
Abstract
Background
Ketones are synthesised as an alternative fuel source during times of energy restriction. In the absence of a hyperglycemic emergency, ketosis in patients presenting to the emergency department (ED) may indicate reduced carbohydrate intake. In the perioperative setting, excess fasting with ketosis is associated with worse outcomes; however, whether ketosis in patients without diabetes presenting to ED is also associated with worse outcomes is unclear. This systematic review aims to examine the evidence for ketosis in predicting the need for hospital admission in patients without diabetes, presenting to the ED.
Methods
A systematic review was performed using PRISMA guidelines. We searched electronic bases (OVID-Medline, OVID-EMBASE, Scopus and PubMed) up to December 2022. Eligible studies included children or adults without diabetes presenting to the ED where a point-of-care capillary beta-hydroxybutyrate (BHB) was measured and compared to outcomes including the need for admission. Outcome measures included need for admission and length of stay. Content analysis was performed systematically; bias and certainty assessed using standard tools.
Results
The literature search found 17,133 citations, 14,965 papers were subjected to title and abstract screening. The full text of 62 eligible studies were reviewed. Seven articles met the inclusion criteria. Six studies were conducted solely in the paediatric population, and of these, four were limited to children presenting with gastroenteritis symptoms. Median BHB was higher in children requiring hospital admission with an AUC of 0.64–0.65 across two studies. There was a weak correlation between BHB and dehydration score or duration of symptoms. The single study in adults, limited to stroke presentations, observed no relationship between BHB and neurological deficit at presentation. All studies were at risk of bias using the Newcastle-Ottawa Scale and was assessed of “very low” to “low” quality due to their study design in the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. Heterogeneity amongst selected studies precluded meta-analysis.
Conclusion
The evidence for any utility of BHB measurement in the ED in absence of diabetes is limited to the paediatric population, specifically children presenting with symptoms of gastroenteritis. Any role in adults remains unexplored.
Similar content being viewed by others

Introduction
The ketone bodies β-hydroxybutyrate (BHB), acetoacetate, and acetone are an alternative fuel source primarily utilised by the human body in states of energy restriction with reduced carbohydrate intake, usually characterised by low or normal glucose and appropriately low insulin [1]. BHB is the most abundant ketone body [1]. Normally, circulating BHB levels are < 0.5 mmol/L, but can reach up to 6–7.5 mmol/L during prolonged fasting [2]. Hyperketonemia is defined as BHB > 1.0 mmol/L and ketoacidosis as BHB > 3.0 mmol/L [3, 4].
The most common cause of ketoacidosis amongst patients presenting to ED is diabetic ketoacidosis (DKA), occurring typically in type 1 diabetes, where there is a pathological lack of insulin [5]. More recently, euglycemic ketoacidosis as a complication of sodium-glucose transport protein 2 inhibitors (SGLT2i) has been recognized [6]. Other rarer presentations of ketonaemia or ketoacidosis in adults may occur in association with hyperemesis gravidarum, lactation, or alcoholic ketoacidosis [7, 8].
Children are thought to be more vulnerable to ketosis due to lower glycogen stores and higher metabolic rates compared to adults [4, 9]. Excess fasting perioperatively in young children, or intercurrent illnesses with a period of poor oral intake can result in hypoglycemia and ketosis due to accelerated starvation of childhood (ASC) [10, 11]. However, ketosis in fasted adult patients is uncommon [12]. Many paediatric ED presentations are associated with reduced oral and carbohydrate intake, with one study quantifying 1833 cases of starvation ketosis per 100,000 paediatric presentations (1.8%; 95% confidence interval 1.5–2.2%) [11]. Longer surgical fasting times are associated with greater ketosis and worse hemodynamic parameters [10] and so ketosis in patients presenting to ED may be useful as marker of illness severity or guide the need for hospital admission [12]. BHB measurements via point-of-care (POC) testing is readily available, a survey of 89.9% of UK and Ireland paediatric acute care sites finding it in use, thus examining the utility of such a readily available test is important for patient care [13].
