
Abstract
Background
The Community Attitudes to Mental Illness (CAMI) scale measures social stigma towards people with mental illness. Although it has been used worldwide, the psychometric properties of the CAMI have not been systematically reviewed. The main aim of this study was to systematically review the psychometric properties of the different versions of the CAMI more than 40 years after of its publication.
Methods
A systematic search was conducted in MEDLINE, PsycINFO, Web of Science, and EMBASE from 1981 (year of publication) to 2023 (present). A double review was performed for eligibility, data extraction, and quality assessment.
Results
A total of 15 studies enrolling 10,841 participants were included. The most frequently reported factor structure comprises 3 or 4 factors. Overall, the internal consistency seems adequate for the global scale (α ≥ 0.80), except for CAMI-10 (α = 0.69). Internal consistency of the subscales are not supported, with authoritarianism being the weakest factor (α = 0.27 to 0.68). The stability over time of the total scale has been assessed in the CAMI-40, CAMI-BR, and CAMI-10 (r ≥ 0.39). Few studies have assessed the temporal stability of the CAMI subscales. Most of the correlations with potentially related measures are significant and in the expected direction.
Conclusions
The 3 and 4 factor structure are the most widely reported in the different versions of the CAMI. Even though reliability and construct validity are acceptable, further item refinement by international consensus seems warranted more than 40 years after the original publication.
Systematic review registration
PROSPERO identification number: CRD42018098956.
Similar content being viewed by others

Introduction
Stigma towards people with mental disorders is a sociocultural phenomenon [1, 2] that negatively affects quality of life, self-esteem, interpersonal relationships, health care seeking and provision, and workplace integration [3, 4]. In Europe, it is estimated that there are about 165 million people with mental disorders, and it is calculated that around 38% of people will experience a mental disorder in their lifetime [5]. A recent systematic review confirmed that mental disorders cause a substantial economic burden for societies, with developmental disorders, schizophrenia, and intellectual disabilities obtaining the top median societal cost per patient [6].
Although there is not a universally accepted definition of stigma, it can be considered a multidimensional construct composed of negative elements of knowledge, attitudes, feelings, beliefs, and behaviours towards a group of people [7]. Stigma is a powerful barrier to social participation and professional help-seeking for people with mental disorders and there is a widespread social belief that such people are aggressive and uncontrollable [8,9,10,11,12]. In the last decade, various countries have implemented antidiscrimination campaigns to reduce stigma and improve the integration of people with mental illness into communities [13]. Examples of such programmes are Time to Change in England [14]; Obertament in Spain [15]; Schizophrenia has many faces in Austria [16]; Like minds like mine in New Zealand [17]; One of us in Denmark [18]; and Opening minds in Canada [19].
There is a long history of scales developed to assess attitudes towards mental illness. The Opinion about Mental Illness (OMI) [20] and the Custodial Mental Illness Ideology Scale (CMI) [21] were developed in the 1950s–1960s as the first scales to measure stigma. More recently, the Community Mental Health Ideology (CMHI) [22], the Community Attitudes to Mental Illness Scale (CAMI) [23], the Mental Health Knowledge Schedule (MAKS) [24], and the California Assessment of Stigma Change (CASC) [25] were designed. Since its publication in 1981, the CAMI [23] has been the gold standard measure for assessing stigma towards people with mental disorders. It has been translated into several languages (Spanish, Italian, Swedish, Portuguese, Greek, and Persian, among others) and used to measure stigma in a wide variety of samples (e.g., nurses, psychiatrists, and relatives of psychiatric patients).
The original version of the CAMI was partially derived from a brief, revised, and updated version of the OMI [20], and it was initially developed to predict the reactions of the general population to local services for people with severe mental disorders. This original version is composed of 40 items that are responded on a 5-point Likert scale, ranging from “strongly agree” to “strongly disagree”. According to its developers, the CAMI contains four subscales: authoritarianism, benevolence, social restrictiveness, and community mental health ideology [23]. Each subscale contains 10 items (5 positively formulated plus 5 negatively formulated) on the opinions of treating and caring for people with a serious mental disorder. Therefore, subscale scores can range from 10 to 50, with higher scores indicating less stigma towards people with mental disorders.
Given that the CAMI has been available for more than four decades, with hundreds of citations, the time is right for a systematic review of the psychometric properties of its different versions. As far as it is known, there are no previous reviews summarizing available psychometric information on the CAMI. This systematic review bridges this gap by synthesizing and critically appraising the psychometric properties of this stigma scale.
Method
Protocol and registration
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines (PRISMA) [26]. The review protocol was registered in Prospective Register of Systematic Reviews (PROSPERO) on July 25th, 2018, under identification number: CRD42018098956.
