
Abstract
To understand the mechanisms involved in the anti-obesity effects Centella asiatica (CA), we examined body weight, serum levels, white adipose tissue (WAT) weight, histological analysis, and the expression of cholesterol homeostasis- and lipid metabolism-related genes in mice with high-fat, high-sugar diet (HFHSD)-induced obesity that were orally treated with CA for 12 weeks. Eight-week-old, male C57BL/6J mice were assigned to the following four groups (8 mice/group): NOR, normal diet; HFHSD (Control), HFHSD; CA-L, HFHSD + CA 300 mg/kg; CA-H, HFHSD+CA 600 mg/kg. The suspension of powdered CA leaf was fed using oral gavage. CA treatment significantly attenuated HFHSD-induced increase in body weight gain, serum glucose, triacylglycerol, and WAT weight (p < 0.05). Compared to that in HFHSD, adipocyte diameter and macrovesicular area of epididymal WAT significantly decreased with CA treatment (p < 0.05). The mRNA expression levels of peroxisome proliferator-activated receptor gamma (PPARγ), fatty acid synthase (FAS), cluster of differentiation 36 (CD36), 3- hydroxyl-3-methylglutaryl CoA reductase (HMGCR), and stearoyl CoA desaturase 1 (SCD 1) were significantly downregulated in the CA-H compared to the HFHSD (p < 0.05). CA exerts anti-obesity effects by lowering body fat accumulation via regulating gene expression and thus, is a potential lipid-lowering agent.
Similar content being viewed by others


Introduction
Obesity, defined as accumulation of excessive body fat, is driven by an imbalance in energy input and expenditure [1, 2]. It is a medical condition that raises the risk of several diseases such as diabetes, stroke, heart ailments, arthritis, inflammation, and even cancer [3]. Since the introduction of medicines to treat obesity in the 1930s, various substances have been tested, although most were only marginally effective in lowering body weight, and some are no longer marketed owing to their side effects [4, 5]. Alternative and complementary medicine has gained increasing attention because of the unsatisfactory results and adverse reactions of medical intervention in obesity management [6, 7]. Epidemiological studies have recommended the use of plants to reduce the risk of obesity [8].
Plants are natural resources for medicine that exert no toxic or adverse effects. They synthesize hundreds of chemical compounds for various functions, including protection against fungi, insects, and disease. Medicinal plants, also known as medicinal herbs, have been discovered and used in traditional medicine since prehistoric times [9]. Numerous animal- and cell-based studies have been performed on medicinal plants and their active components to confirm their efficacy and mechanisms of action [10, 11].
Centella asiatica (CA) has been receiving widespread attention from researchers interested in both its phytochemical and biological properties [12, 13]. A perennial herbaceous plant belonging to the family Apiaceae, CA is a valuable medicinal herb mainly grown in swampy areas of India, China, Malaysia, Sri Lanka, Indonesia, Madagascar, and Korea. According to the Indian pharmacopeia, CA exhibits various therapeutic effects on psoriasis, diarrhea, fever, varicose ulcers, eczema, leprosy, lupus, and amenorrhea. Recent studies have reported various biological properties of CA, since it comprises several anti-oxidant, anti-inflammatory, anti-microbial, neuroprotective, memory improvement, and anti-depressant compounds [13,14,15,16]. Recent studies have shown that CA is effective for treating endocrine diseases, such as obesity, because it improves certain metabolic pathways and has fat-suppressing effects [17, 18]. There have been several claims regarding the underlying mechanisms involved in the anti-obesity effects of CA over the past few decades [19, 20]; however, more scientific data are needed to justify its ever-increasing use.
Some principal mechanisms of lipid metabolism are modulated by insulin signaling, adipogenesis, adipocyte differentiation, lipolysis, and β-oxidation of free fatty acid (FFA) in the obese state. Lipolysis refers to the degradation of triglyceride to yield FFA and glycerol. It can be induced by lipase, which are the direct transcriptional target of peroxisome proliferator activated receptor gamma (PPARγ) [21]. Excess FFA produced by lipolysis can migrate in the circulation and accumulate in the blood or the liver, resulting in upregulation of proteins involved in de novo lipogenesis, such as sterol regulatory element-binding protein (SREBP) and fatty acid synthase (FAS) [22]. Conversely, lipid accumulation can be reduced by upregulation of genes involved in β-oxidation of FFA in the adipose tissue and liver [23]. For this reason, controlling these factors has been an ideal therapeutic strategy to prevent or ameliorate obesity associated complications. Furthermore, the use of natural products as therapeutic agents in treating and preventing obesity has become popular [24]. Activated 5’adenosine monophosphate activated protein kinase (AMPK) triggers beneficial physiological effects, including reductions in fat deposition. AMPK knockdown upregulated FAS, and SREBP which is another key enzyme of fat synthesis [25]. The mechanistic study of CA on adipogenesis and lipolysis in white adipose tissue (WAT) in obese mice remains unresearched. Thus, in this study, we investigated its ameliorative effects in vivo to understand the underlying mechanisms involved in the anti-obesity effects of CA and provide scientific evidence to support CA as a supplement to prevent obesity. We examined body weight, serum levels, WAT weight, histological analysis, and the expression of cholesterol homeostasis- and lipid metabolism-related genes in obese mice treated orally with CA.
