
Abstract
Background
Much less is known about the importance of blood pressure (BP) trajectories concerning the incidence of coronary heart disease (CHD) in people with disabilities. Our aim was to evaluate this association.
Methods
This cohort study surveyed 5711 adults from the Shanghai Disability Health Survey from June 2012 to June 2019. The latent class growth mixture model was used to examine distinct BP trajectories. We evaluated the association of BP trajectories with the risk of CHD by Cox proportional hazard models. The model for CHD risk fitted to BP trajectories was compared with models fitted to other BP-related indicators by goodness-of-fit, discrimination, and calibration.
Results
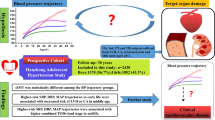
During a median follow-up of 71.74 months, 686 cases (median age was 49.03 (54.49, 58.55) years, 51.90% female) with CHD were identified, with a cumulative incidence of 12.01%. Systolic BP (SBP) and diastolic BP (DBP) were categorized into three classes, respectively. A statistically significant association was only observed between SBP trajectories and CHD. Compared with the normotensive stable SBP group (n = 1956), the prehypertension-stable group (n = 3268) had a higher risk (adjust hazards ratio (aHR) = 1.266, 95% confidence interval (CI) 1.014–1.581), and the stage 1 hypertension-decreasing group (n = 487) had the highest risk (aHR = 1.609, 95%CI 1.157–2.238). Among the BP-related indicators, the SBP trajectory was the strongest predictor of new-onset CHD. Findings were similar when sensitivity analyses were conducted.
Conclusions
SBP trajectory was a more important risk factor for CHD than other BP-related indicators and stringent BP control strategies may be effective for primary CHD prevention in the disabled population.
Similar content being viewed by others


Background
According to the latest report on disability by the World Health Organization [1], more than one billion individuals, around 15% of the global population, lived with some form of disability. Meanwhile, a recent report indicated that the number of people with disabilities has reached nearly 7% of China's total population [2]. Studies have shown a strong link between the increased incidence of disability and chronic diseases, such as hypertension, diabetes, and stroke [3, 4]. In addition, the huge health disparity between people with and without disabilities has been widely demonstrated [5, 6]. People with disabilities may be more susceptible to various chronic diseases due to greater social isolation and less access to preventive care [7, 8]. However, few studies have analyzed the epidemic of the coronary heart disease (CHD) that accompany individuals who are already disabled.
Blood pressure (BP) is a leading treatable risk factor for CHD, a common chronic cardiovascular disease (CVD) that exists widely in the world, and has been deeply studied in the general population [9, 10]. Most studies focusing on the relationship between BP and the onset of CHD were mainly based on BP data from single measurements at baseline or the variability of multiple measurements [11,12,13,14]. Results from such approaches have suggested that the risk of incident CHD increases with increasing baseline BP and variability in BP. However, the above BP indicators may not adequately reflect longitudinal BP changes in individuals. Several recent studies have explored the role of BP patterns over time (i.e., BP trajectories) in predicting CVD outcomes, dynamically reflecting the impact of arterial BP on the development of diseases [15,16,17,18,19]. In particular, high-level and rapidly increasing BP patterns are associated with a high risk of stroke over an age range from 55 to 106 years. Nevertheless, much less is known about the importance of BP trajectories over time concerning the incidence of CHD in people with disabilities.
Thus, this study aimed to identify distinct longitudinal trajectories of systolic BP (SBP) and diastolic BP (DBP) over 7 years and to investigate the association of these trajectories with the risk of the onset of CHD among the disabled population. Moreover, we compared other BP-related indicators concerning the incident CHD.
Methods
Design and study populations
The cohort study comprised the adult disabled population who were newly diagnosed with CHD and derived from the Shanghai Disability Health Survey (SDHS) conducted by the Shanghai Disabled Persons' Federation. This ongoing SDHS was initiated in June 2012 and followed up annually to provide free health examination services to disabled people through designated medical institutions. Until June 2019, 10,505 potential individuals from 16 districts in Shanghai were recruited for the SDHS at Shanghai YangZhi Rehabilitation Hospital (Shanghai Sunshine Rehabilitation Center), one of the largest designated medical and healthcare institutions. Subjects who voluntarily participated in this program have informed and consented to the possible use of relevant health data for scientific research. The study has been ethically approved by the medical ethics committee of the institution (No. YZ 2019-051).