The aim of this study is to conduct a systematic review to assess the utility of ketone measurement, using POC devices measuring BHB, in patients without diabetes presenting to the ED as a predictor of illness severity.
Methods
Search strategy and data sources
A systematic review was developed utilising the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) reporting guidelines and was registered at the International Prospective Register of Systematic Reviews (PROSPERO) with the protocol number CRD42022304390. We searched OVID-MEDLINE, OVID-EMBASE, Scopus, and PubMed from inception until March 2021. The reference lists of relevant articles and existing reviews were also manually searched. The search strategy was formulated using search terms relating 2 main themes: ketones, with keywords “ketone*”, “beta-hydroxybutyrate”, “acetylacetone” and “acetone”, and the emergency department with keywords including “emergency” and “hospital” (see complete search strategy in Additional file 1).
Study selection/eligibility criteria
Study types
Randomised controlled trials, prospective non-randomised cohort studies, retrospective cohort studies and retrospective case-controlled studies with an appropriate comparison group were included. Authors of studies were not contacted for additional unpublished data. Studies were excluded if the patient cohort was less than 6 patients. Review articles, conference abstracts, case reports, articles not published in English, or studies not conducted on humans were excluded.
Participants
Eligible studies included patients without diabetes presenting to the emergency department (ED). Studies reporting on both adult and paediatric patients were eligible for inclusion. Studies limited to patients with known diabetes mellitus or who were diagnosed with diabetes mellitus during that presentation were excluded.
Intervention
The intervention was point-of-care (POC) BHB measured in the ED.
Outcomes
Studies whereby BHB levels were assessed in relation to any objective measure of patient outcomes were included. Clinical outcomes of interest included primarily mortality and mortality scores, secondary outcomes were need for admission to hospital from ED, and any reported indicators of illness severity, such as dehydration scores. Studies were excluded if POC BHB level was not linked to any measurable outcome, and so studies limited to prevalence were also excluded.
Study selection
All studies retrieved from the four databases were exported to a referencing software (EndNote) with duplicates removed for title and abstract screening. One reviewer screened titles and abstracts for valid articles (S.H.). Following which, two independent reviewers retrieved and screened the full texts for eligibility, using the specified inclusion and exclusion criteria (S.H. and B.D.). Any uncertainty over the study eligibility was resolved through discussions between the two reviewers. If there were any unresolved differences in opinion by these two reviewers, a third reviewer was consulted (A.C.).
Data collection process
Data extracted included general study characteristics (authors, publication year, country, study design, sample size), patient population (age), details on the intervention (source and collection time of blood sample for ketone measurement), the studies’ primary outcomes, other measured outcomes, and any other key findings.
Risk of bias and certainty of evidence
Assessment of risk of bias was conducted using the Cochrane-Collaboration risk of bias tool for RCTs and the Newcastle-Ottawa scale for non-randomised studies [14, 15]. Assessment of certainty of evidence of included studies was conducted independently by two authors (S.H. and B.D) using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach [16].
Data synthesis
Due to the clinical heterogeneity amongst studies, meta-analysis was precluded. Instead, a narrative summary analysis of predefined outcome measures was performed. Additionally, the median and interquartile ranges of ketones from individual studies were compiled quantitatively for each outcome using GraphPad Prism version 9.5.0 for Mac, GraphPad Software, San Diego, CA, USA, www.graphpad.com.
Results
Study selection
The initial electronic database search identified 17,133 records, of which 14,965 were unique records (Fig. 1). Of the 62 full-text articles retrieved and assessed for eligibility, 55 were excluded. Reasons for exclusion at full-text review or data extraction stages were participants not meeting the inclusion criteria (n = 5), using interventions other than BHB measurements (n = 27), lack of measurable outcomes (n = 17), study design (n = 4), and conference abstract, commentary or protocol for a study already included (n = 2) (Fig. 1).

