
Abstract
Objectives
Fournier’s gangrene (FG) is an devastating disease that affects the perineum and genitourinary region, and is commonly a result of poly-microbial infection. This study is aimed to determine the correlation between micrology and prognosis of FG in the past five years.
Methods
This study was a retrospective cohort study that was designed to study the trends in micrology and prognosis of FG. From the PubMed database, articles published in the recent 5 years (from Jan1st, 2009 to Dec 31st, 2013) were reviewed. A total of 19 articles (each with n > 30 and with thorough data descriptions in the topic of Fournier's gangrene), were enrolled in this study. The consolidated data was further analyzed by commercial statistical software (SPSS for Windows).
Results
The twenty-two studies have covered FG cases from year 1981 to 2011, with a mean duration of 9.2 years. The total number of cases is 4,365. Majority of the cases are male (84.1%). The mean age and mortality rate is 51.8 ± 5 years old and 11.1 ± 8.9%, respectivly. The most commonly found pathogen is poly-microbial organism (54%), followed by Escherichia coli (46.6%) and Streptococcus (36.8%). The major risk factors are diabetes (43.7%), Body mass index of > 30 (40.7%), and hypertension (38.1%). Mortality rate in older patient group (age > 51.8 years old) is significantly higher than those of the younger group (22% vs. 5.5%, p = 0.0001).
Conclusions
Older patients with genital or perineal pain should be examined for crepitus dermis. When a patient is diagnosed with FG, swift consultation with surgeons and administration of broad-spectrum antibiotics are required in order to save the patient’s live.
Similar content being viewed by others

Background
Fournier’s gangrene (FG) is a devastating necrotising disease that affects the perineum and genitourinary regions. The common cause of FG is poly-microbial infections, where the diabetes mellitus is an attributing common risk factor (Shyam and Rapsang [2013]). Study has shown that males, especially in their 60 to 70s, are more often affected by FG when compared to other populations (Rodríguez Alonso et al. [2000]). Aside from diabetes, other risk factors of FG also include chronic alcoholism, renal failure, and obesity (Montoya Chinchilla et al. [2009]). The majorities of FG studies have shown that early diagnosis and aggressive management of FG are required to significantly improve patient outcome. Due to the fact that FG is not a common disease, a prospective study is difficult to perform. Therefore, In this study, a large number of FG cases that have occurred in the past five years are gathered by retrospective literature review and analyzed to determined the relationship between micrology and prognosis of FG.
Methods
A retrospective cohort study was designed to investigate the correlation between micrology and prognosis of FG. A search from the PubMed database returned a total of 1,015 literatures that contain the keyword “Fournier’s gangrene”. The resulting literatures were further limited to the literature s that were published within the past 5 years, (from Jan.1, 2009 to Dec 31, 2013), where a total of 330 articles remained. The articles that contain case numbers of less than 30 were excluded from the study, since the low sample number cannot establish a normal distribution for the evaluation of statistical significance. In the end, there were 19 articles that was enrolled into this study. The combined data and descriptions of Fournier’s gangrene are listed in Table. 1 References (Martinschek et al. [2012]) to (Ersoz et al. [2012]). These enrolled research literatures are from Germany (n = 4, 21%), Turkey (n = 4), United States of America (n = 2), Pakistan (n = 2), Spain (n = 2), Mexico (n = 1), Brazil (n = 1), Taiwan (n = 1), Tunisia (n = 1) and Croatia (n = 1). The data was analyzed with a commercial statistical software (SPSS for Windows, version 11.0, SPSS Ltd., Chicago, IL). Statistical χ2 tests were performed and the significance was set at a p value of less than 0.05 (2-tailed).
Results
The twenty-two studies have covered FG cases from year 1981 to 2011, with a mean duration of 9.2 years. The total number of cases is 2,656. Majority of cases are male (84.1%) and female is accounted for 15.9%.
