
Abstract
Given the growing aged care population, the complexity of their medication-related needs and increased risk of adverse drug events, there is a necessity to systematically monitor and manage medication-related quality of care. The aim of this systematic review was to identify and synthesise medication-related quality of care indicators with respect to application to residential aged care. MEDLINE (Ovid), Psychinfo, CINAHL, Embase and Google® were searched from 2001 to 2013 for studies that were in English, focused on older people aged 65+ years and discussed the development, application or validation of original medication-related quality of care indicators. The quality of selected articles was appraised using the Critical Appraisal Skills Program and psychometric qualities extracted and synthesised using content analysis. Indicators were mapped to six medication-related quality of care attributes and a minimum indicator set derived. Thirty three articles describing 25 indicator sets met the inclusion criteria. Thirteen (52%) contained prescribing quality indicators only. Eight (32%) were developed specifically for aged care. Twenty three (92%) were validated and seven (28%) assessed for reliability. The most common attribute addressed was medication appropriateness (n = 24). There were no indicators for evaluating medication use in those with limited life expectancy, which resulted in only five of the six attributes being addressed. The developed minimum indicator set contains 28 indicators representing 22 of 25 identified indicator sets. Whilst a wide variety of validated indicator sets exist, none addressed all aspects of medication-related quality of care pertinent to residential aged care. The minimum indicator set is intended as a foundation for comprehensively evaluating medication-related quality of care in this setting. Future work should focus on bridging identified gaps.
Similar content being viewed by others

Key points
-
Twenty eight previously validated medication-related quality of care indicators (minimum indicator set) were identified as relevant to both the aged care setting and clinical needs of residents.
-
Validated indicators which address appropriate medication-related care in those with limited life expectancy are lacking and need to be explored further.
-
The minimum indicator set developed in this study is intended as a foundation for increasing the utilisation of medication-related quality of care indicators in the aged care sector.
Introduction
In Australia and other developed countries the population is ageing rapidly. Since 1970, the Australian population has aged significantly with a six-fold increase in the proportion of adults aged 85 years and older (Australian Institute of Health and Welfare 2010) with similar statistics reported in the UK, Europe and the USA (Office for National Statistics. Statistical Bulletin: Older People’s Day 2011; Howden & Meyer 2011). One consequence of an ageing population is increased demand on health care and social support systems. In 2011, 165,000 Australians lived in permanent aged care (Australian Institute of Health and Welfare 2012) and it is projected that by 2050 aged care services will be provided to around 3.5 million Australians (1 million in permanent residential care) at a financial cost of $1.8% of the GDP (Commonwealth of Australia 2010).
The prevalence of multiple chronic conditions (multimorbidity) in the older population is reported to be between 65 to 80% (Britt et al. 2008). Multimorbidity is associated with use of multiple medicines (polypharmacy) which in turn is linked to medication-related adverse outcomes including falls, death and hospitalisation (Wilson et al. 2010; Milton et al. 2008). This is compounded by the physiologic effects of ageing, such as altered clearance of medicines (Milton et al. 2008). In the United States medication-related adverse events in residential aged care have been estimated to be between 1.19 to 7.26 incidents per 100 resident-months and for every $1 (US) spent on medicines in aged care it is estimated $1.33 is spent on treating adverse events (Bootman et al. 1997).
Given the growing aged care population, the complexity of their medication-related needs and increased risk of adverse drug events, there is a necessity to systematically monitor and manage medication-related quality of care. Quality of care is traditionally evaluated using indicators which target the most relevant aspects of healthcare (Arah et al. 2006; Mainz 2003). Whilst there is ongoing constructive debate regarding the relationship between quality of care indicators and patient outcomes, they remain the gold standard for evaluating the quality of many aspects of health care. For example, the National Committee for Quality Assurance in the USA and the National Institute for Health and Care Excellence in the United Kingdom both advocate the use indicators for evaluating quality of care (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; National Institute for Health and Care Excellence 2014a). In the Australian setting, the 2011 Productivity Commission Inquiry Report, Caring for Older Australians, identified the need for validated indicators that address the quality of care in the aged care population, including medication-related quality of care (Productivity Commission 2011).
Whilst a variety of indicators exist to evaluate the medication-related quality of care in the ambulatory elderly, few specifically address the needs of the residential aged care population. The aged care population is commonly frailer and more dependent than the ambulatory older population and as a consequence has different medication-related needs. Expectations of health outcomes may also differ between the two populations due to differences in quality of life values and life expectancy. Additionally, many medication-related quality of care sets are overburdened with dozens of indicators and minimal direction for prioritising the evaluation process, minimizing their utilisation in the clinical setting.
The aims of this systematic review were to identify, describe and consolidate the most appropriate and feasibly actionable medication-related quality of care indicators for use in residential aged care and more specifically for Australian residential aged care.
Methods
Data sources
MEDLINE (Ovid), PsycINFO, Embase and CINAHL databases were searched between January 2001 to December 2013. The following search terms (Medical Subject Headings and keywords) were used for all four databases: Quality Assurance, Health Care/ or *“Quality of Health Care”/ or “quality of health care*”.mp. AND*Quality Indicators, Health Care/ or *“Outcome and Process Assessment (Health Care)”/ or clinical indicator*.mp. OR prescribing indicator*.mp. OR *Polypharmacy/ or polypharmacy*.mp. OR inappropriate prescribing*.mp. OR “Quality use of medicine*”.mp. The search was limited to articles published in English and focusing on older people aged 65 years and older. Reference lists of eligible papers were searched to further identify suitable publications. If an article identified via reference check list was not published within the pre-defined time frame it was included if the indicator(s) was currently used in public reporting or research. ‘Quality in Health care’ was used as the search term for Google® with the first 100 hits screened to maximize relevance to the search criteria. Authors’ knowledge of government and organisation websites with a focus on delivery and/or evaluation of health care were also searched for relevant articles (Websites searched include AIHW (Australian Institute of Health and Welfare) (www.aihw.gov.au), Institute for Healthcare Improvement (www.ihi.org), NPS (National Prescribing Service) (www.nps.org.au), European Directorate for the Quality Use of Medicines & Healthcare (www.edqm.eu), European Society for Quality in Health care (www.esqh.net), CMS (Centers for Medicare and Medicaid Services) (www.cms.gov), Health Indicators Warehouse (www.healthindicators.gov), NICE (National Institute for Health and Clinical Excellence) (www.nice.org.uk), RAND Corporation (www.rand.org), Cochrane Collaboration (www.cochrane.org) and Emerging Researchers in Ageing (www.era.edu.au).