PRISMA flowchart outlining process for inclusion/ exclusion of studies [17]
Study characteristics
The characteristics of the seven included studies are shown in Table 1. Each was undertaken at a single centre. Six reported on paediatric patients only with ages ranging from 0 to 14 years old. Three of the six paediatric studies were limited to children with symptoms of gastroenteritis only [18,19,20], one was limited to children with benign convulsions with mild gastroenteritis [21], one was limited to children requiring venepuncture as part of their medical work-up [12], and the other paediatric study was limited to children presenting with acute abdominal pain suggestive of paediatric acute appendicitis (PAA) [22]. Only one study was conducted in adults (median age 77 years) and was limited to patients presenting with a diagnosis of first-ever acute stroke [23].
Studies utilised whole blood or capillary blood samples to measure BHB levels and samples were collected at triage, time of venepuncture or after physical examination. Hyperketonaemia was not specifically defined in four of the seven studies [12, 19, 20]. In the two studies [18, 23], hyperketonemia was defined as BHB > 1.0 mmol/L while the one other study [21] defined ketosis and severe ketosis as blood BHB levels of ≥ 0.6 mmol/L and ≥ 4.5 mmol/L respectively.
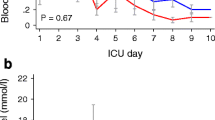
BHB levels
Median or mean BHB varied across studies. As shown in Fig. 2, numerically higher median or mean BHB were found in the series reported by Levy et al. (2013) (median BHB 3.1 mmol/L), Durnin et al. (2020) (median BHB 4.6 mmol/L) and Lee et al. (2019) (mean BHB 3.65 mmol/L); these studies recruited patients with gastroenteritis symptoms [18, 19, 21]. In contrast, Torres et al. (2018) did not report overall median BHB but reported a numerically lower median BHB in patients presenting with similar symptoms, of 1mmol/L in successful oral replacement therapy (ORT) patients and 0.55 mmol/L in patients who failed ORT, with limited statistical significance p = 0.087 [20]. Montero et al.’s (2019) study found median BHB of 0.3 mmol/L in patients with non-surgical abdominal pain, while median BHB in their second group of patients with histologically confirmed diagnosis of acute appendicitis (group 2) was 0.7 mmol/L [22]. Comparatively, Pikija et al. (2013) in adult first-ever stroke presentation and O’Donohoe et al. (2006) in unwell children requiring venepuncture at ED presentation reported lower median BHB levels, both of which were 0.2 mmol/L [12, 23].

Outcomes
We initially planned to access mortality as a primary outcome, followed by mortality scores and length of hospital stay. However, none of the studies measured these outcomes. As such, admission to hospital versus discharge from ED was selected as the primary outcome of this systematic review. Secondary outcomes included the severity of illness assessed via length of symptoms and dehydration scores upon presentation in studies that recruited patients with likely gastroenteritis. The following sections present narrative summarises for each outcome measure. Table 2 summarises outcomes reported in each study.
Admission versus discharge
The BHB values of patients requiring admission as compared to those discharged from ED was reported in 2 studies [12, 18]. All patients were admitted in Montero et al. (2022) and Pikija et al. (2013) with no data on BHB levels of those discharged. Lee et al. (2019) reported admission to ward in 4 patients (26.7%) in the “severe- ketosis” group (BHB ≥ 4.5 mmol/L) compared to 7 patients (25.9%) in the “non-severe ketosis” group (BHB ≥ 0.6 < 4.5 mmol/L) (p = 1.000) [22, 23]. The median BHB was higher in admitted patients with gastroenteritis [18], as compared to non-specific medical presentations requiring blood testing as part of their medical work up (Fig. 3) [12]. Data available on the AUC of ROC of triage BHB as a predictor of admission is similar across the two studies- 0.64 (95% CI 0.56 to 0.72) [12] and 0.65 (95% CI 0.57 to 0.73) [18].