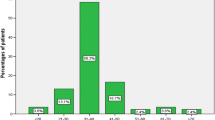
The mean age of the patients is 51.8 years old, and the average mortality rate is 11.1 ± 8.9%. When comparing between the older age group (age > 51.8 years old) and the younger group (age of less or equal to 51.8), the mortality rate was found to be higher in the older group than younger (22 ± 8.8% versus 5.5 ± 2%, p = 0.0001) The most commonly found pathogen is poly-microbial organism (54%), followed by Escherichia coli (46.6%) and Streptococcus (36.8%). The other contributing pathogens also include Bacteroides, Enterbacter, Staphylococcus, Enterococcus, Pseudomonas, Corynebacterium, and Klebsiella pneumoniae (Figure 1).

List of commonly found pathogens involving Fournier’ s gangrene (presented in percentages).
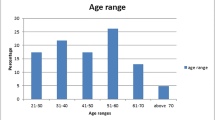
The major risk factors for FG are diabetes (43.7%), body mass index of higher than 30 (40.7%), and hypertension (38.1%). Other risk factors also include heart disease (38%), alcoholism (31.4%), smoking (22.5%), renal failure (13.8%), urethral operation history, neurogenic bladder, and corticosteroid user (Figure 2).

List of commonly found risk factors involving Fournier’ s gangrene (presented in percentages).
Discussion
Fournier’s gangrene (FG) is a rare emergent condition that affects the perineum and urogenital region. The clinical course of FG is fulminant and serious regardless of parenteral antibiotic treatment. The median time from syptom presentations to skin gangrenous change is 6 days (Altarac et al. [2012]). When managing FG patients, this gangrenous tissue requires extensive and repeated debridement (Sallami et al. [2012]). Several literatures have shown that patients with diabetes, old age, low blood pressure, high creatine kinase, high lactate, abdominal affection, hemoglobin of less than 10 g/dL, and platelet count of less than 150 × 109/L are associated with poor outcomes (Martinschek et al. [2012]; Ruiz-Tovar et al. [2012]).
Many literatures have determined that the risk factors of FG include diabetes mellitus, hypertension, heart disease, smoking, long-term steroid therapy, alcoholism or alcohol abuse, in hot and humid season, and renal failure (Martinschek et al. [2012]; Sallami et al. [2012]; Czymek et al. [2010]; Mehl et al. [2010]; Malik et al. [2010]; Ullah and Khan [2009]). Out of the many risk factors, diabetes mellitus is still the highest influencing factor on FG where 43.7% of FG patients are diabetic. A report by Czymek et. al. showed that being overweight is also a risk factor of FG, where nearly 40 % of FG patients have body mass indexes (BMIs) of higher than 30 (Czymek et al. [2010]; Mehl et al. [2010]). Although there are several known risk factors that can lead to the development of FG, the clinical onset of FG is still unpredictable.
The most common symptoms of FG are perineal pain and fever that are accompanied by swelling and reddening of perineum or genital area, and the gangreneous change of overlaying skin (Ruiz-Tovar et al. [2012]).
The most common microbiology involved in FG is poly-microbial infection (54%), and the most common found pathogen isolate is Escherichia coli (46.6%). Others contributing pathogen are Streptococcal infection, Bacteroides, Enterobacter, Staphylococcus, Enterococcus, Pseudomonas, Corynebacterium, and Klebsiella pneumoniae (Rodríguez Alonso et al. [2000]; Czymek et al. [2010]; Mehl et al. [2010]). Broad-spectrum antibiotic treatment is suggested to adequately cover poly-microbial pathogen, and careful patient monitoring is required to avoid is fungal or hospital-acquired pathogen infection (Bjurlin et al. [2013]).
In terms of gender, there was no significant mortality rate that was found between the genders (Ersoz et al. [2012]). A study from Spain (n = 51) showed that the survivors of FG are 13.5 years younger than those who have died (60 versus 73.5, p = 0.02) (Luján Marco et al. [2010]). In a 2012 report from Turkey ( n = 52), the non-survivors group are older in age than survivors (62 versus 55 years old]. In our study, the results also showed that the older patients age had higher rates of mortality. This result is concurrent with in the other previous studies, where increased age was shown to be related to higher mortality rate (Martinschek et al. [2012]; Roghmann et al. [2012]).
