
Abstract
Purpose
During the last few decades, the increased use of various types of antibiotics in the general population caused a significant change in regional Helicobacter pylori (H. pylori) antibiotic resistance. Our aim is to study the changes in H. pylori resistance in patients who had undergone an esophagogastroduodenoscopy (EGD) and susceptibility testing and found positive for H. pylori. The study was conducted in a university affiliated hospital between 2013–2020.
Methods
A cross-sectional study was performed on all consecutive patients who had undergone an EGD and tested positive for H. pylori at the Kaplan Medical Center, Israel. The study period was divided into two sub-periods: 2013–2016 and 2017–2020. Data on age, sex, comorbidities, previous treatments, and antimicrobial susceptibility testing for six antimicrobial agents were compared.
Results
The resistance rates of H. pylori to clarithromycin and dual resistance to clarithromycin and metronidazole were found significantly higher during the late period. Multivariable analysis showed that the later period, older age, and diabetes mellitus were independent predictors for antimicrobial resistance.
Conclusions
Our study has shown that there is an increasing resistance of H. pylori to clarithromycin and metronidazole while its susceptibility is unaffected with time to other antibiotics. More recent cross-sectional studies with larger samples are warranted in order to evaluate the changes in the resistance patterns of H. pylori to various antibiotics with time.
Similar content being viewed by others


Introduction
Helicobacter pylori (H. pylori) infection has been linked to peptic ulcer disease and gastric cancer [1]. The seroprevalence of H. pylori in Israel is ~ 45%; the annual incidence of gastric cancer is ~ 9/100,000 people [2, 3]. The first line of H. pylori treatment in Israel includes a proton pump inhibitor (PPI), amoxicillin (AMP), clarithromycin (CLR) and/or metronidazole (MET); the second line comprises PPI, and bismuth quadruple therapy, including tetracycline (TET) and MET. Triple therapy comprises PPI, AMP and levofloxacin (LEV) or rifabutin (RIF) which is used as a rescue therapy. Resistance prevalence varies by country and within the same region. Possible causes of treatment failure are the increased use of different antibiotics prescribed for adults and children for dental work, and respiratory, gynecological, and parasitic infectious diseases. Primary resistance can significantly impair the efficacy of eradication regimens, especially the inclusion of macrolides (i.e., clarithromycin) [4]. High secondary resistance to metronidazole or clarithromycin is expected after treatment failure with therapeutic combinations containing one of these compounds [5]. Since multi-resistance frequently develops against most implemented antibiotics thus, leading to increased inadequate success rates, new therapeutic strategies are urgently needed. Only a few Israeli studies have investigated antibiotic resistance of H. pylori [6, 7].
The rates of antibiotic resistance may fluctuate over the years and between different regions [8]. The aims of this study were to evaluate recent changes in H. pylori resistance between patients who had undergone an EGD and susceptibility testing and were found positive for H. pylori, in addition to identifying independent predictors for antimicrobial resistance in a single hospital during 2013–2016 (the early period) and 2017–2020 (the later period).
Methods
Study design
Cross-sectional.
Setting
The Department of Gastroenterology, Kaplan Medical Center, a university-affiliated hospital (600 beds) located in central Israel. Kaplan Medical Center’s institutional review board approved the study.
Participants
Between January 1, 2013 and December 31, 2020, 269 clinical isolates of H. pylori were isolated from antral biopsy specimens of 269 adult patients, one isolate from each patient. Fifty-seven were naïve patients previously not treated for H. pylori infection; 212 had been previously treated for this infection and had failed ≥ 1 treatment regimen, i.e., first-line triple therapy with a PPI, AMP, CLR or MET or second-line quadruple therapy with second-line quadruple therapy with PPI, MET, TET and bismuth or rescue treatment with PPI, AMP, LEV or RIF. The study period was divided into two sub-periods, 2013 to 2016 and 2017 to 2020. Patient characteristics and antimicrobial resistance between the two periods were compared.
