
Abstract
Background
International guidelines promote preoperative education for patients undergoing orthopedic surgery. However, the evidence sustaining these recommendations comes mainly from studies for hip and knee replacement surgery. Little is known about patients undergoing foot and ankle surgery. We aimed to map and characterize all the available evidence on preoperative education for patients undergoing foot and ankle surgery.
Methods
This study complies with the PRISMA-ScR guidelines. We searched eight databases, including MEDLINE, Embase, and CENTRAL. We performed cross-citations and revised the references of included studies. We included studies addressing preoperative education in patients undergoing foot and ankle surgery. We did not exclude studies because of the way of delivering education, the agent that provided it, or the content of the preoperative education addressed in the study. Two independent authors screened the articles and extracted the data. The aggregated data are presented in descriptive tables.
Results
Of 1596 retrieved records, only 15 fulfilled the inclusion criteria. Four addressed preoperative education on patients undergoing foot and ankle surgery and the remaining 11 addressed a broader population, including patients undergoing foot and ankle surgery but did not provide separate data of them. Two studies reported that preoperative education decreases the length of stay of these patients, another reported that education increased the knowledge of the participants, and the other leaflets were well received by patients.
Conclusion
This scoping review demonstrates that evidence on preoperative education in foot and ankle surgery is scarce. The available evidence supports the implementation of preoperative education in patients undergoing foot and ankle surgery for now. The best method of education and the real impact of this education remain to be determined.
Similar content being viewed by others


Background
Preoperative education refers to any educational process that healthcare professionals deliver to patients before surgery to improve their knowledge of the procedure, health behaviors, and clinical outcomes [1, 2]. It may have several benefits, such as reducing patients’ anxiety, lowering postoperative pain, improving patients’ satisfaction, and improving other outcomes depending on the performed surgery [2,3,4,5,6,7]. There are many ways to deliver education to patients: perform face-to-face teaching, yield written or pictorial information, establish surgery schools, and produce digital data (e.g., DVDs or online videos), among others [2]. The education content may vary between health centers and by the patient’s illness.
The Enhanced Recovery After Surgery (ERAS) Society suggests that education should be carried out with a multidisciplinary approach in orthopedics surgery: with physiotherapists, occupational therapists, and nurses [2]. It should consider “joint schools” and be undertaken by small groups focusing on patient expectations and postoperative recovery [2].
Mostly, evidence from preoperative education for total hip and knee arthroplasty studies supports these guidelines [8,9,10,11,12,13]. Multiple studies addressing preoperative education for total hip and knee have been published and widely diffused later [14,15,16,17]. However, evidence specifically regarding preoperative education for patients undergoing foot and ankle surgery is less widespread and has not been summarized yet.
There is a vast spectrum of different foot and ankle orthopedic surgeries, with a high rate of elective procedures [18]. Patients undergoing elective foot and ankle procedures may be exposed to preoperative education, but there is no evidence-based recommendation to guide education in this group of patients.
This scoping review aims to identify and describe all the available evidence addressing preoperative education in patients undergoing foot and ankle surgery.
Methods
Study design
This manuscript is a scoping review addressing the studies about preoperative education on patients undergoing foot and ankle surgery. It complies with the PRISMA-ScR extension for reporting scoping reviews [19]. A protocol for this study was previously published in Open Science Framework [20].
Eligibility criteria
We included all published and ongoing available studies addressing preoperative education on patients undergoing foot and ankle surgery. We also included all available studies addressing preoperative education on patients undergoing any orthopedic surgery, including those patients undergoing foot and ankle surgery, even if they do not present separate data from this population.
We considered preoperative education any intervention aimed to improve patients’ knowledge about their surgery or patient outcomes. Therefore, we excluded studies addressing how to deliver proper informed consent to the patient. We did not exclude studies because of the way of delivering education, the agent that provided it, or the content of the preoperative education addressed in the study.
We included studies written in any language; those in a language different than English, Spanish, or French were translated with Google translator.
We included every study addressing our question with any original methodological design (primary or secondary), excluding narrative reviews, opinion articles, and letters to the editor.
