
Abstract
The genetic cause of idiopathic congenital talipes equinovarus (ICTEV) is largely unknown. We performed a systematic review to describe the findings from 21 studies that have examined the genetic variants related to ICTEV, and to evaluate the quality of reporting. We found that ICTEV was positively associated with Hox family genes, collagen family genes, GLI3, N-acetylation genes, T-box family genes, apoptotic pathway genes, and muscle contractile family genes. Negative and controversial results were also discussed, and several genes associated with ICTEV were identified. Due to the limitation of the included studies, rare coding variants should be further investigated, sample size should be enlarged, and candidate genes should be replicated in larger ICTEV populations. Epigenetic study, pathways, chromosome capture, and detailed gene-environment interaction will also allow further elucidation of factors involved in ICTEV pathogenesis and may shed light on diagnosis and timely and accurate interventions.
Similar content being viewed by others

Background
Idiopathic congenital talipes equinovarus (ICTEV), also called clubfoot, is a common orthopedic birth defect found in 1 of 1000 infants (Wynne-Davies 1964). Males are more commonly affected than females by a ratio of 2 to 1 and the incidence of bilaterality is 50 %. The highest prevalence is found in Hawaiians and Maoris, and the lowest in Chinese (Chapman et al. 2000; Chung et al. 1969). The etiology of ICTEV is largely unknown, but it is universally acknowledged that gene-environment interaction plays a major role (Lochmiller et al. 1998). A genetic component to the etiology of clubfoot has been established in several studies (Bacino and Hecht 2014). In this paper, we systematically review and summarize studies performed on ICTEV probands and families regarding susceptible genes, pathways, and epigenetic changes. Major findings in humans in the last 30 years are presented and ideas for further study are discussed.
Methods
Literature search strategy
This systematic review was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Moher et al. 2009). The process began with the first author (YBC) performing a systematic electronic literature search of PubMed, Web of Science, China Wanfang Med Online, and Cochrane Library, for publications from Jan 1985 to Dec 2014. Queries to identify potentially relevant publications on the genetic study of patients with ICTEV were based on Boolean combinations of the following search terms: ((Talipes Equinovarus (MeSH) OR Club Foot (MeSH)) AND (Gene (MeSH) OR Genetics (MeSH)).
Study eligibility criteria
We limited this review to publications that were in English and Chinese, with full text available, concerning patients diagnosed with ICTEV. Family based, discordant sib pair association and case–control studies were included. Studies were excluded if they were case reports, dissertations, editorials, commentaries, or review articles.
Data extraction
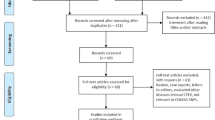
The first author (YBC) screened the titles and abstracts of all the retrieved articles to determine whether they met the eligibility criteria, and appraised the methodological quality and evidence of each selected study. The second author (XFX) subsequently reviewed the accuracy and quality of the appraisal. Any disagreements were discussed between the first and the second authors until consensus was reached. The flow diagram describes the process used to select articles for this study, and the results of the literature search (Fig. 1). The following information was extracted from each study: (1) Year of publication, (2) Study objectives, (3) Study’s inclusion and exclusion criteria, (4) Sample size, (5) Method, (6) Gene examined, (7) Association or non-association study, (8) Results, and (9) Corresponding author. Due to the heterogeneity in the study design, in this review, meta-analysis was not performed for those observational gene(s) identified among the various reviewed studies. Two investigators independently assessed the quality of the reporting. Differences in the assessment were resolved by discussion.

Flow diagram of the study identification and selection process
Results
Literature search
We identified 902 relevant studies from various resources (Fig. 1); the included studies examined the genetic associations between relevant genes and ICTEV. After reading the titles, 715 irrelevant articles were excluded. A total of 67 abstracts addressing certain gene(s) associated with ICTEV were selected to be reviewed. After reviewing, 36 articles did not meet our criteria and were excluded, including case reports (n = 4), letters to the editor (n = 3), reviews (n = 16), animal only studies (n = 7), no specific genes studied (n = 5), and treatment related (n = 1). For the remaining 30 articles, full texts were screened. Nine more articles were excluded due to normal control being unavailable (n = 1), inconsistency between method and result (n = 1), and functional study and other reasons (n = 7). Twenty-one studies met the predetermined inclusion criteria (Fig. 1).
