
Abstract
Background
Reduced physical activity (PA) is one of the significant health concerns in adults and children alike. Despite the proven benefits of PA, most children, globally, do not meet the weekly criteria of enough PA to maintain health. The proposed systematic review is the review of the factors and will provide information on the factors associated with PA participation in children.
Methods
The proposed systematic review will be conducted based on the methodology from the Cochrane Handbook for Systematic Reviews of Interventions. We will include observational studies (cross-sectional, case–control, and cohort studies), randomized controlled trials (RCTs), and non-randomized study designs for information on factors associated with PA participation among children. Studies with participants in the age range of 5–18 years, indulging in physical activity of 60 min per day for a minimum of 3 days a week, will be included. Studies including differently abled children, children under medical treatment, and those taking medications for illnesses such as neurological, cardiac, and mental health conditions will be excluded from the review. We will search MEDLINE (via PubMed and Web of Science), Scopus, EMBASE, CINAHL, Cochrane CENTRAL, and PEDro for English language publications published from the inception till October 2022. For additional studies, we will search websites such as the Australian Association for Adolescent Health International Association for Adolescent Health and a reference list of the included publications. Selection of studies, data extraction, and quality assessment of the included studies will be performed in duplicate. Quality assessment of the included studies will be performed using the Cochrane Risk of Bias tool (ROB-II) for RCTs, New-Castle Ottawa, for observational studies, and ROBINS-I (Risk of Bias for Non-Randomized studies of Interventions) for non-randomized study designs.
Discussion
The proposed systematic review and meta-analysis will present a summary of the available evidence on factors associated with PA participation in children. The findings of this review will provide new insights into how exercise providers can improve PA participation among children and can also help healthcare workers, clinicians, researchers, and policymakers to plan long-term interventions targeting child health.
Systematic review registration
PROSPERO CRD42021270057.
Similar content being viewed by others

Background
Regular physical activity (PA) is essential for healthy adulthood and reducing the risk of chronic diseases such as hypertension, and metabolic and cardiovascular disorders [1, 2]. Regular PA in childhood helps to maintain normal body weight, improve muscular and cardiorespiratory health, and enhance brain development [3,4,5,6,7,8,9]. Thus, regular PA in childhood lowers the risk of chronic diseases in adulthood [2]. The American College of Sports Medicine (ACSM) recommends a minimum of 60 min of PA per day for a minimum of 3 days a week in children [10]. The recommendations suggest combinations of moderate and vigorous intensity activity such as walking, running, dancing, and cycling [10]. However, industrialization, modernization, and digitalization have contributed to a steep decrease in PA among children [11]. A systematic review conducted in 2018 by Sharara et al. reported that physical activity among Arab children and adolescents was significantly less than the prescribed ACSM guidelines [12]. Several recent reviews also reported the trends of decreased PA among children and adolescents worldwide [13, 14]. The World Health Organisation (WHO) published a global report on PA, and it concluded that 81% of adolescents aged 11–15 years do not meet the WHO recommendations of being physically active for health [15]. This physical inactivity has burdened public health indirectly as a physically inactive child is most likely to be an inactive adult [16]. A 2016 report by Martinez et al. showed that physical inactivity linked to increased morbidity and mortality costs the public health sector $53.8 billion worldwide [16].
The Institute of Medicine (IOM) proposed the use of the social-ecological model (SEM) for childhood obesity interventions [17]. This model categorizes factors influencing PA as an individual (e.g., age, gender, physical development), social (e.g., family, peers, education), environmental (e.g., green spaces, playgrounds, bicycle lanes), and policy-related (e.g., education, transport) [17]. Researchers hypothesize that such factors cumulatively affect the PA of an individual and should be included in interventions to bring about behavioral change and increase PA [17]. The influence of these factors on children’s PA has been individually investigated but not summarized systematically [18,19,20].
Reduced PA levels among children are a global health issue. Examining the magnitude of the influence of factors affecting PA participation among children will be valuable in setting priorities and designing interventions to increase PA in children and prevent chronic diseases in adulthood. Previous reviews have reported that children globally do not meet recommended levels of PA, but the specific contributing factors have not been identified. Our review will address the gap in the evidence by systematically reviewing published literature to establish the specific factors that influence PA participation in children. Summarizing the factors associated with PA participation in children can inform policymakers, researchers, and healthcare practitioners to formulate appropriate PA strategies and facilitation of PA adherence.
