
Abstract
Background
Following the emergence of the COVID-19 pandemic in Europe at the start of 2020, most countries had implemented various measures in an attempt to control the spread of the virus. This study analyses the main non-pharmaceutical interventions and their impact on the rate by which cumulative cases and deaths were growing in Europe during the first wave of this pandemic.
Methods
The interventions analysed are the school closures, restrictions on travel, cancellation of events, restrictions on gatherings, partial and full lockdowns. Data was collected on the implementation date of these interventions, and the number of daily cases and deaths during the first wave of the pandemic for every country and territory geographically located in Europe. The study uses growth rates to calculate the increase in cumulative cases and deaths in Europe before, during, and after these interventions were implemented.
Results
The results show that decisions to close schools, cancel events, and restrict travel were taken during the same time period, whereas the decisions for the other interventions were taken when the growth rates were similar. The most effective interventions at lowering the rate by which cumulative cases were increasing were the travel restrictions, school closures, and the partial lockdown, while most effective against cumulative deaths were the partial lockdown, travel restrictions, and full lockdown.
Conclusion
All the interventions reduced the rate by which cumulative cases and deaths were increasing with the partial lockdowns being the most effective from the other interventions, during the first wave of the pandemic in Europe.
Similar content being viewed by others


Background
The COVID-19 pandemic has been the focus of interest for the past months and will continue to serve as a platform for discussions in health management for many years. Typical study cases include an understanding of differences in frequency and severity (for example [6, 15, 16]; and [35]), its effect on other aspects (for example [24, 27, 28]) as well as measures to contain the epidemic (for example [2, 8, 15]).
This paper analyses the effects of the main six non-pharmaceutical interventions (NPIs) and their impact on the rate by which cumulative cases and deaths were increasing during the first wave of the pandemic in Europe. Non-pharmaceutical interventions are defined as measures that can be taken to limit the spread of a virus. These measures need to be taken by governments to reduce transmission in the absence of pharmaceutical interventions such as vaccines [13].
Method
Our investigation focuses on the first wave in EuropeFootnote 1 which started at the end of January 2020 when the first cases were being reported, and ended around the end of May when the total number of daily cases for each country in the study summed up together remained below 20,000 and many countries had begun easing the restrictions implemented in the previous months [29].
Data collection
Data was collected on the six NPIs listed in Table 1, and the date on which they were implemented during the first wave of the pandemic in Europe.
This data was collected for all countries and territories geographically located in Europe using various secondary sources of data (Appendix 1). For the majority of countries, the ACAPSFootnote 2 global dataset was used. However, this dataset did not include data for Liechtenstein, Isle of Man, Gibraltar, Channel Islands, and Vatican City. The data for these countries was taken from each country’s respective government website on COVID-19 [10, 18, 19, 21, 31, 34].
Data was also collected on the number of daily cases and deaths from the European Centre for Disease Prevention and Control (ECDC) dataset on the geographic distribution of COVID-19 cases worldwide for all countries, except for the Vatican City for which data was taken from the Worldometer Coronavirus Statistics website [9, 40].
Data analysis
The first part of the analysis involved identifying the order in which the interventions were implemented. Measures of central tendency including the median and mean were used to find the average number of days each NPI was implemented after the first intervention. The standard deviation was also calculated as it showed the variability in the data.
The analysis also involved the calculation of nine growth rates that represent the percentage increase in the number of cumulative cases and deaths for each NPI. It is estimated that the incubation period for COVID-19 is on average 5–6 days, but it could also take up to 14 days for symptoms to appear [23, 36, 39].
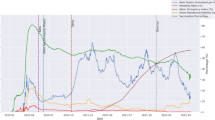
Therefore, this analysis used two sets of rates to analyse the effect of NPIs, as can be seen in Fig. 1. The first set of rates (A, B, C, D) show the percentage increase in seven-day periods, while the second set of rates (E, F, G, H, I) show the percentage increase in fourteen-day periods.

Rates of Growth
Each rate of growth was calculated for every country individually and for each of the six NPIs. Measures of central tendency, including both the median and mean were then used to find the overall rate of growth for each rate and for each NPI. With respect to the mean, the geometric mean was chosen since it is typically used when dealing with growth rates [7].