This study selected 5711 participants based on the exclusion criteria: (i) under 18 or over 65 years; (ii) with CHD at enrollment between 2012 and 2013; (iii) with other serious diseases, such as malignancy, organ failure, severe trauma, cortical damage; (iii) pregnant or lactating women, or those who are planning to become pregnant; (iv) failure to complete electronic health records; (v) less than 3 health examinations if CHD was not diagnosed in 2019, as shown in Fig. 1.

Consort flow diagram for participants included in the study
Assessment of blood pressure
BP was measured by trained technicians using a cuffed electronic sphygmomanometer (Omron Corp., Tokyo, Japan) on participants after at least a 5-min rest, the upper arm with the higher reading was measured twice and the average was recorded in the electronic health system. For participants with missing upper limbs, the physician measured BP from both legs (ankle-posterior tibial artery) in the prone position. A total of 23 participants underwent leg BP measurements and the results were converted by a formula that was used to ensure consistency with arm measurements [20].
Assessment of coronary heart disease
CHD was defined as fatal ischemic heart disease (International Classification of Disease 10th revision code, ICD-10 I20-I25) or non-fatal myocardial infarction (ICD-10 I21-I23). At baseline, the history of CHD was assessed by interview and verified using medical records. Of all potential CHD, medical records from general practitioners and hospital discharge diagnoses were collected and reviewed by physicians.
Covariates
All participants had a medical and functional assessment by a medical professional. The health examination included anthropometry measurements (height, weight, resting BP, etc.), fasting biochemical indicators (blood, urine indicators, etc.), electrocardiogram, imaging ultrasound, as well as a questionnaire on demographic variables (gender, age, education, etc.), comorbidities (hypertension, diabetes, fatty liver disease, etc.) and disability condition (classification and grade). The classification and grade criteria of disabilities are based on the Chinese national standard for Classification and Grading Criteria of Disabilities (GB/T 26341-2010) [21]. Body mass index (BMI) was defined as the weight (kg)/(height (m)2), with the height measured in the supine position for those unable to stand.
Laboratory tests included red blood cell count (RBC), white blood cell count (WBC), platelet (PLT), hemoglobin (Hb), serum creatinine (SCr), serum urea (SU); uric acid (UA); fasting blood glucose (FBG), total cholesterol (TC), triglyceride (TG), total protein (TP), albumin (Alb), globulin (Glo), alpha fetoprotein (AFP), carcinoembryonic antigen (CEA), and alanine aminotransferase (Alt). The estimated glomerular filtration rate (eGFR) was calculated based on the Modification of Diet in the Renal Disease equation [22].
Statistical analysis
Using the lcmm package in Statistical software R (version 4.2.1, R Core Team, R Foundation for Statistical Computing, Vienna, Austria), the latent class growth mixture model (LCGMM) was applied to identify longitudinal trajectories over time in the disabled population. We compared two- to five-class models iterating 1st- to 3rd-degree fractional polynomials. The best-fitting one was determined by the minimum absolute value of the Bayesian information criterion (BIC), the average posterior probability (AvePP) of each subgroup, the proportion of each subgroup with eligible posterior probability, and the membership of each subgroup. The age and gender of each wave were adjusted when the LCGMM was performed as relevant studies have shown that these variables may influence the evolution of BP [16, 23].
If distributed normally by the Kolmogorov–Smirnov test, continuous variables were presented as means and standard deviations; otherwise, medians and interquartile ranges were applied. Categorical variables were presented by numbers and proportions. Descriptive analyses were compared between the CHD group and non-CHD group using independent sample t-test for normally distributed data, Pearson χ2 test for categorical variables, and Mann–Whitney U test or Kruskal–Wallis test for non-parametric continuous data.