Materials and methods
Preparation of Centella asiatica (CA)
CA leaf was collected during early summer from Jeju (Republic of Korea) and provided by ASKBASE Co. (Seoul, Republic of Korea). Briefly, CA was cultivated in a pesticide-free greenhouse facility for 45 days. The harvested CA was immediately dried at 60 °C for 24 h in a forced-convection oven (VS-1202D4N; Vision Bionex, Bucheon, Korea). The dried CA leaf was pulverized using a food processor and passed through a 25-mesh sieve to collect CA particles than 0.70 mm. The dried and powdered CA leaf was weighed and suspended in distilled water. The CA leaf suspension was sonicated for 30 min in a water bath set at 37 °C just before feeding it.
Animals
Eight-week-old, C57BL/6J male mice were procured from Orient Bio (Seongnam, Korea). All animal use and euthanasia protocols were reviewed and approved by the Animal Care and Use Committee of Korea University (KUIACUC-2021-0098). In accordance with the institution’s guidelines, the mice were individually housed in stainless steel cages and were maintained in standard environmental conditions (temperature: 24 ± 1℃, humidity: 50–60%, and light-dark cycle: 12/12 hour). After one week acclimatization, 32 mice were randomly assigned to four groups (8 mice/group) and fed with either a normal diet or high-fat high-sugar diet (HFHSD, 45 kcal% fat and 32 kcal% sucrose) for 12 weeks as follows: Group 1: mice fed with normal diet (NOR), Group 2: mice fed with HFHSD (HFHSD), Group 3: mice fed with HFHSD along with 300 mg/kg CA leaf suspension treatment (CA-L), Group 4: mice fed with HFHSD along with 600 mg/kg CA leaf suspension treatment (CA-H). The composition of the experimental diets (normal diet and HFHSD) is shown in Table 1. The dosage of CA (300 mg/kg or 600 mg/kg) was determined based on previous studies in consideration of its effectiveness and safety [17, 26, 27]. The CA suspension (200 µl/mice) was fed using oral gavage with a ball-tip needle of the same volume every day.
Body weight and food consumption were monitored weekly. At the end of the experiment, the mice were starved for 12 h and sacrificed by CO2 asphyxiation. Blood samples were collected from inferior vena cava. Serum was separated by centrifugation at 3000g for 15 min at 4 °C. Serum glucose, triacylglycerol, and cholesterol levels were measured using FUJI DRI-CHEM 3500 (Fuji Photo Film, Osaka, Japan). After collecting blood, WAT (inguinal WAT, iWAT; mesenteric WAT, mWAT; epididymal WAT, eWAT) were removed and weighed immediately. They were then rinsed with phosphate-buffered saline, and stored at − 80 °C until analysis.
Histological analysis
Liver and eWAT were fixed in 10% neutral formalin for 42 h. The tissues were placed in cassettes, washed in phosphate-buffered saline with three changes, cleared in xylene for 30 min with two changes, and embedded in paraffin for 1 h with three changes. The tissues were blocked in paraffin and cut to 5 μm thickness. The sections were stained with hematoxylin and eosin (H&E) and viewed under a light microscope (Leica, Wetzlar, Germany). The tissues were photographed at 200× magnification. The diameter and macrovesicular area were evaluated using the ImageJ software (National Institutes of Health, Bethesda, MD, USA).
Quantitative real-time polymerase chain reaction (PCR)
Total RNA was extracted from the liver using Trizol reagent (Gibco-BRL, Grand Island, NY, USA), according to the manufacturer’s instructions. The extracted RNA was reverse-transcribed using Moloney murine leukemia virus transcriptase. The expression levels of genes of interest were determined from the synthesized cDNA using AccuPower GreenStar qPCR PreMix (Bioneer, Daejeon, Korea) on an Excycler 96 Real-Time Quantitative Thermal Block machine (Bioneer). The primer sequences used in the experiments is shown in Table 2. The PCR included the following steps: denaturing at 95 °C for 5 min followed by 50 cycles of 95 °C for 10 s, 60 °C for 40 s, and 72 °C for 10 s. Transcript concentrations were calculated as copies per µl using a standard curve. The mRNA expression was normalized to that of glyceraldehyde-3-phosphate dehydrogenase (GAPDH), and the results are presented as fold-changes relative to NOR.