Although FG is rare, its rapid progression can lead to life-threatening conditions that require early surgical intervention and parenteral antibiotics to improve patient outcomes (Morua et al. [2009]). The mortality rate of FG remains high and ranges from 4.9 to 36.6% in the recent five years. Due to its high mortality rate and rapid progress, FG must be regarded in clinical settings. The reduction of obesity, alcohol consumption, tobacco use is helpful in reducing the possible risk of FG. Furthermore, older patients with genital or perineal pain should be examined for crepitus dermis. Finally, when a patient is diagnosed with FG, swift consultation with surgeons and administration of broad-spectrum antibiotics are required in order to save the patient’s live.
Authors’ information
Dr. Lap-Ming Tang and Dr. Yu-Jang Su are senior attending physicians worked at Department of Emergency Medicine, Mackay Memorial Hospital, Taipei 10449, Taiwan. Dr. Yu-Jang Su is also awarded six times of best teacher of Mackay Memorial Hospital, Taipei till 2014, and teaches at department of Oral Hygiene, College of Oral Medicine, Taipei Medical University, Taipei, Taiwan as an Assistant Professor. Dr. Yen-Chun Lai is a professional anesthesiologist working at Department of Anesthesiology, Taiwan Adventist Hospital, Taipei, Taiwan. We all have copious clinical experiences in practice.
References
Altarac S, Katušin D, Crnica S, Papeš D, Rajković Z, Arslani N: Fournier’s gangrene: etiology and outcome analysis of 41 patients. Urol Int 2012, 88(3):289-293. 10.1159/000335507
Bjurlin MA, O’Grady T, Kim DY, Divakaruni N, Drago A, Blumetti J, Hollowell CM: Causative pathogens, antibiotic sensitivity, resistance patterns, and severity in a contemporary series of Fournier’s gangrene. Urology 2013, 81(4):752-758. 10.1016/j.urology.2012.12.041
Chen SY, Fu JP, Chen TM, Chen SG: Reconstruction of scrotal and perineal defects in Fournier’s gangrene. J Plast Reconstr Aesthet Surg 2011, 64(4):528-534. 10.1016/j.bjps.2010.07.018
Czymek R, Frank P, Limmer S, Schmidt A, Jungbluth T, Roblick U, Bürk C, Bruch HP, Kujath P: Fournier’s gangrene: is the female gender a risk factor? Langenbecks. Arch Surg 2010, 395(2):173-180. 10.1007/s00423-008-0461-9
Ersoz F, Sari S, Arikan S, Altiok M, Bektas H, Adas G, Poyraz B, Ozcan O: Factors affecting mortality in Fournier’s gangrene: experience with fifty-two patients. Singapore Med J 2012, 53(8):537-540.
Göktaş C, Yıldırım M, Horuz R, Faydacı G, Akça O, Cetinel CA: Factors affecting the number of debridements in Fournier’s gangrene: our results in 36 cases. Ulus Travma Acil Cerrahi Derg 2012, 18(1):43-48. 10.5505/tjtes.2012.36599
Koukouras D, Kallidonis P, Panagopoulos C, Al-Aown A, Athanasopoulos A, Rigopoulos C, Fokaefs E, Stolzenburg JU, Perimenis P, Liatsikos E: Fournier’s gangrene, a urologic and surgical emergency: presentation of a multi-institutional experience with 45 cases. Urol Int 2011, 86(2):167-172. 10.1159/000321691
Luján Marco S, Budía A, Di Capua C, Broseta E, Jiménez CF: Evaluation of a severity score to predict the prognosis of Fournier’s gangrene. BJU Int 2010, 106(3):373-376. 10.1111/j.1464-410X.2009.09075.x
Malik AM, Sheikh S, Pathan R, Khan A, Sheikh U: The spectrum of presentation and management of Fournier’s gangrene–an experience of 73 cases. J Pak Med Assoc 2010, 60(8):617-619.