Objectives
Primary objective
To identify the factors (enablers and barriers) associated with PA participation among children.
Secondary objective
To provide recommendations for increasing the PA participation among children (based on the findings of the primary objective)
Methods
This systematic review protocol is based on the Preferred Reporting Items for Systematic Review and Meta-analysis Protocols (PRISMA-P) guideline [21], and the systematic review and meta-analysis will be conducted according to the Cochrane Handbook for Systematic Review of Interventions [22]. The protocol for the systematic review is registered in the International Prospective Register of Systematic Review (PROSPERO) with registration number CRD42021270057. Any amendments in the protocol will be documented in the final review.
Eligibility criteria for study selection
Types of participants
The review will include studies assessing the influence of factors on children’s participation in PA, regardless of gender, ethnicity, and socio-economic status. The age groups for inclusion will be 5–18 years. Studies on differently abled children, children under medical treatment and those taking medications for illnesses such as neurological, cardiac and mental health conditions will be excluded from the review as the factors influencing differently abled and children under medical treatment will vary.
Exposure
The exposures in the review will be factors (both facilitators and barriers) influencing PA participation in children. The factors can be categorized as (a) individual factors known to influence one’s propensity for being physically active regularly [17]; (b) social environmental factors: the way one interacts socially and with the environment [17]; (c) policy factors: which include the regulatory laws, formal or informal, implied by government or organizations to support PA participation [17].
Dependent variable
The dependent variable is the participation of children in PA where PA is defined as any bodily movement increasing resting energy expenditure [10]. Studies with repeated bouts of physical activity or exercise to improve physical fitness, including multiple sessions over weeks, months, or years, will be eligible for inclusion. To be eligible for inclusion, PA should be a minimum of 60 min per day for a minimum of 3 days a week, primarily a combination of moderate-intensity to vigorous-intensity activities, causing a noticeable to a substantial increase in heart rate and breathing, respectively [10]. The PA should combine aerobic activities such as brisk walking, running, swimming, dancing, and strength training (e.g., tug of war, climbing a tree, or working with Thera bands) [10]. Studies reporting the transient effect of a single bout of exercise or PA will be excluded. Studies with PA interventions in school settings and extracurricular settings such as home, community, or other settings will be included.
Types of studies
Observational studies such as analytical cross-sectional studies, case–control studies, and longitudinal studies (e.g., cohort studies) will be included for information on factors associated with PA participation among children. We will also include experimental study designs such as randomized controlled trials (RCTs). In cases where RCTs are not possible due to the nature of the intervention or due to ethical concerns, we will include the non-randomized trials or the experimental studies not following randomization for the allocation of participants. Additionally, we will also include other non-randomized study designs such as controlled before and after studies (CBAs) and quasi-experimental studies.
Conceptual framework
We hypothesize several factors’ direct and indirect effects on PA participation in children through the conceptual framework (Fig. 1). Several factors (involving individual, social, and policy-related factors) directly or indirectly influence PA participation among children [23]. The individual factors are psychological, behavioral, and demographic factors and will include age, sex, likes or dislikes, education, socioeconomic status, self-efficacy, skill levels, and attitude towards PA [24]. As their age increases, children are less likely to be physically active [24]. Gender plays an essential role in participation because females tend to play less vigorous games than their male counterparts [25]. Educated children or parents tend to understand the importance of PA participation better than less educated or uneducated parents [26].

Conceptual Framework of direct and indirect factors effecting PA participation in children
The social factors also play an essential role in PA participation [27]. The social factors can be interpersonal (peers, parents, teachers), organizational (schools, day-care, home, neighborhood), and community (worship place, geographical locality) [27]. A child is likely to be more active if the parents are physically active as compared to sedentary parents; also, a friend’s PA participation reinforces PA in individuals; therefore, peer validation of PA plays a key role, and children tend to be socially more interactive with physically active peers as compared to inactive or less active peers [28]. A habit of PA participation should be encouraged in children in schools, homes, and healthy neighborhoods [29]. Children who are part of dense, homogenous communities are more likely to be influenced by the norms and culture of that community [29].