Length of symptoms
Two studies, Durnin et al. (2020) and Levy et al. (2013) compared the duration of symptoms of gastroenteritis with ketone concentrations seen in Fig. 4 whereas Lee et al. (2019) reported duration of gastroenteritis symptoms at ED visit ≥ 4 days in 4 patients (36.7%) in the “severe ketosis” group compared to 8 patients (29.6%) in the “non-severe ketosis” group [18, 19, 21]. Both Durnin et al. (2020) and Levy et al. (2013) studied the same time intervals of < 1 day, 1–2 days and > 3 days [18, 19].

The median ketone levels of patients in the groups of different lengths of symptoms < 1 day, 1–2 days and > 3 days, progressively increase within the studies. In Durnin et al. (2020), the association between elevated triage ketones and duration symptoms was noted to be statistically significant comparing symptoms < 1 day to symptoms ≥ 1 day (Wilcoxon-Mann-Whitney U = 656, p = 0.017) [18]. Levy et al. (2013) reported a statistically significant difference in ketone concentration between patients with symptom duration of < 1 day compared to 1–2 days (p = 0.001), and between patients with symptom duration < 1 day compared to > 3 days, p < 0.001, but not between patients with symptom duration 1–2 days compared to > 3 days (p = 0.736) [19]. However, given that the heterogeneity in the population of patients recruited, whereby with younger median age of 1.8 years in Durnin et al. (2020) compared to Levy et al. (2013) with a median age of 2.3 years, and with Durnin et al. (2020) including patients with symptoms of vomiting and/or diarrhoea and/or decreased fluid intake with 4-point Gorelick Score (4PGS) of 2 or greater or concern at triage of possible hypoglycemia while Levy et al. (2013) recruited children with symptoms of gastroenteritis and were deemed to require IV fluids for dehydration, the two studies cannot be directly compared [18, 19].
Dehydration scores
Two studies that calculated dehydration scores in children with symptoms of gastroenteritis utilised different dehydration scores, making direct comparison difficult—Durnin et al. (2020) used the 4PGS and 10-point Gorelick Score (10PGS) while Levy et al. (2013) used the Clinical Dehydration Score (CDS) [18, 19]. In Durnin et al. (2020), there was no correlation identified between triage ketone levels and 4PGS (Spearman’s ρ = 0.97, p = 0.175), and a weak correlation between triage ketones and 10PGS (Spearman’s ρ = 0.217, p = 0.002) [18]. Levy et al. (2013) identified a positive relationship between serum BHB and the prospectively assigned CDS (Spearman’s ρ = 0.22, p = 0.003) [19].
Other markers of illness severity
Several studies measured distinct outcomes which did not allow comparison to the other studies. Within the six studies conducted in the paediatric population, one study measured a single outcome- the failure of oral rehydration and found that initial BHB level had no statistical predictive value of predicting the failure of oral rehydration (p = 0.087) [20]. Another distinctive outcome was measured in O’Donohoe et al. (2006) qualitative feeding estimated by parents or caregivers, where it was reported that patients with normal feeding in their cohort had significantly lower median ketones compared to those with less than normal feeding (0.206 mmol/L vs 1.324 mmol/L), with the correlation of BHB to decreased oral intake being R2 = 0.25 (p = 0.001) [12]. Additionally, Levy et al. (2013) explored a general appearance score (1 = obtunded to 5 = alert and active) which was significantly correlated with serum BHB concentrations (ρ = − 0.26, p < 0.001) [19]. Lee et al. (2019) also quantified patients in the “severe ketosis” compared to the “non-severe-ketosis” groups who had multiple seizures prior to ED arrival and seizure recurrence in the ED as 3 (20.0%) vs 4 (14.8%) patients (p = 0.686) and 8 (53.3%) vs 10 (37.0%) patients (p = 0.307) respectively [21]. Montero et al. (2022) compared BHB between uncomplicated PAA 0.6 mmol/L (IQR 0.4–0.9) and complicated PAA 1.2 mmol/L (IQR 0.8–1.4) with AUC 0.69 (95% CI 0.54 = 0.85) (p = 0.04), and a cut-off point of 1.1 mmol/L, sensitivity 61.1% and specificity 76.9% [22]. Additionally, Montero et al. (2022) correlated other outcomes with BHB, including number of emetic episodes Pearson’s r = 0.25 (p = 0.03) and days of admission Spearman’s Rho = 0.32 (p = 0.02) [22]. Since Pikija et al. (2013) population was specific to stroke, the National Institutes of Health Stroke Scale (NIHSS) was used as a measure of outcome [23]. No relationship was found between admission BHB and NIHSS scores at presentation or day 5 [23].