Results
Order of implementation
Forty-six out of fifty-four countries and territories in Europe implemented the cancellation of events as one of their first measures to control transmission of the virus. Out of the remaining eight countries, five countries implemented school closure as their first NPI and three countries set international travel restrictions first. The countries that set international travel restrictions quickly followed their decision with school closures prior to cancelling large events (Appendix 4).
Table 2 shows the order in which the other five NPIs were implemented.
School closures were implemented on average between 1 and 2 days after events were cancelled. This was followed by the restrictions on gatherings and travel which were implemented on average within less than a week after events were cancelled. The lockdowns were the last decisions taken, with the partial lockdown implemented on average over a week after events were cancelled, and the full lockdown implemented on average 24 days after events were cancelled. The standard deviation shows that this was not the case for all countries, since some took either much longer to implement additional restrictions or were quicker to do so.
Cumulative cases
Table 3 summarises the median growth rates in terms of cumulative cases for each growth rate and every NPI, with the mean growth rates also giving similar results (Appendix 2). Rates A and E measure the growth rate before the NPI was implemented, while Rate F measures the growth rate during the implementation of the NPI. All other rates measure the growth rate after the NPI was implemented.
As a first example, we compare the partial lockdown median cumulative rates. The figures for rate E and G are 3461% and 555% respectively. This means that if there were 100 cases 2 weeks prior to school closures, there would have been 3561 cases by the day partial lockdowns were effective and 23,324 cumulative cases to date 2 weeks later. The typical growth was 35-fold in the 2 weeks up to the NPI but ‘only’ six-fold 2 weeks later.
Similarly, we can clarify rates A, B and C for travel restrictions. If there were 100 cumulative cases a week before travel restrictions is implemented, there were typically 609 (+ 509%) cases on that day, 2320 (+ 281%) cases a week later and 5221 (+125%) cases a week after that (2 weeks after decision is taken). While the absolute increase is larger as time passes, the relative change is lower. In the week just prior to the decision, there was a six-fold increase (100 to 609) but the difference 2 weeks later was about double (2320 to 5221).
Figure 2 shows the distribution of incident growth rates in the week preceding the decision of any NPI. The widest distribution of COVID-19 cases was occurring prior to the decision to close schools, restrict travel and cancel events. This can be explained by the fact that most countries took these three decisions during a similar timeframe despite being at different experience of the incidence growth rate.

Rate A in terms of Cumulative Cases
Weekly rates (rates A – D)
Given the length of the incubation period, some of the individuals exposed a week before an intervention was implemented could have developed symptoms up to a week after. Therefore, Rate B is expected to be similar or smaller than Rate A, especially if other interventions have already been implemented. With the interventions in place for a longer time, Rate C and D should decrease further from Rate A. Table 4 shows the percentage change between the weekly median rates.
We can again use the travel restrictions rate changes as an example. In the previous section we noted that in the week just prior to the decision, there was a six-fold increase (100 to 609) but the weekly-difference 2 weeks later was about double (2320 to 5221). This can be measured to be about a third of the old cumulative growth (since double is a third of a sixth). The exact measure is that the growth rate in the period C is 36.94%Footnote 3 of the growth rate in period A which is a 63.05% difference.
Cumulative cases were increasing at the highest rate before events were cancelled. Rate A was also high for the school closures and travel restrictions NPIs. Before the other interventions were implemented the growth rate decreased slightly and decreased even further before the full lockdown.
The partial lockdown and travel restriction were two of the most effective interventions as they had the highest improvement from Rate A to both Rates B and C, lowering the growth rate by over 60%. Over another week, the travel restrictions had the highest improvement, followed by the school closures, cancellation of events, and partial lockdown, all of which lowered the growth rate by over 70%.
Fortnightly rates (rates E to I)
Due to the length of the incubation period, Rate F is expected to be similar to Rate E. With the interventions in place longer, Rates G, H, and I are expected to decrease from Rates E and F. Table 5 shows the percentage change between these median rates.