Search strategy
Searches were conducted through four electronic databases: MEDLINE (PubMed), PsycINFO (ProQuest), Web of Science (Core Collection), and EMBASE (Elsevier). The search strategy included terms related to psychometrics (psychometrics OR factor analysis OR reliability OR intra-class OR test–retest OR internal consistency OR validity OR dimensionality OR sensitivity to change OR responsiveness OR sensibility OR specificity) and to the original scale name ((attitude* AND toward* AND mental* AND Ill*) OR ("CAMI")), found using keywords in all fields and in the Medical Subject Headings (MeSH). The search string used in MEDLINE (PubMed) is shown in the Supplementary Table S1. Limits and filters were not activated in any of the database searches to avoid loss of potential eligible studies. The references of included studies were screened by reverse citation search to identify studies not detected in the electronic searches.
Eligibility criteria
The search in the databases incorporated studies published in peer-reviewed journals from 1981 (when the original version was published [23]) to February 28th, 2023 (present). This systematic review included all studies that provided evidence on the psychometric properties (content validity, factor structure, internal consistency, test–retest reliability, construct validity, floor/ceiling effects, and interpretability) of the different versions of the CAMI. No restrictions were placed on the characteristics of the participants and the type of sampling used in the search. To ensure the rigour of the included studies, non-original studies (reviews, books, doctoral dissertations, commentaries, conference abstracts, study protocols, case reports, and qualitative studies, among others) and grey literature (i.e., non-peer-reviewed manuscripts) were excluded. Non-English, non-Spanish, or non-Italian papers were also excluded.
Data management and study selection
In the first phase, duplicate articles in the databases were removed using Mendeley. In the second phase, two reviewers (AB and NA–O) independently assessed the articles based on their title and abstract according to the eligibility criteria. In the third phase, the full text of those articles that met the second phase was reviewed to verify compliance with the eligibility criteria. In the fourth phase, discrepancies in study selection were resolved with the help of two additional external reviewers (JVL and MR-V). In the fifth phase, relevant data were extracted from the selected documents with a standardised data extraction form and the respective quality assessment was carried out for each study.
Data extraction
Data extraction from the selected articles was performed independently by two reviewers (AB and NA–O), using a template containing the following sections: authors, year of publication, country, CAMI version, study design, target population, sample type, sample size, age, gender, results depending on sociodemographic variables, and psychometric results about CAMI. The authors of the study were contacted to obtain additional information on the psychometric properties of the scale when it was necessary.
Quality assessment
The quality of the included studies was assessed using the criteria proposed by Terwee et al. [27] for health measures. Each of the 7 criteria is scored 2 if the criteria are fulfilled, 1 if they are partially fulfilled, and 0 if no criteria are fulfilled. The total score can range from 0 to 14. The quality assessment was carried out by two reviewers (JPS-M and AB), with the supervision of two external reviewers (JVL and MR-V). Specifically, the following psychometric properties were assessed:
-
1.
Content validity indicates whether the construct of interest is sampled by the questionnaire items. A score of 2 was assigned if the measurement objective of the questionnaire and the target population were explicitly defined. For this criterion to be met, it was necessary to develop the questionnaire items in consensus with the general population and stigma experts [27]. A score of 1 was given if some of the aspects mentioned above were missing and a score of 0 if none of the above information was described.
-
2.
Factor structure refers to the dimensionality of the scale [27]. A score of 2 was given if an exploratory factor analysis (EFA) and a confirmatory factor analysis (CFA) had been performed on different samples or if the CFA had been calculated considering a theoretical model. This score was only given if the factor analyses supported the structure promoted by the authors. A score of 1 was awarded if only the EFA had been carried out, and if the EFA supported the factor structure. A score of 0 was awarded if factor analysis has not been conducted or if EFA or CFA does not support the proposed dimensionality.
-
3.
Internal consistency is used to indicate the degree of reliability of a scale. For health scales, Cronbach’s α should be between 0.70 and 0.95 [27]. For greater rigour in the findings, the Nunnally and Bernstein [28] criteria were used in this study, which present scores above 0.80 as acceptable. A score of 2 was given if Cronbach's α was calculated for each dimension and if it was between 0.80 and 0.95. A score of 1 was assigned if internal consistence was calculated only for some dimensions and if it was below 0.80. A score of 0 was reported if no internal consistency information was found or if the evidence was questionable.
-
4.
Test–retest reliability is a measure used to validate the stability of the scale over time. For acceptable temporal stability, the test–retest needs to be at least r = 0.70 [27, 29]. The intraclass correlation coefficient (ICC) is the most recommended statistical index for continuous measures in the assessment of temporal stability. To reduce possible recall bias, a score of 2 was indicated if the time interval between test administration was 1–2 weeks. A score of 1 was assigned if the time interval between test administration was less than 1 week or greater than 2 weeks and a score of 0 if no information on test–retest reliability was reported.
-
5.
Construct validity addresses whether scores on a questionnaire are significantly associated with potentially related measures. A theoretical underpinning is needed to verify the hypotheses of expected correlations between different scales. At least two of the correlations between two theoretically related constructs had to have a minimum of r = 0.50 [27]. A score of 2 was given if information about convergent validity and divergent validity was provided. A score of 1 was assigned if information was provided for only one of the concepts mentioned above and score of 0 if no construct validity information was provided.