Quality appraisal
Risk of bias of individual studies
Variability in the risk of bias was minimal according to the Newcastle-Ottawa scale (n = 7) whereby all studies included were assessed as cohort studies, including Levy et al. (2013) as it was conducted as a secondary post-hoc analysis of an RCT (Additional file 1) [19].
In terms of representativeness, while O’Donohoe et al.’s (2006) study was not limited to a pre-specified diagnosis like the other studies, it was conducted in the paediatric population requiring venepuncture, thus they were determined to have been conducted in a very selected group [12]. Selection of non-exposed cohort (low ketones) were all drawn from the same community as the exposed cohort and ascertainment of such exposure was all recorded from secure records or structured interviews. Only Lee et al. (2019), a retrospective cohort study had its outcomes present at the start of the study [21]. For outcomes, they were mostly assessed through independent blinding or record linkage and follow-up was assessed as adequate and sufficiently long enough for outcome to occur for all studies.
The main source of variability was comparability. All studies mostly accounted for the variances in population. However, only two studies were explicitly blinded, O’Donohoe et al. (2006), which was blinded to relatives and care providers, and Levy et al. (2013), a secondary analysis of a double-blinded RCT [12, 19].
Certainty of evidence
The quality of evidence according to the GRADE system for the included studies (Additional file 1). Most were rated “low” or “very” low, predominantly due to their observational nature.
For admission versus discharge, only O’Donohoe et al. (2006) and Durnin et al. (2020) were assessed as Pikija et al.’s (2013) and Montero et al. (2022)’s population was all admitted, and in Pikija et al.’s (2013), BHB was not a primary outcome measure [12, 18, 22, 23]. Additionally, Lee et al. (2019) presented their data categorically rather than continuously thus proving difficult for comparison [21]. As one study included sample size calculations [18] while the other [12] did not, this outcome was rated “serious” for imprecision and were thus downgraded to “very low”.
For the two secondary outcomes of dehydration scores and length of stay, the same two studies were used—Durnin et al. (2020) and Levy et al. (2013) [18, 19]. Lee et al.’s (2019) study was not included in length of stay due to a difference in length of stay intervals, and the categorical presentation of their data [21]. Since the two studies has similar populations, had direct measures and sample size calculation, inconsistency, indirectness and imprecision were unaffected. However, since the population studies were specific to children with symptoms of gastroenteritis, risk of bias was adversely impacted. Overall, the certainty of evidence was thus rated “low”.
Discussion
This systemic review found few publications examining the utility of BHB measurement in patients without diabetes presenting to the ED. Most studies were conducted in children. Although the Newcastle-Ottawa Scale revealed no large discrepancy in risk of bias of the non-randomised cohort studies, the GRADE approach downgraded these studies based on their design. The ability of BHB to predict need for admission was modest at best, with optimal cut off levels of BHB of 4 and 4.6 mmol/L [12, 18].
In children with gastroenteritis, a higher median BHB may be linked to a longer duration of symptoms, and so ketosis is more likely to occur in those who have been unable to tolerate oral rehydration prior to presentation [18, 19], however one study found BHB at presentation was not a predictor of failure of ORT in the ED [20]. Similarly, the relationship between BHB levels and dehydration scores may reflect an inability to tolerate oral hydration therapy, otherwise the ingested carbohydrate should have been sufficient to increase insulin/glucagon ratio and switch off BHB production. However, recent animal studies have suggested that glucagon is not the sole primary factor in the regulation of ketone production [24]. Work from an animal model has shown that increased glucocorticoids and catecholamines due to dehydration in the presence of insulinopenia is sufficient to induce ketogenesis [25]. It is unclear whether the gradient of BHB levels from patients with nonsurgical abdominal pain, to uncomplicated PAA to complicated PAA may reflect a greater reduction in carbohydrate intake or illness severity [22]. Whether acute illness with associated increased counter-regulatory hormones coupled with dehydration in a vulnerable patient can induce ketosis and the clinical relevance remains unknown.
