
Abstract
Background
Strengthening healthcare systems is a practical approach to enhance healthcare delivery and services. Although there has been a rise in the number of health systems strengthening (HSS) interventions in sub-Saharan Africa (SSA), there is limited evidence on the causal effect of these activities on child survival. Furthermore, the findings reported so far have been varied, and how they relate to each other remains unclear. This systematic review study aims to assess all available evidence to understand the impact of HSS activities on child survival in SSA.
Methods
We developed a search strategy to retrieve all relevant studies from electronic databases such as PubMed/MEDLINE, Web of Science, and African Journals Online. We will use a combination of search terms such as “under-five mortality,” “child mortality,” “infant mortality,” “neonatal mortality,” “child survival,” and “health systems strengthening.” The review will include studies that establish a causal relationship between HSS interventions and child survival. This will include studies with designs such as randomized controlled trials and quasi-experimental and methods like difference-in-difference. Two reviewers will independently screen all citations, abstracts, and full-text data and a third reviewer will act as a tiebreaker in case of disagreements. The primary outcome of interest is the impact of HSS activities on under-five survival. We will evaluate the quality of each study using the Bradford Hill criteria for causation.
Discussion
Our systematic review will identify and evaluate all relevant evidence that establishes a causal relationship between HSS activities and the survival of children under five years in SSA. The review’s findings regarding the impact of HSS activities on child survival could be of significant interest to the donor community and policy actors in the region. We also anticipate that the review’s conclusions could serve as a valuable guide for the development of future health system interventions and strategies in SSA.
Systematic review registration
PROSPERO CRD42022333913.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Globally, significant progress has been made in improving childhood survival indicators [1]. However, despite efforts in sub-Saharan Africa (SSA), there has not been a substantial reduction in under-five (U5) mortality rates [2,3,4,5]. According to a recent study, the U5 mortality rate has been reduced by 59% worldwide, from 93 deaths per 1000 live births in 1990 to 38 deaths per 1000 live births in 2019 [6]. However, for the same period, a 57% reduction was observed for SSA, from 197 to 76 deaths per 1000 live births [6]. Similarly, other granular mortality measures for children below 5 years also showed the same trend. For instance, while the global neonatal mortality rate reduced by 51% (from 37 to 18 deaths per 1000 live births) between 1990 and 2017, for SSA, the reduction was much lower at 40% [7]. The neonatal mortality rate decreased from 46 to 27 deaths per 1000 live births for SSA [7]. The progress made so far in the sub-region is modest and this may be a result of a combination of several factors.
Different stakeholders, including international donors, governments, and other healthcare investors, have implemented both specific and comprehensive interventions to improve the functioning of health systems in countries in SSA [8,9,10,11]. The goal of these interventions is to improve health outcomes, including the survival of children, by generating demand and supply of quality and timely health service delivery [9,10,11]. The interventions take the form of strategies that affect the building blocks of health systems, including health workforce, service delivery, information, leadership/governance, medicines/supplies, and finances [10, 12]. Examples of the strategies include covering expenses for maternal, newborn, and child health (MNCH), providing incentives for health workers directly providing MNCH services, developing infrastructure for service delivery, training health workers, and improving emergency and referral care through ambulance services [13,14,15].
Limited evidence exists in SSA regarding the impact of health system strengthening (HSS) activities on child survival [16,17,18]. Aside from being insufficient, the evidence also presents mixed findings. Furthermore, due to methodological shortcomings, it is difficult to attribute changes or effects to the implementation of the interventions in some cases. Most studies conducted in SSA for evaluating the impact of HSS interventions/activities do not employ robust designs, and findings may not reflect causal effects [19]. The common concerns with the study designs used for evaluating the impact of HSS interventions in SSA include insufficient time for the maturity of interventions, lack of comparison sites, and contaminations [13, 19]. Besides, most studies do not apply appropriate methods that establish causal effects and/or fit the design used. These issues make it unclear to understand the impact of HSS interventions on child survival, especially in the milieu of complex health systems and social dynamics in SSA.