The search strategy was developed in consultation with a librarian specialising in health databases. Methods for identifying and selecting the articles were predetermined in a protocol developed collaboratively by all three authors. The reporting of this systematic review conforms to the PRISMA checklist endorsed by the Cochrane Collaboration (Moher et al. 2009).
Study selection
Original articles describing the development of an indicator or set of indicators to assess the quality of care in the elderly (>65 years) were included if they addressed at least one aspect of medication use. Articles were excluded if they: (1) were undertaken in populations with specific care needs mostly unrelated to the older population such as paediatrics, oncology, obstetrics and HIV patients (2) focused on assessing the quality of care in settings unrelated to aged care such as emergency care and surgery or (3) discussed the application of, or adaptation of an existing indicator(s). For example, articles which discussed the adaption of Beers Criteria to a country’s pharmacopeia were excluded as this was considered an adaption of an existing indicator set. Research involving the amalgamation of several indicator sets was also excluded. Articles relating to transitional care were excluded as the focus of this research is not the process of moving into or out of aged care.
For the purposes of this research a medication-related quality of care indicator was defined as a ‘measure to be used as a guide to monitor, evaluate and improve the direct and indirect aspects of medication use affecting quality of care and patient outcomes.’ Direct aspects of medication use include prescribing, administration of medications and clinical services related to medication use. Indirect aspects of medication use include organisational factors and health outcomes.
Reviewers
One author (JH) conducted the initial database search, the first three sifts of articles, the Google® search and reference list check. Relevant articles were assessed for quality using the Critical Appraisal Skills Program (CASP) criteria by one author (JH) (Critical Appraisal Skills & United Kingdom: www.casp-uk.net Accessed [September 2011). All three reviewers (JH, AV and GC) met to discuss the appropriateness of inclusion of each article with respect to the inclusion criteria and the quality of the article. Disagreements were resolved by discussion. Articles were excluded if they did not meet all CASP criteria. CASP is recommended by the Cochrane Collaboration as a simple and effective tool to analyse the quality of qualitative research (Hannes 2011).
Data extraction and synthesis
Data extraction and synthesis was undertaken in several stages. Firstly, descriptive qualities were extracted from each indicator set with an emphasis on medication use, country of origin, target population and operational status by one author (JH). Secondly, content analysis was used to synthesise the psychometric properties of the indicator sets as it is a systematic, effective and transparent method for categorising data and identifying commonalities between qualitative studies (Dixon-Woods et al. 2005). Whilst there is no standardised way of categorising quality of care indicators, several key psychometric qualities were identified from the literature (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Clark & Bierman 2009; Australian Institute of Health and Welfare 2009). Consumer involvement was added due to its significance to Australian medicines policy (Department of Health and Ageing 1999). The final content analysis template was approved by all authors and systematically applied using a standardised data collection form by one author (JH). All authors (JH, AV and GC) met and reviewed the descriptive qualities and content analysis results for each article. Disagreements were resolved by discussion.
Thirdly, a subsequent search to establish basic operational status and further validation studies of the included indicator sets was performed by one author (JH) in February 2014 using Google® and Google scholar® with the indicator name.
Definitions of key psychometric properties
The aspect of health care they evaluate: indicators can be described using a three part inter related hierarchical structure (Donabedian 1966). Structural indicators evaluate the characteristics of the organisation providing the care, process indicators evaluate the care that is provided and outcome indicators evaluate the results of the care provided.
Type of indicator: explicit indicators are criteria-based whereas implicit indicators rely more on individual clinical judgment (Donabedian 1988; Lund et al. 2011; Chang & Chan 2010; Spinewine et al. 2007).
Scientific merit of the indicators: indicators should measure what they intend to measure (content validity), be meaningful and relevant to the key audience (face validity) and identify the same effect when measured at different times or by different people (reliability) (Martirosyan et al. 2010). Other properties that are useful to demonstrate are concurrent validity (comparison of indicator to a gold standard) and predictive validity (the ability of the indicator to predict a health outcome) (Martirosyan et al. 2010).
Real life application: both external validity (the ability of the indicator to be applied as effectively to another health care setting or in another country) and feasibility (the degree to which the required data can be collected and reported in a timely manner) describe the practicality of the indicator and can often determine if the indicator is reported (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Burchett et al. 2011).
Consumer involvement: consumers are central to Australia’s National Medicines Policy (Department of Health and Ageing 1999) and should contribute to the discussion on prioritizing measures to evaluate aspects of health care rather than relying solely on expert opinion.
Once identified and described each indicator set was mapped to six of the most relevant medication-related quality of care attributes for Australian residential aged care. These attributes were derived by all authors (JH, AV and GC) from sentinel papers on quality of care for the medically complex elderly, known epidemiology of chronic disease and medication use in Australian residential aged care and Australian medicines policy. The initial mapping was undertaken by one author (JH) and results were reviewed by two authors (AV and GC). These attributes do not address every medication-related quality of care issue for aged care residents. They are intended to assist with targeting the most significant issues according to the available information at the time of this study. They are intended to focus evaluation of medication-related QOC on the greatest burden of disease, greatest medication-related risk factors and relevant quality of care activities in the aged care population. This parsimonious approach to selecting indicators is concordant with the conceptual framework for developing and implementing health care indicators as it improves the feasibility of implementation (Donabedian 1980).
Medication-related attributes relevant to Australian residential aged care
General medication appropriateness: Appropriateness of medication is a central tenant to many quality of care models including the Australian quality use of medicines strategic plan (Australian Institute of Health and Welfare 2009; Department of Health and Ageing 1999; Donabedian 1980). Medication appropriateness is defined as the use of a medication only when necessary, with consideration to an individual’s clinical indications, co-existing conditions and the risk-benefit profile using evidenced-based criteria.
