
Abstract
From an initial pool of 2303 studies, ten eligible and potential studies were selected through rigor inclusion and exclusion criteria for this systematic review to examine music therapy's effect on dementia. The review included 967 participants, with the majority being female. A significant number of studies were conducted in Taiwan. Although several cognitive ability assessment methods were employed in the selected studies, the Mini-Mental State Examination (MMSE) was the most commonly used tool for evaluating the effects of music therapy on dementia. Overall, the current review demonstrates that music therapy can be a valuable strategy for treating patients with dementia, with its outcomes including improved cognitive function and potentially slowing the progression of the disease's severity. Therefore, this study can significantly contribute to future studies and practices aimed at using music therapy to treat dementia.
Similar content being viewed by others


Introduction
Dementia is a general term that describes diseases and conditions marked by a gradual decline in cognitive abilities, such as memory and language, as well as changes in behavior that may include depression and anxiety [1, 2]. It is a neurodegenerative disorder characterized by a decline in cognitive function, affecting memory, thinking, behavior, and emotion. The recent World Health Organization (WHO) report showed that more than 55 million people worldwide are currently affected by dementia [3]. According to this report, age—most commonly 65 years or older—increases the risk of developing dementia. Hence, with an aging population, the prevalence of dementia is expected to rise, creating significant challenges for healthcare systems worldwide. As China has undergone social and economic development in recent decades, its population has rapidly aged, leading to a proliferation of neurodegenerative disorders such as dementia [4].
It is a common trend to treat patients with dementia via pharmacological as well as non-pharmacological approaches. However, the pharmaceutical approaches cause side effects, including sedation, falls and extrapyramidal signs, reduced well-being and quality of life, increased cognitive decline rate, and more [5]. To make matters worse, pharmaceutical intervention for older adults may be even more challenging. Therefore, it is crucial at this point to explore alternative non-pharmaceutical approaches for treating dementia. Music therapy has been employed for several years to help alleviate symptoms of dementia [6, 7]. This technique can enhance mood, cognitive functions, and memory while providing a sense of connection and socialization for patients experiencing isolation [7, 8].
Despite music therapy being considered a promising intervention for people with dementia, the results of previous studies have shown discrepancies. While some studies suggest positive outcomes, others report inconclusive or adverse effects. Therefore, a systematic review is necessary to summarize and evaluate the existing evidence on the effectiveness of music therapy against dementia in older adults. We searched scientific literature using well-known databases to gather recent studies on the effect of music on dementia. After applying appropriate screening criteria, we selected the necessary number of studies for analysis in the current systematic review. This review will provide an overview of the current state of research, highlight potential gaps in knowledge, and offer recommendations for future studies and clinical practice.
Methods
Literature search
To examine the literature, we used PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines, the recommended standards for conducting systematic reviews [9, 10]. The PRISMA guidelines involve three planning phases: study identification, literature examination, and inclusion. We searched for articles about music therapy's effect on dementia based on our research objective.
The articles were searched against the well-known scientific literature repository databases, including Scopus, PubMed, and Web of Science. A combination of terms such as ("music," OR "music therapy," OR "music intervention," OR "music care") AND ("dementia" OR "Alzheimer's disease") was employed for the literature search. The literature search was conducted in March 2023.
Study selection
The selection criteria for including articles in this systemic review are listed in Table 1. Accordingly, articles were screened considering the study topic, geographic area, participants' age, publication year, article type, and publication language. The details of each selection criteria can be referred to in Table 1.
Data extraction and organization
First, the studies that fulfill the criteria above to be included in this review were imported into the Endnote reference management software. The selected articles were organized orderly in serial numbers (Table 2) for further communications. Articles were arranged based on their year of publication from the earliest to the latest. The selected articles were studied thoroughly to find common extractable data to assess the intervention approaches and outcomes. These extractable data items should commonly be found in two or more selected studies. The extracted data were handled in the Excel spreadsheet.
Quality assessment
In this review, the Mixed Methods Appraisal Tool (MMAT) version 2018 [11] was employed to evaluate the quality of the selected articles. To eliminate bias, the selected studies' quality was checked by two authors simultaneously. In this version of the MMAT, five different criteria for each category of study and two common screening questions are considered. The responses, including yes, no, or cannot tell, accompany these questions. The quality of the final articles to be included in this systematic review (Table 2) was evaluated and approved following these steps.