Statistical analyses
Each result is expressed as mean ± standard error of mean (SEM). Statistical analyses were performed using the SPSS statistical analysis software (version 19.0; International Business Machines, Armonk, NY, USA). Differences between groups were evaluated statistically using one-way analysis of variance and Tukey’s multiple tests. Differences between the HFHSD and others were evaluated using Student’s t-test. Results with p < 0.05 were considered statistically significant.
Results
Body weight gain and food consumption
No signs of toxicity, such as piloerection, alterations in locomotor activity, diarrhea, or deaths, were recorded during the 12 weeks of oral CA treatment. Figure 1 illustrates the effect of CA on body weight gain in mice with HFHSD-induced obesity. The initial weights of the mice were 22.70 g (NOR), 22.71 g (HFHSD), 22.80 g (CA-L), and 22.76 g (CA-H). HFHSD triggered significant changes in body weight gain pattern, with the weight gain in mice fed with HFHSD being considerably higher than in mice fed with normal diet throughout the study (12th week, NOR 4.32 g vs. HFHSD 20.00 g, p < 0.001). The average daily food consumption was 2.48 g/day (NOR), 2.72 g/day (HFHSD), 2.58 g/day (CA-L), and 2.55 g/day (CA-H) (data not shown). Food consumption did not differ between groups during the experimental period. CA treatment showed a tendency to attenuate HFHSD-induced body weight gain. Despite comparable food consumption, body weight gain in the CA-L was suppressed significantly from week 10 compared to the HFHSD (10th week, CA-L 13.22 g vs. HFHSD 16.70 g, p < 0.01; 11th week, CA-L 15.24 g vs. HFHSD 18.98 g, p < 0.01, 12th week, CA-L 14.56 g vs. HFHSD 20.00 g, p < 0.001).

Body weight gains in mice with high-fat, high-sugar diet (HFHSD)-induced obesity treated orally with Centella asiatica (CA) for 12 weeks. Values are the means ± standard error of mean (SEM) for eight mice. The asterisk indicates a significant difference compared to HFHSD (**p < 0.01, ***p < 0.001). NOR, normal diet; HFHSD (Control), HFHSD; CA-L, HFHSD + CA 300 mg/kg; CA-H, HFHSD + CA 600 mg/kg
Serum glucose, triacylglycerol, and cholesterol
The effects of CA treatment on serum glucose, triacylglycerol, and cholesterol levels in HFHSD-induced obese mice are shown in Fig. 2. HFHSD induced significant increases in serum glucose (NOR 183.38 mg/dl vs. HFHSD 266.83 mg/dl, p < 0.001), triacylglycerol (NOR 92.00 mg/dl vs. HFHSD 139.20 mg/dl, p < 0.001), and cholesterol levels (NOR 45.38 mg/dl vs. HFHSD 86.80 mg/dl, p < 0.001). CA treatment attenuated HFHSD-induced increase in serum glucose and triacylglycerol levels. In particular, CA-H had significantly lower both of serum glucose (CA-H 216.86 mg/dl vs. HFHSD 266.83 mg/dl, p < 0.05) and triacylglycerol (CA-H 115.20 mg/dl vs. HFHSD 139.20 mg/dl, p < 0.05) than the HFHSD. However, there were no significant differences in serum cholesterol levels between the HFHSD and groups treated with CA.

Serum glucose, triacylglycerol, and cholesterol in mice with high-fat, high-sugar diet (HFHSD)-induced obesity orally treated with Centella asiatica (CA) for 12 weeks. Values are the means ± standard error of mean (SEM) for 8 mice. The asterisk indicates a significant difference compared to HFHSD (* p < 0.05, *** p < 0.001). NOR, normal diet; HFHSD (Control), HFHSD; CA-L, HFHSD + CA 300 mg/kg; CA-H, HFHSD + CA 600 mg/kg
Relative weights of WAT
The relative weights of the iWAT, mWAT, and eWAT were measured to examine the effect of CA treatment on body fat distribution. Figure 3 shows the relative weights of iWAT, mWAT, and eWAT in mice with HFHSD-induced obesity that were orally treated with CA for 12 weeks. All relative weights of WAT were significantly lower in mice fed on normal diet than in mice fed HFHSD (iWAT, NOR 5.74 mg/g vs. HFHSD 44.14 mg/g, p < 0.001; mWAT, NOR 11.89 mg/g vs. HFHSD 25.33 mg/g, p < 0.001; eWAT, NOR 12.93 mg/g vs. HFHSD 57.76 mg/g, p < 0.001). Although CA treatment did not affect mWAT, it tended to lower the volume of iWAT and eWAT; CA treatment significantly reduced the relative weight of iWAT in mice with HFHSD-induced obesity (CA-L 37.30 mg/g vs. HFHSD 44.14 mg/g, p < 0.05; CA-H 36.36 mg/g vs. HFHSD 44.14 mg/g, p < 0.01) and relative weight of eWAT in CA-L group was significantly lower than that in the HFHSD (CA-L 48.65 mg/g vs. HFHSD 57.76 mg/g, p < 0.01).