Description of the included studies (Table 1)
From the studies gathered, we identified 21 that investigated genes or pathways which may contribute to the occurrence of ICTEV. Among them, some genes are positively associated with ICTEV, while others have shown no evidence of association. The genes with positive results include: (1) Hox family genes (HoxA and HoxD), (2) collagen family genes (COL9A1 and COL1A1), (3) GLI3, (4) N-acetylation genes (NAT2), (5) T-box family genes (TBX3 and TBX4), (6) apoptotic pathway genes (Casp3, Casp8, Casp9, Casp10, Bid, Bcl-2, and Apaf1), and (7) muscle contractile family genes (TNNC2 and TPM1). The genes with negative or controversial results are CAND2, WNT7a, MYH, and DTDST. Our critical review of these genes affecting ICTEV is summarized as follows:
Positive gene results
Hox family genes
The HOX genes encode a highly conserved family of transcription factors that play fundamental roles in morphogenesis during embryonic development. This group of genes determines the segment identity and also helps pattern the developing embryo in the development of the axial skeleton and limbs. Hoxa13 and Hoxd10-Hoxd13 are expressed during specification of the hand/foot (autopod) (Favier and Dollé 1997). A variety of limb malformations including synpolydactyly and hand-foot-genital syndrome are known to be caused by specific mutations in HOXD13 and HOXA13, respectively (Muragaki et al. 1996; Mortlock and Innis 1997) In 2003, Wang identified 12 alleles at Hox4Ep-a microsatellite marker on HoxD gene; transmission of disequilibrium was found at the 12th allele, indicating that HoxD may be a potential gene for ICTEV (Wang et al. 2003). Wang and her colleagues, who identified the susceptibility of HoxD with ICTEV from the previous study group, further found SNP rs847154 located in 5′ flanking sequence of HoxD12 gene and SNP rs13392701 located in exon 1 of HoxD13 to be associated with ICTEV (Wang et al. 2005). In another study investigating HoxA in ICTEV patients, the authors found seven alleles at D7S516 microsatellite and the presence of transmission disequilibrium in Chinese populations (Wang et al. 2008). Variants in HoxA and HoxD clusters and altered transmission in multiplex and simplex families were validated in a larger Western population with ICTEV in 2009 (Ester et al. 2009).
Collagen family genes
COL9A1 encodes one of the three alpha chains of Type IX collagen, which is a minor (5–20 %) collagen component of hyaline cartilage. Lack of Type IX collagen is associated with early onset of osteoarthritis, epiphyseal dysplasia, and intervertebral disc degeneration (Czarny-Ratajczak et al. 2001; Alizadeh et al. 2005; Boyd et al. 2008). Liu et al. studied COL9A1 which maps to chromosome 6q12-13 and found that 84 nuclear pedigrees had transmission disequilibrium in SNPs rs592121 and rs1135056, which are found in COL9A1(Liu et al. 2007). Expression of COL9A1 mRNA is significantly higher in patients with ICTEV than in healthy human subjects.
COL1A1 encodes the pro-alpha1 chains of Type I collagen, a fibril-forming collagen found in most connective tissues and abundant in bone, cornea, dermis, and tendon. Mutations in this gene are associated with osteogenesis imperfecta Types I–IV (Prockop et al. 1989; Takagi et al. 2015). Gene encoding collagen Type IV (COL1A1) was investigated in 2008 (Zhao et al. 2008). The results of this study show that expression of COL1A1 on mRNA levels is significantly higher in patients with ICTEV than in healthy patients. A −161(T → C) heterozygous mutation and a +274(C → G) homozygous mutation were also detected in the COL1A1 gene in patients with ICTEV, suggesting that COL1A1 mutations could cause ICTEV.