Limited data on BHB concentrations in the adult population who present to the emergency department was found. Given the increasing likelihood that of the use of SGLT2i in a broader range of adult patients without diabetes, establishing expected degrees of ketosis with acute illness may be useful in the evaluation of such patients. The single study in the adult cohort was limited to patients presenting with first-ever stroke [23]. BHB is said to have neuroprotective and anti-inflammatory effects [26,27,28]. In adults, production of BHB is impaired in individuals with COVID-19-induced acute respiratory distress syndrome (ARDS) but not in those with influenza-induced ARDS [29]. Whether finding lower serum concentrations of BHB in patients with newly diagnosed COVID-19 infection presenting to ED might serve as a predictive risk factor for the development of severe COVID-19 remains to be demonstrated [30]. Currently, there is no evidence to support routine BHB testing in adults presenting to the ED.
Studies assessing BHB in other adult populations without diabetes at risk of ketosis were not found. Women presenting with hyperemesis gravidarum may have positive urinary ketones, however it is currently unclear if blood ketones may be more useful in assessing severity and response to therapy, rather than urinary ketones which are slower to clear [31, 32]. While it has been suggested that alcoholic ketoacidosis is a commonly missed diagnosis [33] in ED, the frequency is unclear. Overt ketoacidosis has been reported with low carbohydrate diets [34]. Such presentations to ED is likely to be rare and evident on history as in a series of patients fasting for surgery, increased BHB (> 1 mmol/L) was only seen in 3% of patients [9].
Limitations
This systematic review is limited by the small number of studies, and a preponderance of observational studies with BHB result being unblinded to the treating team. A high degree of inconsistency/heterogeneity was observed. The reason for heterogeneity is likely due to the paucity of paediatric studies and studies focussing on gastroenteritis. Additionally, some of the studies were conducted using convenience sampling, with potential for selection bias.
When assessing clinical outcome measures, since the majority of studies were conducted in paediatric patients, more appropriate endpoints for such a specific population such as length of symptoms and dehydration scores were reported. However, dehydration scores and length of symptoms are not easily applicable to the rest of the population presenting to the ED without symptoms of gastroenteritis.
Future directions
Due to the paucity of studies in adults, further studies are required to determine any clinical utility of blood BHB. In this review, several paediatric studies were included, but were mostly a specific subgroup of patients presenting with gastrointestinal symptoms, it is thus unclear whether BHB may have utility in guiding therapy, such as ORT or intravenous rehydration, and whether the change of BHB in response to therapy could be useful for monitoring clinical progress.
Conclusion
This systematic review reveals limited evidence in the use of ketones in predicting need for hospital admission. The frequency of ketosis in adults without diabetes presenting with acute illness is unclear. Thus, well-designed studies on both the paediatric and adult population without diabetes are required to determine expected degrees of ketosis with acute illness and its clinical utility.
Availability of data and materials
All data relevant to the study are included in the article or uploaded as online supplemental information.
References
Newman JC, Verdin E. β-Hydroxybutyrate: a signaling metabolite. Ann Rev Nutr. 2017;37:51.
Kanikarla-Marie P, Jain SK. Hyperketonemia and ketosis increase the risk of complications in type 1 diabetes. Free Rad Biol Med. 2016;95:268–77.
Sheikh-Ali M, et al. Can serum β-hydroxybutyrate be used to diagnose diabetic ketoacidosis? Diabetes Care. 2008;31:643–7.
George F, Cahill J. Fuel metabolism in starvation. Ann Rev Nutr. 2006;26:1–22.