Relative weight of white adipose tissue (WAT) in mice with high-fat, high-sugar diet (HFHSD)-induced obesity that were orally treated with Centella asiatica (CA) for 12 weeks. Values are the means ± standard error of mean (SEM) for eight mice. The asterisk indicates a significant difference compared to HFHSD (* p < 0.05, ** p < 0.01, *** p < 0.001). NOR, normal diet; HFHSD (Control), HFHSD; CA-L, HFHSD + CA 300 mg/kg; CA-H, HFHSD + CA 600 mg/kg. iWAT, inguinal WAT; mWAT, mesenteric WAT; eWAT, epididymal WAT.
Microphotographic observations
As illustrated in Fig. 4A, large macrovascular adipocytes were observed in the liver tissue of the HFHSD compared with those in the NOR. However, CA treatment markedly reduced hepatic steatosis in mice with HFHSD-induced obesity. The adipocyte size of eWAT in mice with HFHSD-induced obesity also increased compared to that in mice fed a normal diet (Fig. 4B). In the groups treated orally with CA, we observed a marked reduction in adipocyte hypertrophy compared to the HFHSD. The histological analysis of eWAT in HFHSD-induced obese mice treated orally with CA is shown in Fig. 4C. There was a significant increase in the adipocyte diameter of eWAT in mice fed on HFHSD compared to those fed on normal diet (NOR 39.50 μm vs. HFHSD 104.83 μm, p < 0.001). HFHSD also caused a significant increase in the macrovesicular area of eWAT compared to the normal diet (NOR 100% vs. HFHSD 841.51%, p < 0.001). CA treatment attenuated HFHSD-induced increase in adipocyte size in eWAT. In particular, CA-H had significantly smaller adipocyte diameter in eWAT than the HFHSD (CA-H 80.50 μm vs. HFHSD 104.83 μm, p < 0.001). Compared to that in the HFHSD, macrovesicular area of eWAT was decreased following CA treatment (CA-L 428.54% vs. HFHSD 841.51%, p < 0.05; CA-H 458.84% vs. HFHSD 841.51%, p < 0.05).

Microphotographic observation in mice with high-fat, high-sugar diet (HFHSD)-induced obesity that were orally treated with Centella asiatica (CA) for 12 weeks. The liver tissue (A) and epididymal white adipose tissue (eWAT) (B) were stained with hematoxylin and eosin (H&E), and viewed under a microscope (×200) (scale bar = 100 μm). The diameter and macrovesicular area of eWAT (C) were evaluated using ImageJ. Values are the means ± standard error of mean (SEM) for eight mice. The asterisk indicates a significant difference compared to HFHSD (* p < 0.05, *** p < 0.001). NOR, normal diet; HFHSD (Control), HFHSD; CA-L, HFHSD + CA 300 mg/kg; CA-H, HFHSD+CA 600 mg/kg
mRNA expression profile
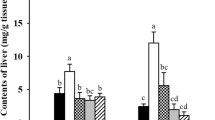
We evaluated the effects of CA on cholesterol homeostasis- and lipid metabolism-related genes by analyzing mRNA expression in liver tissue using quantitative real-time PCR (Fig. 5). The mRNA expression levels of PPARγ, FAS, CD36, SREBP-2, HMGCR, SREBP-1 C, LDLR, and SCD1 were significantly higher in mice with HFHSD-induced obesity than in mice fed a normal diet (p < 0.001). In mice with HFHSD-induced obesity that were orally treated with CA, the mRNA expression levels of PPARγ, FAS, CD36, HMGCR, and SCD1 were downregulated in a dose-dependent manner; in the CA-H, the mRNA expression levels of PPARγ, FAS, CD36, HMGCR, and SCD 1 were significantly decreased compared to those in the HFHSD (PPARγ, CA-H 2.36 vs. HFHSD 3.66, p < 0.01; FAS, CA-H 2.36 vs. HFHSD 3.78, p < 0.01; CD36, CA-H 3.90 vs. HFHSD 5.41, p < 0.05; HMGCR, CA-H 2.64 vs. HFHSD 4.36, p < 0.01; SCD1, CA-H 2.90 vs. HFHSD 5.87, p < 0.001). During CA treatment, SREBP-2 expression was slightly reduced in the groups treated orally with CA compared to that in the HFHSD, without significant differences. In this study, we did not observe any effect of CA treatment on SREBP-1 C or LDLR in mice with HFHSD-induced obesity.