Data sources and search strategies
We conducted electronic searches in databases to identify studies. Studies were not excluded based on their language of publication or publication status.
The searches were conducted in the databases below:
-
MEDLINE (Ovid) (1946 to November 2021)
-
Embase (Elsevier.com) (1974 to November 2021)
-
Latin American and Caribbean Literature in Health Sciences (LILACS), from 1982 to November 2021)
-
Education Resources Information Center (ERIC; EBSCO) (from 1966 to November 2021)
-
ISI Web of Science (Clarivate, WoS) (from inception to November 2021)
-
Cochrane Central Register of Controlled Trials (CENTRAL) (from inception to November 2021);
To address grey literature, we performed a cross-citation search in Google Scholar and checked the references list for each included study. We also searched for unpublished and ongoing studies in the following:
-
ClinicalTrials.gov trials registry at the USA National Institutes of Health (ClinicalTrials.gov)
-
World Health Organization International Clinical Trials Registry Platform (ICTRP) (trialsearch.who.int; from inception to November 2021)
Furthermore, Embase database retrieves abstracts from medical congress, which had widen our gray literature search.
All the strategies were peer reviewed by another senior information specialist prior to execution using the PRESS checklist [21]. For detailed search strategies, see Additional file 1.
We managed search results and removed duplicates in EndNote X9 (Clarivate).
Selection of studies
Two independent reviewers screened the titles and abstracts of studies retrieved from the search with the aid of Rayyan [22]. Two independent reviewers then selected the studies by reading the full text of potentially eligible studies. If there was a discrepancy during any selection process step, a third reviewer decided whether to include or exclude the study. We registered the reasons for exclusion throughout the whole process. We present the selection process in a PRISMA flow diagram [23].
Data extraction and presentation
Two authors independently extracted all the relevant data from included studies in a previously piloted chart. In case of disagreement, the two reviewers revised the study together and amended the data.
We extracted the following general data from all the included studies: authors, year of publication, type of publication, journal, language, country, number of participants, inclusion and exclusion criteria, and measured outcomes in each study when possible.
For selecting the data about preoperative education to be extracted, we followed the template for intervention description and replication (TIDieR) checklist and guide [24]. However, we did not extract all the items because of the specificities and scope of our study. This way, the items we extracted were as follows: the diagnosis of included participants, which surgery the patients underwent, the surgeon profession (e.g., orthopedic surgeon, podiatrist, general surgeon), the method of education delivered, used materials, who delivered the education, when it was delivered (e.g., a week before surgery, a month before surgery), where it was delivered, and the number of sessions received by the participants. Finally, we extracted the main conclusions of each included study. All the data are presented in descriptive tables.
We did not combine any results of included studies, and we did not assess the risk of bias of each included study, nor the certainty of the evidence, because this was out of the scope of our review.
Results
Our electronic searches retrieved 1578 records. We selected 42 full-text reports after eliminating duplicates and title and abstract screening. We included eight studies after reading those 42 full text. Exclusion details are shown in Additional file 2. Also, we retrieved 18 potentially relevant studies by cross-citation or references checking, and seven of them fulfilled the inclusion criteria after full-text revision, as detailed in Additional file 3. This way, 15 studies were included in our review (Fig. 1) [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39].

PRISMA flow diagram
The general demographics of the included studies are shown in Table 1. All but one studies were published in English [25,26,27,28,29,30,31, 33,34,35,36,37,38,39], and most of them assessed a broader population than only patients undergoing foot and ankle surgery [25,26,27,28,29,30,31, 33, 37,38,39]. Six of 15 studies were carried out in Europe [32, 34,35,36], five [26,27,28,29, 31] in the USA, three [37,38,39] in Asia, and one [30] in Africa. Figure 2 shows the date of publication of studies separated by continent. Below, we present separately the studies that exclusively address patients undergoing foot and ankle surgery (Table 2) and those addressing a broader population (Table 3).