-
6.
Floor and ceiling effects is a measure to detect the number of participants achieving the highest or lowest possible scores [27]. A score of 2 was assigned if less than 15% of respondents achieved the highest or lowest possible scores. A score of 1 was reported if more than 15% of respondents achieved the highest or lowest possible scores and a score of 0 if this information was not provided.
-
7.
Interpretability indicates how differences in scores on the CAMI can be interpreted or the degree to which qualitative meaning can be obtained from quantitative scores. A known-groups validity approach is suggested with means and standard deviations (SDs) of scores of relevant subgroups of participants who are expected to differ in the CAMI [27]. A score of 2 was assigned if mean and SDs of four or more relevant groups were reported. A score of 1 was given if mean and SDs of less than four relevant groups were informed and score of 0 if no information about interpretability was found.
Results
Selection and inclusion of studies
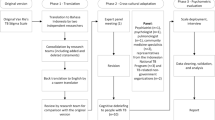
As displayed in Fig. 1, the initial database search yielded a total of 537published articles. In addition, 5 articles were included by reverse citation and 5 by experts. After removal of duplicates, 498 titles and abstracts were reviewed, of which 25 was selected for full-text review. After this process, 10 articles were excluded, 4 articles because they were not related to the CAMI, 2 because they did not focus on the psychometric properties of the scale, 2 because they did not provide relevant information, and 2 because it was written in other languages (German or Chinese). Finally, a total of 15 studies were included in this systematic review.

PRISMA flowchart from record identification to study inclusion
Characteristics of included studies
The 15 included studies were conducted in 12 different countries: Spain (n = 2), United Kingdom (n = 2), Italy (n = 1), France (n = 1), Sweden (n = 1), Ireland (n = 1), Canada (n = 1), China (n = 1), Chile (n = 1), Argentina (n = 1), Kenya (n = 1), and Iran (n = 1). Participants in most studies were healthy individuals (n = 13) and the most frequent type of sampling was non-probability (n = 12). The sample size of the studies ranged from 130 [30] to 2000 [31], enrolling a total of 10,841 participants, and the mean age ranged from 15 [32] to 48 [15] years old. The proportion of women in all studies was higher than 50%. The design of all included studies was observational.
The included studies were published between 1981 [23] and 2023 [30]. The original CAMI-40 (n = 5) [23, 30, 32,33,34] and the CAMI-20 (n = 3) [33, 35, 36] were the most psychometrically analysed versions, followed by CAMI-W (n = 2) [33, 37], CAMI-26 (n = 2) [15, 38], CAMI-BR (n = 1) [39], CAMI-31 (n = 1) [31], CAMI-10 (n = 1) [40], CAMI-24 (n = 1) [41], CAMI-22 (n = 1) [42], CAMI-1 [33], CAMI-2 [33], and CAMI-W (n = 1) [33]. In total, 14 studies examined the psychometric properties of CAMI using classical test theory [15, 23, 30,31,32,33, 35,36,37,38,39,40,41,42] and one using item response theory (IRT) [34]. Table 1 provides a detailed description of the included studies.
Quality assessment
As shown in Table 2, the overall methodological quality of the included studies was low. On a scale of 0 to 14 points, 8 studies scored 5 or less [30, 31, 33, 35, 37, 38, 41, 42] and 6 scored 6–7 [15, 23, 32, 34, 39, 40]. Only one study [36] scored higher than 10 on the quality assessment, which indicates that in general the psychometric properties of the CAMI have not been adequately assessed.
Content validity
The construct of interest in all included studies (n = 15) was the assessment of attitudes towards people suffering from mental disorders. The developers of the CAMI generated part of the scale by extracting items from previously published measures [23], whereas the subsequent versions were adaptations with different length of the original scale.
Factor structure
The dimensionality of the CAMI was assessed in most of the included articles (n = 11). Three studies computed a CFA [34, 35, 38], six opted for an EFA or principal component analysis [15, 23, 31, 37, 40, 42], and 2 computed EFA and CFA [38, 39]. The number of dimensions ranged between 2 and 5. Regarding item allocation, it was found that items loaded on different subscales depending on the version of the CAMI. Considering suggested “Rules of thumb” [41, 43], in the original CAMI (40 items distributed in 4 factors) only 26 of the 40 items had a factor loading greater than 0.40, with a difference ≥ 0.15 in the factor loadings of each item in the different factors. In addition, some items load more strongly on other factors than on the original factor assignment reported by Taylor and Dear [23].