GLI3 gene
GLI3 encodes a protein which belongs to the C2H2-type zinc finger proteins subclass of the Gli family. The GLI3 protein localizes in the cytoplasm and activates patched Drosophila homolog (PTCH) gene expression. Mutations in the limb development related gene GLI3 have been associated with polydactyly (Volodarsky et al. 2014). SNP rs929387, located in exon 14 of the GLI3 gene, has transmission disequilibrium in 84 nuclear pedigrees, showing the association between the GLI3 gene and occurrence of ICTEV (Zha et al. 2006).
N-Acetylation genes
The NAT2 gene encodes an enzyme that functions to both activate and deactivate arylamine, hydrazine drugs and carcinogens. Polymorphisms in this gene are responsible for the N-acetylation polymorphism which in human populations segregates into rapid, intermediate, and slow acetylator phenotypes. Since smoking is one of the known environmental risk factors for ICTEV and NAT2 metabolizes tobacco byproducts, Hecht et al. (2007) examined the variants of the NAT2 gene in 56 ICTEV multiplex families, 57 trios with a positive family history, and 160 simplex individuals. They reported a slight decrease in the expected number of homozygotes for the NAT2 normal allele in the Hispanic simplex trios. Significantly slow NAT2 acetylator phenotype was detected among the ICTEV patients, suggesting slow acetylation may be a risk factor for ICTEV.
T-box family genes
A possible association between TBX3 and ICTEV has been reported. The TBX3 gene is a member of a phylogenetically conserved family of genes that share a common DNA-binding domain, the T-box. T-box genes encode transcription factors involved in the regulation of developmental processes. The TBX3 protein is a transcriptional repressor and mutations in this gene affect limb development. The third allele short tandem repeat (D12S378) in the region of chromosome 12q24, where the TBX3 gene is located, was proven to have transmission disequilibrium in ICTEV patients, suggesting that TBX3 is a susceptible gene for ICTEV (Ren et al. 2004). TBX4 shares a similar structure with TBX3. Expression studies in mice and chickens show that TBX4 is expressed in developing hindlimb but not forelimb buds, suggesting a potential role for this gene in regulating limb development and specification of limb identity (Dai et al. 2014; Menke et al. 2008). TBX4 microdeletions/microduplications have been found in individuals with clubfoot (Alvarado et al. 2010). However, another study which examined the possible correlation between hindfoot specific gene TBX4 and ICTEV concluded that (1) there was minimal evidence indicating an association between TBX4 and clubfoot; (2) no pathogenic sequence variants were identified in the two known TBX4 hindlimb enhancer elements (Lu et al. 2012). However, the PITX-TBX4 pathway was studied and further investigated by the common disease-rare gene supporters (Gurnett et al. 2008). The study concludes that PITX1 or its pathways may be etiologically responsible for the increased incidence of ICTEV.
Apoptotic pathway genes
Cysteine-dependent aspartate-directed proteases (Caspases) are a family of cysteine proteases that play essential roles in apoptosis (programmed cell death), necrosis, and inflammation (Alnemri et al. 1996). The association between caspase genes and ICTEV was first studied in 2005 (Heck et al. 2005). The authors reported that the major allele of a variant in the CASP10 gene, a gene in the apoptotic pathway, is associated with ICTEV in simplex white and Hispanic trios. Further examination on the mitochondrial apoptotic related genes was performed to investigate their association with ICTEV (Ester et al. 2007). One SNP in each of the apoptotic genes (Casp3, Casp8, Casp9, Casp10, Bid, Bcl-2, and Apaf1) provided evidence implying correlation with ICTEV, suggesting the potential role of genetic variation in apoptotic genes in development of ICTEV (Gahlmann and Kedes 1990).
Muscle contractile family genes
Troponin (Tn), a key protein complex in the regulation of striated muscle contraction, is composed of three subunits (Tn-I, Tn-T, and Tn-C). The Tn-I subunit inhibits actomyosin ATPase. The Tn-T subunit binds tropomyosin and Tn-C. The Tn-C subunit binds calcium and overcomes the inhibitory action of the troponin complex on actin filaments. TNNC2 encodes Tn-C subunit and plays a key role in initiating muscle contraction in fast-twitching muscle fibers (Mckillop and Geeves 1993). In 2011, Weymouth et al. studied the association of the muscle contractile genes with ICTEV and identified two muscle contractile genes (TNNC2 and TPM1) associated with ICTEV (Weymouth et al. 2011).
