
Abstract
Background
Recently, electronic cigarette (e-cig) usage has increased significantly, making it a potentially effective smoking cessation tool. In Muslim countries, most people who use e-cigarettes fast the month of Ramadan, which results in intermittent fasting. This study aims to reveal the severity of e-cig withdrawal symptoms among users during this intermittent fasting period.
Methods
A self-administered survey was developed and validated to solicit anonymous responses from e-cig users living in Jordan, through a cross-sectional study design. Participants were recruited through social media resources. Severity scores of physical (out of 11) and psychological (out of 8) withdrawal symptoms for each participant were assessed and calculated for each participant, depending on the symptoms reported.
Results
A convenience sample (n = 523) of e-cig adult users were recruited. The majority of the participants were males (96.4%) aged between 18 and 40 years (86.4%). Many participants replaced tobacco smoking with e-cig (53.5%) in order to help them stop smoking. More than half of the participants experienced relatively weak physical (0.82 ± 1.78) and psychological (1.24 ± 1.89) withdrawal symptoms during the month of fasting. Most of the participants (63.2%) preferred to engage themselves with a busy schedule to tolerate the related withdrawal symptoms they experienced.
Conclusion
E-cigs could play a vital role in smoking cessation among tobacco smokers during intermittent fasting. Ramadan offers a good opportunity for smokers to quit, as the reported physical and psychological e-cig withdrawal symptoms were found to be relatively weak. Awareness and behavioral interventions would help clarify the effect of e-cigs and help determine alternative ways to cease smoking.
Similar content being viewed by others


Background
Worldwide, electronic cigarettes (e-cig) usage has increased significantly in recent years, and it has been proposed as a potentially effective smoking cessation tool [1]. E-cig devices are defined as “a group of products that produce a heated aerosol, typically containing nicotine, which users inhale via a mouthpiece” [2]. E-cig usage has followed different patterns over the years, including dual use of tobacco and e-cigs among smokers, use by non-smoking youth, and young-adult smokers who have switched to the sole use of the e-cig [1]. Recently, the overall current prevalence of e-cig use in different countries has ranged from 2.8 to 3.2% [3], while, the prevalence of e-cig use in Jordan has been found to be much higher than that reported in other countries, ranging from 18 to 27.3%, with 50.9% replacing tobacco with e-cigs [4, 5]. According to a government study carried out by the Jordan health ministry in collaboration with the World Health Organization in 2019, 8 out of 10 Jordanian men smoke or regularly use nicotine products, including s-cigs [6]. With the exclusion of e-cig use and other smokeless patterns, research has shown that 66% of Jordanian men and more than 17% of women are smokers [6, 7].
Nicotine is widely known as a psychoactive drug and it is highly addictive [8]. Many nicotine smokers use smoking cessation products to stop smoking [8]. The main addictive component in many e-liquids used in e-cigs (referred to as vaping) is nicotine [1]. Thus, e-cigs can also lead to nicotine addiction for tobacco non-smoker adults and youth [1]. In addition, e-cigs may increase the severity of nicotine dependence in dual-users of cigarettes [1].
The long-term effects of e-cig use as a smoke cessation tool are debatable and have become a public health concern [9]. Furthermore, little is known about how vaping affects the use of and dependence on tobacco cigarettes, nor is much known regarding total nicotine use and dependence. Access to such information is vital when assessing the influence of vaping on smoke cessation and other health-related outcomes [10]. The onset, duration, and intensity of nicotine withdrawal symptoms depend on the smoking duration, the number of milliliters of the e-liquids consumed, and the concentration of the nicotine included. Hence, symptoms of withdrawal can last from several days to several weeks [10].