Results
Literature search
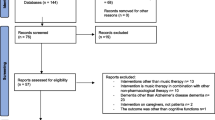
Literature was searched to collect studies on the effect of music therapy on dementia, as explained in the Methods section. The first search was conducted using the abovementioned terms without filtration. During this stage, 2303 studies were generated, of which 1222, 797, and 284 were from Scopus, PubMed, and Web of Science. As the largest abstract and citation research literature database, Scopus [12] comprised 53% of the total searched studies on this topic. The studies were filtered using the PRISMA approach. Nearly 68 and 31% of the literature were excluded from this review due to the replication of studies in the databases and using inclusion/exclusion criteria, respectively. The inclusion criteria employed in this review include (1) age group (elderly), (2) study geographic area (China), (3) article type (complete length journal research), (4) publication year (2013–2023), (5) article category (quantitative), and (6) language (English) (Table 1). Finally, ten studies were screened out to be included in this systemic review (Table 2). The detailed literature screening process is shown in Fig. 1.

Flowchart showing literature search for this review; prepared using PRISMA
Information on the selected studies and participants
Table 2 organized selected studies in an orderly based on publication year and contained information on the study period and publication, places of study in China, and participants' ages. The earliest and the latest studies were published in 2014 and 2023, respectively. Half of the literature screened for this systemic review was studied in Taiwan. This review also included other studies, consisting of two from Beijing and Hong Kong and one from Hangzhou. Regarding the participant's age, most studies include ≥ 65 years old. Only one study (Table 2 #6) included participants ≥ 55 years old.
Information on the number of participants in the selected studies is shown in Table 3. The total number of participants allocated in the initial stage of the study was 967. However, nearly 10% of the participants discontinued the study process for various reasons. Most participants (~ 53% of the initially allocated participants) discontinued study #2. On the contrary, all the initially allocated participants in studies #7 and #10 could complete the experimentation. Study #5 and #6 included the highest and the lowest number of participants in their research, respectively. Therefore, it is essential to consider these scenarios when allocating study participants to avoid ending up with a statistically unacceptable sample size. All studies allocate experimental (music therapy) and control groups. There were more participants in the experimental group than in the control counterpart. Another interesting fact is that all the studies included in this review allocated a significantly higher number of female participants than males.
Music therapy for dementia
Table 4 shows approaches, durations, and outcomes of music intervention to treat dementia. Various music therapy approaches, such as listening, singing, dancing, and playing instruments, were employed alone or in combination with other activities. Singing followed by listening was the most implemented music therapy approach. Singing or listening was employed in all the selected studies in Table 4. Generally, interventions were conducted up to 30–120 min/session for 6–24 weeks. Study #1 and #5, which conducted interventions for 30 and 30–40 min/session, twice/week, and twice/day for six weeks and three months, respectively, represent the shortest and the most extended intervention durations.
The standard methods to evaluate the effect of music therapy on dementia were the Mini-Mental State Examination (MMSE), Cornell Scale for Depression in Dementia (CSDD), Cohen-Mansfield Agitation Inventory (CMAI), and agitation. All studies combined various methods to assess the impact of music therapy on dementia. In Table 4, we included only common strategies for more studies, as explained in the Methods section. However, MMSE was the most utilized tool for such applications. All selected literature except study #10 employs MMSE. The MMSE scores for studies #6–#9 were only applied at baseline stages. The overall lowest (10.99 ± 4.16) and highest (22.71 ± 6.47) scores of MMSE were recorded in baselines of the study #8 experimental group and study #4 control group, respectively. The follow-up outcomes in the experimental groups of study #1 and #3 revealed improvements in their MMSE test scores, whereas studies #2, #4, and #5 decreased scores when compared with baseline counterparts. For instance, in study #1, the mean MMSE scores of the experimental group were 1.44–2.69 points higher than those of the control group at Times 2, 3, and 4, which were statistically significant differences (p = 0.026, p < 0.001, p = 0.044, respectively, Table 4). GEE analysis of scores for the six major cognitive domains in the MMSE indicated that the mean registration score of the experimental group was 0.50 points higher than that of the control group at Time 2, a statistically significant difference (p = 0.006) and that the mean recall scores for the experimental group were 0.63, 0.92, and 0.79 points higher than those of the control group at Times 2, 3, and 4 (p = 0.014, p < 0.001, and p = 0.004, respectively; Table 4). Likewise, in study 3, for the experimental group, the scores of MMSE had a statistically significant increase after 16 weeks (p < 0.01) after four months, which affirms that the level of cognition in elders with dementia significantly increased after receiving group recreational activities. This could be explained by the fact that the patients in familiar leisure activities might enhance cognitive reserve and delay the pathological onset of dementia.