TPM1 is a member of the tropomyosin family of highly conserved, widely distributed actin-binding proteins involved in the contractile system of striated and smooth muscles and the cytoskeleton of non-muscle cells. Tropomyosin functions in association with the troponin complex to regulate the calcium-dependent interaction of actin and myosin during muscle contraction. The associations of multiple SNPs in the TPM1 gene with ICETV suggest a potential role of genes that encode contractile proteins of skeletal myofibers on the etiology of ICTEV (Shyy et al. 2010a, b).
Genome-wide association study
Besides the aforementioned candidate gene studies, a genome-wide association study was conducted in 396 isolated ICTEV patients and 1000 controls of European descent to identify novel genes for ICTEV (Zhang et al. 2014). The selected genetic variants from the genome-wide association study were further replicated with an independent cohort of 370 isolated ICTEV cases and 363 controls with the same ethnicity. The genome-wide association and replication study found an intergenic SNP on chromosome 12q24.31 between NCOR2 and ZNF664 that was significantly associated with ICTEV. However, Additional suggestive SNPs (Hox Genes, PITX1, TBX4, FOXN3, SORCS1 and MMP7/TMEM123) and identified pathways were not significant in the replication phase.
Negative or controversial results
Shyy et al. (2009) studied two candidate genes (CAND2 and WNT7a) and tested the hypothesis that mutations in these genes would be associated with the phenotype of ICTEV. After sequencing ICTEV patients, they found a polymorphism in each gene. However, the association results indicated that CAND2 and WNT7a are not the major genes that cause ICETV. In a study exploring variation in MYH gene families, the authors sequenced the exons, splice sites, and predicted promoters of MYH genes in ICETV patients (Shyy et al. 2010a, b). They found many SNPs, but none proved to be significantly associated with the phenotype of ICTEV. Bonafé et al. conducted research on diastrophic dysplasia sulphate transporter gene (DTDST) to test whether R279 W mutations are responsible for occurrence of ICTEV (Bonafé et al. 2002). Alterations in the coding region were not identified in 10 probands with ICTEV and a positive family history. The authors concluded that the R279 W mutation is no more frequent in this population of ICTEV probands than in controls. Contrary to this finding, another author reported in 2009 that DTDST gene mutations were detected in 27 children with ICTEV, but in only two normal children in the Chinese population, indicating the possible role of DTDST in ICTEV (He et al. 2009).
Other miscellaneous findings
In 2006, Sharp et al. found that children who carry the 677T variant of the MTHFR gene have a lower risk of ICTEV (Sharp et al. 2006). In 2009, Li and his colleagues compared the expression of CD-RAP (cartilage derived retinoic acid sensitive protein) in the abductor hallucis muscle from ICTEV and normal controls and found CD-RAP over-expressed in ICTEV patients, showing that CD-RAP might be a susceptibility gene of ICTEV (Li et al. 2009).
Discussion
In this systematic review, positive associations between genetic variants and ICTEV were established in several studies. Certain genetic variants were found to have significant association with ICTEV. However, it must be noted that conflicting and negative results were also identified which do not necessarily undermine their contribution to the occurrence of ICTEV.
ICTEV’s genetic study history is described in Fig. 2. Simple major genes like X-linked genes, autosomal recessive genes and autosomal dominant genes used to be considered as possible genetic factors for ICTEV (Palmer 1964; Böök 1948; Wynne 1965). At the same time, another study concluded that multifactorial inheritance is significant in the etiology of ICTEV (Yamamoto 1979). Palmer et al. (1974) suggested simple major inheritance and multifactorial inheritance might be operating together to induce ICTEV. This theory was supported later by Wang et al. and Yang et al. who showed that a major gene component played a dominant role with additional minor contributions of multifactorial genes (Yang et al. 1987; Wang et al. 1988). In 1993, Rebbeck et al. (1993) rejected the non-Mendelian transmission pattern and concluded that the single Mendelian gene theory is adequate to explain the etiology of ICTEV. However, recent studies suggest that a polygenetic threshold model may explain its inheritance patterns. Contrary to the common disease-common variant hypothesis, one author introduced an alternative theory based on recent reports that rare genetic variants (with allele frequencies of <5 %) each confer a moderate risk with higher penetrance, which might be the genetic inheritance pattern of ICTEV. According to this theory, the PITX1-TBX4 transcriptional pathway directing early limb development is responsible for ICTEV (Dobbs and Christina 2012). However, further studies should be done to investigate other genes with low frequencies and how their variants affect ICTEV occurrence. Not only were gene mutations found in ICTEV, but chromosomal deletions and regulatory mutations were also reported.