Internal consistency
The internal consistency was assessed in 9 of the included studies. It was assessed for both the global CAMI (n = 7) [23, 30, 32, 34, 35, 39, 40] and its subscales (n = 7) [15, 23, 30, 32, 39, 40, 42]. All studies that assessed the Cronbach’s α or McDonald`s Omega (ω) of the global scale, both original CAMI-40 and its versions (i.e., CAMI-BR, CAMI-20, and CAMI-10), exceeded the minimum established by Nunnally and Bernstein [28] of 0.80, except for three studies: (ω = 0.78 for the CAMI-40) [34], (α = 0.59 for the CAMI-40) [30], and (α = 0.69 for the CAMI-10) [40]. Studies that assessed the Cronbach’s α of the subscales in the original CAMI-40 [23, 30, 32] and its versions (i.e., CAMI-26, CAMI-BR, CAMI-10, and CAMI-22) [15, 37, 39, 40] showed some heterogeneity in their coefficients. Of these, some (n = 4) [15, 30, 40, 42] reported internal consistency values below the recommended minimum cut-off point in the CAMI subscales.
On one hand, the study assessing the subscales of the CAMI-22 [42] reported internal consistency values below the minimum recommended score on benevolence (α = 0.63), non-authoritarianism (α = 0.52), non-social restrictiveness (α = 0.53), normalisation (α = 0.43), and community rehabilitation (α = 0.61). The study examining the subscales of the CAMI-10 [40] obtained alpha values below the minimum recommended cut-off point on acceptance (all α < 0.70). The study assessing the subscales of the CAMI-26 [15] reported alpha values below the recommended cut-off point on benevolence (α = 0.63), authoritarianism (α = 0.54), and support for the mental health community (α = 0.72).
On the other hand, there were studies that reported a Cronbach’s α value below the recommended cut-off only in some specific subscales of the original CAMI-40 [23, 30, 32] and the CAMI-BR [39]. The three studies [23, 30, 32] that evaluated the original CAMI indicated values below the cut-off on the dimensions of benevolence (α = 0.64 [23]; α = 0.76 [32]; α = 0.49 [30]), authoritarism (α = 0.27 [23]; α = 0.68 [32]; α = 0.61 [30]), social restrictiveness (α = 0.67 [32]; α = 0.64 [30]), and CMHI (α = 0.76 [30]). The study [39] focused on the subscales of the CAMI-BR reported very low alpha values on benevolence (α = 0.69), authoritarism (α = 0.35). In general, authoritarism is the least reliable subscale [23, 32, 39, 40, 42].
Regarding the original CAMI, two [23, 32] out of three studies that assessed its subscales reported an acceptable internal consistency on the CMHI subscale (α = 0.88; α = 0.81, respectively), while only one [23] of the two studies reported an adequate value in social restrictiveness (α = 0.80). The study [39] that assessed the reliability of the CAMI-BR subscales also reported an adequate value on the CMHI subscale (α = 0.81).
Test–retest reliability
The temporal stability was assessed in five studies [30, 32, 34, 38, 39] by computing the ICC coefficient. One study that used the original CAMI [32] calculated temporal stability on all subscales, without reporting the global coefficient: benevolence (r = 0.85), authoritarianism (r = 0.81), social restrictiveness (r = 0.81), and CMHI (r = 0.88). Other study [34] explored the temporal stability of the original CAMI in the global coefficient (r = 0.39), with questionable results, but not in its subscales. The study that evaluated the temporal stability of the original CAMI [30] reported excellent results in both the global coefficient (r = 0.93) and its subscales: authoritarianism (r = 0.97), benevolence (r = 0.92), social restrictiveness (r = 0.95), and CMHI (r = 0.95).
The study assessing temporal stability on the CAMI-BR [39] found acceptable temporal stability for the overall scale (r = 0.69). However, the subscales of benevolence (r = 0.62), authoritarianism (r = 0.37), social restrictiveness (r = 0.64), and CMHI (r = 0.54) did not exhibit good temporal stability. The temporal stability of the CAMI-10 [40] was acceptable only for the overall scale (r = 0.79), but not in the case of the subscales: benevolence (r = 0.39), authoritarianism (r = 0.57), social restrictiveness (r = 0.62), and CMHI (r = 0.63).
Construct validity
Three studies found positive statistically significant correlations of low magnitude (< 0.50) between the CAMI and potentially related instruments such as the MAKS and the Reported and Intended Behaviours Scale (RIBS). One study [40] identified correlations between the factors of the CAMI-10 (i.e., CMHI, authoritarianism, benevolence, and social restrictiveness) and the Social Dominance Orientation (SDO), with values ranging from − 0.31 to 0.16. Other study [38] found negative correlations between the CAMI-26 and instruments such as the RIBS (− 0.44) and the MAKS (− 0.30). Finally, one study [34] identified a negative correlation between original CAMI and RIBS (− 0.08) and a positive correlation with MAKS (0.09).
Floor and ceiling effects
None of the included studies reported information on ceiling and/or floor effects.
Interpretability
The interpretability was analysed from a known-groups validity approach in several studies (n = 11) [15, 23, 31, 32, 36,37,38,39,40,41,42]. For instance, older participants with low employment status and low social class have higher CAMI scores compared to younger participants and those with high employment and social status [31, 33]. Men also reported higher scores than women [15]. As expected, those participants who had undertaken volunteering or social activities scored lower than those who had not [41].