Different types of e-cig devices are currently available on the market, including the box mod, vape-pen, vape-pod and other different types [11]. E-cig devices have a specific e-liquid that is used to provide different concentrations of nicotine [12]. No previous study has looked into the severity of the withdrawal symptoms experienced by e-cig users in months of fasting. Ramadan is the holy fasting month for Muslims all around the world. Many things are prohibited during fasting time (from sunrise to sunset) including food, drink and smoking [13]. This month is known to be full of spirituality, religious worship and self-control [13]. During the month of Ramadan, people who follow the faith of Islam fast around 16 h a day. Ideally, this month is supposed to be a good chance for smokers to quit smoking [14]. Hence, this study is the first study conducted in Jordan that aims to evaluate the severity of e-cig withdrawal symptoms during intermittent fasting, particularly during Ramadan.
Materials and methods
Study design and participants
The study followed a descriptive cross-sectional design and the objectives were addressed via an online survey. The study was conducted in Jordan from 26 April to 15 June 2020. The online survey was developed and validated by clinical researchers to solicit anonymous responses, which were treated confidentially. Eligible participants included e-cig users who had experienced intermittent fasting, such as Ramadan. They could be of any nationality but must reside in Jordan. The inclusion criteria were explained upfront at the start of the survey (Additional file 1: Appendix S1). Participants were recruited through social media platforms: Facebook, WhatsApp, LinkedIn, and Twitter. Participants were also advised that their participation in the study was voluntary and that their participation did not pose any risks. Potential participants who completed the survey were considered to have given informed consent for participation.
Survey development, validation, and reliability
The online survey was developed after reviewing similar validated surveys in the literature [15, 16] and was designed using the general principles of good survey design [17]. Several sources were used to generate a pool of questions considered to be relevant to the study objectives [15,16,17,18]. The online survey was finally prepared using the technology of Google Forms, and although it was constructed in English, it was delivered to the participants in Arabic—the formal language of Jordan. The survey contained multiple-choice questions and was designed to be completed within 10 min.
To ensure face validity, the first draft of the survey was evaluated by fifteen independent academics who had previous experience in smoking and vaping related work and research studies; a statistician was also involved at this stage of evaluation. The comments and feedback they provided were considered and incorporated where appropriate to prepare the final version of the survey. The survey was then translated from English into Arabic, and was then back-translated by two senior academic staff members who were considered fluent in both languages. Survey piloting took place to determine words that do not translate particularly well, words that are ambiguous, and whether or not another word or phrase would work better, and further, to confirm if the survey items were clearly presented. The questions were free from medical jargon or difficult terminology. To help the participants report accurate data, the popular types of e-cig devices were mentioned in the survey in the form of images, to help participants recognize the type of e-cig device they were using. Finally, the survey was piloted with a sample of 25 academic and 25 non-academic participants. This stage of the study was conducted to enhance clarity, readability, understandability, and confirm the study’s applicability to the Jordanian population. Internal consistency reliability was tested by the Cronbach’s alpha coefficient, which equaled to 0.88.
The final version of the survey contained three parts. The first part (Part A) comprised of nine questions, which included sociodemographic information; the second part (Part B) consisted of seven questions comprising details of participants’ use of e-cigs; the third part (Part C) consisted of 11 physical and 8 psychological withdrawal symptoms. The scores were assessed for each participant depending on the symptoms reported during the month of fasting, i.e. Ramadan. The participants were also asked to estimate the severity of withdrawal symptoms during the fasting month, using a score of severity (0–5). The severity reported by participants was rated as weak (score = 1) to very severe (score = 5). Participants were also asked to report the time their withdrawal symptoms started since their last e-cig use (in hours).
Sample size
The most recent demographic statistics of citizens living in Jordan showed that 10.554 million people live in the country [19]. Based on that, the sample size was calculated using a margin of error of 5%, a confidence level of 95%, and a response distribution of 50%, giving a minimum sample size of 385 [20]. It was decided that the number should be increased to around 600 to take into account missing responses and other unknown issues that might arise.
Statistical analyses
Completed surveys were extracted from Google Forms as an Excel sheet and were then exported to Statistical Package for Social Sciences version 24.0 (SPSS Inc., Chicago, IL, USA) for the statistical analysis. Descriptive statistics included percentages, means and frequency distribution, which were calculated for each question. Descriptive and univariate correlation analyses using Pearson correlation coefficient (r) were used for the correlation, which was conducted at a 5% significance level. A p-value of < 0.05 represented a significant difference. Factors affecting the severity scores of withdrawal symptoms were analyzed using simple and multivariant linear regression.