Genetic study history of ICTEV is shown. Different genes were identified in different years which are listed in blue boxes. The genetic theories to explain the etiology of ICTEV are marked in the green boxes. Several genes were identified and verified by Professor Jacqueline T. Hecht and her research group (under the timeline on the left); they identified and verified several genes in addition to caspase pathway changes in ICTEV patients. Dr. Christina A Gurnett (under on the timeline on the right) first used second generation sequencing methods to study ICTEV. Professor Chun-Lian Jin (above the timeline) pioneered clubfoot genetic study among Chinese patients
Conclusion
Several genes were identified, though none of them could solely explain the occurrence of ICTEV. Because the sample size of most association studies was small, most of the studies included are largely underpowered. In those included studies, rare coding variants were rarely investigated. Candidate genes were not replicated in larger ICTEV populations. These limitations should be addressed in future studies. In the future, genetic research on ICTEV could be focused on at least five aspects. First, high-throughput sequencing instead of GWA studies might be used to detect replicable candidate genes. The sample size should be calculated and candidate genes must be replicated in other studies. Second, epigenetic sequencing examining regulatory mechanisms for RNA could be studied. Third, novel genes like FOXN3 and SORCS1 identified by the GWAS may be further investigated. Studying genes and their interactions could reveal common pathways which are responsible for the occurrence of ICTEV. Their functions and interactions are worthy of clarification. Fourth, recent advances in chromosome conformation capture may show more structural changes on a chromosomal level (Imakaev et al. 2012). Three-dimensional variants may shed light on ICTEV etiology and treatment. Fifth, in clinical practice, some patients do not have any recurrence although they are not completely compliant with the brace treatment, whereas other patients have a recurrence even though they are strictly compliant with the brace treatment (Zhao et al. 2014). It is conceivable that certain genes being activated at certain times results in the relapse of ICTEV. Therefore, integration of genomic risk assessment alongside other clinical investigations may help personalize the treatment of ICTEV and improve the prognosis in the era of precision medicine (Castaneda et al. 2015).
References
Alizadeh BZ, Njajou OT, Bijkerk C, Meulenbelt I, Wildt SC, Hofman A, Pols HA, Slagboom PE, Duijn CM (2005) Evidence for a role of the genomic region of the gene encoding for the alpha1 chain of type IX collagen (COL9A1) in hip osteoarthritis: a population-based study. Arthritis Rheum 52(5):1437–1442
Alnemri ES, Livingston DJ, Nicholson DW, Salvesen G, Thornberry NA, Wong WW, Yuan J (1996) Human ICE/CED-3 Protease Nomenclature. Cell 87(2):171. doi:10.1016/S0092-8674(00)81334-3
Alvarado DM, Aferol H, McCall K, Huang JB, Techy M, Buchan J, Cady J, Gonzales PR, Dobbs MB, Gurnett CA (2010) Familial isolated clubfoot is associated with recurrent chromosome 17q23.1q23.2 microduplications containing TBX4. Am J Hum Genet 87:157–160. doi:10.1016/j.ajhg.2010.06.010
Bacino AG, Hecht TJ (2014) Etiopathogenesis of equinovarus foot malformations. Eur J Med Genet 57:473–479