Publication date of studies by continent
Studies addressing exclusively patients undergoing foot and ankle surgery
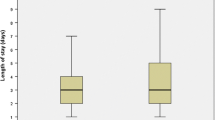
Only four [17, 32, 34,35,36] of the 15 studies included patients undergoing foot and ankle surgery exclusively. Three [34,35,36] of these four studies were conducted in the UK and one [32] in Germany. Three [34,35,36] were observational studies, and one [32] had a quasi-experimental design. The included patients ranged from 56 [32] to 161 [35]. Regarding the primary outcome of each study, two evaluated the length of stay [34, 36], one evaluated the knowledge growth [32], and the other mainly assessed the readability and understanding of the preoperative information sheets [35]. The main characteristics, the evaluated education intervention, and the principal conclusions of the included studies assessing patients undergoing foot and ankle surgeries are shown in Table 2.
Overall, these four studies reported positive results: Speirs et al. [35] concluded that preoperative information sheets were well received by patients undergoing foot and ankle surgery, Thomas et al. [36] and Selvan et al. [34] demonstrated that preoperative education—in the form of foot school and a preoperative session respectively—reduced length of stay in the hospital, and Schafer et al. [32] concluded that patients’ knowledge and satisfaction improved with one formal session of preoperative education.
Studies addressing patients undergoing any orthopedic surgery, including foot and ankle procedures
Eleven studies [25,26,27,28,29,30,31, 33, 37,38,39] included patients undergoing orthopedic surgery, including foot and ankle procedures. However, none of these studies presents separate data from patients undergoing specifically foot and ankle surgery, nor specify how many of their included participants underwent foot and ankle surgery.
All of these studies were published in English, three [27, 29, 30] were randomized clinical trials, five [26, 31, 37,38,39] had a quasi-experimental design, and the rest were observational studies [25, 28, 33]. The main characteristics of each study are shown in Table 3 and complemented with more detailed data in Additional file 4.
Regarding the primary outcome reported by each study, four evaluated [30, 37,38,39] the postoperative pain level, two [26, 27] specifically evaluated the use of opioids after surgery, and the others primarily assessed patient expectation [25], compliance [28], satisfaction [29], amount of information received [33], or empowerment [31].
Discussion
Our study characterizes and resumes the existing literature after a broad and reproducible search in multiple databases and a careful screening and full-text selection process. This study is the first to map the available evidence of preoperative education for patients undergoing foot and ankle surgery. We found four [17, 32, 34,35,36] studies that specifically assessed different forms of preoperative education in patients undergoing foot and ankle surgery and 11 [25,26,27,28,29,30,31, 33, 37,38,39] studies that evaluated this in a broader population that included patients undergoing foot and ankle surgery, but that did not provide separate data of these patients.
Regarding the reported outcomes, as mentioned in the results section, the four studies including only foot and ankle surgery patients reported positive results with preoperative education. These results could vary with further studies because of the small sample sizes of the included studies. It is remarkable that the evaluated outcomes in all the included studies in our review varied widely (e.g., level of pain, length of stay, patient knowledge). This heterogeneity in the evaluated outcomes would make it very difficult to extrapolate, to compare, and—eventually—to combine the studies’ results. A way to homogenize the outcomes and to overcome the aforementioned difficulties could be to use patient-reported outcomes measures (PROM), which was already encouraged by the American Orthopedic Foot and Ankle Society (AOFAS) [40].
Furthermore, there was also a wide heterogeneity among each evaluated education intervention, going from foot school [36] to delivering a leaflet at the moment of informed consent [35]. As the interventions are heterogeneous and we did not find any study that compares different methods of education, the real impact of each of these educational methods remains to be determined. Some authors [17] have already suggested that preoperative education should consist of a live class to improve patient experience and reduce costs. This suggestion stands out from the diversity of educational interventions for all orthopedic surgeries, making it challenging to provide evidence-based recommendations.