Previous review studies on the effect of HSS interventions on mortality, such as those conducted by Lassi et al. [20] and Lassi and Bhutta [16], did not focus on U5 mortality in SSA and failed to provide a breakdown analysis such as neonatal, infant, and post-infant deaths. However, it is important to analyze the survival of children under 5 years in detail, considering neonates, infants, and post-infants separately, since the probability of survival varies with time [19]. Additionally, since the HSS literature was at a nascent stage during the previous studies, they may not have captured the latest evidence. Therefore, our protocol aims to assess all the available evidence on the causal effect of HSS activities on U5 mortality, including neonatal, infant, and post-infant deaths. This may enable a better understanding of the trickling effects of HSS interventions on child survival in SSA.
HSS interventions and child survival nexus—an impact framework
Mapping out a logical connection between HSS interventions and their impact on child survival is essential, as the pathway for the causal effect of these interventions can be quite complex. This complexity arises because a health system, regardless of its level, involves complex interactions between communities, households, and the healthcare sector to deliver health services to clients [21]. Generally, government actions greatly influence a health system at any level through certain pillars [22]. These pillars, also known as the “control knobs”, are broadly classified into financing (including payment), organization, regulation, and communication (persuasion) [21, 22]. On the other hand, the state of a health system can also influence government response through the control knobs (Fig. 1) [21].

For example, introducing HSS interventions at a district level is expected to generate changes in the district healthcare sector, communities, and families [21]. The healthcare sector may be affected by changes in service delivery, governance, and operational management of health facilities because of the interventions implemented [21, 23]. The changes in service delivery and management of health facilities are expected to translate into improved quality of care [23]. Further, the interventions may drive changes at the community level through, for example, the creation of community action groups/organizations and leadership to support improving community members’ health-seeking and utilization behavior [21, 23]. At the family level, the influence of the interventions can be through education or income to improve family members’ health consciousness and utilization of health services [21, 23]. Improvement in the quality of care in health facilities also feeds into improving health-seeking behavior and utilization of health services at the family and community levels [23]. These multi-level interactions within the district health system are expected to culminate in improved child survival, through increased coverage for child survival interventions [24]. A detailed pathway of how HSS interventions affect childhood survival, as well as the counter-interactions between the components of the health system, is shown in Fig. 1.
Methods
Protocol registration and reporting
This protocol has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) database and assigned a registration number CRD42022333913. The protocol was designed using the guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) (see checklist in Additional file 1) [25, 26]. The findings of the completed systematic review will be reported in accordance with the updated guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) [27].
Eligibility criteria
The Population, Intervention, Comparison, Outcome, and Study design (PICOS) framework and other criteria will be used to assess the eligibility of studies. The details for including and excluding studies are provided below.
Population
We will include any population-level study conducted in SSA that considered the impact of HSS interventions on the survival of U5 children. Studies conducted in countries outside the SSA settings will be excluded. In addition, we will not include facility-level studies and those that have not addressed the impact of HSS interventions on the survival of children below 5 years.
Intervention
We will include studies with relevant interventions aimed at improving health systems at any level, including interventions that bring about behavioral change (for example, training, and education), health information interventions, medical technology interventions, and financial interventions (such as conditional cash transfers and pay-for-performance). However, we will exclude studies with interventions that do not affect any of the six building blocks of a health system, namely (1) service delivery; (2) health workforce; (3) health information systems; (4) medical products, vaccines, and technologies; (5) health financing; and (6) leadership/governance [28].
Comparison
We will only include studies with a comparison group; those without a comparison group will be excluded.
Outcomes
Our primary outcome measure is U5 mortality. Neonatal, infant, and post-infant mortality indicators are secondary outcome measures. Studies that do not report U5 mortality will be excluded.