Bonafé L, Blanton SH, Scott A, Broussard S, Wise CA, Superti-Furga A, Hecht JT (2002) DTDST mutations are not a frequent cause of idiopathic talipes equinovarus (club foot). J Med Genet 39:e20
Böök JAA (1948) Contribution to the genetics of congenital clubfoot. Hereditas 34:289–300
Boyd LM, Richardson WJ, Allen KD, Flahiff C, Jing L, Li Y, Chen J, Setton LA (2008) Early-onset degeneration of the intervertebral disc and vertebral end plate in mice deficient in type IX collagen. Arthritis Rheum 58(1):164–171
Castaneda C, Nalley K, Mannion C, Bhattacharyya P, Blake P, Pecora A, Goy A, Suh KS (2015) Clinical decision support systems for improving diagnostic accuracy and achieving precision medicine. J Clin Bioinforma 26(5):4. doi:10.1186/s13336-015-0019-3
Chapman C, Stott NS, Port RV, Nicol RO (2000) Genetics of club foot in Maori and Pacific people. J Med Genet 37(9):680–683
Chung CS, Nemechek RW, Larsen IJ, Ching GH (1969) Genetic and epidemiological studies of clubfoot in Hawaii. General and medical considerations. Hum Hered 9:321–342
Czarny-Ratajczak M, Lohiniva J, Rogala P, Kozlowski K, Perälä M, Carter L, Spector TD, Kolodziej L, Seppänen U, Glazar R, Królewski J, Latos-Bielenska A, Ala-Kokko L (2001) A mutation in COL9A1 causes multiple epiphyseal dysplasia: further evidence for locus heterogeneity. Am J Hum Genet 69(5):969–980
Dai M, Wang Y, Fang L, Irwin DM, Zhu T, Zhang J, Zhang S, Wang Z (2014) Differential expression of Meis2, Mab21l2 and Tbx3 during limb development associated with diversification of limb morphology in mammals. PLoS ONE 9(8):106100. doi:10.1371/journal.pone.0106100
Dobbs BM, Christina AG (2012) Genetics of Clubfoot. J Pediatr Orthop B 21(1):7–9
Ester AR, Tyerman G, Wise CA, Blanton SH, Hecht JT (2007) Apoptotic gene analysis in idiopathic talipes equinovarus (Clubfoot). Clin Orthop Relat Res 462:32–37
Ester AR, Weymouth KS, Burt A, Wise CA, Scott A, Gurnett CA, Dobbs MB, Blanton SH, Hecht JT (2009) Altered transmission of HOX and apoptotic SNPs identify a potential common pathway for clubfoot. Am J Med Genet A 149A(12):2745–2752
Favier B, Dollé P (1997) Developmental functions of mammalian Hox genes. Mol Hum Reprod 3:115–131
Gahlmann R, Kedes L (1990) Cloning, structural analysis, and expression of the human fast twitch skeletal muscle troponin C gene. J Biol Chem 265(21):12520–12528
Gurnett CA, Alaee F, Kruse LM, Desruisseau DM, Hecht JT, Wise CA, Bowcock AM, Dobbs MB (2008) Asymmetric lower-limb malformations in individuals with homeobox PITX1 gene mutation. Am J Hum Genet 83(5):616–622
He BB, Wu XL, Du XP, Xiong ZG, Zeng XH (2009) Research of association between DTDST gene mutation and congenital talipes equinovarus. J Clin Pediatr Sug 8(2):32–34
Hecht JT, Ester A, Scott A, Wise CA, Iovannisci DM, Lammer EJ, Langlois PH, Blanton SH (2007) NAT2 variation and idiopathic talipes equinovarus (clubfoot). Am J Med Genet A 143A:2285–2291
Heck AL, Bray MS, Scott A, Blanton SH, Hecht JT (2005) Variation in CASP10 gene is associated with idiopathic talipes equinovarus. J Pediatr Orthop 25:598–602
Imakaev M, Fudenberg G, McCord RP, Naumova N, Goloborodko A, Lajoie BR, Dekker J, Mirny LA (2012) Iterative correction of Hi-C data reveals hallmarks of chromosome organization. Nat Methods 9(10):999–1003
Li LY, Zhao Q, Sun KL, Sun KL, Jin CL (2009) Expression of cartilage-derived retinoic acid sensitive protein gene in muscular tissue from patients with congenital clubfoot. Chin J Pediatr Surg 30(8):551–554