Results
Participant characteristics
Sociodemographic characteristics
Out of the total completed questionnaires (n = 610), eighty-seven forms (14.3%) were excluded from the main study measures due to missing data. Accordingly, 523 (85.7%) of the answered questionnaires were included in the study analysis. The majority of the participants were men (n = 504, 96.4%), and had a wide age-range with the highest percentage (48.2%) aged 26–40 years (Table 1). More than half of the participants (55.6%) were Jordanian in nationality and had a bachelor's university degree (n = 305, 58.3%). Only 7.6% (n = 40) of the study participants worked in the health sector, while others (n = 171, 32.7%) were employed in the non-health sector. More than half (n = 280, 53.5%) of the participants were single, while, (n = 241, 46.1%) were married and 41.3% had children.
Information related to e-cigarette usage
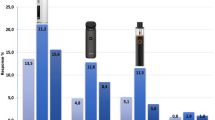
Upon asking the study participants about the main reason behind their use of e-cigarettes, more than half (n = 297, 56.8%) reported smoking cessation as a reason (Table 2). Others (n = 157, 30.0%) stated that the e-cig has a better smell and taste than tobacco cigarettes. The percentage of participants who replaced tobacco smoking with e-cigs (n = 280, 53.5%) was significantly (p < 0.05) higher than both dual e-cig users (e-cig with tobacco smoking) and sole e-cig users. Many (n = 307, 58.6%) participants believed that the e-cig has the capability to reduce their desire for tobacco smoking and helped them cease tobacco smoking (Fig. 1).

The percentage of E-cig users who replaced or combine tobacco smoking (n = 373)
The most commonly used e-cig device, as reported by the participants, was the ‘Box-mod’ (64.1%), followed by the ‘Vape pod’ (17.2%), then other types such as Ciga-like (10.9%) and ‘Vape pen’ (7.8%). More than half (54.1%) of the participants consumed between 2.0 to 5.0 mL/day of the e-liquid. The majority (n = 416, 79.5%) of the participants used unsalted nicotine-containing e-liquid (Fig. 2). The majority of those users (n = 191, 36.6%) consumed 2–5 mL/day of the 3 mg/mL nicotine-containing e-liquids. Hence, the daily nicotine consumption ranged between 6.0 and 15.0 mg/day. Other e-cig users (17.2%) used a salted nicotine-containing e-liquid, which was consumed using the ‘vape mod’ device.

Summary for types of consumed E-liquids and the most common used concentrations of nicotine among the participants (n = 523)
E-cigarette withdrawal symptoms during fasting time
More than half of the e-cig users experienced both physical (55.1%) and psychological (53.0%) withdrawal symptoms during the fasting month of Ramadan. The most common physical withdrawal symptoms (Table 3) experienced by the participants included heart palpitations (10.3%), dizziness (10.5%), headaches (10.5%) and nausea (10.8%). Intense cravings (29.6%) and restlessness (22.5%) were the most common psychological withdrawal symptoms reported by the participants. Severity scores for both the physical (score out of 11) and psychological (score out of 8) withdrawal symptoms equaled 0.82 ± 1.78 and 1.24 ± 1.89, respectively. Those results indicated that most of the study participants experienced a relatively weak severity of withdrawal symptoms. Upon asking the participants to estimate the severity of withdrawal symptoms during fasting time using a score of severity (0–5, weak-sever) (Table 4), more than half (n = 288, 53%) of the e-cig users reported that the severity of withdrawal symptoms ranged between weak (score of 1, 20.1%) to very severe (score of 5, 0.8%). Some participants (15.9%; n = 81) reported that the withdrawal symptoms started in less than 6 h since their last e-cig use, while 15.5% (n = 81) started to feel the withdrawal symptoms after more than 16 h.