Policy factors are another influence on PA participation behavior and are a crucial feature of public health [30]. Policies can range from the restrictive, such as banning exposure to sugar-based product advertisements to increasing health promotion resources such as parks and community exercise facilities [30]. These policies may increase PA participation among children [30]. We anticipate that modifying these factors will increase the PA participation in children and decrease obesity and sedentary lifestyle-related health risk factors.
Searching for studies
We will search Medical Literature Analysis and Retrieval System Online (MEDLINE) via PubMed and Web of Science, Scopus, Excerpta Medica Database (EMBASE), Cumulated Index to Nursing and Allied Health Literature (CINAHL), The Cochrane Library (Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials (CENTRAL), and Physiotherapy Evidence Database (PEDro) for English language publications, published from the inception of the database till November 2021. In addition, we will search the following websites: Australian Association for Adolescent Health (https://www.aaah.org.au/), International Association for Adolescent Health (https://iaah.org/, https://www.who.int/data/maternal-newborn-child-adolescent-ageing/documents/mca), Association of Adolescent and Childcare in India (https://www.aacci.in/), Society for Adolescent Health and Medicine (https://www.adolescenthealth.org/Home.aspx), The Childhood Obesity Foundation (https://childhoodobesityfoundation.ca/about/), and Centres for Disease Control and Prevention, (https://www.cdc.gov/obesity/data/childhood.html), for additional resources. We will search the reference list of the included publications for additional studies. Search keywords will be “Physical activity, exercise, sports, physical education, children, adolescents, kids, youth, factors and determinants.” We will use a combination of controlled vocabulary terms such as Medical Subject Headings (MeSH) and free text words for designing the search strategy. The initial search will be conducted in PubMed, and the search terms will then be modified according to the requirements for different databases. The preliminary search strategy for PubMed is given in Additional file 1.
Selection of studies
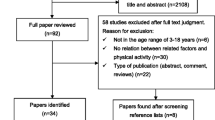
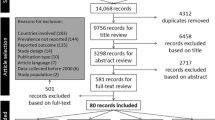
Two reviewers (PS and ER) will independently screen the titles and abstracts of potential studies for eligibility based on the eligibility criteria of the review. Any disagreement at this stage will be resolved via discussion or in consultation with the third reviewer (SB). Full texts of all the included studies will be downloaded, and in case of non-available full texts study, authors or subject experts will be contacted for full texts: in case the full text remains unavailable, we will exclude that study. In case of two reports of the same study, the latest and the one with the complete information will be included for full-text and the other report will be marked as a duplicate. In the next step, a full-text screening will be performed by two review authors (PS and ER) independently. Any disagreement during this stage will be resolved by consensus or via contacting the third author (SB). More information about the process of selection of studies is given in Table 1.
Data management and extraction
Data will be managed using the EndNote reference manager and Microsoft Excel Office software. Data will be extracted by two review authors (PS and ER) independently by using the pre-tested data extraction sheet. All the reviewers will perform pilot testing of the data extraction sheet. Information related to bibliographic details, participants, PA, and outcome details will be extracted. An example of the data extraction form is given in Table 2. We plan to contact the study authors in case of any missing or unclear information. Any disagreements between the review authors will be resolved by discussion and input from a third reviewer (SB).
Critical appraisal of the included studies risk of bias in individual studies
The reviewers will use the Cochrane Risk of Bias (ROB2) for assessing the quality of included RCTs [31]. Each selected publication will be checked for i) bias from the randomization process, (ii) bias due to deviations from intended interventions, (iii) bias due to missing outcome data, (iv) bias in the measurement of the outcome, and (v) bias in the selection of reported result. Each domain will be judged as “low risk,” “high risk,” or “risk with some concerns” with appropriate reasoning. The JBI Checklist for Analytical Cross-Sectional Studies’ is for assessing the quality of the analytical cross-sectional studies [32, 33]. The Newcastle Ottawa scale for assessing the quality of the observational studies such as case–control and cohort studies [34]. Quality assessment of non-randomized studies will be performed using the Risk Of Bias in Non-Randomized Studies-of Interventions (ROBINS-I) [35]. According to this tool, bias in a non-randomized trial will be assessed for the following seven domains: (a) bias due to confounding, (b) bias in the selection of participants into the study, (c) bias in the classification of interventions, (d) bias due to deviations from intended interventions, (e) bias due to missing data, (f) bias in the measurement of outcomes, and (g) bias in the selection of the reported result. The assessed risk will be categorized as low risk, moderate risk, serious risk, and critical risk. The risk of bias will be performed by two reviewers (PS and ER) independently, and any disagreement will be resolved by consensus or by consultation with the third reviewer (SB).