Cumulative cases were increasing at the highest rate from 2 weeks before schools were closed and travel was restricted. Rates E and F were slightly lower for the other NPIs, and even lower for the full lockdown, which means that 2 weeks before their implementation cumulative cases were increasing at a lower rate.
The partial lockdown was the most effective as it had one of the highest improvements between growth rates, followed by the school closures and travel restrictions which were also more effective in comparison to the other NPIs.
Cumulative deaths
Table 6 summarises the median growth rates in terms of cumulative deaths for each growth rate and for each NPI, with the mean growth rates giving similar results (Appendix 3).
Weekly rates (rates A to D)
Due to the length of the incubation period, Rate B is expected to be similar to Rate A. With the interventions in place for a longer time Rate C and D should decrease further from Rate A. Table 7 shows the percentage change between the median rates.
Cumulative deaths were increasing at the highest rate before the implementation of travel restrictions. Rate A was also high before the implementation of school closures and partial lockdown. The travel restrictions and lockdowns were the most effective at lowering the rate by which cumulative deaths were increasing as they had the highest improvements between growth rates.
Fortnightly rates (rates E to I)
Due to the length of the incubation period, Rate F is expected to be similar to Rate E. With the interventions in place longer, Rates G, H, and I are expected to decrease from Rates E and F. Table 8 shows the percentage change between these median rates.
Cumulative deaths were increasing at the highest rate before the implementation of the cancellation of events and closure of schools. Directly after implementation, the cancellation of events, school closures, and lockdowns were the most effective as they had the highest improvements from rate E to F.
After 2 weeks, the school closures and lockdowns were the most effective. As the interventions were in place for another week, the restrictions on gatherings had the highest improvement, followed by the partial lockdown. Over time, the partial lockdown, school closures, and travel restrictions were the most effective.
Only France had deaths 2 weeks prior to schools closing and travel being restricted, and so, there was no discrepancy observed in Rate E for these NPIs. Whereas before the other interventions were implemented cumulative deaths were increasing by varying rates.
Discussion
The high variability in the pre- and mid-intervention rates A, E and F would show that interventions were implemented when countries where in different stages of the pandemic in terms of cumulative cases and/or deaths. However, a low variability in these rates would mean that the interventions were implemented when countries reached the same or a similar stage of the pandemic and not necessarily during the same time period.
School closures
The decision to close schools was taken by Europe during the same time period since cumulative cases were increasing by varying rates between countries. The discrepancy observed in terms of cumulative deaths showed that this time period was the start of the pandemic. In fact, 2 weeks before implementation, only France had recorded any deaths and by the following week deaths started increasing by low and similar rates in more countries [33].
The results obtained coincide with the claims made by Brauner et al. [3], that the closure of schools and universities does reduce transmission of COVID-19. When comparing growth rates, the closure of schools was observed to be one of the most effective at improving the rate by which cumulative cases were increasing over time. On the other hand, even though it was effective at lowering the growth rate in terms of cumulative deaths, it was less effective than the other NPIs.
Travel restrictions
The decision to restrict travel was also taken throughout Europe during the same time period and not when cumulative cases and deaths were increasing by similar rates. However, there was no discrepancy in Rate E in terms of cumulative deaths since only France had recorded deaths 2 weeks before restricting travel. By a week later more countries were reporting deaths which were increasing by varying rates across Europe. This was possibly due to people having contracted the virus prior to the NPI being implemented.
The decision was likely taken at the start of the pandemic following the recommendations issued by the EU on March 16 2020, after the majority of countries had already cancelled events and closed schools [12]. In fact, prior to implementation the growth rates were lower than previously implemented interventions.
The travel restrictions were one of the most effective mitigation measures during the first wave in Europe as indicated by the consistently high improvements between growth rates, both in terms of cumulative cases and deaths. This is in agreement with existing studies such as those by Espinoza, et al. [11] and Primc and Slabe-Erker [26] which found that travel restrictions are highly effective at reducing transmission rates of COVID-19.