Study design
We will only include studies that used research designs and methods that establish a causal relationship between HSS activities and child survival. Specifically, we will include designs such as randomized controlled trials (RCTs) and quasi-experiments and methods like difference-in-difference and propensity score matching. In addition, we will only include studies with a longitudinal design, with a baseline and at least one follow-up survey. On the other hand, we will exclude studies with designs and methods that do not establish a causal relationship between HSS interventions and child survival. Cross-sectional studies, observational studies, case studies, study protocols, editorials, review studies, comments, speeches, and conference abstracts will be excluded.
Timing
We will also consider the period between the implementation of interventions and follow-up data collection. Studies that meet the criterion of conducting follow-up (or endline) surveys at least 6 months after the implementation of interventions will be included. This is because HSS interventions often require enough time to mature for the desired impact to be achieved at a population level.
Language
The studies to be included are those published in English from 2010 to now, excluding those published before 2010 and/or in other languages.
Information sources
The primary sources of information will be electronic databases such as PubMed, Web of Science, and African Journals Online (AJOL). We will also consider gray literature such as reports published by international organizations such as the World Health Organization (WHO), World Bank (WB), and the Organization for Economic Co-operation and Development (OECD). In addition, we will consult with experts on HSS interventions, particularly those with experience in implementing such activities in SSA.
Search strategy
To conduct a comprehensive search, we will use a combination of keywords and terms such as mortality, under-five mortality, child mortality, infant mortality, neonatal mortality, child survival, and health systems strengthening. These keywords will be combined using the Boolean operator (AND). A draft of the search strategy tested in PubMed is attached as Additional file 2.
Selection process
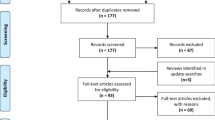
All articles retrieved from the databases’ searches will be imported into an Endnote library to identify duplicates. Any duplicates found will be removed, and the remaining articles or publications will be used for the title and abstract screenings. Two of the authors (CA and PK) will independently screen the titles and abstracts for eligibility based on the inclusion and exclusion criteria. The independent screening is to validate the selection of eligible articles based on title/abstract. If discrepancies arise in the selection of titles/abstracts, discussions will be held, and a third author (either AAB or POA or AB) will make the final decision. Eligible titles and abstracts will be transitioned into a full-text screening. After identifying eligible titles and abstracts, full-text articles will be screened for eligibility based on the inclusion and exclusion criteria. The process will be carried out independently by two authors (CA and AB). Any disagreement will be resolved by discussion and a verdict by a third independent author (AAB or POA). The PRISMA 2020 flow chart will be used to show the selection process (see Additional file 3 for a sample flow chart) [27].
Data collection process and data items
An Excel template will be used to extract all relevant data from the included studies to enable us to achieve the objective of the study and assess the quality of each study and for data synthesis. The information that will be extracted includes the following:
-
Background information related to the study, including the author(s), publication year, the journal where the study was published, and the country(ies) where the study was conducted.
-
Details on the HSS interventions implemented, such as the name of the intervention, specific strategies or activities that were implemented, health system’s building block(s) that the implemented activities targeted, and whether the building blocks were directly or indirectly affected by the activities.
-
Health system interactions, changes generated as a result of the implemented interventions, enablers of the changes, barriers to the changes, and the role of the health system control knobs towards the changes.
-
Information on the study design. For example, randomized control trials and quasi-experiments.
-
Information on the sampling procedure and the sample, such as the size of samples at baseline and endline for comparison and intervention areas and response rates.
-
Information of the methods used for analysis. For example, difference-in-difference analysis, propensity score matching, coarsened exact matching, and other treatment effect analysis.
-
Results on U5 mortality, including neonatal, infant, and post-infant.
-
Main concluding message.
-
Recommendations.
Two authors (CA and AB) will extract data from the studies accepted for inclusion and summarize them in a table. For data to be included, both authors must agree. If there are conflicts in opinion, a third verdict will be reached through discussions. In addition, our data extraction will consider distinct follow-up periods, aiming to capture both short-term and long-term impacts of HSS interventions. The classification is based on the duration from the baseline. Follow-ups conducted from 6 to 12 months after the baseline will be considered short-term effects. On the other hand, follow-ups conducted over 12 months after the baseline will be considered long-term effects. In cases where a follow-up includes two or more time points, we will prioritize the time point closest to the end of the intervention.