Measure of effects
If continuous, data will be reported as mean and standard deviation with a 95% confidence interval (CI). For categorical data, estimates of odds ratio (OR) and risk ratio (RR) with 95% CI will be used for reporting.
Odds ratio will be extracted and reported for observational studies where the estimation of risk is difficult, such as analytical cross-sectional studies and case–control studies. Risk ratio (95%CI) will be extracted and reported for longitudinal studies (e.g., cohort studies) and experimental studies (RCTs and NRCTs). The final results will be reported as RR (95% CI), as relative risk or risk ratio is considered as a more intuitive measure of effect and is easy to interpret [22].
Data synthesis
For primary objective
Findings of the review will be presented via “the characteristics of included studies” and “summary of findings” table (as shown in Table 1). Meta-analysis will be performed only if it is appropriate, i.e., for studies that are clinically and methodologically similar. Odds ratio and risk ratio will be computed as effect measures and will be pooled in a meta-analysis RR (95% CI) will be used to finally report the findings. In case all the studies provide only OR as an effect measure statistic, in this case, meta-analysis will be computed using OR and the final results will be re-expressed as RR [22]. Statistical heterogeneity will be determined using the chi-square (Q) statistic, where a P value < 0.1 will be considered as statistically significant. Statistical heterogeneity will be quantified using I-squared statistics, describing the percentage of the variability in effect estimates that is due to heterogeneity rather than chance [22]. Based on the I 2 statistic, the level of heterogeneity will be categorized as follows [22]:
-
1.
0 to 40%: might not be important
-
2.
30 to 60%: may represent moderate heterogeneity
-
3.
50 to 90%: may represent substantial heterogeneity
-
4.
75 to 100%: considerable heterogeneity
Random effects model with and inverse-variance approach, i.e., DerSimonian and Laird method will be used for meta-analysis [22]. This method given by DerSimonian and Lair in 1986 makes use of a “moment-based” estimate of the between-study variance [22]. The random effects model is chosen because of the assumed distribution of effects between the studies and as it is assumed that the results are not fixed [22]. The results of the meta-analysis will be reported via a forest plot.
A narrative synthesis will be performed in case of high heterogeneity and when meta-analysis is not possible, i.e., due to the presence of “clinical,” “methodological,” and “statistical.” In the narrative synthesis, the outcome and findings will be reported narratively, and tables/figures will be used for explanation.
If it is possible, sub-group analyses will be performed based on geographical location, age, gender, type of physical activity, etc. If sufficient data is available, we will perform sensitivity analysis for assessing the robustness of the results.
For secondary objective
The primary objective findings, i.e., the factors associated with PA participation among children will be used to frame the policy and practice recommendations. The different factors for PA participation will be listed, based on our contextual framework. Additionally, a list of recommendations present in the available scientific literature will be prepared. These findings will be further discussed with all the relevant stakeholders to frame the appropriate recommendations.
Meta-biases
Funnel plots will be used for the identification of reporting or publication bias. The identification of reporting bias will be done based on a visual assessment of the funnel plot, where a symmetrical funnel plot will be interpreted as the absence of reporting bias and an asymmetrical plot will indicate the presence of reporting bias.
Discussion
Physical inactivity is one of the leading risk factors for lifestyle diseases and increased morbidity worldwide. PA is a modifiable factor and increasing PA levels among children can help reduce health risk factors, promote healthy lifestyles, and improve their quality of life.
In this review, we expect to identify the factors associated with PA participation among children. We hope that systematically reviewing such factors will help address the paucity of evidence surrounding factors contributing to poor engagement with physical activity, which can lead to obesity and other medical conditions. Identifying the factors influencing PA participation in children and adolescents can provide guidance, health promotion, and resources for the families, policymakers, and authorities to improve the lifestyle and health of young people. Any major changes in the protocol will be amended in PROSPERO. An abstract of the complete synthesis will be presented in relevant conferences. The manuscript will be submitted to a relevant journal for publication. This systematic review will support the caregivers, policymakers, and healthcare providers by summarising the evidence for different behavioral interventions intended to increase the physical activity participation among children. This behavioral change is particularly relevant globally given WHO’s focus on preventing diseases in children.