There is a growing awareness of the complexity between managing patient’s multiple chronic diseases using evidence based guidelines for each condition and maximising the benefit to the individual (Tinetti et al. 2004; Tinetti et al. 2012; Gilbert et al. 2011). This is particularly relevant to the challenges of assessing quality of care in the frail and medically complex older population, who are commonly excluded from clinical trials from which evidence based guidelines are derived. (Holmes et al. 2013; Marengoni 2013). Attention will be directed to identifying indicators which attempt to address this gap.
Medication appropriateness for the most prevalent chronic diseases: The most prevalent diseases in the Australian aged care population are dementia, cardiovascular disease (CVD) and musculoskeletal conditions (Australian Institute of Health and Welfare 2012).
Medication appropriateness those with limited life expectancy: The majority of Australian aged care residents die within three years of admission to residential care (Australian Institute of Health and Welfare 2012). Medication should be reconciled with respect to time to benefit (Holmes et al. 2013).
Detection and monitoring for adverse drug events: Chart review studies undertaken in Australian residential aged care reveal that the majority of residents are exposed to over five medicines per day many of which are associated with adverse outcomes in the older population (Somers et al. 2010; Wilson et al. 2011). In 2008, a population based study found that residents were taking on average nine or more medicines with 50% exposed to psychotropic medication which are known to be related to adverse events such as falls (Roughead et al. 2008). Attention will be directed to indicators which monitor and detect for adverse drug events.
Access to medication-related services: Australian aged care residents are entitled to several medication-related services, such as medication reviews, which may influence the quality of medication use (Gilbert et al. 2002). These services are an opportunity to modify prescribing according to the resident’s current clinical condition as well as identifying adverse drug reactions.
Medication-related quality of care policies: Both in Australia and overseas, it is recommended that residential aged care facilities regularly review medication management policies and procedures as part of their quality improvement cycle (Department of Health 2012; National Institute for Health and Care Excellence 2014b).
Developing the minimum indicator set
The results from mapping were used to guide the development of a minimum indicator set for evaluating medication-related quality of care in Australian residential aged care. The objectives were to identify and synthesise the most appropriate indicators with respect to the core needs of this population (six key medication-related attributes) which can be feasibly implemented within the Australian aged care setting to facilitate the assessment of quality of care.
Individual indicators were included in the minimum indicator set if they addressed at least one of the six core medication-related attributes and were present in three or more of the identified indicator sets. This represented the most parsimonious balance of addressing the majority of attributes without overburdening the evaluation process. Indicators included in the minimum indicator set also needed to be feasibly collected and reported at a population level. The minimum indicator set was initially developed by one author (JH) and reviewed by two authors (AV and GC) and disagreements resolved by discussion.
Results
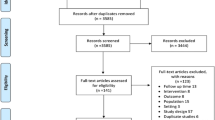
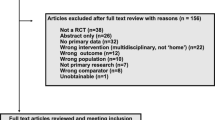
A total of 33 articles discussing 25 independent indicator sets were included in the systematic review (see Figure 1 for study selection flowchart). For some indicator sets more than one article was necessary to describe their development. Table 1 describes the included indicator sets grouped according to their emphasis on medication use and described by country of origin, target population and current operational status.

Flowchart of the study selection process.
Eight of the identified indicator sets are general quality of care indicator sets which contain at least one medication-related quality of care indicator (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Australian Institute of Health and Welfare 2009; Campbell Research and Consulting (CR&C) 2006; Nay et al. 2004; Courtney et al. 2007; Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; Wegner et al. 2007; Primary Care & Social Care Information Centre 2013). Four indicator sets focus on medication-related quality of care and evaluate a range of activities related to medication use (Department of Health 2012; NSW Therapeutic Assessment Group 2007; National Prescribing Service 2006; Mackinnon & Hepler 2002). Thirteen sets address prescribing and these are commonly referred to in the literature as prescribing quality indicators or PQIs (Basger et al. 2008; Hilmer et al. 2007; Holt et al. 2010; McLeod et al. 1997; The American Geriatrics Society 2012; Hanlon et al. 1992; Rognstad et al. 2009; Huisman-Baron et al. 2011; O'Mahony et al. 2010; Winit-Watjana et al. 2008; Laroche et al. 2007; Rancourt et al. 2004; Onder et al. 2013). The majority of indicator sets originated from Australia (n = 8) (Australian Institute of Health and Welfare 2009; Department of Health 2012; Campbell Research and Consulting (CR&C) 2006; Nay et al. 2004; Courtney et al. 2007; NSW Therapeutic Assessment Group 2007; National Prescribing Service 2006; Basger et al. 2008) and the USA (n = 6) (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; Wegner et al. 2007; Hilmer et al. 2007; The American Geriatrics Society 2012; Hanlon et al. 1992).
Eight of the indicator sets were developed specifically for aged care. Two of these eight addressed several aspects of medication-related quality of care (e.g. prescribing, medication review, consumer counseling, medication reconciliation) (Department of Health 2012; Wegner et al. 2007). Three included one or more of the following medication-related quality of care indicators: polypharmacy, prevalence of medication use and medication review (Campbell Research and Consulting (CR&C) (Campbell Research and Consulting (CR&C) 2006); (Nay et al. 2004; Courtney et al. 2007)) and the remaining three indicator sets developed for residential aged care contained PQIs (Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; The American Geriatrics Society 2012; Rancourt et al. 2004).
Three indicator sets are currently systematically externally reported (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; Primary Care & Social Care Information Centre 2013). Sixteen of the indicator sets have or are undergoing further validation studies and/or subsets of their dataset have been reported elsewhere (Nay et al. 2004; Courtney et al. 2007; Wegner et al. 2007; Basger et al. 2008; Hilmer et al. 2007; Holt et al. 2010; McLeod et al. 1997; The American Geriatrics Society 2012; Hanlon et al. 1992; Rognstad et al. 2009; Huisman-Baron et al. 2011; O'Mahony et al. 2010; Laroche et al. 2007; Rancourt et al. 2004; Onder et al. 2013; Robertson & MacKinnon 2002). No evidence of further validation, use or reporting was found for six indicator sets (Australian Institute of Health and Welfare 2009; Department of Health 2012; Campbell Research and Consulting (CR&C) 2006; NSW Therapeutic Assessment Group 2007; National Prescribing Service 2006; Winit-Watjana et al. 2008).