Liu LY, Jin CL, Cao DH, Zhao N, Lin CK, Sun KL (2007) Analysis of association between COL9A1 gene and idiopathic congenital talipes equinovarus. Hereditas (Beijing) 29(4):427–432
Lochmiller C, Johnston D, Scott A, Risman M, Hecht JT (1998) Genetic epidemiology study of idiopathic talipes equinovarus. Am J Med Genet 79:90–96
Lu W, Bacino CA, Richards BS, Alvarez C, VanderMeer JE, Vella M, Ahituv N, Sikka N, Dietz FR, Blanton SH, Hecht JT (2012) Studies of TBX4 and chromosome 17q23.1q23.2: an uncommoncause of nonsyndromic clubfoot. Am J Med Genet A 158A(7):1620–1627
McKillop DF, Geeves MA (1993) Regulation of the interaction between actin and myosin subfragment 1: evidence for three states of the thin filament. Biophys J 65(2):693–701
Menke DB, Guenther C, Kingsley DM (2008) Dual hindlimb control elements in the Tbx4 gene and region-specific control of bone size in vertebrate limbs. Development 135:2543–2553
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009) Reprint preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther 89:873–880
Mortlock DP, Innis JW (1997) Mutation of HOXA13 in hand-foot-genital syndrome. Nat Genet 15:179–180
Muragaki Y, Mundlos S, Upton J, Olsen BR (1996) Altered growth and branching patterns in synpolydactyly caused by mutations in HOXD13. Science 272:548–551
Palmer RM (1964) The genetics of talipes equinovarus. J Bone Joint Surg 46A:542–556
Palmer RM, Conneally PM, Yu PL (1974) Studies of the inheritance of idiopathic talipes equinovarus. Orthop Clin North Am 5:99–108
Prockop DJ, Constantinou CD, Dombrowski KE, Hojima Y, Kadler KE, Kuivaniemi H, Tromp G, Vogel BE (1989) Type I procollagen: the geneprotein system that harbors most of the mutations causing osteogenesis imperfecta and probably morecommonheritable disorders of connective tissue. Am J Med Genet 34:60–67
Rebbeck TR, Dietz FR, Murray JC, Buetow KH (1993) A Single-Gene Explanation for the Probability of Having Idiopathic Talipes Equinovarus. Am J Hum Genet 53:1051–1063
Ren SY, Ma HW, Jiang J, Ji SJ, Ma RX, Wang DJ, Chen Q (2004) Transmission disequilibrium test for congenital clubfoot and PAX5, PAX6 and TBX3 genes. Chin J Pediatr Surg 25(5):444–447
Sharp L, Miedzybrodzka Z, Cardy AH, Inglis J, Madrigal L, Barker S, Chesney D, Clark C, Maffulli N (2006) The C677T polymorphism in the methylenetetra hydrofolate reductase gene (MTHFR), maternal use of folic acid supplements, and risk of isolated clubfoot: a case-parent-triad analysis. Am J Epidemiol 164:852–861
Shyy W, Dietz F, Dobbs MB, Sheffield VC, Morcuende JA (2009) Evaluation of CAND2 and WNT7a as candidate genes for congenital idiopathic clubfoot. Clin Orthop Relat Res 467:1201–1205
Shyy W, Wang K, Sheffield VC, Morcuende JA (2010a) Evaluation of embryonic and perinatal myosin gene mutationsand the etiology of congenital Idiopathic clubfoot. J Pediatr Orthop. doi:10.1097/BPO.0b013e3181d35e3f
Shyy W, Wang K, Sheffield VC, Morcuende JA (2010b) Evaluation of embryonic and perinatal myosin gene mutations and the etiology of congenital idiopathic clubfoot. J Pediatr Orthop 30(3):231–234
Takagi M, Shinohara H, Narumi S, Nishimura G, Hasegawa Y, Hasegawa T (2015) Severe osteogenesis imperfecta caused by double glycine substitutions near the amino-terminal triple helical region in COL1A2. Am J Med Genet A. doi:10.1002/ajmg.a.37051