Availability of data and materials
Data sharing is not applicable to this protocol as datasets are not generated or analysed.
Abbreviations
- ACSM:
-
American College of Sports Medicine
- CBA:
-
Controlled before-after studies
- CI:
-
Confidence interval
- GDT:
-
Guideline Development Tool
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluations
- IOM:
-
Institute of Medicine
- MeSH:
-
Medical Subject Headings
- OR:
-
Odds ratio
- PA:
-
Physical activity
- PRISMA-P:
-
Preferred Reporting Items for Systematic Review and Metanalysis Protocols
- RCT:
-
Randomized controlled trials
- RoB2:
-
Cochrane Risk-of-Bias tool
- ROBINS-I:
-
Risk Of Bias tool to assess Non-Randomized studies of Interventions
- RR:
-
Risk ratio
- SEM:
-
Social-ecological model
- WHO:
-
World Health Organization
References
Fühner T, Kliegl R, Arntz F, Kriemler S, Granacher U. An update on secular trends in physical fitness of children and adolescents from 1972 to 2015: a systematic review. Sports Med. 2021;51(2):303–20.
Logan K, Lloyd RS, Schafer-Kalkhoff T, Khoury JC, Ehrlich S, Dolan LM, Shah AS, Myer GD. Youth sports participation and health status in early adulthood: a 12-year follow-up. Prev Med Rep. 2020;19:101107.
Dale LP, Vanderloo L, Moore S, Faulkner G. Physical activity and depression, anxiety, and self-esteem in children and youth: an umbrella systematic review. Ment Health Phys Act. 2019;16:66–79.
Rhodes RE, Janssen I, Bredin SS, Warburton DE, Bauman A. Physical activity: health impact, prevalence, correlates and interventions. Psychol Health. 2017;32(8):942–75.
Aadland E, Kvalheim OM, Anderssen SA, Resaland GK, Andersen LB. The multivariate physical activity signature associated with metabolic health in children. Int J Behav Nutr Phys Act. 2018;15(1):1–1.
Smith JJ, Eather N, Morgan PJ, Plotnikoff RC, Faigenbaum AD, Lubans DR. The health benefits of muscular fitness for children and adolescents: a systematic review and meta-analysis. Sports Med. 2014;44(9):1209–23.
Foster HE, Scott C, Tiderius CJ, Dobbs MB, Ang E, Charuvanij S, et al. Improving musculoskeletal health for children and young people–a ‘call to action’. Best Pract Res Clin Rheumatol. 2020;35(4):101566.
Di Liegro CM, Schiera G, Proia P, Di Liegro I. Physical activity and brain health. Genes (Basel). 2019;10(9):720.
Macpherson H, Teo WP, Schneider LA, Smith AE. A life-long approach to physical activity for brain health. Frontiers in aging neuroscience. 2017;9:147.
Roitman J, Kelsey M. ACSM’s resource manual for guidelines for exercise testing and prescription. 9th ed. Baltimore: Williams & Wilkins; 2020.
O’Brien W, Issartel J, Belton S. Relationship between physical activity, screen time and weight status among young adolescents. Sports. 2018;6(3):57.
Sharara E, Akik C, Ghattas H, et al. Physical inactivity, gender and culture in Arab countries: a systematic assessment of the literature. BMC Public Health. 2018;18:639.
Aubert S, Brazo-Sayavera J, González SA, Janssen I, Manyanga T, Oyeyemi AL, Picard P, Sherar LB, Turner E, Tremblay MS. Global prevalence of physical activity for children and adolescents; inconsistencies, research gaps, and recommendations: a narrative review. Int J Behav Nutr Phys Act. 2021;18(1):1–1.
Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. 2020;4(1):23–35.
Chaput JP, LeBlanc AG. Pokémon GO: snake oil or miracle cure for physical inactivity? Ann Transl Med. 2017;5(1):S3. Apps.who.int. 2021 [cited 26 August 2021]. Available from: https://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf.
Martinez-Andrés M, Bartolomé-Gutiérrez R, Rodríguez-Martín B, Pardo-Guijarro MJ, Garrido-Miguel M, Martínez-Vizcaíno V. Barriers and facilitators to leisure physical activity in children: a qualitative approach using the socio-ecological model. Int J Environ Res Public Health. 2020;17(9):3033.