Multivariable linear regression outcome (Table 5) showed a positive significant correlation (p ≤ 0.001) between the severity of physical and psychological withdrawal symptoms and the daily consumed nicotine concentration.
Participants responses upon experiencing e-cig withdrawal symptoms during fasting
Most of the participants (63.2%, n = 182) who suffered from withdrawal symptoms during the fasting month of Ramadan attempted to keep themselves busy to tolerate the withdrawal symptoms. Others (24.7%, n = 71) preferred to go back to tobacco smoking instead of e-cigs once they broke their fasting. Only 2.1% (n = 6) of the participants took advice from a pharmacist or other healthcare provider regarding their withdrawal symptoms. A small number of participants (1.4%) preferred using nicotine replacement therapy.
Discussion
Globally, the prevalence of tobacco smoking increases greatly every year, which is associated with significantly high rates of mortality and morbidity [21]. In Jordan, recent statistics have shown that the tobacco smoking rate among the population is one of the highest rates in the world [22]. The use of e-cigs and their popularity has been well documented in the last few years worldwide. Specifically in Jordan, it is considered an innovative smoking tool that is sold as an alternative to traditional tobacco cigarettes. This cross-sectional study is the first to reveal the severity of e-cig related physical and psychological withdrawal symptoms during the fasting month of Ramadan among the general Jordanian population. Factors affecting these withdrawal symptoms have also been revealed. The majority of the participants were men who were using e-cigs for the purpose of smoking cessation. More than half of the e-cig users experienced physical and psychological withdrawal symptoms during intermittent fasting, particularly during Ramadan, including heart palpitations, dizziness, headaches, and nausea. However, the severity of these withdrawal symptoms was found to be relatively weak. A significant correlation was found between the severity of the physical and psychological withdrawal symptoms and daily consumed nicotine concentration.
Predictably, the majority of the study participants were men. Previous studies have shown a significant correlation between e-cig use and male gender due to different factors including smoking cessation, health care, and enjoyment purposes having a higher influence on men than women [4, 23]. Moreover, this finding could be related to the Jordanian cultural acceptance of public smoking for males only [24]. The usage of e-cigarettes among females, on the other hand, could be related more to recommendations from the surrounding milieu (family and friends), and psychological related causes such as stress and mood management [23].
Interestingly, the findings of this study showed that more than half of the e-cig users completely replaced tobacco smoking with e-cigs and were aiming to quit smoking via e-cig vaping. A study conducted by Berry et al. in 2019 showed that e-cig users were successful at quitting or reducing their tobacco smoking using e-cigarettes as a smoking cessation tool [25]. Besides, one-third of the participants chose e-cig use due to its better taste and smell compared to tobacco smoking. Piñeiro et al. also reported similar findings, as e-cig usage among men was found to be associated with positive expectancies, including better taste and social facilitation [23]. E-cigs are widely used for smoking cessation due to the common belief in their safety compared to tobacco smoking [25]. Similar results were found in a study conducted in Jordan, which showed that e-cig users agreed that using an e-cig is safer than tobacco smoking to both the user and surroundings, and that it is cheaper and can help in smoking cessation [4]. On the other hand, the literature suggests that high use of e-cigs is not medically recommended as most healthcare providers believe that e-cigs are unsafe and do not help with tobacco smoking cessation [26].