Baseline characteristics were compared between the different BP trajectory subgroups. The Kaplan–Meier method was performed to estimate the overall cumulative incidence of CHD from the baseline study visit onwards. Next, Cox proportional hazards models by survival package in R (version 4.2.1, R Core Team, R Foundation for Statistical Computing, Vienna, Austria) were used to investigate the association of BP trajectories, single BP (measured at baseline), average BP (average of all available BP levels during the follow-up), and coefficient of variation (CV) of BP (standard deviation/average BP during the follow-up) with risk of CHD by adjusting hazards ratio (aHR) and the corresponding 95% confidence interval (CI), respectively. Significant variables in the univariate model (p < 0.1) were entered into the multivariate model as covariates, including age, gender, education, etc. In addition, we calculated the population attributable risk (PAR). The akaike information criterion (AIC) and BIC of models were compared to investigate the best model fit. In addition, discrimination was measured using receiver operating characteristic (ROC) curves and the area under the curve (AUC), and calibration was measured using calibration plots. Sensitivity analyses were conducted to explore the robustness of our results in modeling without fitting age and sex and hypertension stratification subgroups. A 2-sided P < 0.05 was considered statistically significant. (see Additional file 1 for details).
Results
Baseline characteristics of all participants
A total of 5711 eligible individuals were included in this study, of which 686 cases had new-onset CHD during a median follow-up period of 71.74 months, with a cumulative incidence of 12.01%. The median age was 49.03 (54.49, 58.55) years and 2759 (48.31%) were female. More than half (55.86%) of the participants were physically disabled, and the highest percentage of disability grades were mild and moderate (76.88%). Baseline characteristics of the participant by CHD status are summarized in Additional file 2: Table S1. People with CHD were more likely to be older, female, higher educational level, fatter and physically disabled, and had a higher prevalence of hypertension and diabetes mellitus, as well as higher SBP compared to those with no CHD. Several metabolic biomarkers were also significantly different when compared between the two groups, including Hb, RBC, WBC, FBG, TC, TG, Alb, UA, SU, and eGFR (all p < 0.05).
Characteristics of the BP trajectory classes
When investigating the trajectories, three categories of SBP and DBP were identified as the best fit with the lowest BIC, suitable AvePP, and a sufficient number of each subgroup, respectively (Additional file 2: Tables S2 and S3). Figure 2A shows the three trajectories of SBP based on the LCGMM. The largest class was characterized by a sustained slow decline in prehypertensive SBP, starting at ≈136 mmHg at enrollment and declining to ≈130 mm Hg at the end (class 2, n = 3268). The smallest class was characterized by a much steeper decrease in high-level SBP from approximately 161 to 129 mmHg during the follow-up (class 3, n = 487). In addition, another class was characterized by a sustained slow rise in normotensive SBP from approximately 122 to 129 mmHg (class 1, n = 1956). Figure 2B presents the three trajectories of DBP, similar to that of SBP, but the smallest class drops rapidly from 100 to 82 mmHg and then rises slowly (class 3, n = 534). In addition, the shape of trajectories for the other indicators (FBG, TC, TG, and eGFR) was shown in Additional file 2: Figure S1.

Trajectories of blood pressure predicted by the LCGMM among 5711 disabled individuals. A, SBP. B, DBP. The solid line represents the average BP in a class and the shaded area indicated 95% CIs
Demographic and health-related characteristics across BP trajectory groups were described in Table 1. Statistically significant differences were detected among SBP classes in age, gender, education level, BMI, classification of disabilities, comorbidities (except hyperlipemia), BP (SBP and DBP), and some metabolic biomarkers (FBG, TC, TG, etc.) (all p < 0.05). Characteristics with statistically significant differences among DBP trajectory groups were almost identical to those for SBP. During the follow-up period, longitudinal BP and some metabolic indicators (FBG, TC, TG, and eGFR) of the disabled population by BP trajectories and CHD status were displayed in Additional file 2: Tables S4 and S5, respectively. There were both significant differences in five average indicators (SBP, DBP, FBG, TC, and TG), three CV indicators (SBP, DBP, and FBG), and trajectories of four metabolic biomarkers among different SBP and DBP trajectory groups (all p < 0.05). Compared to the group without CHD, disabled people with CHD had higher average SBP and FBG, higher CVs for SBP, DBP, FBG, TC, and eGFR, as well as different proportions of trajectories for SBP, DBP, FBG, TC, and eGFR (all p < 0.05).