Content analysis
The psychometric properties of the identified indicators sets are listed in Table 2. Nineteen (76%) of the indicator sets contained only process indicators (Campbell Research and Consulting (CR&C) 2006; Nay et al. 2004; Courtney et al. 2007; Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; Wegner et al. 2007; NSW Therapeutic Assessment Group 2007; Basger et al. 2008; Hilmer et al. 2007; Holt et al. 2010; The American Geriatrics Society 2012; Hanlon et al. 1992; Rognstad et al. 2009; Huisman-Baron et al. 2011; O'Mahony et al. 2010; Winit-Watjana et al. 2008; Laroche et al. 2007; Rancourt et al. 2004; Onder et al. 2013; Naugler et al. 2000) and the majority of these (n = 13) were PQIs. Only one indicator set included medication-related outcome indicators, the preventable drug-related morbidity (PDRM) indicator set, which had over fifty medication-related outcome indicators (Mackinnon & Hepler 2002). Five sets contained a combination of structural, process and outcome indicators (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Australian Institute of Health and Welfare 2009; Department of Health 2012; Primary Care & Social Care Information Centre 2013; National Prescribing Service 2006). The majority (80%) included only explicit indicators (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Australian Institute of Health and Welfare 2009; Campbell Research and Consulting (CR&C) 2006; Nay et al. 2004; Courtney et al. 2007; Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; Wegner et al. 2007; Primary Care & Social Care Information Centre 2013; NSW Therapeutic Assessment Group 2007; National Prescribing Service 2006; Mackinnon & Hepler 2002; Hilmer et al. 2007; Holt et al. 2010; The American Geriatrics Society 2012; Rognstad et al. 2009; O'Mahony et al. 2010; Winit-Watjana et al. 2008; Laroche et al. 2007; Rancourt et al. 2004; Naugler et al. 2000) and 92% were developed through extensive literature reviews and expert consensus methods, which implies both face and content validity. Common methodologies used to achieve consensus were the Delphi method, which uses consecutive rounds of anonymous consultation to achieve group consensus, and expert panels. Reliability was tested in seven of the indicator sets (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; NSW Therapeutic Assessment Group 2007; National Prescribing Service 2006; The American Geriatrics Society 2012; Hanlon et al. 1992; Naugler et al. 2000). Feasibility, usually in the form of piloting was undertaken for eight of the indicator sets (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Courtney et al. 2007; NSW Therapeutic Assessment Group 2007; National Prescribing Service 2006; The American Geriatrics Society 2012; Hanlon et al. 1992; O'Mahony et al. 2010; Naugler et al. 2000). Consumers were involved in the development process for seven of the indicator sets (Australian Institute of Health and Welfare 2009; Department of Health 2012; Campbell Research and Consulting (CR&C) 2006; Nay et al. 2004; Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; Primary Care & Social Care Information Centre 2013; National Prescribing Service 2006) five of which were Australian.
Many of the indicator sets have been further validated through application in research and reporting. Five indicators sets have been specifically assessed for their association (predictive validity) with health outcomes. These are the Beer’s criteria, Inappropriate Prescribing in the Elderly Tool (IPET), Medication Appropriateness Index (MAI), Drug Burden Index (DBI) and the Screening Tool of Older Person’s Prescriptions (STOPP) indicators. A review of Beer’s criteria, IPET and MAI found results ranging from a positive association with a higher risk of death, adverse drug reactions and health service utilisation to no association with mortality and hospital admissions (Spinewine et al. 2007). STOPP indicators have recently been significantly associated with preventable medication-related hospitalizations (Hamilton et al. 2011). No association between the DBI and mortality in older residential aged care residents has been reported (Wilson et al. 2012). Polypharmacy is used as an indicator of medication-related quality of care in several of the identified indicator sets and this has been associated with an increased risk of adverse events such as hospitalisation and death (Frazier 2005).
Concurrent validity has been examined for five indicator sets. A study compared the sensitivity and feasibility of the Beer’s criteria, IPET, Healthcare Effectiveness Data and Information Set (HEDIS) and the MAI and demonstrated an inverse relationship between ease of application (in terms of time and resources) and comprehensiveness (Luo et al. 2012). The MAI was found to be the most comprehensive and time consuming. HEDIS was reported as the simplest approach but less sensitive to detecting inappropriate prescribing (Luo et al. 2012). A study comparing the STOPP and Beer’s criteria found that the STOPP criteria were more sensitive to detecting potentially inappropriate medications and associated hospital admissions than Beer’s criteria (Hamilton et al. 2011).
In terms of external validity, the Beer’s criteria, STOPP/Screening Tool to Alert to Right Treatment (START) criteria, Assessing Care of Vulnerable Elders (ACOVE) indicators and MAI have been applied to many health care settings (often with minor adaptations) and in different countries with varying results (Gallagher et al. 2011; Askari et al. 2012; Hanlon & Schmader 2013). The Quality and Outcomes Framework indicators were applied to aged care residents (Fiona 2011) and found poor quality of care.
The three indicator sets which are routinely externally reported (Minimum Dataset (MDS), HEDIS and Quality and Outcomes Framework) are reviewed regularly for clinical validity and reliability (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; Primary Care & Social Care Information Centre 2013) and demonstrate feasibility on a large scale.
Relevance to medication-related quality of care needs for Australian residential aged care (minimum indicator set)
Presence of indicators which address one or more of the pre-determined six medication-related attributes is shown in Table 3, for each of the 25 indicator sets. Approximately half of the sets (n = 12) addressed medication use in the most prevalent chronic diseases (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Australian Institute of Health and Welfare 2009; Wegner et al. 2007; Primary Care & Social Care Information Centre 2013; NSW Therapeutic Assessment Group 2007; National Prescribing Service 2006; Mackinnon & Hepler 2002; Basger et al. 2008; The American Geriatrics Society 2012; O'Mahony et al. 2010; Onder et al. 2013; Naugler et al. 2000). Twenty four indicator sets addressed general medication appropriateness and eight addressed (directly or indirectly) detection of medication-related adverse events, namely falls (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Australian Institute of Health and Welfare 2009; Campbell Research and Consulting (CR&C) 2006; Courtney et al. 2007; Centres for Medicare and Medicaid Services & USA: www.cms.gov Accessed [February 2014; Wegner et al. 2007; NSW Therapeutic Assessment Group 2007; Mackinnon & Hepler 2002). Seven assessed medication-related services (National Committee for Quality Assurance & USA: www.ncqa.org Accessed [September 2013; Australian Institute of Health and Welfare 2009; Department of Health 2012; Courtney et al. 2007; Wegner et al. 2007; Primary Care & Social Care Information Centre 2013; National Prescribing Service 2006) and four addressed medication policy (Department of Health 2012; Wegner et al. 2007; Primary Care & Social Care Information Centre 2013; National Prescribing Service 2006). Two indicator sets (Assessing Care of Vulnerable Elders (ACOVE) and CRIteria to assess appropriate Medication use among Elderly complex patients (CRIME)) addressed review of medication with respect to limited life expectancy (O'Mahony et al. 2010; Onder et al. 2013).