Quality assessment
To determine the quality of each study we will include, we have adapted the Bradford Hill criteria for causation [29, 30]. Bradford Hill proposed nine viewpoints for determining causation. These viewpoints are the strength of association, consistency, specificity, temporality, biological gradient, plausibility, coherence, experiment, and analogy [29, 30]. We will assess and rate each study based on all the criteria. The maximum score for each study is 14 points. A study with a score of less than 5 points will be rated as weak quality. Studies with a score of 5–9 will be rated as moderate quality, while those with a score of 10 points or more will be rated as high quality. Table 1 provides a detailed explanation of how we will apply Bradford Hill’s criteria.
Data synthesis and analysis
The studies will be grouped based on their quality. Studies with high quality will be analyzed separately from those with moderate and weak qualities. Our study will use a narrative approach to synthesize data from all studies included for analysis. Narrative methods of synthesis rely on the use of words and text to summarize findings from multiple studies [31]. The aim of this systematic review is to assess all available evidence and enhance understanding of the impact of HSS interventions on child survival. Therefore, a narrative method of synthesis would be suitable since the approach enables interpretive synthesis of both quantitative and qualitative studies [31].
Discussion
Deaths of children under the age of five continue to be a major public health concern in many parts of SSA [32]. While other parts of the world with well-functioning health systems have seen a significant improvement in the survival of children U5, SSA remains different [32, 33]. The health systems in most countries in SSA are still weak, and U5 survival rates are relatively low [34]. According to the WHO [32], one in thirteen children dies before his/her fifth birthday. Improving health systems by implementing system-strengthening strategies is expected to translate into better health outcomes [32]. Various HSS interventions have been implemented in SSA by governments and other stakeholders, but the impact of these system interventions in the sub-region is unclear, as the literature shows mixed findings.
This systematic review will evaluate the causal effect of HSS activities on U5 child survival in SSA by synthesizing all available evidence using a narrative approach. The review will also focus on the impact of HSS activities among sub-categories of U5 children, including neonatal, infant, and post-infant. We hope that the findings of this review will provide valuable evidence to the funding community and policy stakeholders about the impact of HSS activities in SSA. We also hope that the findings will be relevant in guiding the programming of future HSS interventions and strategies in the sub-region.
Limitations
It is important to note that our planned review may have certain limitations. Due to the strict criteria used for study inclusion, it is possible that only a few studies may meet the eligibility requirements. As a result, we may not get a diverse picture of the causal effect of HSS activities on child survival in SSA. However, we are confident that the findings will accurately reflect the impact of HSS activities on U5 child survival in SSA.
Availability of data and materials
Not applicable.
Abbreviations
- AJOL:
-
African Journals Online
- HSS:
-
Health System Strengthening
- MNCH:
-
Maternal, Newborn and Child Health
- PICOS:
-
Population, Intervention, Comparison, Outcome and Study design
- OECD:
-
Organization for Economic Co-operation and Development
- PROSPERO:
-
International Prospective Register of Systematic Reviews
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis
- PRISMA-P:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols
- RIPS:
-
Regional Institute for Population Studies
- SSA:
-
Sub-Saharan Africa
- U5:
-
Under-five
- UGBS:
-
University of Ghana Business School
- WB:
-
World Bank
- WHO:
-
World Health Organization
References
You D, Hug L, Ejdemyr S, Idele P, Hogan D, Mathers C, Gerland P, New JR, Alkema L. Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet. 2015;386(10010):2275–86.
Amegah AK. Improving child survival in sub-Saharan Africa: key environmental and nutritional interventions. Ann Glob Health. 2020;86(1):73.