Even though the existing evidence for preoperative education in foot and ankle surgery is scarce, evidence of preoperative education in other specialties of orthopedic surgery is slightly broader. It is outstanding that the four studies specifically addressing preoperative education for patients undergoing foot and ankle surgery were conducted in Europe. When comparing this with other orthopedics fields, already in 2014, a Cochrane systematic review published assessed preoperative education for hip or knee replacement [13], including 18 trials that were conducted mostly in Europe and North America (all randomized or quasi-randomized trials). This shows that evidence on preoperative education for other orthopedic surgeries is more substantial and of better quality than the included evidence regarding patients undergoing foot and ankle surgery in our study. However, for both patients undergoing foot and ankle surgeries or other orthopedic specialties, evidence regarding preoperative education comes from developed countries. In Cochrane’s systematic review mentioned above, despite the more extensive availability of data, the evidence for all the assessed outcomes—for both hip and knee replacement—was graded as low or very low quality of evidence, meaning that further studies are very likely to impact their estimated effects. Finally, the included studies in our review and the evidence for other orthopedic specialties make us question if preoperative education offers benefits over usual care. But, besides this reasonable doubt, it must be recognized that preoperative education might be a helpful adjunct with low risk of undesirable effects.
Further studies addressing preoperative education for patients undergoing foot and ankle surgery are needed to conclude about its effectiveness. We specifically suggest conducting prospective studies, either interventional or observational, on patients undergoing foot and ankle elective orthopedic surgery. First, these studies may compare a standardized educational method (e.g., foot school, nurse education session, video-recorded sessions) against the actual standard of care in a specific center (even if this is no formal educational). In places where a specific preoperative education tool is already in use, different formal education methods may be compared to address which tool is more effective. Regarding the evaluated outcomes in future studies, we encourage that future studies address PROMs as mentioned above; this may allow standardization of measurements and a combination of multiple studies results [40]. Authors should also measure patient satisfaction with the evaluated intervention, pain, use of analgesics (especially opioids), and length of hospital stay because all these outcomes are clinically relevant to decision-making. The outcomes should be measured at standardized time intervals, either preoperative when possible or postoperative. Taking into account these considerations, future studies may elucidate the real impact of preoperative education in this specific population.
A limitation of our study is that we did not assess the risk of bias in each included article. However, this was beyond the scope of our review, as we aimed to map, identify, and characterize all the existing evidence for preoperative education in patients undergoing foot and ankle surgery—which we properly accomplished.
Conclusion
The available evidence on preoperative education for patients undergoing foot and ankle surgery is scarce and heterogeneous. However, this—very limited—evidence provides favorable outcomes regarding the length of hospital stay and patient knowledge and satisfaction. Further studies are needed to establish whether preoperative education positively impacts patients undergoing foot and ankle surgery and which methods are more effective for this purpose.
More studies addressing preoperative education in patients undergoing foot and ankle surgery are required to evidence-based recommend its use. With the (scarce) existent evidence, foot and ankle orthopedic surgeons should ensure that their patients receive preoperative education as it may decrease the length of stay in the hospital and increase the patient’s knowledge of the procedure.
Availability of data and materials
Not applicable.
References
Oshodi TO. The impact of preoperative education on postoperative pain. Part 1. Br J Nurs. 2007;16(12):706–10.
Ljungqvist O, Francis NK, Urman RD. Enhanced recovery after surgery. a complete guide to optimizing outcomes. Switzerland AG: Springer Nature; 2020.
Guo P, East L, Arthur A. A preoperative education intervention to reduce anxiety and improve recovery among Chinese cardiac patients: a randomized controlled trial. Int J Nurs Stud. 2012;49(2):129–37.
Sjoling M, Nordahl G, Olofsson N, Asplund K. The impact of preoperative information on state anxiety, postoperative pain and satisfaction with pain management. Patient Educ Couns. 2003;51(2):169–76.
Forsmo HM, Erichsen C, Rasdal A, Tvinnereim JM, Korner H, Pfeffer F. Randomized controlled trial of extended perioperative counseling in enhanced recovery after colorectal surgery. Dis Colon Rectum. 2018;61(6):724–32.