Variables/data sources/measurement
Biopsy specimens were inoculated directly onto a Columbia blood agar (Difco, Detroit, MI) supplemented with a yeast extract of 5 g/L, laked lysed horse blood (7%), vancomycin (3 mg/L), colistin sulfate (7.5 mg/L), nystatin (12,500 IU/L) and co-trimoxazole (5 mg/L). Cultures were incubated for 72h at 37°C under microaerophilic conditions. H. pylori isolates were identified by colony morphology, characteristic spiral morphology on Gram staining and positive findings on catalase, urease, and oxidase tests. Susceptibility to six antibiotic agents: AMP, CLR, MET, TET, LEV and rifampicin were tested by the E-test (BioMérieux France). The strips were placed on dry agar plates. The minimum inhibitory concentration (MIC) values were determined after 72 h of incubation according to the E-test’s instructions. The H. pylori strain ATCC 43526 was used as quality control for the selective medium. The files of all cases were reviewed for age, gender, and comorbidities. Data regarding allergies to antibiotics and previous eradication treatments were identified from the patient's electronic medical records and recorded. Susceptibility to MET, CLR, TET, AMP, LEV and RIF was obtained from Kaplan’s Microbiology Laboratory electronic system.
Quantitative variables
Resistance was defined according to the clinical breakpoints proposed by the European Committee on Antimicrobial Susceptibility Testing for H. pylori [9]: AMP, MIC > 0.125 mg/l; TET, MIC > 1 mg/l; CLR, MIC > 0.5 mg/l; MET, MIC > 8 mg/l, LEV, MIC > 1 mg/l and RIF, MIC > 1 mg/l.
Statistical methods
Categorical variables were expressed as number and percentages. Distribution of age was assessed using a histogram and Q–Q plot. Since age was not normally distributed, it was reported as median and interquartile range (IQR). Categorical variables were compared by the Chi-square or Fisher's exact tests; age was compared by the Mann–Whitney test. Multivariable logistic regression calculated the independent association between time period and antimicrobial resistance. The time period was forced into the regression at the first block and then at the second. Variables that were significantly associated with the studied outcome were included in the regression. The backward method was applied for the second block using p > 0.1, the Wald test as criteria for variable removal. All statistical tests were two-sided; p < 0.05 was considered statistically significant. SPSS software was used for all statistical analyses (IBM SPSS statistics for window, version 27, IBM corp., Armonk, NY, USA, 2020).
Results
Patients
The study included 269 H. pylori isolates cultured from 269 patients. Of them, 86 were cultured before 2017 and 183 after. A comparison of the patients’ characteristics is presented in Table 1. Age, sex, comorbidities: diabetes mellitus (DM), ischemic heart disease, congestive heart failure and chronic renal failure were similar during the two periods. Patients grouped in the later period had a higher prevalence of DM (16.9% vs 7% P < 0.02). Allergies to penicillin, CLR, MET and TET were similar in the two groups. More previously treated patients and naïve untreated patients were included (P = 0.003) in the later period group; 135 had been previously treated for infection and failed more than one treatment regimen (first-line triple therapy with PPI, AMP, CLR, and/or MET or second-line quadruple therapy with second-line quadruple therapy with PPI, MET, TET, and bismuth or rescue treatment with PPI, AMP, LEV or RIF). Patients in the later period group were treated significantly more with CLR, MET, TET and bismuth.
Culture and susceptibility
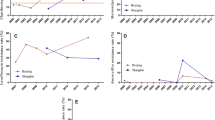
One hundred and thirty (71%) isolates out of 183 isolates of H. pylori were found significantly more resistant to CLR during the later period compared to 42 out of 86 isolates (48.8%, P < 0.001) during the early period (Table 2). Significantly higher dual CLR + MET resistance was seen during the late period in 59.6% isolates compared to 40.7% during the early period (P = 0.004). No statistically significant difference was found in resistance to MET, LEV or in simultaneous resistance for CLR-MET-LEV between the 2 time periods (Table 1). All cultures tested for AMP, TET and rifampicin in both periods, showed antibiotic susceptibility.
Factors independently associated with antibiotic resistance
A multivariate regression analysis revealed that the late period was an independent predictor of resistance to CLR (P = 0.001) and CLR + MET (P = 0.004) (Table 3). Increased age was significantly associated with resistance to CLR (P < 0.001), MET (P < 0.001) and dual resistance to CLR and MET (P < 0.001). DM was a predictor of MET resistance (P = 0.037). No statistically significant association was found between antibiotic resistance, gender, ischemic heart disease, congestive heart failure or previous antibiotic treatments.