Ramadan is the holy fasting month for Muslims all around the world. Ideally, this month is supposed to be a good chance for smokers to quit smoking [14]. However, due to nicotine withdrawal symptoms, especially at the commencement of Ramadan, many fail to quit smoking [27]. Accordingly, smokers have reported following different methods to quit smoking, including a gradual reduction in nicotine consumption prior to fasting, using nicotine replacement therapy (particularly nicotine patches), and switching either completely or partially to e-cigs [14, 28, 29]. E-cig use yields quick and high levels of nicotine, which could help in smoke cessation, but conversely could also lead to physical dependence on nicotine [30]. A limited number of studies have investigated the occurrence and severity of nicotine withdrawal symptoms post the absence of e-cigs among users [30,31,32]. This study was concerned with this aspect during intermittent fasting, particularly during the month of Ramadan. Interestingly, more than half of the participants experienced relatively weak physical and psychological withdrawal symptoms, while the rest did not experience any withdrawal symptoms. Hughes and Callas state that a minority of e-cig users experience withdrawal symptoms when they quit or decrease the use of e-cigs, and suggest that the reported symptoms were much less than those reported by tobacco smokers [30]. Moreover, it was mentioned that e-cig withdrawal symptoms were not significantly greater in those who had attempted to quit e-cigs but failed. The importance behind revealing the severity of withdrawal symptoms comes from the fact that such severity can affect the cessation process [33]. In addition, the consequences of withdrawal symptoms, such as poor concentration or depression, could disturb the normal day of the life of the individual [34]. During fasting time, non-smokers usually complain of certain symptoms, such as headaches, dizziness and nausea, which could be related to hypoglycemia and/or caffeine withdrawal [35, 36]. In this study, only 10% of the participating e-cig users also reported symptoms that could be related to both fasting and nicotine withdrawal symptoms.
Intense craving (i.e. an increased urge to smoke) is one of the most common psychological withdrawal symptoms that contribute to smoking relapse and failure of cessation [37, 38]. In this study, around 30% of e-cig users suffered from intense craving during fasting time, which was associated with the usage of high concentrations of nicotine (24–50 mg/mL). Such findings could be considered a recidivism factor, which may limit the effectiveness of e-cig cessation during fasting and may require a strong and mindful will to succeed [38]. Development of coping behaviors and resilience processes during fasting (especially during Ramadan) could support e-cig users to quit and reduce the rate of smoking relapse [39,40,41]. Most of the study’s e-cig users preferred to keep themselves busy during fasting time as a way to help them control the withdrawal symptoms they experienced. This action could be useful in Ramadan, as this month is naturally rich with community gatherings and worship, which results in many distractions and thus empowers individuals to overcome physical and psychological withdrawal symptoms [27]. In addition, many published articles have highlighted the role of spirituality in the management and prevention of addiction (e.g. nicotine, alcohol, etc.) and have thus supported smoking or addiction recovery tools [42,43,44]. The minority of the study’s e-cig users reported that they preferred to take medications to manage their withdrawal symptoms, use patches of nicotine replacement therapy, and only a small number advised that they consulted a healthcare provider. Such responses highlight the suboptimal role of healthcare services offered to e-cig users, which are supposed to be essential for health consultations and user guidance in order to achieve the goal of smoke reduction and cessation [14]. It is important to note that the use of nicotine replacement therapy in the form of patches does not break the user’s fasting, as long as no direct oral intake happens [28].
More than half of the e-cig users consumed e-liquid containing nicotine (6.0 and 15.0 mg/day). There was a positive significant correlation between e-cig withdrawal symptoms and the daily consumed nicotine concentration. Most of the smoking-related studies demonstrated the addictive potential of nicotine, regardless of the source, be it tobacco smoking, waterpipe smoking, or e-cigs [2]. A study conducted by Talih et al. in 2015 found that higher nicotine concentrations in e-liquid and higher voltage in e-cig devices resulted in a higher nicotine yield via e-cigs [45]. However, the evidence has revealed that, in general, the nicotine produced from e-cigs is less than that from tobacco cigarette smoking [30]. The majority of this study’s participants used the ‘Vape mode’ device, which is a third-generation e-cig device that is characterized by providing the user the ability to change the voltage and the produced nicotine concentration [1]. Moreover, this study’s results show a significant correlation between the severity of withdrawal symptoms and the type of device being used.
The harmful effects of e-cigs are still not fully clear, and many cases have been recorded from around the world regarding the use of e-cigs, which include the induction of acute lung injury. There were documented cases for immature use of these devices as well, which contradict the original objective of their synthesis [46]. To summarise, this study’s findings indicate that e-cigarettes could play a successful role in smoking cessation among tobacco smokers via short term use by adults during intermittent fasting. Ramadan offers a good opportunity for smokers to quit. This should be managed under professional healthcare supervision and boosted by well-designed educational/awareness programs to facilitate the cessation during and post fasting. Further studies should be conducted to assess the applicability of such processes among e-cig users.