The follow-up was compared with their corresponding baselines. Furthermore, studies #1, #4, and #10 employed the CSDD test to measure the effect of music therapy on dementia. The CSDD scores for all these studies exhibited a decline in the follow-up stage of the experimental group. CMAI was also used in the studies of #6 and #8. The detailed outcomes of music therapy on dementia can be referred to in Table 4.
Discussion
This systemic review assessed the effect of music therapy on dementia for older adults residing in China. After the successive screening processes, ten studies were selected to be analyzed in this study. This review sought to provide up-to-date information on the topic as it covers recent research progress in the last decade (2013–2023). The current review identified the importance of incorporating a combination of various intervention approaches and measurement methods while studying the effects of music therapy on dementia. Most studies selected for this review implemented additional interventions along with music therapy (Table 4), including color sound bell (#1), folk recreation (#3), walking (#6), movement (#8), stories and drama (#9), discussion and games (#10), etc. Studies #2 and #5 only applied singing and/or listening. Moreover, these studies' cognitive function test results did not significantly improve. However, further research is needed to conclude this idea. Previous studies that were not included in this review also used additional activities such as cooking [23], nature videos [24], meditation [25], and painting [26] with music therapy to treat patients with dementia.
All studies selected in this systemic review (Table 4) applied multiple methods to measure the effect of music therapy on dementia. However, we have included in Table 4 those measurement methods common to at least two studies. MMSE has employed 90% of the studies. MMSE is considered the best and the most known tool to generate the overall measurement of cognitive impairment for clinical, community, and research settings [27]. This method is preferred due to its simple administration process and high acceptance among healthcare professionals working with individuals with dementia. The MMSE assesses an individual's orientation, concentration, attention, verbal memory, naming ability, and visuospatial skills, with a possible maximum score of 30 points. The scoring system of MMSE is as follows: higher scores suggest better cognitive functioning, a score of 23 or lower may indicate cognitive impairment and a score of 18 or lower suggests severe cognitive impairment [28]. Accordingly, the MMSE score for all the studies in the experimental groups indicated a severe cognitive impairment; out of the nine studies that included MMSE in their cognitive analysis, only five of the studies measured for both the baseline and follow-up stages. Out of these, studies #1 and #3 showed increments in their corresponding follow-up MMSE scores.
According to a recent study [27], using the MMSE alone as a single-administration test may not be sufficient to identify patients at risk of developing dementia. Therefore, it is crucial to conduct a series of tests to determine the status of dementia and develop proper management of patients. To this end, the studies selected for this systemic review have incorporated other dementia measurement techniques, such as CSDD, CMAI, and agitation (Table 4).
The effects of music therapy on dementia can be assessed by comparing (1) baseline and follow-up, (2) experimental and control groups within the same study, and (3) a particular study with other similar studies. It is worth noting that music therapy can also be used to treat and potentially slow the progression of dementia to its severe stages. For example, in study #10, the experimental CSSD, which was 5.6 ± 4.7 in the baseline, remained 5.2 ± 4.6 after four weeks of follow-up. On the other hand, the control group showed significant progress, with the score increasing from 6.8 ± 6.6 to 11.7 ± 7.2. Overall, this review showed that music therapy significantly affects dementia by improving depression and anxiety scores or prolonging disease progression easily, which are substantially related to older people's mental health.
The current review has limitations, including heterogeneously in the intervention approaches and cognitive measurement methods between the selected studies. These factors have a substantial effect in analyzing the effect of music therapy on dementia. Due to the limited number of studies included in this systematic review and the limitations above, it is challenging to arrive at a concrete conclusion. Nonetheless, we believe this study can offer valuable and up-to-date information on the impact of music therapy on dementia. Moreover, it can be a foundation for future studies and reviews in this field.