Volodarsky M, Langer Y, Birk OS (2014) A novel GLI3 mutation affecting the zinc finger domain leads to preaxial-postaxial polydactyly-syndactyly complex. BMC Med Genet 30(15):110. doi:10.1186/s12881-014-0110-9
Wang J, Palmer RM, Chung CS (1988) The role of major gene in clubfoot. Am J Hum Genet 42:772–776
Wang DJ, Ma RX, Chen Q, Gao H, Ma HW, Ji SJ (2003) Transmission test for linkage disequilibrium in HoxD gene and congenital club foot. Chin J Pediatr Surg 24(4):348–350
Wang LL, Jin CL, Liu LY, Zhang X, Ji SJ, Sun KL (2005) Analysis of association between 5′HOXD gene and idiopathic congenital talipes equinovarus. Chin J Med Genet 22(6):653–656
Wang NQ, Ma RX, Ji SJ, Jin CL (2008) HoxA transmission disequilibrium in congenital clubfoot. Chin J Pediatr Surg 29(2):104–106
Weymouth KS, Blanton SH, Bamshad MJ, Beck AE, Alvarez C, Richards S, Gurnett CA, Dobbs MB, Barnes D, Mitchell LE, Hecht JT (2011) Variants in genes that encode muscle contractile proteins influence risk for isolated clubfoot. Am J Med Genet A 155(9):2170–2179
Wynne DR (1965) Family studies and aetiology of clubfoot. J Med Genet 2:227–232
Wynne-Davies R (1964) Family studies and the cause of congenital club foot: talipesequinovarus, talipescalcaneo-valgus and metatarsus varus. J Bone Joint Surg Br 46:445–463
Yamamoto H (1979) A clinical genetic and epidemiologic study of congenital clubfoot. Jpn J Hum Genet 24:37–44
Yang H, Chung CS, Nemechek RW (1987) A genetic analysis of clubfoot in Hawaii. Genet Epidemiol 4:299–306
Zha X, Jin CL, Liu LY, Zhao N, Zhang LJ, Sun KL (2006) Association and mutation analysis of GLI3 gene in idiopathic congenital talipes equinovarus. Chin J Med Genet 23(5):551–554
Zhang TX, Haller G, Lin P, Alvarado DM, Hecht JT, Blanton SH, Stephens Richards B, Rice JP, Dobbs MB, Gurnett CA (2014) Genome-wide association study identifies new disease loci for isolated clubfoot. J Med Genet 51:334–339
Zhao N, Jin CL, Liu LY, Cao DH, Lin CK, Ji SJ, Sun KL (2008) Association study between mutations of transcription regulator sequences of COL1A1 gene and idiopathic congenital talipes equinovarus. Hereditas (Beijing) 30(6):723–727
Zhao D, Liu J, Zhao L, Wu Z (2014) Relapse of clubfoot after treatment with the Ponseti method and the function of the foot abduction orthosis. Clin Orthop Surg 6(3):245–252
Authors’ contributions
Dr. H-WX and Dr. B-CY designed the study. Dr. B-CY and F-XX searched articles and extracted the data. Dr. B-CY and Dr. L-JZ analyzed the data. Prof. H-WD and Dr. L-JZ revised the manuscript critically. All authors read and approved the final manuscript.
Acknowledgements
This study was financed by research grants awarded by Bureau of Health of Guangzhou Municipality (20141A010022). Dr. Hong-Wen Deng and Dr. Lan-Juan Zhao are partially supported by grants from National Institute of Health (R01AR059781, R01AR050496, R01AR057049), and Edward G. Schlieder Endowment from Tulane University. English editing for the manuscript was made by Joanna Yong and Loula Burton.
The present study was performed in Guangzhou Women and Children’s Medical Center.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Yong, BC., Xun, FX., Zhao, LJ. et al. A systematic review of association studies of common variants associated with idiopathic congenital talipes equinovarus (ICTEV) in humans in the past 30 years. SpringerPlus 5, 896 (2016). https://doi.org/10.1186/s40064-016-2353-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40064-016-2353-8