Limitations
The first limitation of this study was the patient self-selection process that was followed. The survey was conducted online due to the novel coronavirus pandemic that started around January of this year, 2020 [47], and the public quarantine currently imposed in Jordan. Hence, only people who use the Internet and other social media platforms were able to participate. The second limitation is the representativeness of the sample to the population of Jordan, given that males actively participated in this survey more than females. The third limitation is that this study assessed the e-cig withdrawal symptoms among users during Ramadan only. Future studies should evaluate e-cig usage in months other than Ramadan, in order to compare the findings and provide a broader view of e-cig withdrawal symptoms. Moreover, some of the mentioned symptoms could be potentiated during fasting such as dizziness, headache and nausea.
Conclusion
This study has shown that the majority of e-cig users sought smoking cessation as the main reason behind using e-cigs. The severity of the physical and psychological withdrawal symptoms upon the intermittent fasting during the month of Ramadan was relatively weak. Accordingly, these results could imply that e-cigs are compatible with being used as a smoking cessation tool in conjunction with intermittent fasting. However, success in ceasing smoking is highly dependent on the mindfulness of the Jordanian smoker and required motivational awareness programs and feasible behavioral interventions offered to support smoking cessation.
Availability of data and materials
The data will be made available by the corresponding author upon request.
Abbreviations
- E-cig:
-
Electronic cigarettes
- E-liquid:
-
Electronic liquid.
- SPSS:
-
Statistical Package for the Social Sciences
References
DeVito EE, Krishnan-Sarin S. E-cigarettes: impact of e-liquid components and device characteristics on nicotine exposure. Curr Neuropharmacol. 2018;16(4):438–59.
National Academies of Sciences E, and Medicine. Public health consequences of e-cigarettes. Washington, D.C.: National Academies Press; 2018.
Soteriades S, Barbouni A, Rachiotis G, Grevenitou P, Mouchtouri V, Pinaka O, et al. Prevalence of electronic cigarette use and its determinants among 13-to-15-year-old students in Greece: results from the 2013 global youth tobacco survey (GYTS). Int J Environ Res Public Health. 2020;17(5):1671.
Barakat M, Assaf AM, Al-Qudah RA, Thiab S, Alhamd M, Al-Obaidi HJ, et al. Perceptions of adults toward electronic cigarettes: a cross-sectional study from Jordan. Primary Health Care Res Dev. 2021;22(e3).
Al-Balas HI, Al-Balas M, Al-Balas H, Almehaiza S, Bayan A-BJJoCH. Electronic cigarettes prevalence and awareness among Jordanian individuals. 2020:1–4.
Safi M, al-Tahat J. Jordan smoking rates highest in world amid claims of big tobacco interference. The guardian. 2020.
Spellberg B, Guidos R, Gilbert D, Bradley J, Boucher HW, Scheld WM, et al. The epidemic of antibiotic-resistant infections: a call to action for the medical community from the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(2):155–64.
Centers for Disease Control and Prevention (CDC). How tobacco smoke causes disease: the biology and behavioral basis for smoking-attributable disease: a report of the Surgeon General. Washington, D.C.: US Government Printing Office; 2010.
Rodriguez E, Parrón T, Alarcón R. Perceptions and Use of the e-Cigarette Among University Students. Archivos de Bronconeumología (English Edition).
Martínez Ú, Martínez-Loredo V, Simmons VN, Meltzer LR, Drobes DJ, Brandon KO, et al. Erratum: how does smoking and nicotine dependence change after onset of vaping? A retrospective analysis of dual users. Nicotine Tobacco Res. 2020;22(5):864.
Adriaens K, Gucht DV, Baeyens F. IQOS(TM) vs. e-cigarette vs. tobacco cigarette: a direct comparison of short-term effects after overnight-abstinence. Int J Environ Res Public Health. 2018;15(12):2902.