Table 4 shows the selected indicators, derived from the mapping results in Table 3, to define a minimum indicator set for evaluating medication-related care in Australian residential aged care. In total 28 individual indicators were identified which address five of the six attributes. Twenty two of the 25 indicator sets are represented in the minimum dataset.
Discussion
In this study we identified 25 sets of medication-related quality of care indicators relevant to residential aged care. From these, 28 indicators that address key medication-related quality of care issues specific for residential aged care were selected to form the minimum indicator set. All 28 indictors have been previously validated for face and content validity through either extensive literature reviews and or expert consensus. Furthermore, external validity was demonstrated across countries for some of these indicators. Indicators for assessment of medication appropriateness, PQIs, were common among the identified indicators sets which demonstrated a strong international consensus on the appropriateness of these medications use in the elderly. Indicators for addressing the medication appropriateness for the most prevalent diseases, detecting and monitoring adverse drug events, access to relevant services and medication-related policy were identified in at least three of the included indicators sets. Indicators to address medication use in limited life expectancy in aged care residents are lacking.
Two of the identified indicator sets developed specifically for aged care take quite an extensive approach to medication management. ACOVE-3 contains nearly 400 indicators with one quarter of the indicators related to medication use (Wegner et al. 2007). This indicator set addresses prescribing, monitoring of medicines and consumer involvement in medication management. It has been extended to several subsets of indicators such as quality of care in dementia and poor prognosis. The Australian Guiding Principles for Medication Management in Residential Aged Care has a broad approach to evaluating medication use ranging from reviewing medicines policies and procedures to annual medication review but does not target specific medications (Department of Health 2012). Twelve of the indicators in our minimum indicator set are from ACOVE-3 and three are from the Australian Guiding Principles for Medication Management in Residential Aged Care. This demonstrates the relevance of these indicators for evaluating medication-related quality of care in Australian residential aged care. Whilst ACOVE-3 is a very comprehensive indicator set, it is burdensome for implementing in a clinical setting with 98 indicators relating to medication-related quality of care, many of which address clinical conditions not prevalent in the residential Australian aged care population. Currently quality of care indicator sets developed specifically for Australian residential aged care include simplistic medication-related quality of care indicators such as polypharmacy and medication review (Table 1). These two indicators are useful tools for identifying residents at risk of inappropriate medication-related quality of care and predicting adverse health outcomes however they do not reflect the complexity of medication-related care for the residential aged care population (Duerden et al. 2013). The minimum indicator set developed in this study provides a platform for a quality of care indicator set specific for Australian residential aged care that focuses on the key requirements to examine medication-related quality of care in this setting.
The overwhelming majority of medication-related quality of care indicator sets identified included exclusively PQIs. PQIs play an important role in evaluating medication-related quality of care. They are evidence based and specifically target medications known to cause adverse effects. Furthermore, the PQI sets developed for the older age groups address medicines most problematic in this population. PQI sets are often criticised due to their lack of sensitivity as they are designed to be generically applied across a population and do not consider variability in individual patient medical needs and preferences (Spinewine et al. 2007; Steinman et al. 2007). This however enhances the feasibility in reporting of these indicators. These qualities of PQIs are reflected by their prevalence in the minimum indicator set. Some PQI sets target medications to be avoided in certain comorbid states (e.g. Beer's criteria) and others (e.g. CRIME) addressed medication use in clinically complex frail elderly patients (Onder et al. 2013).
This review identified indicator sets which involved consumers in the development, however an indicator set with a more holistic approach to medication-management in the frail elderly with respect to prioritizing patient preferences and quality of life (patient-centred care) was not identified. The patient-centred care approach aligns with the current approach to delivering quality health care services in many countries, including Australia (Institute of Medicine. Committee on Quality of Health Care in America 2001; Australian Commission on Safety and Quality in Health Care 2010). Development of medication-related quality of care indicators with respect to patient-centred care warrants further consideration.
Collection and analysis of data for reporting quality of care indicators can be resource intensive. Experts in performance measurement in health care rate feasibility, scientific soundness and relevance as the three most desirable attributes for indicators (National Committe for Quality Assurance. (Desirable attributes of HEDIS). USA: www.ncqa.org/tabid/415/Default.aspx Accessed [March 2012). All of the indictors in the minimum indicator set are operational in that they are currently used in research and or quality of care reporting systems
Study limitations
The potential for bias in identification and selection of articles was limited by strictly adhering to predefined inclusion and exclusion criteria and group consensus on differences. The PRISMA guidelines were used in both the study methodology and reporting of the results however, we cannot rule out that relevant studies or reports have been missed. We also used the CASP criteria to ensure that all included articles were of a minimum quality. Two authors (AV and GC) were deemed suitable to oversee and contribute to all steps of this study as they are experienced in undertaking and publishing systematic reviews (Spurling et al. 2010; Caughey et al. 2008).
We also chose a systematic approach to the data extraction using predefined criteria to minimise bias in reporting of the qualities of each identified indicator set. Content analysis methodology has been criticised for being too reductive and consequently we may have missed identifying important indicator qualities (Dixon-Woods et al. 2005).
Every effort was made to correctly designate operational status to each indicator set. However, many of the indicator sets are intended for internal quality monitoring and reporting and it is possible that some of the indicators are reported in house or are operational through incorporation into other datasets.
Only five of the indicators sets identified have been formally assessed for predictive validity (with varying results). Further research should focus on investigating the relationships between our developed minimum indicator set and health outcomes.