Gardner TF, Nnadozie MU Sr, Davis BA, Kirk S. Patient anxiety and patient satisfaction in hospital-based and freestanding ambulatory surgery centers. J Nurs Care Qual. 2005;20(3):238–43.
Iqbal U, Green JB, Patel S, Tong Y, Zebrower M, Kaye AD, Urman RD, Eng MR, Cornett EM, Liu H. Preoperative patient preparation in enhanced recovery pathways. J Anaesthesiol Clin Pharmacol. 2019;35(Suppl 1):S14–23.
Wainwright T, Middleton R. An orthopaedic enhanced recovery pathway. Curr Anaesth Crit Care. 2010;21(3):114–20.
Place K, Scott N. Enhanced recovery for lower limb arthroplasty. Cont Educ Anaesth Crit Care Pain. 2014;14(3):95–9.
Chen A, Sabharwal S, Akhtar K, Makaram N, Gupte CM. Time-driven activity based costing of total knee replacement surgery at a London teaching hospital. Knee. 2015;22(6):640–5.
Galbraith AS, McGloughlin E, Cashman J. Enhanced recovery protocols in total joint arthroplasty: a review of the literature and their implementation. Ir J Med Sci. 2018;187(1):97–109.
Brennan C, Parsons G. Enhanced recovery in orthopedics: a prospective audit of an enhanced recovery program for patients undergoing hip or knee arthroplasty. Medsurg Nurs. 2017;26(2):99–104.
McDonald S, Page MJ, Beringer K, Wasiak J, Sprowson A. Preoperative education for hip or knee replacement. Cochrane Database Syst Rev. 2014;2014(5):CD003526.
Causey-Upton R, Howell DM, Kitzman PH, Custer MG, Dressler EV. Preoperative education for total knee replacement: a national survey of orthopaedic nurses. Orthop Nurs. 2020;39(1):23–34.
Dayucos A, French LA, Kelemen A, Liang Y, SikLanyi C. Creation and evaluation of a preoperative education website for hip and knee replacement patients-a pilot study. Medicina (Kaunas). 2019;55(2):32.
Edwards PK, Levine M, Cullinan K, Newbern G, Barnes CL. Avoiding readmissions-support systems required after discharge to continue rapid recovery? J Arthroplasty. 2015;30(4):527–30.
Edwards PK, Mears SC, Lowry Barnes C. Preoperative education for hip and knee replacement: never stop learning. Curr Rev Musculoskelet Med. 2017;10(3):356–64.
Burton A, Aynardi MC, Aydogan U. Demographic distribution of foot and ankle surgeries among orthopaedic surgeons and podiatrists: a 10-year database retrospective study. Foot Ankle Spec. 2021;14(3):206–12.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Moher D, Peters MDJ, Horsley T, Weeks L, et al. PRISMA extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
Vergara-Merino L, Lira MJ, Escobar-Liquitay C, et al. Preoperative education in patients undergoing foot and ankle surgery: a scoping review protocol. In: Open Science Framework. 2021.
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40–6.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, Altman DG, Barbour V, Macdonald H, Johnston M, et al. Better reporting of interventions: Template for Intervention Description and Replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687.
Heikkinen K, Leino-Kilpi H, Hiltunen A, Johansson K, Kaljonen A, Rankinen S, Virtanen H, Salantera S. Ambulatory orthopaedic surgery patients’ knowledge expectations and perceptions of received knowledge. J Adv Nurs. 2007;60(3):270–8.
Holman JE, Stoddard GJ, Horwitz DS, Higgins TF. The effect of preoperative counseling on duration of postoperative opiate use in orthopaedic trauma surgery: a surgeon-based comparative cohort study. J Orthop Trauma. 2014;28(9):502–6.
Ilyas AM, Chapman T, Zmistowski B, Sandrowski K, Graham J, Hammoud S. The effect of preoperative opioid education on opioid consumption after outpatient orthopedic surgery: a prospective randomized trial. Orthopedics. 2021;44(2):123–7.
Laude K, Buchholz SW, Rodts M. Improving patient education at a large Midwest Urban Orthopaedic Center. Orthop Nurs. 2017;36(2):133–9.