Cancellation of events
Two weeks before events were cancelled, the virus had not yet reached all of Europe and cases were still increasing at low rates. Within the next week, the majority of countries were affected and cases were increasing more rapidly at varying rates across Europe. Similarly to school closure and travel restrictions, the decision to cancel events was taken during the same time period and not when countries were in similar stages in terms of cases.
Given that it was first to be implemented and at a time when cases had just started rapidly increasing, only two countries had registered their first deaths 2 weeks before cancellation causing the high variability in Rate E. By the following week a few more countries were registering their first deaths which were increasing at low and similar rates.
Hunter et al. [20] & Garchitorena et al. [17] argued that the cancellation of events, most notably superspreader events, had a large effect on reducing transmission. The results obtained agree with these studies and show that over time the cancellation of events did lower the rate of growth. However, it was one of the least effective in comparison to the other NPIs, especially in terms of cumulative deaths. Our understanding is that cancellation of events act as a reducer in the probability of significant jumps in the spike rate (due to superspreader events) rather than a lowering of the growth rate per se.
Restrictions on gatherings
The decision to restrict gatherings was taken when countries were in the same stage in terms of cumulative cases as they were increasing by similar rates across Europe rather than at a similar timepoint. On the other hand, cumulative deaths were increasing at varying rates, possibly due to the additional delay from exposure to potential death.
The pre and mid intervention rates (rates A, E, and F) were also observed to be relatively lower than other NPIs. This could be because the effects of previously implemented interventions were being reflected in this intervention’s growth rates.
Brauner et al. [3] explain the effects of restricting gatherings depend on the limit set by countries. The lower the limit for gatherings is, the higher would be the effect of the intervention. The results show that the intervention had a moderate effect on the rate of growth for both cases and deaths and had one of the worst improvements in rates in comparison to the other NPIs. This could potentially mean that the limit set for gatherings by the majority of countries was not sufficient or possibly this is a dilution of the effects of earlier NPIs.
Partial lockdown
The discrepancy observed in growth rates for cumulative cases shows that the partial lockdown was implemented when cumulative cases were growing by similar rates (four-fold increase over 2 weeks), whereas cumulative deaths were increasing by higher (six-fold increase over 2 weeks) and varying ratesFootnote 4 across Europe.
Before the implementation of the partial lockdown cumulative cases were increasing at lower rates, whereas cumulative deaths were increasing more rapidly in comparison to the previously implemented interventions. This could explain why countries felt the need to implement more stringent measures to control transmission.
This suppression measure was not implemented as early as the other interventions due to the negative consequences it has on the economy and mental health of individuals as well as the difficulty in monitoring compliance by individuals.
The studies by Flaxman et al. [14] and Ferguson et al. [13] found that in Europe lockdowns would have the highest impact on transmission rates and that their implementation would reduce transmission significantly. The results obtained when comparing the growth rates both in terms of cumulative cases and deaths, coincided with both studies and showed that the partial lockdown consistently had either the highest or one of the highest improvements between growth rates.
Full lockdown
The countries that decided to implement a full lockdown did so when they were in very similar situations in terms of cases and deaths. This was shown by the very low variability in growth rates A, E, and F for both cumulative cases and deaths. Prior to implementation, cumulative cases and deaths were increasing by much lower rates, however, some countries wanted to further control transmission.
This intervention was one of the least effective at lowering the growth rate in terms of cumulative cases. On the other hand, it was more effective at lowering the rate by which cumulative deaths were increasing.
Limitations
There where various limitation to this research. Firstly, the NPIs were implemented very close to each other which makes it difficult to measure their singular effect. The implementation of NPIs is also affected by other factors whose effects cannot always be measured. These include testing capabilities; timing, method and severity of implementation; population demographics socio-economic conditions; and public response and awareness [4, 5].
For example, countries with a higher population density and older population are more susceptible to cases and deaths [22, 30, 37]. Outbreaks in high-risk environments such as long-term care facilities also affect growth rates. A report by the European Centre for Disease Prevention and Control showed that in some European countries, 50% of deaths were attributable to patients in these facilities [9, 32]. Moreover these may have been unreported [25]. A similar discrepancy might have been that some countries may have had more time to report deaths while having Covid-19 as compared to deaths due to Covid-19. It would therefore be of great interest to revisit this work using excess mortality rates.