Tesfa D, Tiruneh SA, Azanaw MM, Gebremariam AD, Engdaw MT, Kefale B, Abebe B, Dessalegn T. Time to death and its determinants among under-five children in Sub-Saharan Africa using the recent (2010–2018) demographic and health survey data: country-based shared frailty analyses. BMC Pediatr. 2021;21(1):1–1.
WHO. Children: reducing mortality. 2016. http://www.who.int/mediacentre/factsheets/fs178/en/. Accessed 26 Jul 2022.
UNICEF. Committing to child survival: a promise renewed progress report 2014. New York: UNICEF; 2014. http://data.unicef.org/corecode/uploads/document6/uploaded_pdfs/corecode/APR-2014-17Oct14-web_194.pdf. Accessed 26 Jul 2022.
Sharrow D, Hug L, You D, Alkema L, Black R, Cousens S, Croft T, Gaigbe-Togbe V, Gerland P, Guillot M, Hill K. Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet Glob Health. 2022;10(2):e195-206.
Hug L, Alexander M, You D, Alkema L, for Child UI. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: a systematic analysis. Lancet Global Health. 2019;7(6):e710-20.
Hatt L, Johns B, Connor C, Meline M, Kukla M, Moat K. Impact of health systems strengthening on health. Bethesda: Health Finance and Governance Project, Abt Associates Inc.; 2015.
Bassett MT, Gallin EK, Adedokun L, Toner C. From the ground up: strengthening health systems at district level. BMC Health Serv Res. 2013;13(2):1–4.
Rwabukwisi FC, Bawah AA, Gimbel S, Phillips JF, Mutale W, Drobac P. Health system strengthening: a qualitative evaluation of implementation experience and lessons learned across five African countries. BMC Health Serv Res. 2017;17(3):77–89.
Sherr K, Fernandes Q, Kanté AM, Bawah A, Condo J, Mutale W. Measuring health systems strength and its impact: experiences from the African Health Initiative. BMC Health Serv Res. 2017;17(3):29–38.
De Savigny D, Adam T, editors. Systems thinking for health systems strengthening. Geneva: World Health Organization; 2009.
Awoonor-Williams JK, Bawah AA, Nyonator FK, Asuru R, Oduro A, Ofosu A, Phillips JF. The Ghana essential health interventions program: a plausibility trial of the impact of health systems strengthening on maternal & child survival. BMC Health Serv Res. 2013;13(2):1–2.
Ramsey K, Hingora A, Kante M, Jackson E, Exavery A, Pemba S, Manzi F, Baynes C, Helleringer S, Phillips JF. The Tanzania Connect Project: a cluster-randomized trial of the child survival impact of adding paid community health workers to an existing facility-focused health system. BMC Health Serv Res. 2013;13(2):1–4.
Stringer JS, Chisembele-Taylor A, Chibwesha CJ, Chi HF, Ayles H, Manda H, Mazimba W, Schuttner L, Sindano N, Williams FB, Chintu N. Protocol-driven primary care and community linkages to improve population health in rural Zambia: the Better Health Outcomes through Mentoring and Assessment (BHOMA) project. BMC Health Serv Res. 2013;13(2):1.
Lassi ZS, Bhutta ZA. Community-based intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. Cochrane Database Syst Rev. 2015;3:CD007754.
Kanté AM, Exavery A, Jackson EF, Kassimu T, Baynes CD, Hingora A, Phillips JF. The impact of paid community health worker deployment on child survival: the connect randomized cluster trial in rural Tanzania. BMC Health Serv Res. 2019;19(1):1–4.
Kirkwood BR, Manu A, ten Asbroek AH, Soremekun S, Weobong B, Gyan T, Danso S, Amenga-Etego S, Tawiah-Agyemang C, Owusu-Agyei S, Hill Z. Effect of the Newhints home-visits intervention on neonatal mortality rate and care practices in Ghana: a cluster randomised controlled trial. Lancet. 2013;381(9884):2184–92.