Morris BJ, Richards JE, Archer KR, Lasater M, Rabalais D, Sethi MK, Jahangir AA. Improving patient satisfaction in the orthopaedic trauma population. J Orthop Trauma. 2014;28(4):e80-84.
Othin M, Sendagire C, Mukisa J, et al. Effect of preoperative information about pain on postoperative pain experience and patient satisfaction following orthopaedic surgery: a randomised controlled trial. In: Research Square. 2020.
Pellino T, Tluczek A, Collins M, et al. Increasing self-efficacy through empowerment. Orthop Nurs. 1998;17(4):48–59.
Schäfer A, Jettkowski K, Kretschmann J, Wurg M, Stukenborg-Colsmann C, Plaaß C. Development and evaluation of interdisciplinary preoperative patient education in foot and ankle surgery: immediate effects on knowledge, satisfaction and anxiety / Entwicklung und erste Evaluation eines präoperativen interdisziplinären Schulungskonzeptes für Patienten/-innen der Fußchirurgie: unmittelbare Effekte auf Wissenszuwachs, Zufriedenheit und Angst. International Journal of Health Professions. 2017;4(1):25–32.
Scott A. How much information is too much information for patients? J Integr Care Pathw. 2001;5(3):119–25.
Selvan D, Molloy A, Abdelmalek A, Mulvey I, Alnwick R. The effect of preoperative foot and ankle physiotherapy group on reducing inpatient stay and improving patient care. Foot Ankle Surg. 2013;19(2):118–20.
Speirs S, Rees S, Tagoe M. An audit of foot surgery information leaflets from the patients’ perspective. Foot. 2008;18(1):7–14.
Thomas T, Khan S, Saldanha K, Ballester JS, Stott R, Morgan S. Foot school: preoperative education before day case elective foot and ankle surgery reduces the length of stay after surgery. Foot (Edinb). 2022;50:101893.
Wong EM, Chair SY, Leung DY, Chan SW. Can a brief educational intervention improve sleep and anxiety outcomes for emergency orthopaedic surgical patients? Contemp Nurse. 2014;47:132–43.
Wong EM, Chan SW, Chair SY. Effectiveness of an educational intervention on levels of pain, anxiety and self-efficacy for patients with musculoskeletal trauma. J Adv Nurs. 2010;66(5):1120–31.
Wong EM, Chan SW, Chair SY. The effect of educational intervention on pain beliefs and postoperative pain relief among Chinese patients with fractured limbs. J Clin Nurs. 2010;19(17–18):2652–5.
Lakey E, Hunt KJ. Patient-reported outcomes in foot and ankle orthopedics. Foot Ankle Orthop. 2019;4(3):2473011419852930.
Acknowledgements
The authors would like to thank the Orthopedic Surgery Department of the Pontificia Universidad Católica de Chile for encouraging them to perform this research. The authors also thank Eva Madrid for her review and feedback of the original manuscript.
Funding
This project did not receive any funding.
Author information
Authors and Affiliations
Contributions
LVM, conceptualization, methodology, validation, formal analysis, investigation, data curation, writing—original draft, visualization, and project administration. ML, validation, formal analysis, investigation, data curation, and writing—review and editing. CEL, validation, formal analysis, investigation, data curation, and writing—review and editing. NGK, validation, formal analysis, investigation, data curation, and writing—review and editing. SM, conceptualization, methodology, writing—review and editing, supervision, and project administration. All the authors read and approved the final version of this manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search strategies.
Additional file 2.
Reports assessed for eligibility and reasons for exclusion.
Additional file 3.
Cross citation (scholar google) and review of included studies references.
Additional file 4.
Detailed data of studies addressing patients undergoing any orthopedic surgery, including foot and ankle procedures but not providing specific data of them.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Vergara-Merino, L., Lira, M.J., Liquitay, C.M.E. et al. Preoperative education in patients undergoing foot and ankle surgery: a scoping review. Syst Rev 12, 210 (2023). https://doi.org/10.1186/s13643-023-02375-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-023-02375-2