Conclusions
Our study concludes that music therapy has improved cognitive and psychiatric trends in people with dementia. Furthermore, a long-term MT intervention positively affects depression and anxiety. Moreover, music therapy intervention seems to improve the quality of life of dementia patients. Music therapy could improve verbal fluency and reduce anxiety, depression, and apathy in selected patients living with dementia, although there do not appear to be proven benefits on memory, daily function, or overall quality of life. More clinical trials are needed to allow for more definitive conclusions on the therapeutic value of music therapy to patients with dementia.
Future research recommendation
Regardless of limitations, music therapy is an effective intervention treatment. For this reason, more medical involvement and procedures should be promoted to confirm the positive effect of music interventions. Second, most review studies have fewer participants, which cannot provide robust, randomized findings. Since each clinical practice procedure and method is varied, it is necessary to implement a standardized medical trial to measure patients' cognitive function and behavioral features. More longitudinal studies are recommended to explore the development and benefits of music therapy. More theoretical models for outcomes and results should be defined to treat dementia patients.
Availability of data and materials
Not applicable.
References
Dyer SM, Harrison SL, Laver K, Whitehead C, Crotty M. An overview of systematic reviews of pharmacological and non-pharmacological interventions for the treatment of behavioral and psychological symptoms of dementia. Int Psychogeriatr. 2017;30:295–309. https://doi.org/10.1017/S1041610217002344.
Moreno-Morales C, Calero R, Moreno-Morales P, Pintado C. Music therapy in the treatment of dementia: a systematic review and meta-analysis. Front Med. 2020. https://doi.org/10.3389/fmed.2020.00160.
WHO. Dementia. https://www.who.int/news-room/fact-sheets/detail/dementia; 2023. Accessed 18 Apr 2023.
Ren R, Qi J, Lin S, Liu X, Yin P, Wang Z, Tang R, Wang J, Huang Q, Li J, et al. The China Alzheimer Report 2022. Gen Psychiatr. 2022;35: e100751. https://doi.org/10.1136/gpsych-2022-100751.
Douglas S, James I, Ballard C. Non-pharmacological interventions in dementia. Adv Psychiatr Treat. 2018;10:171–7. https://doi.org/10.1192/apt.10.3.171.
Raglio A, Oasi O. Music and health: what interventions for what results? Front Psychol. 2015. https://doi.org/10.3389/fpsyg.2015.00230.
Bleibel M, El Cheikh A, Sadier NS, Abou-Abbas L. The effect of music therapy on cognitive functions in patients with Alzheimer’s disease: a systematic review of randomized controlled trials. Alzheimers Res Ther. 2023;15:65. https://doi.org/10.1186/s13195-023-01214-9.
Koelsch S. Brain correlates of music-evoked emotions. Nat Rev Neurosci. 2014;15:170–80. https://doi.org/10.1038/nrn3666.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71. https://doi.org/10.1136/bmj.n71.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6: e1000097. https://doi.org/10.1371/journal.pmed.1000097.
Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, Gagnon M-P, Griffiths F, Nicolau B, O’Cathain A, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018;34:285–91. https://doi.org/10.3233/EFI-180221.
Luo X, Chen H, Song Y, Qin Z, Xu L, He N, Tan Y, Dessie W. Advancements, challenges and future perspectives on peptide-based drugs: focus on antimicrobial peptides. Eur J Pharm Sci. 2023;181: 106363. https://doi.org/10.1016/j.ejps.2022.106363.
Chu H, Yang CY, Lin Y, Ou KL, Lee TY, O’Brien AP, Chou KR. The impact of group music therapy on depression and cognition in elderly persons with dementia: a randomized controlled study. Biol Res Nurs. 2014;16:209–17. https://doi.org/10.1177/1099800413485410.
Li CH, Liu CK, Yang YH, Chou MC, Chen CH, Lai CL. Adjunct effect of music therapy on cognition in Alzheimer’s disease in Taiwan: a pilot study. Neuropsychiatr Dis Treat. 2015;11:291–6. https://doi.org/10.2147/ndt.s73928.
Li D-M, Li X-X. The effect of folk recreation program in improving symptoms: a study of Chinese elder dementia patients. Int J Geriatr Psychiatry. 2017;32:901–8. https://doi.org/10.1002/gps.4543.