The growth rates could have decreased over time on their own after reaching a peak [38]. There were also missing values in the calculation of growth rates since not all countries had all rates and not all countries implemented all the interventions. Finally, the results obtained did not always apply to every country, that is, while the average rates could have shown a decrease from one rate to another, this might not have been the case for all countries.Footnote 5
Conclusion
For each NPI, the rate at which cumulative cases and deaths were increasing before the implementation of each intervention decreased over time. Without these interventions, the rate of growth would have increased, resulting in many more cases and deaths across Europe.
Our analysis indicates that partial lockdowns were the most effective from the interventions during the first wave in Europe as it reduced both incidence of cases and deaths. Travel restrictions also lowered both the number of cases and deaths. School closures and full lockdowns were effective in reducing the number of cases and deaths respectively.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Notes
NPIs throughout the European continent have been analysed. A list of countries is provided in the Appendix.
ACAPS is an independent information provider providing humanitarian needs analysis and assessment [1].
\(\frac{5221}{2320}\div \frac{609}{100}\times 100=36.94\%\).
Interquartile ranges of Rates A, E and F were 454, 4967 and 4375% respectively)
Only 7.4% and 6.2% showed an increase in weekly and fortnightly cumulative cases post NPIs.
Abbreviations
- ACAPS:
-
The Assessment Capacities Project
- ECDC:
-
European Centre for Disease Prevention and Control
- NPI:
-
Non-pharmaceutical intervention
- WHO:
-
World Health Organisation
References
ACAPS, 2020. COVID-19 government measures dataset. [online] ACAPS. Available at: https://www.acaps.org/covid-19-government-measures-dataset. [Accessed 23 Mar 2021].
Björk J, Mattisson K, Ahlbom A. Impact of winter holiday and government responses on mortality in Europe during the first wave of the COVID-19 pandemic. Eur J Pub Health. 2021;31(2):272–7. https://doi.org/10.1093/eurpub/ckab017.
Brauner J, Mindermann S, Sharma M, Johnston D, Salvatier J, Gavenčiak T, et al. Inferring the effectiveness of government interventions against COVID-19. Science. 2021;371(6531):eabd9338. https://doi.org/10.1126/science.abd9338.
Bruinen de Bruin Y, Lequarre A, McCourt J, Clevestig P, Pigazzani F, Zare Jeddi M, et al. Initial impacts of global risk mitigation measures taken during the combatting of the COVID-19 pandemic. Saf Sci. 2020;128:104773. https://doi.org/10.1016/j.ssci.2020.104773.
Burström B, Tao W. Social determinants of health and inequalities in COVID-19. Eur J Pub Health. 2020;30(4):617–8. https://doi.org/10.1093/eurpub/ckaa095.
Cortis D. On determining the age distribution of COVID-19 pandemic. Front Public Health. 2020;8:202.
C. Longest K. Using Stata for quantitative analysis. Chapter 4: Sage Publ; 2012. https://doi.org/10.4135/9781452269931.
De Matteis A, Turkmen Ceylan FB, Adrianopoli M, Ertek S. The contribution of testing in the fight against COVID-19: evidence from Italy. Eur J Pub Health. 2021. https://doi.org/10.1093/eurpub/ckab064.
ECDC, 2020. Download historical data (to 14 December 2020) on the daily number of new reported COVID-19 cases and deaths worldwide. [online] European Centre for Disease Prevention and Control. Available at: https://www.ecdc.europa.eu/en/publications-data/download-todays-data-geographic-distribution-covid-19-cases-worldwide. [Accessed 22 Mar 2021].
Embassy of the Principality of Liechtenstein, 2020. Measures Taken In Liechtenstein In Response To The Coronavirus Pandemic | Embassy Of The Principality Of Liechtenstein In Washington, D.C.. [online] Liechtensteinusa.org. Available at: http://www.liechtensteinusa.org/article/measures-taken-in-liechtenstein-in-response-to-the-coronavirus-pandemic. [Accessed 22 Mar 2021].