Discussion
In this study, we compared patients’ characteristics and changes in H. pylori resistance in those who had undergone an EGD, H. pylori with susceptibility testing and were found positive for H. pylori. The study took place in a university affiliated hospital between 2013 to 2016 and 2017 to 2020. The main finding of our study was the significant change in H. pylori resistance to CLR and CLR + MET observed during the late period (2017–2020). We found that H. pylori resistance to CLR and CLR + MET was significantly more common during the late period (71.0% vs 48.8%, P < 0.001 and 59.6% vs 40.7%, P = 0.004, respectively).
The CLR resistance rate has been increasing since 1998 [10], although, since 2008, to a lesser extent in Europe [11]. Antibiotic misuse is the primary cause of the increase in resistance. Exposure to antibiotics is very high, Valle Muñoz et al. [12] reported that up to 46% of the patients for whom an eradication treatment was indicated, had received macrolides (mainly, CLR and azithromycin) during the previous 12–14 years. Yet, in our study, previous antibiotic treatment was not associated with antibiotic resistance in the multivariate analysis. Out of 130 H. pylori resistant to CLR in later period, 83 (63.8%) were previously treated with CLR. Out of 109 H. pylori resistance to CLR + MET in later period, sixty-six (60.6%) were previously treated with CLR.
A correlation between antibiotic administration and resistance to CLR has recently been proven in Europe [11, 13]. The H. pylori rate of resistance to LEV during the later period was 13.1%, as new quinolones in Israel are restricted. Resistance to rifampicin was 1.1%, as the use of RIF is very low and mostly used to treat mycobacterial infections.
Univariate analysis showed that the patient groups in the early and later periods were of similar age (mean 45 years vs 45.3 years, P = 0.458) and sex (females: 73.3% vs 68.3%, P = 0.409). The patient population in the later period had a higher prevalence of diabetes.
We also found that the later period and older age were independent predictors of CLR resistance, most probably related to the excessive use of macrolides for respiratory tract infections worldwide, including Israel [13,14,15,16]. Older age was an independent predictor of resistance to CLR, MET and CLR + MET suggesting longer exposure to empiric antibiotic therapy with macrolides and MET for common infections throughout the years [17]. Double H. pylori resistance to CLR and MET has been associated with a later period in time and older age, probably relating to our finding that patients in the later period group were treated significantly more with CLR and MET.
In our study, DM was found to be an independent predictor of MET resistance. Higher MET resistance in H. pylori-infected DM patients may be a result of the frequent use of these antibiotics for recurrent anaerobic bacterial infections due to the development of MET-resistant strains [18, 19].
Conclusions
Our study has shown that there is an increasing resistance of H. pylori to clarithromycin and metronidazole while its susceptibility is unaffected with time to other antibiotics. More recent cross-sectional studies with larger samples are warranted in order to evaluate the changes in the resistance patterns of H. pylori to various antibiotics with time.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MIC:
-
Minimum inhibitory concentration
- HTN:
-
Hypertension
- IHD:
-
Ischemic heart disease
- CHD:
-
Congestive heart failure
- CRF:
-
Chronic renal failure
- H. pylori:
-
Helicobacter pylori
- PPI:
-
Proton pump inhibitor
- AMP:
-
Amoxicillin
- CLR:
-
Clarithromycin
- MET:
-
Metronidazole
- TET:
-
Tetracycline
- LEV:
-
Levofloxacin
- RIF:
-
Rifabutin
- IQR:
-
Median and interquartile range
- DM:
-
Diabetes mellitus
References
Wroblewski LE, Peek RM, Wilson KT. Helicobacter pylori and gastric cancer: factors that modulate disease risk. Clin Microbiol Rev. 2010;23:713–9.
Muhsen K, Cohen D, Spungin-Bialik A, Shohat T. Seroprevalence, correlates and trends of Helicobacter pylori infection in the Israeli population. Epidemiol Infect. 2012;140:1207–14.
Lavy R, Hershkovitz Y, Keinan-Boker L, Halevy A. Incidence and trends of gastrointestinal malignancies in Jewish and Arab populations in Israel over 32 years. Isr Med Assoc J. 2016;18:466–9.
Fallone CA, Fallone CA, Chiba N, van Zanten SV, Fischbach L, Gisbert JP, et al. The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology. 2016;151:51–69.