Hu D, Zhou S, Crowley-McHattan ZJ, Liu Z. Factors that influence participation in physical activity in school-aged children and adolescents: a systematic review from the social ecological model perspective. Int J Environ Res Public Health. 2021;18(6):3147.
Chiarlitti NA, Kolen AM. Parental influences and the relationship to their children’s physical activity levels. Int J Exerc Sci. 2017;10(2):205–12.
Haddad J, Ullah S, Bell L, Leslie E, Magarey A. The influence of home and school environments on children’s diet and physical activity, and body mass index: a structural equation modelling approach. Matern Child Health J. 2018;22(3):364–75.
Tonge K, Jones RA, Okely AD. Environmental influences on children’s physical activity in early childhood education and care. J Phys Act Health. 2020;17(4):423–8.
Moher D, Liberati A, Tetzlaff J, Altman DG, Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane Handbook for systematic reviews of interventions version 6.3 (updated August 2022). Cochrane; 2022.
Stevens CJ, Baldwin AS, Bryan AD, Conner M, Rhodes RE, Williams DM. Affective determinants of physical activity: a conceptual framework and narrative review. Front Psychol. 2020;11: 568331.
Martins J, Costa J, Sarmento H, Marques A, Farias C, Onofre M, Valeiro MG. Adolescents’ perspectives on the barriers and facilitators of physical activity: an updated systematic review of qualitative studies. Int J Environ Res Public Health. 2021;18(9):4954.
Lew-Levy S, Boyette AH, Crittenden AN, Hewlett BS, Lamb ME. Gender-typed and gender-segregated play among Tanzanian Hadza and Congolese BaYaka hunter-gatherer children and adolescents. Child Dev. 2020;91(4):1284–301.
Hesketh KR, Lakshman R, van Sluijs EM. Barriers and facilitators to young children’s physical activity and sedentary behaviour: a systematic review and synthesis of qualitative literature. Obes Rev. 2017;18(9):987–1017.
Kwan MP. The limits of the neighborhood effect: contextual uncertainties in geographic, environmental health, and social science research. Environ Geochem Health. 2018;108(6):1482–90.
McGaughey T, Vlaar J, Naylor PJ, Hanning RM, Le Mare L, Mâsse LC. Individual and environmental factors associated with participation in physical activity as adolescents transition to secondary school: a qualitative inquiry. Int J Environ Res Public Health. 2020;17(20):7646.
Laddu D, Paluch AE, LaMonte MJ. The role of the built environment in promoting movement and physical activity across the lifespan: implications for public health. Prog Cardiovasc Dis. 2021;64:33–40.
Althoff T, Hicks JL, King AC, Delp SL, Leskovec J. Large-scale physical activity data reveal worldwide activity inequality. Nature. 2017;547(7663):336–9.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366: l4898.
Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z (Editors). JBI Manual for Evidence Synthesis. JBI. 2020. Available from https://synthesismanual.jbi.global, https://doi.org/10.46658/JBIMES-20-08.
Ma LL, Wang YY, Yang ZH, Huang D, Weng H, Zeng XT. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Mil Med Res. 2020;7:1–1.
Cook DA, Reed DA. Appraising the quality of medical education research methods: the Medical Education Research Study Quality Instrument and the Newcastle-Ottawa Scale-Education. Acad Med. 2015;90(8):1067–76.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, Carpenter JR. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355: i4919.
Acknowledgements
We would like to acknowledge the Manipal Academy of Higher Education for technological and logistic support.
Funding
No financial support from any commercial or non-commercial funders was done to support this systematic review.
Author information
Authors and Affiliations
Contributions
PS and ER conceptualized the topic. PS, ER, and SB drafted the manuscript. PS and ER edited and finalized the final version of the manuscript. All the authors (PS, ER, SB, VK, HVB) read, provided intellectual feedback, and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA-P 2015 Checklist.
Additional file 2.
Factors determining PA participation.
Additional file 3.
Draft PubMed Search Strategy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Srivastav, P., Vaishali, K., Rajwar, E. et al. Factors associated with physical activity participation among children: a systematic review protocol. Syst Rev 12, 70 (2023). https://doi.org/10.1186/s13643-023-02226-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-023-02226-0