Relative mRNA expression in liver tissues of mice with high-fat, high-sugar diet (HFHSD)-induced obesity that were orally treated with Centella asiatica (CA) for 12 weeks. Values are the means ± standard error of mean (SEM) for eight mice. The asterisk indicates a significant difference compared to HFHSD (* p < 0.05, *** p < 0.001). The mRNA levels of the target genes were normalized to the expression level of glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and the results are presented as the fold changes relative to the NOR. NOR normal diet, HFHSD (Control) HFHSD, CA-L HFHSD+CA 300 mg/kg, CA-H HFHSD+CA 600 mg/kg, PPARγ peroxisome proliferator activated receptor gamma, FAS fatty acid synthase, CD36 cluster of differentiation 36, AMPK 5ʹadenosine monophosphate activated protein kinase, SREBP-2 sterol regulatory element-binding protein 2, HMGCR 3- hydroxyl-3-methylglutaryl CoA reductase, SREBP-1C sterol regulatory element-binding protein 1C, LDLR low-density lipoprotein receptor, SCD1 stearoyl CoA desaturase 1
We also investigated the status of AMPK, which plays a role in cellular energy homeostasis by activating fatty acid uptake and oxidation when cellular energy is low. In mice with HFHSD-induced obesity, AMPK level was markedly reduced compared to mice fed with a normal diet (NOR 1.00 vs. HFHSD 0.22, p < 0.001). AMPK levels were marginally higher in the groups treated orally with CA than the HFHSD; however, the differences were not statistically significant.
Discussion
HFHSD contains high proportions of sugar and saturated fats, which accumulate in fat pads across body and promotes excessive WAT development [28]. HFHSD results in an increase in body weight and serum comorbidity factors. CA is considered useful in the treatment of obesity [29, 30]. Abas et al. [31] reported that long-term treatment of obese rats with CA reversed plasma glucose and lipid levels as well as the tricarboxylic acid cycle and amino acid metabolic disorders, returning them to normal states. Based on biochemical analysis, they concluded that CA exerts anti-obesity effects and modulates specific metabolic pathways. Available evidence shows that CA can inhibit body weight gain, lower plasma glucose levels, and reduce oxidative stress [32]. The potential of CA as an anti-obesity agent has been proven by the fact that it suppresses lipid levels and enhances sensitivity to leptin and insulin. At the molecular level, CA can also increase levels of enzymatic antioxidants, such as superoxide dismutase (SOD), glutathione peroxidase (GPX), and catalase, and reverse the expression of palmitoyltransferase-1 and uncoupling protein-2. In an animal model of obesity, CA increased the activities of SOD, GSH, and catalase, thereby improving the enzyme anti-oxidant system [18, 20]. Therefore, it can be deduced that CA alleviates obesity-driven oxidative stress, and suppress body weight gain by promoting fatty acid oxidation [18]. The anti-obesity effect of CA seems to be due to the effect of madecassic acid. It has been reported that madecassic acid reduces triacylglycerol levels, suppresses lipogenesis in mesenteric fat, promote epididymal lipolysis and fatty acid oxidation [33]. In the present study, CA treatment significantly attenuated HFHSD-induced increases in body weight (p < 0.01) and serum glucose and triacylglycerol levels (p < 0.05). This study confirms the results of previous studies, and our results suggest that CA can attenuate diet-induced hyperlipidemia and hyperglycemia.
Recent studies have shown that CA affects pre-adipocyte differentiation and lipid accumulation by regulating the expression of adipogenic beta-oxidation and lipolysis metabolism-related genes, which are early transcription factors involved in pre-adipocyte differentiation [33, 34]. Previous studies reported the effect of CA on pre-adipocyte differentiation and found that adipocyte accumulation decreased in a dose-dependent manner when pre-adipocytes were treated with CA [18, 35, 36].