Whilst the identified indicators in our minimum indicator set have content and face validity for medication-related quality of care in the elderly, many are yet to be validated for the Australian aged care setting. Indicators for assessing access to medication-related health services were not common and may reflect the differences in health systems between countries. Indicators addressing medication-related health services specific to residential aged care residents in Australia, would need to be further investigated for inclusion in the minimum indicator set. Subsequent development and validation of the minimum indicator set should be the focus of future research.
Conclusion
In this study we have derived a minimum indicator set for evaluating medication-related quality of care in residential aged care using systematically identified and previously validated indicators based on the key medication-related needs of the aged care population. The developed minimum indicator set is intended as a starting point for comprehensively evaluating medication-related quality of care in Australian aged care. This study identified that indicators focusing on pertinent medication-related issues for older aged care residents, namely patient-centred care and limited life expectancy, were lacking and warrant further attention. Also, inclusion of additional indicators which address detection and monitoring of adverse events, not just falls, as these were not overly prevalent in the indicator sets. The focus on the core medication-related attributes in the minimum indicator set improves the feasibility of implementation in the aged care setting by minimising data collection and management. Validation of the minimum indicator set in the Australian aged care setting will provide a means to assess and monitor quality of care in this growing health sector.
References
Australian Institute of Health and Welfare (2012) Residential aged care in Australia 2010–11: a statistical overview. Age care statistics series no. 36. Cat. no. AGE 68. AIHW, Canberra
Arah OA, Westert GP, Hurst J, Klazinga NS (2006) A conceptual framework for the OECD Health Care Quality Indicators Project. Int J Qual Health Care 18(Suppl 1):5–13
Askari M, Wierenga PC, Eslam S, Medlock S, De Rooij SE, Abu-Hanna A (2012) Studies pertaining to the ACOVE quality criteria: asystematic review. Int J Qual Health Care 24(1):80–97
Australian Commission on Safety and Quality in Health Care (2010) Patient-centred care: Improving quality and safety by focussing care on patients and consumers. Discussion paper, Sydney
Australian Institute of Health and Welfare (2009) Towards national indicators of safety and quality in health care. AIHW, Canberra
Australian Institute of Health and Welfare (2010) Residential aged care in Australia 2008–09: a statistical overview. In: Aged care statistics series Cat no AGE 62. AIHW, Canberra
Barry PJ, Gallagher P, Ryan C, O'Mahony D (2007) START (screening tool to alert doctors to the rights treatment) - an evidence-based screening tool to detect prescriging omissions in elderly patients. Age and Ageing 36:632–8
Basger BJ, Chen TF, Moles RJ (2008) Inappropriate Medication Use and Prescribing Indicators in Elderly Australians. Development of a Prescribing Indicators Tool. Drugs Ageing 25(9):777–93
Bootman JL, Harrison DL, Cox E (1997) The Health Care Cost of Drug-Related Morbidity and Mortality in Nursing Facilities. Arch Intern Med 157(18):2089–96
Britt HC, Harrison CM, Miller GC (2008) Prevalence and patterns of multimorbidity in Australia. Med J Aust 189:72–7
Burchett H, Umoquit M, Dobrow M (2011) How do we know when research from one setting can be useful in another? A review of external validity, applicability and transferability frameworks. J Health Serv Res Policy 16(4):238–44
Campbell Research and Consulting (CR&C) (2006) Developing resident-centred quality indicators in residential aged care. Commonwealth of Australia, Canberra
Caughey GE, Vitry AI, Gilbert AL, Roughead EE (2008) Prevalence of comorbidty of chronic disease in Australia. BMC Public Health. 8(221). www.biomedcentral.com/1471-2458/8/221/ doi:10.1186/1471-2458-8-221
Centres for Medicare and Medicaid Services., USA: www.cms.gov Accessed [February 2014].
Chang CB, Chan DC (2010) Comparison of published explicit criteria for potentially inappropriate medications in older adults. Drugs Ageing 27(12):947–57
Commonwealth of Australia (2010) Australia to 2050: future challenges. The 2010 Intergenerational report. Canberra
Courtney M, O'Reilly MT, Edwards H, Hassall S (2007) Development of a systematic approach to assessing quality within Australian residential aged care facilities: the Clinical Care Indicators Tool. Aust Health Rev 31(4):582–91
Courtney M, O'Reilly MT, Edwards H, Hassall S (2010) Benchmarking clinical indicators of quality for Australian residential aged care facilities. Aust Health Rev 34:93–100
Courtney M, O'Reilly M, Edwards H, Hassall S (2011) Content validity of the resCareQA: An Australian resdiential care quality assessment based on residential outcomes. J Adv Nurs 28(3):37–46
Critical Appraisal Skills Programme, United Kingdom: www.casp-uk.net Accessed [September 2011].