Barbeau AM, Burda J, Siegel M. Perceived efficacy of e-cigarettes versus nicotine replacement therapy among successful e-cigarette users: a qualitative approach. Addict Sci Clin Pract. 2013;8(1):5.
Mughal F. Ramadan: what it means for general practice. Br J Gener Pract. 2014;64(624):356.
Mughal F, Kingstone T. Encouraging smoking cessation in Ramadan in primary care. Addiction (Abingdon, England). 2018;113(9):1751.
Etter J-F. A self-administered questionnaire to measure cigarette withdrawal symptoms: the Cigarette Withdrawal Scale. Nicotine Tobacco Res. 2005;7(1):47–57.
Brown J, West R, Beard E, Michie S, Shahab L, McNeill A. Prevalence and characteristics of e-cigarette users in Great Britain: findings from a general population survey of smokers. Addict Behav. 2014;39(6):1120–5.
Boynton PM, Greenhalgh T. Selecting, designing, and developing your questionnaire. BMJ. 2004;328(7451):1312–5.
Couraud S, Cortot AB, Pivot XB, Touboul C, Lhomel C, Blay J-Y, et al. Beliefs and behavior regarding e-cigarettes in a large cross-sectional survey. Prevent Med Rep. 2018;10:332–6.
Department of Statistics. Population Estimates in Jordan 2019. http://dosweb.dos.gov.jo/DataBank/Population_Estimares/PopulationEstimates.pdf .
Taherdoost H. Determining sample size; how to calculate survey sample size. Int J Econ Manage Syst. 2017;2:3.
Centers for disease control and prevention (CDC). Smoking and tobacco use fast facts 2020. https://www.cdc.gov/tobacco/data_statistics/fact_sheets/fast_facts/index.htm.
Marquez PVK, Konstantin; Andreeva, Tatiana. Jordan: overview of tobacco use, tobacco control legislation, and taxation. Washington, D.C.: World Bank Group; 2019.
Piñeiro B, Correa JB, Simmons VN, Harrell PT, Menzie NS, Unrod M, et al. Gender differences in use and expectancies of e-cigarettes: online survey results. Addict Behav. 2016;52:91–7.
Jaghbir M, Shreif S, Ahram M. Pattern of cigarette and waterpipe smoking in the adult population of Jordan. EMHJ-Eastern Mediterranean Health J. 2014;20(9):529–37.
Berry KM, Reynolds LM, Collins JM, Siegel MB, Fetterman JL, Hamburg NM, et al. E-cigarette initiation and associated changes in smoking cessation and reduction: the Population Assessment of Tobacco and Health Study, 2013–2015. Tobacco Control. 2019;28(1):42–9.
Ibrahim Dwedar DR, Aya M. A survey exploring knowledge and beliefs about electronic cigarettes between health care providers and the general population in Egypt. Int J Chronic Obstruct Pulmon Dis. 2019;14:1943–50.
Aveyard P, Begh R, Sheikh A, Amos A. Promoting smoking cessation through smoking reduction during Ramadan. Addiction (Abingdon, England). 2011;106(8):1379–80.
Maarof M, Ali AM, Bakry MM, Taha N. Time Course of Cigarette Withdrawal Symptoms while Using Nicotine Patch during Ramadan. Jurnal Sains Kesihatan Malaysia (Malaysian Journal of Health Sciences). 2018;16
Gualano MR, Passi S, Bert F, La Torre G, Scaioli G, Siliquini R. Electronic cigarettes: assessing the efficacy and the adverse effects through a systematic review of published studies. J Public Health. 2015;37(3):488–97.
Hughes JR, Callas PW. Prevalence of withdrawal symptoms from electronic cigarette cessation: a cross-sectional analysis of the US Population Assessment of Tobacco and Health. Addict Behav. 2019;91:234–7.