We stained the liver tissue (Fig. 4A) and WAT (Fig. 4B) with H&E, and viewed under a microscope. Then to understand the mechanisms involved in the anti-obesity effects of CA in liver tissue and WAT, we evaluated the expression of cholesterol homeostasis- and lipid metabolism-related genes in liver tissues (Fig. 5) and the diameter and macrovesicular area of adipocyte in WAT (Fig. 4C). We confirmed that CA treatment significantly decreased WAT weight in mice with HFHSD-induced obesity (p < 0.05). Moreover, CA treatment markedly reduced hepatic steatosis and adipocyte hypertrophy in these mice. Furthermore, the adipocyte diameter and macrovesicular area of eWAT decreased with CA treatment compared to those in the HFHSD (p < 0.05). Another important finding of our study was that CA may affect cholesterol homeostasis and lipid metabolism in mice with HFHSD-induced obesity. Although consistent results were not produced, CA 300 mg/kg treatment prevented weight gain more than CA 600 mg/kg treatment, and showed better effects on some anti-obesity indicators in liver tissue and WAT. It is thought that CA does not have an anti-obesity effect on a dose-dependent manner and, like other herbal medicines [37, 38], has an appropriate dose for anti-obesity. In this study, the expression levels of cholesterol homeostasis- and lipid metabolism-related genes in the liver revealed that CA treatment significantly attenuated the mRNA expression levels of PPARγ, FAS, CD36, HMGCR, and SCD1 in mice with HFHSD-induced obesity (p < 0.05). CA treatment upregulates lipid oxidation-related genes and downregulates transcription factors that regulate adipocyte differentiation. Therefore, we hypothesized that CA contributes to the inhibition of preadipocyte differentiation by regulating cholesterol homeostasis- and lipid metabolism-related genes. It is likely that the anti-obesity effects of CA treatment are due to the regulation of gene expression in the liver.
CA treatment markedly ameliorated body fat accumulation in mice with HFHSD-induced obesity and reduced their body weight gain, serum glucose, triacylglycerol, WAT weight, and adipocyte size. Furthermore, CA exerts anti-obesity effect by lowering body fat accumulation via regulating the expression of cholesterol homeostasis- and lipid metabolism-related genes in the liver. Thus, we conclude that CA has beneficial lipid-lowering capacity and may be a useful agent for preventing obesity. Additional investigations are required to determine the chemical identities of the bioactive constituents of CA (Additional file 1).
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- AMPK:
-
5ʹAdenosine monophosphate activated protein kinase
- CA:
-
Centella asiatica
- CD36:
-
Cluster of differentiation 36
- eWAT:
-
Epididymal white adipose tissue
- FAS:
-
Fatty acid synthase
- GAPDH:
-
Glyceraldehyde-3-phosphate dehydrogenase
- GPX:
-
Glutathione peroxidase
- H&E:
-
Hematoxylin and eosin
- HFHSD:
-
High-sugar diet
- HMGCR:
-
3-Hydroxyl-3-methylglutaryl CoA reductase
- iWAT:
-
Inguinal white adipose tissue
- LDLR:
-
Low-density lipoprotein receptor
- mWAT:
-
Mesenteric white adipose tissue
- PPARγ:
-
Peroxisome proliferator activated receptor gamma
- SCD1:
-
Stearoyl CoA desaturase 1
- SEM:
-
Standard error of mean
- SOD:
-
Superoxide dismutase
- SREBP-1C:
-
Sterol regulatory element-binding protein 1C
- SREBP-2:
-
Sterol regulatory element-binding protein 2
- WAT:
-
White adipose tissue
References
Powell Wiley TM, Poirier P, Burke LE et al (2021) Obesity and cardiovascular disease: a scientific statement from the American heart association. Circulation 143(21):E984–E1010. https://doi.org/10.1161/Cir.0000000000000973
Mohajan D, Mohajan HK (2023) Body mass index (BMI) is a popular anthropometric tool to measure obesity among adults. J Innov Med Res 2(4):25–33. https://doi.org/10.56397/JIMR/2023.04.06
Mohajan D, Mohajan HK (2023) Obesity and its related diseases: a new escalating alarming in global health. J Innov Med Res 2(3):12–23. https://doi.org/10.56397/JIMR/2023.03.04
Mauer Y, Parker M, Kashyap SR (2021) Antiobesity drug therapy: an individualized and comprehensive approach. Cleve Clin J Med 88(8):440–448. https://doi.org/10.3949/ccjm.88a.20080