Wang S-C, Yu C-L, Chang S-H. Effect of music care on depression and behavioral problems in elderly people with dementia in Taiwan: a quasi-experimental, longitudinal study. Aging Ment Health. 2017;21:156–62. https://doi.org/10.1080/13607863.2015.1093602.
Lyu J, Zhang J, Mu H, Li W, Champ M, Xiong Q, Gao T, Xie L, Jin W, Yang W, et al. The effects of music therapy on cognition, psychiatric symptoms, and activities of daily living in patients with Alzheimer’s disease. J Alzheimers Dis. 2018;64:1347–58. https://doi.org/10.3233/jad-180183.
Chen YL, Pei YC. Musical dual-task training in patients with mild-to-moderate dementia: a randomized controlled trial. Neuropsychiatr Dis Treat. 2018;14:1381–93. https://doi.org/10.2147/ndt.s159174.
Ho RT, Fong TC, Sing CY, Lee PH, Leung AB, Chung KS, Kwok JK. Managing behavioral and psychological symptoms in Chinese elderly with dementia via group-based music intervention: a cluster randomized controlled trial. Dementia (London, England). 2019;18:2785–98. https://doi.org/10.1177/1471301218760023.
Cheung DSK, Lai CKY, Wong FKY, Leung MCP. Is music-with-movement intervention better than music listening and social activities in alleviating agitation of people with moderate dementia? A randomized controlled trial. Dementia. 2020;19:1413–25. https://doi.org/10.1177/1471301218800195.
Chen X, Li D, Xu H, Hu Z. Effect of traditional opera on older adults with dementia. Geriatr Nurs. 2020;41:118–23. https://doi.org/10.1016/j.gerinurse.2019.08.002.
Tz-Han L, Wan-Ru W, I-Hui C, Hui-Chuan H. Reminiscence music intervention on cognitive, depressive, and behavioral symptoms in older adults with dementia. Geriatr Nurs. 2023;49:127–32. https://doi.org/10.1016/j.gerinurse.2022.11.014.
Narme P, Clément S, Ehrlé N, Schiaratura L, Vachez S, Courtaigne B, Munsch F, Samson S. Efficacy of musical interventions in dementia: evidence from a randomized controlled trial. J Alzheimers Dis. 2014;38:359–69. https://doi.org/10.3233/jad-130893.
Gómez-Gallego M, Gómez-Gallego JC, Gallego-Mellado M, García-García J. Comparative efficacy of active group music intervention versus group music listening in Alzheimer’s disease. Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph18158067.
Innes KE, Selfe TK, Brundage K, Montgomery C, Wen S, Kandati S, Bowles H, Khalsa DS, Huysmans Z. Effects of meditation and music-listening on blood biomarkers of cellular aging and Alzheimer’s disease in adults with subjective cognitive decline: an exploratory randomized clinical trial. J Alzheimers Dis. 2018;66:947–70. https://doi.org/10.3233/jad-180164.
Pongan E, Tillmann B, Leveque Y, Trombert B, Getenet JC, Auguste N, Dauphinot V, El Haouari H, Navez M, Dorey JM, et al. Can musical or painting interventions improve chronic pain, mood, quality of life, and cognition in patients with mild Alzheimer’s disease? Evidence from a randomized controlled trial. J Alzheimers Dis. 2017;60:663–77. https://doi.org/10.3233/jad-170410.
Arevalo-Rodriguez I, Smailagic N, Roqué-Figuls M, Ciapponi A, Sanchez-Perez E, Giannakou A, Pedraza OL, Bonfill Cosp X, Cullum S. Mini-Mental State Examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev. 2021;7: CD010783. https://doi.org/10.1002/14651858.CD010783.pub3.
Norris D, Clark MS, Shipley S. The mental status examination. Am Fam Physician. 2016;94:635–41.
Acknowledgements
The authors would like to thank the authors and reviewers of this paper.
Funding
The authors received no funding for this work.
Author information
Authors and Affiliations
Contributions
CG, HX, XZ, and CL participated in the conceptualization, methodology, writing, and editing. CG, CL, and XZ participated in the supervision, revision, and project administration. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lin, C., Xuanxu, H., Yuyang, X. et al. The impact of music listening intervention on Asia elderly with dementia: a systematic review. Eur J Med Res 28, 535 (2023). https://doi.org/10.1186/s40001-023-01355-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01355-5