Espinoza B, Castillo-Chavez C, Perrings C. Mobility restrictions for the control of epidemics: when do they work? PLoS One. 2020;15(7):e0235731. https://doi.org/10.1371/journal.pone.0235731.
European Commission, 2020. Communication from the commission to the European parliament, the European council and the council. [online] Ec.europa.eu. Available at: https://ec.europa.eu/transparency/regdoc/rep/1/2020/EN/COM-2020-115-F1-EN-MAIN-PART-1.PDF. [Accessed 4 Apr 2021].
Ferguson N, Laydon D, Nedjati Gilani G, Imai N, Ainslie K, Baguelin M, et al. Report 9: impact of non-pharmaceutical interventions (Npis) to reduce COVID19 mortality and healthcare demand. 2020. https://doi.org/10.25561/77482.
Flaxman S, Mishra S, Gandy A, Unwin H, Mellan T, Coupland H, et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature. 2020;584(7820):257–61. https://doi.org/10.1038/s41586-020-2405-7.
Fontán-Vela M, Gullón P, Padilla-Bernáldez J. Selective perimeter lockdowns in Madrid: a way to bend the COVID-19 curve? Eur J Pub Health. 2021. https://doi.org/10.1093/eurpub/ckab061.
Francetic I, Munford L. Corona and coffee on your commute: a spatial analysis of COVID-19 mortality and commuting flows in England in 2020. Eur J Pub Health. 2021. https://doi.org/10.1093/eurpub/ckab072.
Garchitorena A, Gruson H, Cazelles B, Karki T, Sudre B, Roche B. Integrated packages of non-pharmaceutical interventions increased public health response efficiency against COVID-19 during the first European wave: evidence from 32 European countries; 2020. https://doi.org/10.1101/2020.08.17.20174821.
Glatz, C., 2020. Vatican closes museums, beefs up measures to stop virus spread. [online] Catholic News Service. Available at: https://www.catholicnews.com/vatican-closes-museums-beefs-up-measures-to-stop-virus-spread/. [Accessed 22 Mar 2021].
HM Government of Gibraltar, 2020. Covid-19 Press Releases. [online] Government of Gibraltar. Available at: https://www.gibraltar.gov.gi/press/covid-19-press-releases. [Accessed 22 Mar 2021].
Hunter P, Colón-González F, Brainard J, Rushton S. Impact of non-pharmaceutical interventions against COVID-19 in Europe: a quasi-experimental study; 2020. https://doi.org/10.1101/2020.05.01.20088260.
Isle of Man Government, 2020. News Releases & Statements. [online] Covid19. Available at: https://covid19.gov.im/news-releases-statements. [Accessed 22 Mar 2021].
Kontis V, Bennett J, Rashid T, Parks R, Pearson-Stuttard J, Guillot M, et al. Magnitude, demographics and dynamics of the effect of the first wave of the COVID-19 pandemic on all-cause mortality in 21 industrialized countries. Nat Med. 2020;26(12):1919–28. https://doi.org/10.1038/s41591-020-1112-0.
Lauer S, Grantz K, Bi Q, Jones F, Zheng Q, Meredith H, Azman A, Reich N, Lessler J. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Ann Intern Med. 2020;172(9):577–82. https://doi.org/10.7326/M20-0504.
Laukkanen L, Lahtinen S, Liisanantti J, Kaakinen T, Ehrola A, Raatiniemi L. Early impact of the COVID-19 pandemic and social restrictions on ambulance missions. Eur J Pub Health. 2021. https://doi.org/10.1093/eurpub/ckab065.
O’Dowd A. Covid-19: Official figures “underestimate” deaths caused by discharging patients into care homes. BMJ. 2021:n1415. https://doi.org/10.1136/bmj.n1415.
Primc K, Slabe-Erker R. The success of public health measures in Europe during the COVID-19 pandemic. Sustainability. 2020;12(10):4321. https://doi.org/10.3390/su12104321.
Reynolds CM, Purdy J, Rodriguez L, McAvoy H. Factors associated with changes in consumption among smokers and alcohol drinkers during the COVID-19 ‘lockdown’period. Eur J Public Health. 2021. https://doi.org/10.1093/eurpub/ckab050.