Onakpoya IJ, Heneghan CJ, Aronson JK (2016) Post-marketing withdrawal of anti-obesity medicinal products because of adverse drug reactions: a systematic review. BMC Med 14:1–11. https://doi.org/10.1186/s12916-016-0735-y
Chang YH, Hung HY (2022) Recent advances in natural anti-obesity compounds and derivatives based on in vivo evidence: a mini-review. Eur J Med Chem 237(5):114405. https://doi.org/10.1016/j.ejmech.2022.114405
Li SZ, Zeng SL, Liu EH (2021) Anti-obesity natural products and gut microbiota. Food Res Int 151:110819. https://doi.org/10.1016/j.foodres.2021.110819
Saad B, Kmail A, Haq SZ (2022) Anti-diabesity middle eastern medicinal plants and their action mechanisms. Evid Based Complement Alternat Med. https://doi.org/10.1155/2022/2276094
Kazemipoor M, Cordell GA, Sarker MMR et al (2015) Alternative treatments for weight loss: Safety/risks and effectiveness of anti-obesity medicinal plants. Int J Food Prop 18(9):1942–1963. https://doi.org/10.1080/10942912.2014.933350
Zhang JH, Onakpoya IJ, Posadzki P et al (2015) The safety of herbal medicine: from prejudice to evidence. Evid Based Complement Alternat Med. https://doi.org/10.1155/2015/316706
Aloo SO, Ofosu FK, Kim NH et al (2023) Insights on dietary polyphenols as agents against metabolic disorders: obesity as a target Disease. Antioxidants 12(2):416. https://doi.org/10.3390/antiox12020416
Oyenihi A, George T, Oyenihi O et al (2023) Three decades of research on Centella asiatica: insights and future trends from bibliometric analysis. J Herb Med. https://doi.org/10.1016/j.hermed.2023.100662
Prakash V, Jaiswal N, Srivastava M (2017) A review on medicinal properties of Centella asiatica. Asian J Pharm Clin Res 10(10):69–74. https://doi.org/10.22159/ajpcr.2017.v10i10.20760
Nora EG, Christopher JH, Joseph FQ et al (2016) Centella asiatica modulates antioxidant and mitochondrial pathways and improves cognitive function in mice. J Ethnopharmacol 180(2):78–86. https://doi.org/10.1016/j.jep.2016.01.013
Nasution MY, Restuati M, Pulungan ASS et al (2018) Antimicrobial activities of Centella asiatica leaf and root extracts on selected pathogenic micro-organisms. J Med Sci 18(4):198–204. https://doi.org/10.3923/jms.2018.198.204
Sultan RA, Mahmood SBZ, Ahmed SW et al (2014) Biological activities Assessment of Centella asiatica (Linn. J Herbs Spices Med Plants 20:319–327. https://doi.org/10.1080/10496475.2013.869521
Gohil KJ, Patel JA, Gajjar AK (2010) Pharmacological review on Centella asiatica: a potential herbal cure-all. Indian J Pharm Sci 72(5):546–556. https://doi.org/10.4103/0250-474X.78519
Rameshreddy P, Uddandrao VVS, Brahmanaidu P et al (2018) Obesity-alleviating potential of asiatic acid and its effects on ACC1, UCP2, and CPT1 mRNA expression in high fat diet-induced obese Sprague-Dawley rats. Mol Cell Biochem 442(1–2):143–154. https://doi.org/10.1007/s11010-017-3199-2
Rao SB, Chetana M, Devi PU (2005) Centella asiatica treatment during postnatal period enhances learning and memory in mice. Physiol Behav 86(4):449–457. https://doi.org/10.1016/j.physbeh.2005.07.019
Masola B, Oguntibeju OO, Oyenihi AB (2018) Centella asiatica ameliorates diabetes-induced stress in rat tissues via influences on antioxidants and inflammatory cytokines. Biomed Pharmacother 101:447–457. https://doi.org/10.1016/j.biopha.2018.02.115
Yajima H, Kobayashi Y, Kanaya T et al (2007) Identification of peroxisome-proliferator responsive element in the mouse HSL gene. Biochem Biophys Res Commun 352(2):526–531. https://doi.org/10.1016/j.bbrc.2006.11.054
Lee YJ, Ko EH, Kim JE et al (2012) Nuclear receptor PPARγ–regulated monoacylglycerol O-acyltransferase 1 expression is responsible for the lipid accumulation in diet-induced hepatic steatosis. Proc Natl Acad Sci 109(34):13656–13661. https://doi.org/10.1073/pnas.1203218109
Den Besten G, Bleeker A, Gerding A et al (2015) Short-chain fatty acids protect against high-fat diet-induced obesity via a PPARγ–dependent switch from lipogenesis to fat oxidation. Diabetes 64(7):2398–2408. https://doi.org/10.2337/db14-1213