Foulds J, Veldheer S, Yingst J, Hrabovsky S, Wilson SJ, Nichols TT, et al. Development of a questionnaire for assessing dependence on electronic cigarettes among a large sample of ex-smoking E-cigarette users. Nicotine Tob Res. 2015;17(2):186–92.
Rostron BL, Schroeder MJ, Ambrose BK. Dependence symptoms and cessation intentions among US adult daily cigarette, cigar, and e-cigarette users, 2012–2013. BMC Public Health. 2016;16(1):814.
Hughes JR. Effects of abstinence from tobacco: etiology, animal models, epidemiology, and significance: a subjective review. Nicotine Tob Res. 2007;9(3):329–39.
Hughes JR. Effects of abstinence from tobacco: valid symptoms and time course. Nicotine Tob Res. 2007;9(3):315–27.
Awada A, Jumah MA, Pain F. The first-of-Ramadan headache. J Head Face Pain. 1999;39(7):490–3.
Siaw MYL, Chew DEK, Dalan R, Abdul Shakoor SAKK, Othman N, Choo CH, et al. Evaluating the effect of Ramadan fasting on muslim patients with diabetes in relation to use of medication and lifestyle patterns: a prospective study. 2014;2014.
Allen SS, Bade T, Hatsukami D, Center BJN, Research T. Craving, withdrawal, and smoking urges on days immediately prior to smoking relapse. Nicotine Tobacco Res. 2008;10(1):35–45.
Jiloha RC. Pharmacotherapy of smoking cessation. Indian J Psychiatry. 2014;56(1):87.
Schmitz JM, Rosenfarb IS, Payne TJ. Cognitive and affective responses to successful coping during smoking cessation. J Subst Abuse. 1993;5(1):61–72.
Hendershot CS, Witkiewitz K, George WH. Marlatt GAJSat, prevention, policy. Relapse Prevent Addict Behav. 2011;6(1):17.
García-Rodríguez O, Secades-Villa R, Flórez-Salamanca L, Okuda M, Liu S-M, Blanco CJD, et al. Probability and predictors of relapse to smoking: results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug Alcohol Depend. 2013;132(3):479–85.
Cook CCJA. Addiction and spirituality. Addiction. 2004;99(5):539–51.
White W, Laudet AJCM. Spirituality, science and addiction counseling. Counselor Mag. 2006;7(1):56–9.
Treloar HR, Dubreuil ME, Miranda JR. Spirituality and treatment of addictive disorders. Rhode Island Med J. 2014;97(3):36–8.
Talih S, Balhas Z, Eissenberg T, Salman R, Karaoghlanian N, El Hellani A, et al. Effects of user puff topography, device voltage, and liquid nicotine concentration on electronic cigarette nicotine yield: measurements and model predictions. Nicotine Tob Res. 2015;17(2):150–7.
Centers for disease control and prevention (CDC). Outbreak of lung injury associated with the use of e-cigarette, or vaping, products; 2020. https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html.
Lai C-C, Shih T-P, Ko W-C, Tang H-J, Hsueh P-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents 2020:105924.
Acknowledgements
Not applicable
Funding
This study has not received any funds.
Author information
Authors and Affiliations
Contributions
All authors were involved in all parts of the study and manuscript preparation including literature search, study design, analysis of data, manuscript preparation, and review of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Ethics approval for the study was obtained from the Faculty of Pharmacy, Applied Science Private University (Approval number: 2020-PHA-5).
Consent to publish
Authors consent for publication of their identifiable details in relation to “Electronic Cigarettes’ Withdrawal Severity Symptoms Among Users During Intermittent Fasting: A cross-sectional study” manuscript.
Competing interests
All authors declare that they have no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix S1.
Electronic cigarettes’ withdrawal severity symptoms among users during intermittent fasting survey.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Barakat, M.M., Al-Qudah, R.A., Alfayoumi, I. et al. Electronic cigarettes’ withdrawal severity symptoms among users during intermittent fasting: a cross-sectional study. Addict Sci Clin Pract 16, 10 (2021). https://doi.org/10.1186/s13722-021-00219-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13722-021-00219-9