to a lower finger temperature in both sexes (Table 3). Finger temperature is important in the evaluation of vasoconstriction. The positive relationship between SpO2 and finger temperature probably reflected peripheral circulation levels; an inadequate blood supply to the finger might cause a lower SpO2. In the high-altitude environment, vasodilation occurs due to nitric oxide (NO) release from vascular endothelial cells with lower SpO2 [29]. Thus, it is expected that a lower SpO2 evokes vasodilation and then decreases DBP; previous studies also reported lower blood pressure in highlanders [30]. Therefore, increasing blood flow due to NO release causes increased finger temperature and decreased DBP [30, 31], but this was not consistent with the present study. These responses were also affected by the sex difference in vasoconstrictor responses [32, 33] or sympathetic vasoconstrictor responsiveness via NO mediation [34]. The present results suggest that vasoconstriction (lower finger temperature) was related to a lower SpO2, which also causes a higher DBP.
Residual analysis showed that most individual values were randomly plotted within the 95% limits of agreement, and there were no significant correlations between the residual and the estimated SpO2 in the regression models (Figs. 3 and 4). Thus, these variations seemed to not be a proportional bias, but random error, such as biological variation. The factors affecting this variation of SpO2 were complex. Finger temperature was related to SpO2 (Table 3), but a low temperature resulted from reduced perfusion of the limb due to a vasoconstrictor response; it does not mean low arterial oxygen saturation (SaO2). A higher SpO2 was related to a lower heart rate in all participants (Table 3); therefore, individual variation of SpO2 was partly explained by heart rate. This correlation was not significant in women, but it might depend on the sample size. From the above, it was thought that individuals who could have higher SpO2 values even in highland areas could live with a lower heart rate, and this might suggest that they are well adapted to the high altitude.

Scatter plot of residual and estimated SpO2 values from the regression model in men. The dotted line represents the 95% limits of agreement (− 4.26 to 4.35)

Scatter plot of residual and estimated SpO2 values from the regression model in women. The dotted line represents the 95% limits of agreement (− 4.91 to 4.89)
Finally, in the total regression analysis, 21% of the variation in SpO2 was explained, but the remaining variation was unclear. Recent studies indicated that the physiological status of highlanders was affected by genetic background, including EPAS1 and EGLN1 genes [4, 16, 17, 35,36,37,38]. These remaining individual variations might be explained by genetic characteristics or other underlying factors in further studies.
The present study has several limitations. First, the results do not necessarily show a causal relationship because this study was cross-sectional in design. Second, information on other determinants (e.g., ventilation, nutritional status, or menstrual cycle) contributing to SpO2 was not clear. Third, hemoglobin concentration was an estimated value that was difficult to compare to values reported by other studies. Finally, the participants were university students and may differ from the general population.
Conclusion
In conclusion, the present study showed that SpO2 values of Andean highlanders were not homogeneous. Residual analysis showed that the plots of SpO2 were random. In men, a higher SpO2 was related to a lower heart rate and finger temperature. A higher SpO2 was related to a higher finger temperature in women. These results suggest that there are individual variations and sex differences in the hemodynamics of high-altitude adaptation in Andean highlanders.
Availability of data and materials
Not applicable.
Abbreviations
- 95% CI:
-
95% confidence interval
- AMS:
-
Acute mountain sickness
- BMI:
-
Body mass index
- DBP:
-
Diastolic blood pressure
- EGLN1:
-
Egl-9 family hypoxia-inducible factor 1
- EPAS1:
-
Endothelial PAS domain-containing protein 1
- Hb:
-
Hemoglobin
- HbA1c:
-
Glycosylated hemoglobin
- HIF:
-
Hypoxia-inducible factor
- NO:
-
Nitric oxide
- SaO2 :
-
Arterial oxygen saturation
- SBP:
-
Systolic blood pressure
- SpO2 :
-
Percutaneous arterial oxygen saturation
References
Bigham AW, Wilson MJ, Julian CG, Kiyamu M, Vargas E, Leon-Velarde F, Rivera-Chira M, Rodriquez C, Browne VA, Parra E, Brutsaert TD, Moore LG, Shriver MD. Andean and Tibetan patterns of adaptation to high altitude. Am J Hum Biol. 2013;25:190–7.
Douglas CG, Haldane JS, Henderson Y, Schneider EC, Webb GB, Richards J. Physiological observations made on Pike’s Peak, Colorado, with special reference to adaptation to low barometric pressures. Philos Trans R Soc Lond B Biol Sci. 1913;203:185–318.