Martinschek A, Evers B, Lampl L, Gerngroß H, Schmidt R, Sparwasser C: Prognostic aspects, survival rate, and predisposing risk factors in patients with Fournier’s gangrene and necrotizing soft tissue infections: evaluation of clinical outcome of 55 patients. Urol Int 2012, 89(2):173-179. 10.1159/000339161
Mehl AA, Nogueira Filho DC, Mantovani LM, Grippa MM, Berger R, Krauss D, Ribas D: Management of Fournier’s gangrene: experience of a university hospital of Curitiba. Rev Col Bras Cir 2010, 37(6):435-441.
Montoya Chinchilla R, Izquierdo Morejon E, Nicolae Pietricicâ B, Pellicer Franco E, Aguayo Albasini JL, Miñana LB: Fournier’s gangrene. Descriptive analysis of 20 cases and literature review. Actas Urol Esp 2009, 33(8):873-880. 10.1016/S0210-4806(09)72875-X
Morua AG, Lopez JA, Garcia JD, Montelongo RM, Guerra LS: Fournier’s gangrene: our experience in 5 years, bibliographic review and assessment of the Fournier’s gangrene severity index. Arch Esp Urol 2009, 62(7):532-540.
Ozturk E, Sonmez Y, Yilmazlar T: What are the indications for a stoma in Fournier’s gangrene? Colorectal Dis 2011, 13(9):1044-1047. 10.1111/j.1463-1318.2010.02353.x
Rodríguez Alonso A, Pérez García MD, Núñez López A, Ojea Calvo A, Alonso Rodrigo A, Rodríguez Iglesias B, Barros Rodríguez JM, Benavente Delgado J, Nogueira March JL: Fournier’s gangrene: anatomo-clinical features in adults and children. Therapy update Actas Urol Esp 2000, 24(4):294-306. 10.1016/S0210-4806(00)72452-1
Roghmann F, von Bodman C, Löppenberg B, Hinkel A, Palisaar J, Noldus J: Is there a need for the Fournier’s gangrene severity index? Comparison of scoring systems for outcome prediction in patients with Fournier’s gangrene. BJU Int 2012, 110(9):1359-1365. 10.1111/j.1464-410X.2012.11082.x
Ruiz-Tovar J, Córdoba L, Devesa JM: Prognostic factors in Fournier gangrene. Asian J Surg 2012, 35(1):37-41. 10.1016/j.asjsur.2012.04.006
Sallami S, Maalla R, Gammoudi A, Ben Jdidia G, Tarhouni L, Horchani A: Fournier’s gangrene: what are the prognostic factors? Our experience with 40 patients. Tunis Med 2012, 90(10):708-714.
Shyam DC, Rapsang AG: Fournier’s gangrene. Surgeon 2013, 11(4):222-232. 10.1016/j.surge.2013.02.001
Sorensen MD, Krieger JN, Rivara FP, Broghammer JA, Klein MB, Mack CD, Wessells H: Fournier’s Gangrene: population based epidemiology and outcomes. J Urol 2009, 181(5):2120-2126. 10.1016/j.juro.2009.01.034
Ullah S, Khan M, Asad Ullah Jan M: Fournier’s gangrene: a dreadful disease. Surgeon 2009, 7(3):138-142. 10.1016/S1479-666X(09)80036-X
Vargas AH, Carbonell J, Osorio D, García HA: Evaluation of Fournier’s necrosis in a high complexity hospital. Arch Esp Urol 2011, 64(10):948-952.
Yilmazlar T, Ozturk E, Ozguc H, Ercan I, Vuruskan H, Oktay B: Fournier’s gangrene: an analysis of 80 patients and a novel scoring system. Tech Coloproctol 2010, 14(3):217-223. 10.1007/s10151-010-0592-1
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that there is no conflict of interests.
Authors’ contribution
Tang LM: Study Design and Draft writing. Su YJ: Statistical analysis, management and revision. Lai YC: Discussion. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made.
The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
To view a copy of this licence, visit https://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
Cite this article
Tang, LM., Su, YJ. & Lai, YC. The evaluation of microbiology and prognosis of fournier’s gangrene in past five years. SpringerPlus 4, 14 (2015). https://doi.org/10.1186/s40064-014-0783-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40064-014-0783-8