Association of BP trajectories with incident CHD
Kaplan–Meier curves for the overall cumulative incidence and number at risk for CHD stratified by BP trajectories and disability-related indicators (classification and grade) are displayed in Fig. 3. Analysis showed significant differences in the cumulative incidence curves for SBP trajectories, DBP trajectories, and the classification (all P < 0.001). Furthermore, the variables that differed significantly in univariate Cox analysis (p < 0.1) were subsequently entered into each of the four multivariate models to assess the risk factors correlated with new-onset CHD (Additional file 2: Tables S6, S7, and S8). Significant differences were detected among SBP trajectories after adjustment for covariates listed above, with a significant increase in CHD risk for class 2 (aHR = 1.266, 95% CI 1.014–1.581) and class 3 (aHR = 1.609, 95% CI 1.157–2.238) relative to class 1, respectively (Table 2). Compared with the normotensive stable SBP group (class 1), the PAR was 12.89% in the prehypertension-stable group (class 2) and 5.24% in the stage 1 hypertension-decreasing group (class 3). However, the DBP trajectory was not statistically significant in the multivariate model.

Kaplan–Meier curves for the overall cumulative incidence of CHD and number at risk, stratified by A SBP trajectories, B DBP trajectories, C classification of disabilities, D grading of disabilities. The shaded area indicates the range of 95% CIs for the corresponding cumulative incidence curve. P-value indicates the significance level from the comparison of incidence curves using the Log-rank test
In addition to the SBP trajectory, CHD risk was also associated with average SBP (aHR = 1.006, 95% CI 1.001, 1.012), CV of SBP (aHR = 10.454, 95% CI 1.407, 77.666), and baseline SBP (aHR = 1.004, 95% CI 1.000–1.008) by model 2 to model 4 analysis, respectively (Table 2). Comparing the evaluation indexes of four models, the SBP trajectory was more likely to be the strongest predictor of new-onset CHD in the disabled population (by the highest AUC and lowest BIC/AIC in Table 3, Additional file 2: Figures S2, S3).
Sensitivity analyses
Without fitting age and sex in the LCGMM, the BP trajectories were in line with the main analyses (Additional file 2: Figure S4). The association of BP trajectories with new-onset CHD and comparison of four Cox models based on different BP-related indicators are presented in Additional file 2: Tables S9 and S10, which did not provide additional insights.
Another sensitivity assessment was performed to model the BP trajectory based on stratification of whether the individuals with disabilities had hypertension at baseline. Although both SBP and DBP trajectories were one less in the hypertensive subgroup than in the non-hypertensive subgroup (Additional file 2: Figures S5 and S6), the relationship between BP trajectories and CHD and the comparison of modeling results for the four BP-related metrics were similar to the primary results (Additional file 2: Tables S9 and S10).
Discussion
Although previous studies have discussed the relationship between BP trajectories and CVDs risk in the general population, the association among the disabled population has rarely been elucidated. In the current study, we explored the association between BP trajectories and CHD risk in the disabled population using a substantial population-based cohort. First, the trajectories of SBP and DBP were categorized into three classes by LCGMM, respectively. Second, the disabled individuals in stage 1 hypertension-decreasing SBP group and prehypertension-stable SBP group had higher CHD risk relative to the normotensive-stable SBP group. Third, the SBP trajectory may be a stronger predictor of CHD than single baseline SBP, average SBP, and CV of SBP.
Our findings identified three SBP and DBP trajectories separately, these overall trend waves were consistent with previous cohort studies on BP trajectories associated with CVDs during follow-up in the general population but the number of trajectories ranged from three to five classes [15, 24, 25]. The main difference is that we did not find a trajectory of BP that rose significantly from normal levels to high values, which may be due to population differences and limitations of the LCGMM fitting subgroup sample. In addition, subgroup analysis revealed almost identical trajectories to the primary results in the no-hypertension group, but only two BP trajectories were found in the hypertensive group without the normotensive-stable BP class (< 130/80 mmHg).