Beall CM. Human adaptability studies at high altitude: research designs and major concepts during fifty years of discovery. Am J Hum Biol. 2013;25:141–7.
Bigham AW, Lee FS. Human high-altitude adaptation: forward genetics meets the HIF pathway. Genes Dev. 2014;28:2189–204.
Beall CM, Almasy LA, Blangero J, Williams-Blangero S, Brittenham GM, Strohl KP, Decker MJ, Vargas E, Villena M, Soria R, Alarcon AM, Gonzales C. Percent of oxygen saturation of arterial hemoglobin among Bolivian Aymara at 3,900-4,000 m. Am J Phys Anthropol. 1999;108:41–51.
Basnyat B. Pro: pulse oximetry is useful in predicting acute mountain sickness. High Alt Med Biol. 2014;15:440–1.
Roach RC, Greene ER, Schoene RB, Hackett PH. Arterial oxygen saturation for prediction of acute mountain sickness. Aviat Space Environ Med. 1998;69:1182–5.
Beall CM, Brittenham GM, Strohl KP, Blangero J, Williams-Blangero S, Goldstein MC, Decker MJ, Vargas E, Villena M, Soria R, Alarcon AM, Gonzales C. Hemoglobin concentration of high-altitude Tibetans and Bolivian Aymara. Am J Phys Anthropol. 1998;106:385–400.
Cueto M. Andean biology in Peru. Scientific styles on the periphery. Isis. 1989;80:640–58.
Beall CM, Reichsman AB. Hemoglobin levels in a Himalayan high altitude population. Am J Phys Anthropol. 1984;63:301–6.
Beall CM. Tibetan and Andean contrasts in adaptation to high-altitude hypoxia. Adv Exp Med Biol. 2000;475:63–74.
Beall CM. Andean, Tibetan, and Ethiopian patterns of adaptation to high-altitude hypoxia. Integr Comp Biol. 2006;46:18–24.
Alkorta-Aranburu G, Beall CM, Witonsky DB, Gebremedhin A, Pritchard JK, Di Rienzo A. The genetic architecture of adaptations to high altitude in Ethiopia. PLoS Genet. 2012;8:e1003110.
Koirala S, Nakano M, Arima H, Takeuchi S, Ichikawa T, Nishimura T, Ito H, Pandey BD, Pandey K, Wada T, Yamamoto T. Current health status and its risk factors of the Tsarang villagers living at high altitude in the Mustang district of Nepal. J Physiol Anthropol. 2018;37:20.
Motoi M, Nishimura T, Egashira Y, Kishida F, Watanuki S. Relationship between mitochondrial haplogroup and physiological responses to hypobaric hypoxia. J Physiol Anthropol. 2016;35:12.
Beall CM, Cavalleri GL, Deng L, Elston RC, Gao Y, Knight J, Li C, Li JC, Liang Y, McCormack M, Montgomery HE, Pan H, Robbins PA, Shianna KV, Tam SC, Tsering N, Veeramah KR, Wang W, Wangdui P, Weale ME, Xu Y, Xu Z, Yang L, Zaman MJ, Zeng C, Zhang L, Zhang X, Zhaxi P, Zheng YT. Natural selection on EPAS1 (HIF2alpha) associated with low hemoglobin concentration in Tibetan highlanders. Proc Natl Acad Sci U S A. 2010;107:11459–64.
Beall CM. Adaptation to high altitude: phenotypes and genotypes. Annu Rev Anthropol. 2014;43:251–72.
Beall CM, Decker MJ, Brittenham GM, Kushner I, Gebremedhin A, Strohl KP. An Ethiopian pattern of human adaptation to high-altitude hypoxia. Proc Natl Acad Sci U S A. 2002;99:17215–8.
Beall CM, Brittenham GM, Macuaga F, Barragan M. Variation in hemoglobin concentration among samples of high-altitude natives in the Andes and the Himalayas. Am J Hum Biol. 1990;2:639–51.
Buckley RG, Aks SE, Eshom JL, Rydman R, Schaider J, Shayne P. The pulse oximetry gap in carbon monoxide intoxication. Ann Emerg Med. 1994;24:252–5.
Glass KL, Dillard TA, Phillips YY, Torrington KG, Thompson JC. Pulse oximetry correction for smoking exposure. Mil Med. 1996;161:273–6.