Discussion
Principal findings and interpretation
The results of this systematic review can be summarized as follows. The CAMI has been used in a wide variety of settings and in diverse samples from many different countries (i.e., Spain, United Kingdom, Italy, France, Sweden, Ireland, Canada, China, Chile, Argentina, Kenya, and Iran). The target population of included studies varied from students [32] and primary healthcare workers [33, 36] to the general population [15, 30, 31, 34, 37, 38, 40,41,42]. These aspects, besides the different CAMI versions used, might account for the heterogeneous findings in the psychometric data of this stigma measure.
In the current systematic review, a total of 15 papers met the inclusion criteria and provided data on several psychometric indices. Although the 3-factor model was the most reported structure [15, 31, 34, 35, 37, 41] followed by a 4-factor model [23, 38, 39], the items considerably varied in their expected allocation among studies. Only 3 out of 15 studies presented the same number of items [23, 30, 32].
There were three studies using the 40-item version that differed from the original dimensions proposed for the CAMI. Two studies [15, 34] supported a 3-factor structure, whereas the other supported a 4-factor structure [38]. The studies with more dramatic changes in item allocation were those using the CAMI-24 [41], CAMI-10 [40], and CAMI-26 [15]. The estimation method of maximum likelihood can only be used in CFA when multivariate normality is met, but in the CAMI-24 study [41] this assumption was violated. Moreover, the different approaches to analyse dimensionality (principal component analysis, EFA, and CFA) and the diverse methods used to estimate the factor models might explain the heterogeneous findings in dimensionality.
Regarding the internal consistency of the CAMI, 9 out of 15 studies addressed this psychometric aspect. Unexpectedly, 7 studies reported the α or ω for the total scale, whereas 7 reported α values only for subscales. According to Nunnally and Bernstein criteria [28], those studies that assessed the internal consistency of the total scale (CAMI-BR [39], CAMI-40 [32], and CAMI-20 [35]) obtained adequate alpha values, except for two studies with CAMI-40 [22, 34] and one study with the CAMI-10 [40]. In contrast, the studies that computed Cronbach’s α of each subscale [15, 23, 30, 32, 39, 40, 42], usually obtained values below the recommended cut-off of 0.80. More specifically, the authoritarism subscale was the least reliable subscale [23, 30, 32, 39, 40, 42].
The CAMI-40 was the only version in which temporal stability of its subscales was analysed, showing adequate stability over time. CAMI-BR [39] and CAMI-10 [40] did not present good stability in the subscales but had an acceptable test–retest on the global scale. In general, there is a lack of longitudinal studies, therefore this psychometric aspect has not been exhaustively addressed.
The pattern of correlations between the CAMI and other potentially related constructs was statistically significant and in the expected directions, partially supporting the construct validity. Following Terwee et al. criteria [27], some correlations were not of the expected magnitude. Finally, the interpretability of the CAMI scale assessed by 11 studies highlight that young female participants who have undertaken volunteering activities and have high employment and/or social status, present less stigma towards people with mental disorders.
Strengths and limitations
As far as it is known, this systematic review is the first to summarize the psychometric properties of the different versions of the CAMI since it was published 40 years ago. The CAMI has been administered to a wide variety of populations. Adapted criteria based on the consensus-based standards for the selection of health measurement instruments (COSMIN) were applied to evaluate the quality of the CAMI measurement properties and provided a comprehensive and qualitative synthesis of its current evidence. For transparency purposes, the review protocol was registered in PROSPERO, and an exhaustive search strategy was carried out, as well as a clear data extraction procedure. In contrast, the scope of this results might be considered as limited due to the exclusion of papers not written in English, Spanish, or Italian. The relatively few included studies in this systematic review underly the need of addressing with more emphasis some psychometric properties of this stigma measure, such as the factorial invariance across age, gender, or cultures.
Conclusions
The CAMI psychometric properties have been examined mainly using classic test theory as a framework. This methodological approach does not allow an assessment of the quality of individual CAMI items and factors. Even though some evidence on its psychometric soundness is beginning to emerge from IRT, the evidence is limited at present. The study that explored the CAMI properties by means of IRT methods indicated significant item bias according to health status, gender, and education level. In general, people with mental health experiences, women, and people with lower levels of education scored higher on some of the three CAMI factors. IRT-based methods can provide valuable information for gauging the quality of individual CAMI items and response options across different levels of stigma. This methodology is also very useful for assessing differential item functioning according to sociodemographic variables of interest. In this sense, more evidence based on a IRT approach is needed for the different versions of the CAMI.
The 3- and 4-factor structure are the most widely reported in the different versions of the CAMI. The general lack of fit of the existing data to the four-factor scale originally proposed by Taylor and Dear (1981) [23] could be related to the diversity of CAMI versions explored and to the changes that have been introduced in the adaptations of this inventory during the last years. Additionally, it is frequent to find in the literature that modern psychometric approaches (i.e., based on CFA) fail to replicate the dimensionality of old instruments developed in the seventies or eighties, which were originally analysed with exploratory techniques [44]. Although this inventory has been employed in many samples from different cultures and with different languages, some aspects have been scarcely addressed. For example, time needed for completion, difficulties in understanding the items, or the scale’s acceptability have not been explored. As stated before, measurement invariance has not been assessed in more than 40 years of history. Additionally, as only a few of the included studies had a longitudinal design, it was not possible to draw firm conclusions about the temporal stability of the CAMI. In the limited evidence available, a lack of good test–retest reliability was detected. This low temporal stability could be related to factors such as social desirability or that stigma is not an enduring trait.