Department of Health (2012) Guiding Principles for Medication Management in Residential Aged Care. Commonwealth of Australia, Canberra
Department of Health and Ageing (1999) National Medicines Policy. Australian Government, Canberra
Dixon-Woods M, Agarwal S, Jones D, Young B, Sutton A (2005) Synthesising qualitative and quantitative evidence: a review of possible methods. J Health Serv Res Pol 10(1):45–53
Donabedian A (1966) Evaluating the Quality of Medical Care. Milbank Q 83(4):697–729
Donabedian A (1980) Explorations in Quality Assessment and Monitoring (Volume 1). The definition of quality and approaches to its assessment, 1st edn. Health Administration Press, Michigan
Donabedian A (1988) The Quality of Care. How can it be assessed? JAMA 260(12):1743–8
Duerden M, Avery T, Payne R (2013) Polypharmacy and medicines optimisation. Making it safe and sound. The Kings Fund, London
Fiona C (2011) Judging quality of care in older people in care homes. BMJ 341:d912
Frazier SC (2005) Health Outcomes and Polypharmacy in Elderly Individuals. J Gerontol Nurs 31(9):4–11
Gallagher P, O'Mahony D (2008) STOPP (Screening Tool of Older Persons’ potentially inappropriate Prescriptions): application to acutely ill elderly patients and comparison with Beers’ criteria. Age Ageing 37:673–9
Gallagher P, Lang PO, Cherubini A, Topinková E, Cruz-Jentoft A, Montero Errasquín B, Madlova P, Gasperini B, Baeyens JP, Michel JP, O’Mahony D (2011) Prevalence of potentially inappropriate prescribing in an acutely ill population of older patients admitted to six European hospitals. Eur J Clin Pharmacol 67:1175–88
Gilbert AL, Roughead EE, Beilby J, Mott K, Barratt JD (2002) Collaborative medication management services: improving patient care. Med J Aust 177:189–92
Gilbert AL, Caughey GE, Vitry AI, Clark A, Ryan P, McDermott RA, Sepehr S, Luszcz MA, Esterman A, Roughead EE (2011) Ageing well: Improving the management of patients with multiple chronic health problems. Australas J Ageing 30(2):32–7
Hamilton H, Gallagher P, Ryan C, Byrne S, O'Mahony D (2011) Potentially Inappropriate Medications Defined by STOPP criteria and the Risk of Adverse Drug Events in Older Hospitalised Patients. Arch Intern Med 171(11):1013–9
Hanlon JT, Schmader KE (2013) The Medication Appropriateness Index at 20: Where it Started, Where It Has Been, and Where It May Be Going. Drugs Ageing 30:893–900
Hanlon JT, Schmader KE, Samsa GP, Weinberger M, Uttech KM, Lewis IK, Cohen HJ, Feussner JR (1992) A method for assessing drug therapy appropriateness. J Clin Epidemiol 45(10):1045–51
Hannes K (2011). Chapter 4. Critical appraisal of qualitative research. In Supplementary Guidance for Inclusion of Qualitative Research in Cochrane Systematic Reviews of Interventions Version 1 (updated August 2011). Noyes J, Booth A, et al., (eds) Cochrane Collaboration Qualitative Methods Group 2011. Available from URL http://cqrmg.cochrane.org/supplemental-handbook-guidance
Hawes C, Morris JN, Phillips CD, Fries BE, Murphy K, Mor V (1997) Development of the nursing home Resident Assessment Instrument in the USA. Age Ageing 26-S2:19–25
Hilmer SN, Mager DE, Simonsick EM, Cao Y, Ling SM, Windham BG, Harris TB, Hanlon JT, Rubin SM, Shorr RI, Bauer DC, Abernethy DR (2007) A Drug Burden Index to define the Functional Burden of Medications in Older People. Arch Intern Med 167:781–7
Holmes HM, Min LC, Yee M, Varadhan R, Basran J, Dale W, Boyd CM (2013) Rationalising Prescribing for Older Patients with Multimorbidity: Considering Time to Benefit. Drugs Ageing 30:655–66
Holt S, Schmiedl S, Thürmann PA (2010) Potentially Inappropriate Medications in the Elderly: The PRISCUS List. Dtsch Arztebl Int 107(31):543–51
Howden L, Meyer J (2011) Age and Sex Compostition: 2010. U.S. Department of Commerce, Washington, DC
Huisman-Baron M, Veen L, Jansen PA, Roon EN, Brouwers JR, Marum RJ (2011) Criteria for Drug Selection in Frail Elderly Persons. Drugs Ageing 28(5):391–402
Institute of Medicine. Committee on Quality of Health Care in America (2001) Crossing the quality chasm: a new health system for the 21st century. National Academy Press, Washington, DC
Clark JP, Bierman AS (2009) The POWER Study Framework. In: Bierman AS (ed) Project for and Ontario Women’s Health Evidence-Based Report. Institute for Clinical and Evaluative Sciences, Toronto
Laroche ML, Charmes JP, Merle L (2007) Potentially inappropriate medications in the elderly: a french consensus panel list. Eur J Clin Pharmacol 63:725–31
Lund BC, Steinman MA, Chrischilles EA, Kaboli PJ (2011) Beers Criteria as a proxy for Inappropriate Prescribing of Other Medications Among Older Adults. Ann Pharmacother 45:1363–70
Luo R, Scullin C, Mullan AM, Scott MG, McElnay JC (2012) Comparison of tools for the assessment of inappropriate prescribing in hospitalised older people. J Eval Clin Pract 18(6):1196–202
Mackinnon NJ, Hepler CD (2002) Preventable Drug-related Morbidity in Older Adults (Part 1). J Manag Care Pharm 8(5):365–71
Mainz J (2003) Defining and classifying clinical indicators for quality improvements. Int J Qual Health Care 15(6):523–30
Marcum ZA, Hanlon JT (2012) Commentary on the New American Geriatric Society Beers Criteria for Potenially Inappropraite Medication use in Olders Adults. Am J Geriatric Pharmacother 10(2):151–9
Marengoni A (2013) Guidelines for elderly patients with multimorbidity: how to cope with a dark night without fear. Aging Clin Exp Res 25:703–5
Martirosyan L, Voorham J, Haaijer-Ruskamp FM, Braspenning J, Wolffenbuttel BH, Denig P (2010) A systematic literature review: prescribing indicators related to type 2 diabetes mellitus and cardiovascular risk. Pharmacoepidemiol Drug Saf 19:319–34
McLeod PJ, Huang AR, Tamblyn RM, Gayton DC (1997) Defining inappropriate practices in prescribing for elderly perople. A national consensus panel. CMAJ 156:385–91
Milton JC, Hill-Smith I, Jackson SHD (2008) Prescribing for older people. BMJ 336(7644):606–9
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group (2009) Preferred reporting items for Systematic reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7):e1000097. doi:10.1371/journal.pmed.1000097
Morris CJ, Cantrill JA, Hepler CD, Noyce PR (2002) Preventing drug-related morbidity - determining valid indicators. Int J Qual Health Care 14(3):183–98
National Aged Care Alliance (2014) Aged Care Reform Series-Quality of Care. National Aged Care Alliance, Australia
National Committe for Quality Assurance. (Desirable attributes of HEDIS). USA: www.ncqa.org/tabid/415/Default.aspx Accessed [March 2012]
National Committee for Quality Assurance, USA: www.ncqa.org Accessed [September 2013].