Roy CM, Bollman EB, Carson LM, Northrop AJ, Jackson EF, Moresky RT. Assessing the indirect effects of COVID-19 on healthcare delivery, utilization and health outcomes: a scoping review. Eur J Public Health. 2021. https://doi.org/10.1093/eurpub/ckab047.
Roser, M., Ritchie, H., Ortiz-Ospina, E. and Hasell, J., 2020. Coronavirus pandemic (COVID-19). [online] Our World in Data. Available at: https://ourworldindata.org/coronavirus. [Accessed 28 Dec 2020].
Sannigrahi S, Pilla F, Basu B, Basu A, Molter A. Examining the association between socio-demographic composition and COVID-19 fatalities in the European region using spatial regression approach. Sustain Cities Soc. 2020;62:102418. https://doi.org/10.1016/j.scs.2020.102418.
States of Jersey, 2020. Government of Jersey. [online] gov.je. Available at: https://www.gov.je/news/2020/pages/index.aspx?departmentid=28. [Accessed 22 Mar 2021].
Stockholm: ECDC, 2020. Coronavirus disease 2019 (COVID-19) in the EU/EEA and the UK – ninth update. [online] Ecdc.europa.eu. Available at: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-rapid-risk-assessment-coronavirus-disease-2019-ninth-update-23-april-2020.pdf. [Accessed 25 Dec 2020].
Taylor, D., 2021. A timeline of the coronavirus pandemic. [online] Nytimes.com. Available at: https://www.nytimes.com/article/coronavirus-timeline.html. [Accessed 13 Apr 2021].
The Government of the Faroe Islands, 2020. Corona Í Føroyum. [online] Corona í Føroyum. Available at: https://corona.fo/news. [Accessed 22 Mar 2021].
Thielecke M, Theuring S, van Loon W, Hommes F, Mall MA, Rosen A, et al. SARS-CoV-2 infections in kindergartens and associated households at the start of the second wave in Berlin, Germany− a cross sectional study. Eur J Pub Health. 2020. https://doi.org/10.1093/eurpub/ckab079.
Velavan T, Meyer C. The COVID-19 epidemic. Tropical Med Int Health. 2020;25(3):278–80. https://doi.org/10.1111/tmi.13383.
Vestergaard L, Nielsen J, Richter L, Schmid D, Bustos N, Braeye T, et al. Excess all-cause mortality during the COVID-19 pandemic in Europe – preliminary pooled estimates from the EuroMOMO network, March to April 2020. Eurosurveillance. 2020;25(26). https://doi.org/10.2807/1560-7917.ES.2020.25.26.2001214.
WHO, n.d. About pandemic phases. [online] Euro.who.int. Available at: https://www.euro.who.int/en/health-topics/communicable-diseases/influenza/data-and-statistics/pandemic-influenza/about-pandemic-phases. [Accessed 4 Apr 2021].
World Health Organisation, 2020. Coronavirus disease 2019 (COVID-19) situation report – 73. [online] Available at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200402-sitrep-73-covid-19.pdf?sfvrsn=5ae25bc7_2. [Accessed 4 May 2021].
Worldometer, 2021. Holy See coronavirus. [online] Worldometers.info. Available at: https://www.worldometers.info/coronavirus/country/holy-see/. [Accessed 22 Mar 2021].
Acknowledgements
Not applicable.
Funding
The authors declare no external funding.
Author information
Authors and Affiliations
Contributions
DC has conceptualised, designed, supervised and revised the work. FVK has collected and analysed the data and drafted the work. The authors read and approved the final manuscript.
Authors’ information
DC is an actuary and academic at the University of Malta. FVK is a masters in risk students at the University of Malta and an insurance professional.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1
Table 9
Appendix 2
Table 10
Appendix 3
Table 11
Appendix 4
Table 12
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Cortis, D., Vella King, F. Back to basics: measuring the impact of interventions to limit the spread of COVID-19 in Europe. Arch Public Health 80, 76 (2022). https://doi.org/10.1186/s13690-022-00830-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13690-022-00830-5