In the opinion of the team of researchers of this article, the next step should focus on item refinement to create a uniform set of items, especially considering the influence of culture and context on the expression of stigma. This task would imply collaboration among an international panel of stigma experts. The resulting candidate scale should be evaluated by using cognitive interviews and surveying different samples to reach a final version of the inventory with adequate dimensionality, reliability, and validity that would allow cross-cultural comparisons. In this sense, the development of tools with room for contextual adaptation could be a valuable scientific contribution for the future. Finally, considering the scientific interest that CAMI has generated for more than forty years, it is suggested that future systematic reviews update the available evidence every 10 years.
Availability of data and materials
All data included in this systematic review were extracted from published papers. The data used for the study are made available within the manuscript and supplementary materials.
Abbreviations
- CAMI:
-
Community Attitudes to Mental Illness
- CASC:
-
California Assessment of Stigma Change
- CMI:
-
Custodial Mental Illness Ideology Scale
- CMHI:
-
Community Mental Health Ideology
- COSMIN:
-
Consensus-based standards for the selection of health measurement instruments
- EFA:
-
Exploratory factor analysis
- CFA:
-
Confirmatory factor analysis
- MAKS:
-
Mental Health Knowledge Schedule
- MESH:
-
Medical Subject Headings
- OMI:
-
Opinion about Mental Illness
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-analyses
- PROSPERO:
-
Prospective Register of Systematic Reviews
- RIBS:
-
Reported and Intended Behaviours Scale
- SDO:
-
Social Dominance Orientation
References
Hinshaw SP, Stier A. Stigma as related to mental disorders. Annu Rev Clin Psychol. 2008;4:367–93. https://doi.org/10.1146/annurev.clinpsy.4.022007.141245.
Vistorte AOR, Ribeiro WS, Jaen D, Jorge MR, Evans-Lacko S, Mari JDJ. Stigmatizing attitudes of primary care professionals towards people with mental disorders: a systematic review. Int J Psychiatry Med. 2018;53:317–38. https://doi.org/10.1177/0091217418778620.
Becker AE, Kleinman A. Mental health and the global agenda. N Engl J Med. 2013;369:66–73. https://doi.org/10.1056/NEJMra1110827.
Evans-Lacko S, Brohan E, Mojtabai R, Thornicroft G. Association between public views of mental illness and self-stigma among individuals with mental illness in 14 European countries. Psychol Med. 2012;42:1741–52. https://doi.org/10.1017/S0033291711002558.
Wittchen HU, Jacobi F, Rehm J, Gustavsson A, Svensson M, Jönsson B, et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharmacol J Eur Coll Neuropsychopharmacol. 2011;21:655–79. https://doi.org/10.1016/j.euroneuro.2011.07.018.
Christensen MK, Lim CCW, Saha S, Plana-Ripoll O, Cannon D, Presley F, et al. The cost of mental disorders: a systematic review. Epidemiol Psychiatr Sci. 2020;29:e161. https://doi.org/10.1017/S204579602000075X.
Subramaniam M, Abdin E, Picco L, Pang S, Shafie S, Vaingankar J, et al. Stigma: dimensions and correlates in a multi-ethnic population. Eur Psychiatry. 2016;33:S522–S522. https://doi.org/10.1016/j.eurpsy.2016.01.1933.
Perry BL, Pescosolido BA, Martin JK, McLeod JD, Jensen PS. Comparison of public attributions, attitudes, and stigma in regard to depression among children and adults. Psychiatr Serv. 2007;58:632–5. https://doi.org/10.1176/ps.2007.58.5.632.
Walker JS, Coleman D, Lee J, Squire PN, Friesen BJ. Children’s stigmatization of childhood depression and ADHD: magnitude and demographic variation in a national sample. J Am Acad Child Adolesc Psychiatry. 2008;47:912–20. https://doi.org/10.1097/CHI.0b013e318179961a.
Stuber JP, Rocha A, Christian A, Link BG. Conceptions of mental illness: attitudes of mental health professionals and the general public. Psychiatr Serv. 2014;65:490–7. https://doi.org/10.1176/appi.ps.201300136.
Martin JK, Pescosolido BA, Tuch SA. Of fear and loathing: the role of “disturbing behavior”, labels, and causal attributions in shaping public attitudes toward people with mental illness. J Health Soc Behav. 2000;41:208–23. https://doi.org/10.2307/2676306.
Perkins R, Repper J. Prejudice, discrimination and social exclusion: Reducing the barriers to recovery for people diagnosed with mental health problems in the UK. Neuropsychiatry. 2013;3:377–84.