Petrovska BB (2012) Historical review of medicinal plants’ usage. Pharmacogn Rev 6(11):1–5. https://doi.org/10.4103/0973-7847.95849
Yang CS, Zhang J, Zhang L et al (2016) Mechanisms of body weight reduction and metabolic syndrome alleviation by tea. Mol Nutr Food Res 60(1):160–174. https://doi.org/10.1002/mnfr.201500428
Yadav MK, Singh SK, Singh M et al (2019) In vivo toxicity study of ethanolic extracts of Evolvulus alsinoides & Centella asiatica in Swiss albino mice. Maced J Med Sci 15(7):1071–1076. https://doi.org/10.3889/oamjms.2019.209
Sari DCR, Arfian N, Tranggono U et al (2019) Centella asiatica (Gotu Kola) ethanol extract up-regulates hippocampal brain-derived neurotrophic factor (BDNF), tyrosine kinase B (TrkB) and extracellular signal-regulated protein kinase 1/2 (ERK1/2) signaling in chronic electrical stress model in rats. Iran J Basic Med Sci 22(10):1218–1224. https://doi.org/10.22038/ijbms.2019.29012.7002
Naidu PB, Uddandrao VVS, Naik RR et al (2016) Ameliorative potential of gingerol: promising modulation of inflammatory factors and lipid marker enzymes expressions in HFD induced obesity in rats. Mol Cell Endocrinol 419(C):139–147. https://doi.org/10.1016/j.mce.2015.10.007
Adtani PN, Narasimhan M, Punnoose AM et al (2017) Antifibrotic effect of Centella asiatica Linn and asiatic acid on arecoline-induced fibrosis in human buccal fibroblasts. J Invest Clin Dent 8(2):1–9. https://doi.org/10.1111/jicd.12208
Begum SA, Swamy K (2019) Studies on the anti-obesity activity of ethanolic extract of Centella asiatica in Triton-X, high fat diet and progesterone induced obesity. Am J PharmTech Res 9:118–132. https://doi.org/10.46624/ajptr.2019.v9.i4.011
Abas F, Khatib A, Perumal V et al (2016) Metabolic alteration in obese Diabetes rats upon treatment with Centella asiatica extract. J Ethnopharmacol 180:60–69. https://doi.org/10.1016/j.jep.2016.01.001
Sun B, Wu L, Wu Y et al (2020) Therapeutic potential of Centella asiatica and its triterpenes. Front Pharmacol 11:568032. https://doi.org/10.3389/fphar.2020.568032
Sun BJ, Hayashi MS, Kudo MY et al (2021) Madecassoside Inhibits body weight gain via modulating SIRT1-AMPK signaling pathway and activating genes related to thermogenesis. Front Endocrinol. https://doi.org/10.3389/fendo.2021.627950
Gooda Sahib N, Saari N, Ismail A et al (2012) Plants’ metabolites as potential antiobesity agents. Sci World J. https://doi.org/10.1100/2012/436039
Kumari S, Deori M, Elancheran R (2016) In vitro and In vivo antioxidant, anti-hyperlipidemic properties and chemical characterization of Centella asiatica (L.) extract. Front Pharmacol 7:400
Maulidiani AF, Khatib A et al (2016) Metabolic alteration in obese Diabetes rats upon treatment with Centella asiatica extract. J Ethnopharmacol 180:60–69. https://doi.org/10.1016/j.jep.2016.01.001
Lim HH, Yang SJ, Kim Y et al (2013) Combined treatment of mulberry leaf and fruit extract ameliorates obesity-related inflammation and oxidative stress in high fat diet-induced obese mice. J Med Food 16(8):673–680. https://doi.org/10.1089/jmf.2012.2582
Lim HH, Lee SO, Kim SY et al (2013) Anti-inflammatory and antiobesity effects of mulberry leaf and fruit extract on high fat diet-induced obesity. Exp Biol Med (Maywood) 238(10):1160–1169. https://doi.org/10.1177/1535370213498982
Acknowledgements
Not applicable.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, HJS and EYJ; formal analysis, YBC and YA; Investigation, DS, SB and YHH; methodology, HJS, DS and EYJ; writing-original draft, YBC, YA, DD, SB and YHH; writing-editing. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Relative weight of organs in mice with high-fat, high-sugar diet (HFHSD)-induced obesity that were treated orally with Centella asiatica (CA) for 12 weeks.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chang, Y.B., Ahn, Y., Seo, D. et al. Centella asiatica lowers body fat accumulation via regulating cholesterol homeostasis- and lipid metabolism-related genes in mice with high-fat, high-sugar diet-induced obesity. Appl Biol Chem 66, 88 (2023). https://doi.org/10.1186/s13765-023-00846-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13765-023-00846-7