The relationship between BP trajectories and CVD is not identical due to the heterogeneity in the characteristics of trajectories and populations in relevant studies. Our study suggests that the disabled individuals in the stage 1 hypertension-decreasing SBP group (160–120 mmHg) and the prehypertension-stable group (130–140 mmHg) may both increase the risk of future CHD, although a statistically significant association was not observed between DBP trajectories and CHD after multivariate adjustment. Among the general population, the Framingham Heart Study explored 16-year trajectories of BP and its association with the risk of atrial fibrillation in 4351 participants and found that the risk was doubled in participants who had initially elevated levels of SBP and then either decreased or increased SBP, yet the trajectory of DBP was not an independent predictor [18]. A 7-year cohort study determined that class 2 (SBP persistently around 133 mmHg) and class 3 (initially elevated SBP decreasing to normal) were associated with increased CVD risk relative to class 1 (initially normal levels increasing to above 140 mmHg) among 4067 individuals [15]. In China, five distinct BP trajectories over 4 years were identified in the Kailuan Study, the prehypertension-stable SBP group had higher stroke risk and individuals in the stage 2 hypertension-stable group (175–179 mmHg) had the highest risk of intracerebral hemorrhage and cerebral infarction relative to the normotensive-stable group (< 130 mmHg), and trajectories of DBP was also significantly associated with the risks of above outcomes [26]. Moreover, a meta-analysis among 123 studies with 613,815 participants revealed that lowering SBP to less than 130 mmHg significantly reduced the risk of CHD [11]. Our results indicated that people with disabilities may have an impact on health outcomes once they are chronically exposed to pre-hypertension or poorly controlled BP over their life course, and a more stringent BP control strategy may be more effective for primary CHD prevention. However, the optimal BP goal for primary CHD prevention remains unclear in the disabled population.
The association between single baseline BP as well as long-term variability and CHD risk have been previously demonstrated [9, 11,12,13, 27]. These findings were also revealed in our study, in addition to the fact that SBP trajectory was considered as an independent better predictor among disabled subjects. More information was added to the existing knowledge regarding risk factors and prevention of CHD as they suggest that effects of elevated BP levels may take several years to appear, and that longitudinal analysis of risk factors can improve the prediction of outcomes compared to single measurements or averages [26, 28]. Group-based trajectory modeling takes into account the averages and variations of multiple measurements to distinguish dynamic exposure in BP over time [29], which could reflect the potential impact of long-term BP on target organs. Available evidence showed that consecutive years of hypertensive trajectories are strongly correlated with subclinical atherosclerosis, intima-media thickness, and left ventricular mass index [30, 31]. Assessing BP trajectories provided a more nuanced understanding of the association between BP and CHD and improved prediction of CVD, our findings could help provide new insights into the prevention and management of CVDs in the disabled population.
Our study has several limitations. First, due to difficulties in collecting self-reported data from disabled people in the early study, we were unable to assess information on their diet, physical activity, the accessibility of medical resources, socioeconomic status, and care for them. However, all SDHS participants have access to Shanghai Disability Living Guarantee, which can reduce this gap to some extent. Second, low/high density lipoprotein cholesterol tests were not included in the examination due to limited funding for SDHS. Therefore, we attempted to mitigate this effect by entering trajectories of other objective indicators affecting BP in the multivariate model. Third, the lack of detailed information on antihypertensive treatment may lead to non-differential misclassification, but a sensitivity analysis stratified by hypertension was performed. Fourth, the subjects in this study may have overrepresented those who lived longer, because participants with poor cardiovascular profiles may have died before their next physical examination, which may have led to an underestimation of the association between BP trajectory and CHD risk.
Conclusion
Our study observed three distinct BP trajectories in people with disabilities and these trajectories were associated with future CHD risk. Monitoring BP trajectories over time could provide a more important approach to identifying these individuals with higher risk and preventing CHD. Future research needs to explore the optimal BP goal for primary CVDs prevention in the disabled population.
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BP:
-
Blood pressure
- CHD:
-
Coronary heart disease
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- HR:
-
Hazard ratio
- aHR:
-
Adjust hazard ratio
- CI:
-
Confidence interval
- CVD:
-
Cardiovascular disease
- SDHS:
-
Shanghai disability health survey
- BMI:
-
Body mass index
- RBC:
-
Red blood cell count
- WBC:
-
White blood cell count
- PLT:
-
Platelet
- Hb:
-
Hemoglobin
- SCr:
-
Serum creatinine
- SU:
-
Serum urea
- UA:
-
Uric acid
- FBG:
-
Fasting blood glucose
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- TP:
-
Total protein
- Alb:
-
Albumin
- Glo:
-
Globulin
- AFP:
-
Alpha fetoprotein
- CEA:
-
Carcinoembryonic antigen
- Alt:
-
Alanine aminotransferase
- eGFR:
-
Estimated glomerular filtration rate
- LCGMM:
-
Latent class growth mixture model
- PAR:
-
Population attributable risk
- BIC:
-
Bayesian information criterion
- AvePP:
-
Average posterior probability
- CV:
-
Coefficient of variation
- AIC:
-
Akaike information criterion
- ROC:
-
Receiver operating characteristic curves
- AUC:
-
Area under the curve
References
Krahn GL. WHO World Report on Disability: a review. Disabil Health J. 2011;4:141–2.