Walsh DAB, Foster JLH. A call to action. A critical review of mental health related anti-stigma campaigns. Front Public Heal. 2020;8:569539. https://doi.org/10.3389/fpubh.2020.569539.
Evans-Lacko S, Malcolm E, West K, Rose D, London J, Rüsch N, et al. Influence of Time to Change’s social marketing interventions on stigma in England 2009–2011. Br J Psychiatry Suppl. 2013;55:s77-88. https://doi.org/10.1192/bjp.bp.113.126672.
Rubio-Valera M, Fernández A, Evans-Lacko S, Luciano JV, Thornicroft G, Aznar-Lou I, et al. Impact of the mass media OBERTAMENT campaign on the levels of stigma among the population of Catalonia. Spain Eur Psychiatry. 2016;31:44–51. https://doi.org/10.1016/j.eurpsy.2015.10.005.
Grausgruber A, Schöny W, Grausgruber-Berner R, Koren G, Apor BF, Wancata J, et al. “Schizophrenie hat viele Gesichter” – Evaluierung der österreichischen Anti-Stigma-Kampagne 2000–2002. Psychiatr Prax. 2009;36:327–33. https://doi.org/10.1055/s-0029-1220386.
Vaughan G, Hansen C. “Like Minds, Like Mine”: A New Zealand project to counter the stigma and discrimination associated with mental illness. Australas psychiatry Bull R Aust New Zeal Coll Psychiatr. 2004;12:113–7. https://doi.org/10.1080/j.1039-8562.2004.02083.x.
Bratbo J, Vedelsby AK. ONE OF US: The National Campaign for Anti-Stigma in Denmark. In: Gaebel W, Rössler W, Sartorius N, editors. The Stigma of Mental Illness - End of the Story? Cham: Springer International Publishing; 2017. 317–38. https://doi.org/10.1007/978-3-319-27839-1_17.
Stuart H, Chen S-P, Christie R, Dobson K, Kirsh B, Knaak S, et al. Opening minds in Canada: background and rationale. Can J Psychiatry. 2014;59(10 Suppl 1):S8-12. https://doi.org/10.1177/070674371405901s04.
Cohen J, Struening EL. Opinions about mental illness in the personnel of two large mental hospitals. J Abnorm Soc Psychol. 1962;64:349–60.
Rogers AH, Cohen M, Naranick CS. A validation study of the custodial mental illness ideology scale. J Clin Psychol. 1958;14:269–70. https://doi.org/10.1002/1097-4679(195807)14:3%3c269::aid-jclp2270140313%3e3.0.co;2-1.
Baker F, Schulberg HC. The development of a community mental health ideology scale. Community Ment Health J. 1967;3:216–25. https://doi.org/10.1007/BF01434874.
Taylor SM, Dear MJ. Scaling community attitudes toward the mentally ill. Schizophr Bull. 1981;7:225–40. https://doi.org/10.1093/schbul/7.2.225.
Evans-Lacko S, Little K, Meltzer H, Rose D, Rhydderch D, Henderson C, et al. Development and psychometric properties of the Mental Health Knowledge Schedule. Can J Psychiatry. 2010;55:440–8. https://doi.org/10.1177/070674371005500707.
Corrigan PW, Gause M, Michaels PJ, Buchholz BA, Larson JE. The California Assessment of Stigma Change: A Short Battery to Measure Improvements in the Public Stigma of Mental Illness. Community Ment Health J. 2015;51:635–40. https://doi.org/10.1007/s10597-014-9797-5.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. https://doi.org/10.1016/j.ijsu.2021.105906.
Terwee CB, Bot SDM, de Boer MR, van der Windt DAWM, Knol DL, Dekker J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60:34–42. https://doi.org/10.1016/j.jclinepi.2006.03.012.
Nunnally JC, Bernstein IH. The Assessment of Reliability. Psychom Theory. 1994;3:248–92.
Barker C, Pistrang N, Elliott R. Research methods in clinical psychology. London: Wiley; 2002.
Kafami Z, Farhoudi F, Alimoradi M, Sangsefidi Z, Delshad N, Khadem-Rezaiyan M. Persian translation and validation of community attitudes toward the mentally ill scale: a tool for assessing social stigma about mental illness. Int Clin Psychopharmacol. 2023;38(1):40–4. https://doi.org/10.1097/YIC.0000000000000419.
Brockington IF, Hall P, Levings J, Murphy C. The community’s tolerance of the mentally ill. Br J Psychiatry. 1993;162:93–9. https://doi.org/10.1192/bjp.162.1.93.
Ochoa S, Martínez-Zambrano F, Vila-Badia R, Arenas O, Casas-Anguera E, García-Morales E, et al. Spanish validation of the social stigma scale: community attitudes towards mental illness. Rev Psiquiatr y Salud Ment. 2016;9:150–7. https://doi.org/10.1016/j.rpsmen.2015.02.002.