National Institute for Health and Care Excellence (2014a) Indicators Process Guide. NICE, Manchester
National Institute for Health and Care Excellence (2014b) Managing medicines in care homes. NICE, United Kingdom
National Prescribing Service (2006) Indicators of Quality Prescribing in Australian General Practice. A manual for users, NPS, Surrey Hills
Naugler CT, Brymer C, Stolee P, Arcese ZA (2000) Development and Validation of an Improving Prescribing in the Elderly Tool. Can J Clin Pharmacol 7(2):103–7
Nay R, Thomas S, Koch S, Wilson J, Garratt S, Fox A, Koch B (2004) Public Sector Residential Aged Care Quality of Care Performance Indicator Project Report. LaTrobe University, Gerontic Nursing Clinical School, Melbourne
NSW Therapeutic Assessment Group (2007) Indicators for Quality Use of Medicines in Australian Hospitals. NSW Therapeutic Advisory Group Inc, Sydney
Office for National Statistics (2011) Statistical Bulletin: Older People’s Day 2011. Newport. Available at www.ons.gov.uk/ons/rel/mortality-ageing/focus-on-older-people/older-people-s-day-2011/stb-opd-2011.html
O'Mahony D, Gallagher P, Ryan C, Byrne S, Hamilton H, Barry P, O’Connor M, Kennedy J (2010) STOPP & START criteria: A new approach to detecting potentially inappropriate prescribing in old age. Eur Geriatr Med 1:45–51
Onder G, Landi F, Fusco D, Corsonello A, Tosato M, Battaglia M et al (2013) Recommendations to Prescribe in Complex Older Adults: Results of the CRIteria to Assess Appropriate Medication Use Among Elderly Complex Patients (CRIME) Project. Drugs Ageing 31:33–45
Prescribing and Primary Care, Health and Social Care Information Centre (2013) Quality and Outcomes Framework. Achievement, prevalence and exceptions data, 2012/13. Technical Annex.
Productivity Commission. (2011). Caring for Older Australians: Overview, Report no. 53, Final Inquiry Report. Canberra.
Rancourt C, Moisan J, Baillargeon L, Verreault R, Laurin D, Gregoire JP (2004) Potentially inappropriate prescriptions for older patients in long-term care. BMC Geriatrics, 4(9). www.biomedcentral.com/1471-2318/4/9
Robertson HA, MacKinnon NJ (2002) Development of a List of Consensus-Approved Clinical Indicators of preventable Drug-related Morbidity in Older Adults. Clin Therapeut 24(10):1595–613
Rognstad S, Brekke M, Fetveit A, Spigset O, Wyller TB, Straand J (2009) The Norwegian general Practice (NORGEP) criteria for assessing potentially inappropriate prescriptions to elderly patients. Scand J Prim Health Care 27:153–9
Roughead EE, Gilbert AL, Woodward MC (2008) Medication Use by Australian War Veterans in Residential Aged-Care Facilities. J Pharm Pract 38(1):14–8
Somers M, Simmonds D, Whitelaw C, Calver J, Beer C (2010) Quality use of medicines in residential aged care. Aust Fam Physician 39(6):413–6
Spinewine A, Schmader KE, Barber N, Hughes C, Lapane KL, Swine C, Hanlon JT (2007) Appropriate prescribing in elderly people: how well can it be measured and optimised? Lancet 370(9582):173–84
Spurling G, Mansfiled P, Montgomery B, Lexchin J, Doust J, Othman N, et al. (2010) Information from pharmaceutical companies and the quality, quantity and cost of physicians’ prescribing: a systematic review. PLoS Medicine. 7(10). http:/journals.plos.org/plosmedicine/article?id10.1371/journal.pmed.1000352
Steinman MA, Rosenthal GE, Landefeld CS, Bertenthal D, Sen S, Kaboli PJ (2007) Conflicts and Concordance Between Measures of Medication Prescribing Quality. Med Care 45(1):95–9
The American Geriatrics Society (2012) Beers Criteria Update Expert Panel (2012) American Geriatrics Society Updated Beers Criteria for Potentially Inappropraite Medication Use in Older Adults. JAGS 60(4):616–631
The SENATOR Project, Europe: www.senator-project.eu Accessed [February 2014].
Tinetti ME, Bogardus ST, Agostini JV (2004) Potential Pitfalls of Disease-Specific Guidelines for Patients with Multiple Conditions. NEJM 351(27):2870–4
Tinetti ME, Fried TR, Boyd CM (2012) Designing Health Care for the Most Common Chronic Condition - Multimorbidity. JAMA 307(23):2493–4
Wegner NS, Roth CP, Shekelle P, ACOVE Investigators (2007) Introduction to the Assessing Care of Vulnerable Elders-3 Quality Indicator Measurement Set. JAGS 55:S247–S52, & S464-S87
Wilson NM, March LM, Sambrook PN, Hilmer SN (2010) Medication safety in residential aged-care facilities: a perspective. Ther Adv Drug Saf 1(1):11–20
Wilson NM, Hilmer SN, March LN, Cameron ID, Lord SR, Seibel MJ, Mason RS, Chen JS, Cumming AG, Sambrook PN (2011) Associations between Drug Burden Index and Falls in Older people in Residential Aged Care. JAGS 59:875–80
Wilson NM, Hilmer SN, March LN, Chen JS, Gnjidic D, Mason RS, Cameron ID, Sambrook PN (2012) Associations between Drug Burden Index and Mortality in Older people in Residential Aged Care Facilities. Drugs Ageing 29(2):157–65
Winit-Watjana W, Sakulrat P, Kespichayawattana J (2008) Criteria for high-risk medication use in Thai older people. Arch Gerontol Geriatr 47:35–51
Zimmerman DR, Karon SL, Arling G, Clark BR, Collins T, Ross R, Sainfort F (1995) Development and Testing of Nursing Home Quality Indicators. Health Care Financing Rev 16(4):107–27
Acknowledgements
This study was undertaken with support from a University of South Australia postgraduate scholarship.
This manuscript does not contain clinical studies or patient data.
This study was approved by the University of South Australia Human Research Ethics Committee in March 2012 (protocol number 27439).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Author’s contributions
JH, AV and GC all contributed to the study design and methodology. JH undertook the primary literature search, data extraction and synthesis. AV and GC reviewed the results from the literature search, data extraction and synthesis. JH prepared the initial manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Hillen, J.B., Vitry, A. & Caughey, G.E. Evaluating medication-related quality of care in residential aged care: a systematic review. SpringerPlus 4, 220 (2015). https://doi.org/10.1186/s40064-015-0984-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40064-015-0984-9