Bawah AA, Awoonor-Williams JK, Asuming PO, Jackson EF, Boyer CB, Kanmiki EW, Achana SF, Akazili J, Phillips JF. The child survival impact of the Ghana essential health interventions program: a health systems strengthening plausibility trial in Northern Ghana. PLoS One. 2019;14(6):e0218025.
Lassi ZS, Haider BA, Bhutta ZA. Community-based intervention packages for reducing maternal morbidity and mortality and improving neonatal outcomes. J Dev Effect. 2012;4(1):151–87.
Ergo A, Eichler R, Koblinsky M, Shah N. Strengthening health systems to improve maternal, neonatal and child health outcomes: a framework. Washington, DC: MCHIP, USAID; 2011.
Roberts MJ, Hsiao W, Berman P, Reich MR. Getting health reform right: a guide to improving performance and equity. New York: Oxford University Press; 2008.
Barber S. Health system strengthening interventions: making the case for impact evaluation. Geneva: The Alliance for Health Policy and Systems Research; 2007.
Bryce J, Victora CG, Habicht JP, Black RE, Scherpbier RW. Programmatic pathways to child survival: results of a multi-country evaluation of integrated management of childhood illness. Health Policy Plan. 2005;20(suppl_1):i5-17.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1–9.
Gebremeskel AT, Omonaiye O, Yaya S. Sex differences in HIV testing among elders in Sub-Saharan Africa: a systematic review protocol. Syst Rev. 2022;11(1):1–6.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):1–1.
World Health Organisation. Strengthening health systems to improve health outcomes. WHO’s framework for action; 2007. https://apps.who.int/iris/bitstream/handle/10665/43918/9789241596077_eng.pdf?sequence=1. Accessed 11 Jun 2023.
Fedak KM, Bernal A, Capshaw ZA, Gross S. Applying the Bradford Hill criteria in the 21st century: how data integration has changed causal inference in molecular epidemiology. Emerg Themes Epidemiol. 2015;12:1–9.
Nowinski CJ, Bureau SC, Buckland ME, Curtis MA, Daneshvar DH, Faull RL, Grinberg LT, Hill-Yardin EL, Murray HC, Pearce AJ, Suter CM. Applying the Bradford Hill criteria for causation to repetitive head impacts and chronic traumatic encephalopathy. Front Neurol. 2022;22(13):938163.
Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, Britten N, Roen K, Duffy S. Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC methods programme Version. 2006;1(1):b92. https://www.lancaster.ac.uk/media/lancaster-university/contentassets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf.
World Health Organisation. Children: improving survival and well-being. Geneva: WHO; 2020
UNICEF. Levels and trends in child mortality: estimates developed by the UN inter-agency group for child mortality estimation. New York: UN Inter-agency Group for Child Mortality Estimation; 2017.
Salvalaggio G, Ferguson L, Brooks HL, Campbell S, Gladue V, Hyshka E, Lam L, Morris H, Nixon L, Springett J. Impact of health system engagement on the health and well-being of people who use drugs: a realist review protocol. Syst Rev. 2022;11(1):66.
Acknowledgements
This protocol paper is one of the products of the first author’s (Caesar Agula) doctoral training, which has been sponsored by the German Academic Exchange Service (DAAD).
Funding
No funding has been received for this systematic review.
Author information
Authors and Affiliations
Contributions
CA substantially contributed to the conception of the study, methods, analysis, and wrote the initial draft of the protocol. AAB, POA, PK, and AB contributed to the methodology. CA and AB contributed to revising the manuscript for important intellectual content. AAB provided leadership and direction, and CA had the final responsibility to submit the protocol for publication. All authors read and approved this final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA-P checklist.
Additional file 2.
Tested search strategy.
Additional file 3.
PRISMA 2020 flow chart for systematic reviews.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Agula, C., Bawah, A.A., Asuming, P.O. et al. Impact of health system strengthening interventions on child survival in sub-Saharan Africa: a systematic review protocol. Syst Rev 13, 15 (2024). https://doi.org/10.1186/s13643-023-02397-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-023-02397-w