Morris R, Scott PA, Cocoman A, Chambers M, Guise V, Välimäki M, et al. Is the Community Attitudes towards the Mentally Ill scale valid for use in the investigation of European nurses’ attitudes towards the mentally ill? A confirmatory factor analytic approach. J Adv Nurs. 2012;68:460–70. https://doi.org/10.1111/j.1365-2648.2011.05739.x.
Bitta MA, Baariu J, Fondo E, Kariuki SM, Lennox B, Newton CR. Validating measures of stigma against those with mental illness among a community sample in Kilifi Kenya. Global Ment Health. 2022;9:241–8. https://doi.org/10.1017/gmh.2022.26.
Högberg T, Magnusson A, Ewertzon M, Lützén K. Attitudes towards mental illness in Sweden: adaptation and development of the Community Attitudes towards Mental Illness questionnaire. Int J Ment Health Nurs. 2008;17:302–10. https://doi.org/10.1111/j.1447-0349.2008.00552.x.
Tong Y, Wang Z, Sun Y, Li S. Psychometric properties of the Chinese version of short-form community attitudes toward mentally illness scale in medical students and primary healthcare workers. Front Psychiatry. 2020;11:337. https://doi.org/10.3389/fpsyt.2020.00337.
Wolff G, Pathare S, Craig T, Leff J. Community attitudes to mental illness. Br J Psychiatry. 1996;168:183–90. https://doi.org/10.1192/bjp.168.2.183.
Garcia C, Golay P, Favrod J, Bonsack C. French translation and validation of three scales evaluating stigma in mental health. Front psychiatry. 2017;8:290. https://doi.org/10.3389/fpsyt.2017.00290.
Abelha L, Gonçalves Siqueira SR, Legay L, Yang LH, Valencia E, Rodrigues Sarução K, et al. Analysis of psychometric properties of the brazilian portuguese version of the community attitudes towards the mentally ill (CAMI-BR). Rev Fac Cien Med Univ Nac Cordoba. 2015;72:211–9.
GrandónFernández P, SaldiviaBórquez S, Cova Solar F, Bustos C, Turra Chávez V. Análisis psicométrico y adaptación de la escala de actitudes comunitarias hacia la enfermedad mental (CAMI) en una muestra chilena. Univ Psychol. 2016;15:153–62. https://doi.org/10.11144/Javeriana.upsy15-2.apae.
Buizza C, Pioli R, Ponteri M, Vittorielli M, Corradi A, Minicuci N, et al. Community attitudes towards mental illness and socio-demographic characteristics: an Italian study. Epidemiol Psichiatr Soc. 2005;14:154–62. https://doi.org/10.1017/s1121189x00006400.
Song L-Y, Chang L-Y, Shih C-Y, Lin C-Y, Yang M-J. Community attitudes towards the mentally ill: the results of a national survey of the Taiwanese population. Int J Soc Psychiatry. 2005;51:162–76. https://doi.org/10.1177/0020764005056765.
Worthington RL, Whittaker TA. Scale development research: a content analysis and recommendations for best practices. Couns Psychol. 2006;34:806–38. https://doi.org/10.1177/0011000006288127.
Coyne JC, van Sonderen E. The Hospital Anxiety and Depression Scale (HADS) is dead, but like Elvis, there will still be citings. J Psychosom Res. 2012;73(1):77–8. https://doi.org/10.1016/j.jpsychores.2012.04.002.
Acknowledgements
The authors are grateful to the CIBER of Epidemiology and Public Health (CIBERESP CB22/02/00052 & CB16/02/00322; ISCIII) for its support.
Funding
JPS-M has a PFIS predoctoral contract from the Institute of Health Carlos III (ISCIII; FI20/00034). AC-C has a FI predoctoral contract from AGAUR (FI_B/00216). GT is supported by the National Institute for Health Research (NIHR) Applied Research Collaboration South London at King’s College London NHS Foundation Trust, and by the NIHR Asset Global Health Unit award. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. GT is also supported by the Guy’s and St Thomas’ Charity for the On Trac project (EFT151101), and by the UK Medical Research Council (UKRI) in relation to the Emilia (MR/S001255/1) and Indigo Partnership (MR/R023697/1) awards. SEL is supported by funding from the Medical Research Council UK, the Economic and Social Research Council and the NIHR. This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
ED, JVL, SE-L, GT, and MR-V designed the study. JPS-M, AB, and AC-C drafted the manuscript. AB and NA–O contributed to the eligibility, systematic data extraction, and quality assessment. JPS-M, ED, AB, NA–O, AC-C, SE-L, GT, JVL, and MR-V critically revised the manuscript. All authors revised and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
N/A.
Consent for publication
N/A.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table S1.
Detailed search strategy in PubMed (it was adapted to each database).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sanabria-Mazo, J.P., Doval, E., Bernadàs, A. et al. Over 40 years (1981–2023) assessing stigma with the Community Attitudes to Mental Illness (CAMI) scale: a systematic review of its psychometric properties. Syst Rev 12, 66 (2023). https://doi.org/10.1186/s13643-023-02230-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-023-02230-4