Leading Group of the Second China National Sample Survey on Disability NBoSotPsRoC. Communiqué on major statistics of the second China National Sample Survey on Disability. Chin J Rehabil Theory Pract. 2006;12:1013.
Collaborators GBDRF. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1345–422.
Fong JH. Disability incidence and functional decline among older adults with major chronic diseases. BMC Geriatr. 2019;19:323.
Kang Q, Chen G, Lu J, Yu H. Health Disparities by type of disability: health examination results of adults (18–64 Years) with disabilities in Shanghai. China PLoS One. 2016;11:e0155700.
Mitra M, Long-Bellil L, Moura I, Miles A, Kaye HS. Advancing health equity and reducing health disparities for people with disabilities in the United States. Health Aff (Millwood). 2022;41:1379–86.
Emerson E, Fortune N, Llewellyn G, Stancliffe R. Loneliness, social support, social isolation and wellbeing among working age adults with and without disability: cross-sectional study. Disabil Health J. 2021;14:100965.
Zhao X, Wang H. Disparities in unmet health service needs among people with disabilities in China. Int J Qual Health Care. 2021;33:136.
Fuchs FD, Whelton PK. High blood pressure and cardiovascular disease. Hypertension. 2020;75:285–92.
Tsao CW, Aday AW, Almarzooq ZI, Anderson CAM, Arora P, Avery CL, et al. Heart disease and stroke statistics-2023 update: a report from the american heart association. Circulation. 2023;147:e93–621.
Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387:957–67.
Stevens SL, Wood S, Koshiaris C, Law K, Glasziou P, Stevens RJ, et al. Blood pressure variability and cardiovascular disease: systematic review and meta-analysis. BMJ. 2016;354:i4098.
Gosmanova EO, Mikkelsen MK, Molnar MZ, Lu JL, Yessayan LT, Kalantar-Zadeh K, et al. Association of systolic blood pressure variability with mortality, coronary heart disease, stroke, and renal disease. J Am Coll Cardiol. 2016;68:1375–86.
Yu J, Song Q, Bai J, Wu S, Bu P, Li Y, et al. Visit-to-visit blood pressure variability and cardiovascular outcomes in patients receiving intensive versus standard blood pressure control: insights from the STEP trial. Hypertension. 2023;80:1507–16.
Smitson CC, Scherzer R, Shlipak MG, Psaty BM, Newman AB, Sarnak MJ, et al. Association of blood pressure trajectory with mortality, incident cardiovascular disease, and heart failure in the cardiovascular health study. Am J Hypertens. 2017;30:587–93.
Portegies ML, Mirza SS, Verlinden VJ, Hofman A, Koudstaal PJ, Swanson SA, et al. Mid- to late-life trajectories of blood pressure and the risk of stroke: the Rotterdam study. Hypertension. 2016;67:1126–32.
Tielemans SM, Geleijnse JM, Menotti A, Boshuizen HC, Soedamah-Muthu SS, Jacobs DR Jr, et al. Ten-year blood pressure trajectories, cardiovascular mortality, and life years lost in 2 extinction cohorts: the Minnesota business and professional men study and the Zutphen study. J Am Heart Assoc. 2015;4:e001378.
Rahman F, Yin X, Larson MG, Ellinor PT, Lubitz SA, Vasan RS, et al. Trajectories of risk factors and risk of new-onset atrial fibrillation in the framingham heart study. Hypertension. 2016;68:597–605.
German CA, Elfassy T, Singleton MJ, Rodriguez CJ, Ambrosius WT, Yeboah J. Trajectories of blood pressure control a year after randomization and incident cardiovascular outcomes in SPRINT. Am J Hypertens. 2021;34:973–80.
Sheppard JP, Albasri A, Franssen M, Fletcher B, Pealing L, Roberts N, et al. Defining the relationship between arm and leg blood pressure readings: a systematic review and meta-analysis. J Hypertens. 2019;37:660–70.