Seppanen A. Smoking in closed space and its effect on carboxyhaemoglobin saturation of smoking and nonsmoking subjects. Ann Clin Res. 1977;9:281–3.
Joyner MJ, Wallin BG, Charkoudian N. Sex differences and blood pressure regulation in humans. Exp Physiol. 2016;101:349–55.
Reckelhoff JF. Sex differences in regulation of blood pressure. Adv Exp Med Biol. 2018;1065:139–51.
Smetana P, Batchvarov V, Hnatkova K, John Camm A, Malik M. Sex differences in the rate dependence of the T wave descending limb. Cardiovasc Res. 2003;58:549–54.
Daanen HA. Finger cold-induced vasodilation: a review. Eur J Appl Physiol. 2003;89:411–26.
Cooke JP, Creager MA, Osmundson PJ, Shepherd JT. Sex differences in control of cutaneous blood flow. Circulation. 1990;82:1607–15.
Mazzeo RS, Bender PR, Brooks GA, Butterfield GE, Groves BM, Sutton JR, Wolfel EE, Reeves JT. Arterial catecholamine responses during exercise with acute and chronic high-altitude exposure. Am J Physiol. 1991;261:E419–24.
Crawford JH, Isbell TS, Huang Z, Shiva S, Chacko BK, Schechter AN, Darley-Usmar VM, Kerby JD, Lang JD Jr, Kraus D, Ho C, Gladwin MT, Patel RP. Hypoxia, red blood cells, and nitrite regulate NO-dependent hypoxic vasodilation. Blood. 2006;107:566–74.
Hanna JM. Climate, altitude, and blood pressure. Hum Biol. 1999;71:553–82.
Sinex JE. Pulse oximetry: principles and limitations. Am J Emerg Med. 1999;17:59–67.
Lott ME, Hogeman C, Herr M, Bhagat M, Sinoway LI. Sex differences in limb vasoconstriction responses to increases in transmural pressures. Am J Physiol Heart Circ Physiol. 2009;296:H186–94.
Patel HM, Heffernan MJ, Ross AJ, Muller MD. Sex differences in forearm vasoconstrictor response to voluntary apnea. Am J Physiol Heart Circ Physiol. 2014;306:H309–16.
Just TP, DeLorey DS. Sex differences in sympathetic vasoconstrictor responsiveness and sympatholysis. J Appl Physiol (1985). 2017;123:128–35.
Simonson TS, Yang Y, Huff CD, Yun H, Qin G, Witherspoon DJ, Bai Z, Lorenzo FR, Xing J, Jorde LB, Prchal JT, Ge R. Genetic evidence for high-altitude adaptation in Tibet. Science. 2010;329:72–5.
Yang J, Jin ZB, Chen J, Huang XF, Li XM, Liang YB, Mao JY, Chen X, Zheng Z, Bakshi A, Zheng DD, Zheng MQ, Wray NR, Visscher PM, Lu F, Qu J. Genetic signatures of high-altitude adaptation in Tibetans. Proc Natl Acad Sci U S A. 2017;114:4189–94.
Yang Y, Du H, Li Y, Guan W, Tang F, Ga Q, Ge RL. NR3C1 gene polymorphisms are associated with high-altitude pulmonary edema in Han Chinese. J Physiol Anthropol. 2019;38:4.
Yasukochi Y, Nishimura T, Motoi M, Watanuki S. Association of EGLN1 genetic polymorphisms with SpO2 responses to acute hypobaric hypoxia in a Japanese cohort. J Physiol Anthropol. 2018;37:9.
Acknowledgements
Not applicable.
Funding
This work was supported by Grants-in-Aid for Scientific Research (KAKENHI No. JP18 K14808, JP15 K18623, and JP17H01453) from the Japan Society for the Promotion of Science.
Author information
Authors and Affiliations
Contributions
TN and KA designed and performed the research. TN, JU, MO, MN, GA, YY, KA, SW, VM, and KA contributed to data acquisition and data analysis or interpretation. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Nagasaki University Graduate School of Biomedical Sciences (No. 16072995). All participants provided written consent for their participation after they were fully informed about the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nishimura, T., Ugarte, J., Ohnishi, M. et al. Individual variations and sex differences in hemodynamics with percutaneous arterial oxygen saturation (SpO2) in young Andean highlanders in Bolivia. J Physiol Anthropol 39, 31 (2020). https://doi.org/10.1186/s40101-020-00240-y
Published:
DOI: https://doi.org/10.1186/s40101-020-00240-y