Graham DY, Lee Y, Wu M. Rational Helicobacter pylori therapy: evidence-based medicine rather than medicine-based evidence. Clin Gastroenterol Hepatol. 2014;12:177-86.e3.
Yahav J, Shmuely H, Niv Y, Samra Z. In vitro activity of levofloxacin against Helicobacter pylori isolates from patients after treatment failure. Diagn Microbiol Infect Dis. 2006;55:81–3.
Zevit N, Levy I, Shmuely H, Samra Z, Yahav J. Antibiotic resistance of Helicobacter pylori in Israeli children. Scand J Gastroenterol. 2010;45:550–5.
Lopo I, Libânio D, Pita I, Dinis-Ribeiro M, Pimental-Nunes P. Helicobacter pylori antibiotic resistance in Portugal: systematic review and meta-analysis. Helicobacter. 2018;23: e12493.
The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 11.0, 2021. http://www.eucast.org.
Glupczynski Y, Mégraud F, Lopez-Brea M, Andersen LP. European multicenter survey of in vitro antimicrobial resistance in Helicobacter pylori. Eur J Clin Microbiol Infect Dis. 2001;20:820–3.
Megraud F, Bruyndonckx R, Coenen S, Wittkop L, Huang TD, Hoebeke M, et al. Helicobacter pylori resistance to antibiotics in Europe in 2018 and its relationship to antibiotic consumption in the community. Gut. 2021;70:1815–22.
Valle Muñoz J, Muñoz Gómez P, Sierra Bernal C, de Andrés E, Gómez Hernando C, Gómez RR. Tailored Helicobacter pylori eradication based on prior intake of macrolide antibiotics allows the use of triple therapy with optimal results in an area with high clarithromycin resistance. Rev Esp Enferm Dig. 2019;111:655–61.
Megraud F, Coenen S, Versporten A, Kist M, Lopez-Brea M, Hirschl AM, et al. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut. 2013;62:34–42.
Miendje Deyi VY, Bontems P, Vanderpas J, de Koster E, Ntounda R, Van den Borre C, Cadranel S, et al. Multicenter survey of routine determinations of resistance of Helicobacter pylori to antimicrobials over the last 20 years (1990 to 2009) in Belgium. J Clin Micro. 2011;49:2200–9.
Karlowsky JA, Lagacé-Wiens Philippe RS, Low DE, Zhanel GG. Annual macrolide prescription rates and the emergence of macrolide resistance among Streptococcus pneumoniae in Canada from 1995 to 2005. Int J Antimicrob Agents. 2009;34:375–9.
Adriaenssens N, Coenen S, Versporten A, Muller A, Minalu G, Faes C, et al. European Surveillance of Antimicrobial Consumption (ESAC): outpatient antibiotic use in Europe (1997–2009). J Antimicrob Chemother. 2011;66:vi3-12.
Savoldi A, Carrara E, Graham DY, Conti M, Tacconelli E. Prevalence of antibiotic resistance in Helicobacter pylori: a systematic review and meta-analysis in World Health Organization regions. Gastroenterology. 2018;155:1372–82.
Ojetti V, Migneco A, Silveri N, Ghirlanda G, Gasbarrini G, Gasbarrini A. The role of H. pylori infection in diabetes. Curr Diabetes Rev. 2005;1:343–7.
Boyanova L, Nikolov R, Gergova G, Evstatiev I, Lazarova E, Kamburov V, et al. Two-decade trends in primary Helicobacter pylori resistance to antibiotics in Bulgaria. Diagn Microbiol Infect Dis. 2010;67:319–26.
Acknowledgements
The authors thank Mrs. Phyllis Curchack Kornspan for her editorial services.
Funding
No sources of funding.
Author information
Authors and Affiliations
Contributions
HS was study initiator and prepared the manuscript. YS, RB, JY performed the data mining. RB, JY, EM gave technical support, consultation, and proof-read the manuscript. EM was the study coordinator. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Kaplan Medical Center’s institutional review board approved the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shmuely, H., Shvartsman, Y., Berdinstein, R. et al. The epidemiology of Helicobacter pylori resistance in a university affiliated hospital: a comparison between two time periods—a cross-sectional design. Eur J Med Res 28, 538 (2023). https://doi.org/10.1186/s40001-023-01500-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01500-0