Chen Xinmin, Zhang Zongjiu, Ye Qi, Zhao Jialiang, Xibin S. Standardization Administration of the P.R.C. Classification and Grading Criteria of Disability. General administration of quality supervision, inspection and quarantine of the P.R.C. 1 May 2011. http://std.samr.gov.cn/gb/search/gbDetailed?id=71F772D7E01ED3A7E05397BE0A0AB82A.
Ndrepepa G, Holdenrieder S, Neumann FJ, Lahu S, Cassese S, Joner M, et al. Prognostic value of glomerular function estimated by Cockcroft-Gault creatinine clearance, MDRD-4, CKD-EPI and European Kidney Function Consortium equations in patients with acute coronary syndromes. Clin Chim Acta. 2021;523:106–13.
Ji H, Kim A, Ebinger JE, Niiranen TJ, Claggett BL, Bairey Merz CN, et al. Sex differences in blood pressure trajectories over the life course. JAMA Cardiol. 2020;5:19–26.
Li F, Lin Q, Li M, Chen L, Li Y. The association between blood pressure trajectories and risk of cardiovascular diseases among non-hypertensive Chinese population: a population-based cohort study. Int J Environ Res Public Health. 2021;18:2909.
Sharashova E, Wilsgaard T, Ball J, Morseth B, Gerdts E, Hopstock LA, et al. Long-term blood pressure trajectories and incident atrial fibrillation in women and men: the Tromso Study. Eur Heart J. 2020;41:1554–62.
Li W, Jin C, Vaidya A, Wu Y, Rexrode K, Zheng X, et al. Blood pressure trajectories and the risk of intracerebral hemorrhage and cerebral infarction: a prospective study. Hypertension. 2017;70:508–14.
Hajar R. Risk factors for coronary artery disease: historical perspectives. Heart Views. 2017;18:109–14.
Zheng W, Mu J, Chu C, Hu J, Yan Y, Ma Q, et al. Association of blood pressure trajectories in early life with subclinical renal damage in middle age. J Am Soc Nephrol. 2018;29:2835–46.
Herle M, Micali N, Abdulkadir M, Loos R, Bryant-Waugh R, Hubel C, et al. Identifying typical trajectories in longitudinal data: modelling strategies and interpretations. Eur J Epidemiol. 2020;35:205–22.
Allen NB, Siddique J, Wilkins JT, Shay C, Lewis CE, Goff DC, et al. Blood pressure trajectories in early adulthood and subclinical atherosclerosis in middle age. JAMA. 2014;311:490–7.
Hao G, Wang X, Treiber FA, Harshfield G, Kapuku G, Su S. Blood pressure trajectories from childhood to young adulthood associated with cardiovascular risk: results from the 23-year longitudinal Georgia stress and heart study. Hypertension. 2017;69:435–42.
Acknowledgements
We thank the information center, the medical examination center and the director Lingjing Jin of Shanghai YangZhi Rehabilitation Hospital (Shanghai Sunshine Rehabilitation Center) for their support.
Funding
This work was supported by the Grant of the Clinical Research Plan of Shanghai Hospital Development Centre (No. SHDC2022CRS049).
Author information
Authors and Affiliations
Contributions
YL, JW, HZ and HW designed the study. HZ and HW provided data. YL, JW, YW and CJ were involved in data preparation. YL and JW produced the analysis plan, processed data, conducted the statistical analysis, prepared the results and wrote the first version of the manuscript. HL and CJ contributed to the study methods and discussion. All authors reviewed and edited the manuscript. HZ and HW are the guarantors of this work and take responsibility for the contents of the article.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the medical ethics committee of the Shanghai YangZhi Rehabilitation Hospital (Shanghai Sunshine Rehabilitation Center) (No. YZ 2019-051). In addition, subjects who voluntarily participated in this program have informed and consented to the possible use of relevant health data for scientific research.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Detailed description of statistical methods.
Additional file 2.
eFigures and eTables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, Y., Wu, J., Wang, Y. et al. Association of blood pressure trajectories with coronary heart disease among the disabled population in Shanghai, China: a cohort study of 7 years following up. Eur J Med Res 28, 275 (2023). https://doi.org/10.1186/s40001-023-01240-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01240-1