Ehrmann D, et al. Risk factors and prevention strategies for diabetic ketoacidosis in people with established type 1 diabetes. Lancet Diabetes Endocrinol. 2020;8:436–46.
Qiu H, Novikov A, Vallon V. Ketosis and diabetic ketoacidosis in response to SGLT2 inhibitors: basic mechanisms and therapeutic perspectives. Diabetes Metab Res Rev. 2017;33:e2886.
Bashir B, Fahmy AA, Raza F, Banerjee M. Non-diabetic ketoacidosis: a case series and literature review. Postgraduate Med J. 2021;97:667–71.
McGuire L, Cruickshank A, Munro P. Alcoholic ketoacidosis. Emerg Med J. 2006;23:417–20.
Burstal R, Reilly J, Burstal B. Fasting or starving? Measurement of blood ketone levels in 100 fasted elective and emergency adult surgical patients at an Australian tertiary hospital. Anaesth Intensive Care. 2018;46:463–7.
Dennhardt N, et al. Impact of preoperative fasting times on blood glucose concentration, ketone bodies and acid–base balance in children younger than 36 months: a prospective observational study. Eur J Anaesthesiol. 2015;32:857–61.
Millar R, Chiappazzo A, Palmer B. Starvation ketosis in the pediatric emergency department: a prospective estimate of prevalence. Pediatr Emerg Care. 2022;38:e147–50.
O'Donohoe PB, Kessler R, Beattie TF. Exploring the clinical utility of blood ketone levels in the emergency department assessment of paediatric patients. Emerg Med J. 2006;23:783–7.
Pandey M, et al. Point-of-care testing in paediatric settings in the UK and Ireland: a cross-sectional study. BMC Emerg Med. 2022;22:1–9.
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Wells GA, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute: Oxford; 2000.
Schünemann H, Brozek J, Guyatt G, Oxman A. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from guidelinedevelopment.org/handbook. 2019.
Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Durnin S, et al. The utility of ketones at triage: a prospective cohort study. Arch Dis Childhood. 2020;105:1157–61.
Levy JA, Waltzman M, Monuteaux MC, Bachur RG. Value of point-of-care ketones in assessing dehydration and acidosis in children with gastroenteritis. Acad Emerg Med. 2013;20:1146–50.
Torres L, Sanchez M, Cid B, Vicente E, Velasco R. A higher level of ketonaemia does not predict oral rehydration failure in vomiting paediatric patients and routine measurement is unnecessary. Acta paediatrica (Oslo, Norway : 1992). 2018;107:714–7.
Lee J-Y, Ryu J-M, Lee JS, Ko T-S, Yum M-S. Clinical implications of ketosis in children with benign convulsions with mild gastroenteritis. J Clin Neurol. 2020;16:96–101.
Arredondo Montero J, et al. Alterations and diagnostic performance of capillary ketonemia in pediatric acute appendicitis: a pilot study. Pediatr Surg Int. 2023;39:1–8.
Pikija S, et al. Is on-admission capillary blood beta-hydroxybutyrate concentration associated with the acute stroke severity and short-term functional outcome? Neurol Res. 2013;35:959–67.
Capozzi ME, et al. The limited role of glucagon for ketogenesis during fasting or in response to SGLT2 inhibition. Diabetes. 2020;69:882–92.
Perry RJ, et al. Dehydration and insulinopenia are necessary and sufficient for euglycemic ketoacidosis in SGLT2 inhibitor-treated rats. Nat Commun. 2019;10:1–10.
Bernini A, et al. Modulation of cerebral ketone metabolism following traumatic brain injury in humans. J Cerebral Blood Flow Metab. 2020;40:177–86.
Rojas-Morales P, Tapia E, Pedraza-Chaverri J. β-Hydroxybutyrate: a signaling metabolite in starvation response? Cell Sign. 2016;28:917–23.
Gunst J, et al. Impact of tight glucose control on circulating 3-hydroxybutyrate in critically ill patients. Critical Care. 2021;25:1–8.
Karagiannis F, et al. Impaired ketogenesis ties metabolism to T cell dysfunction in COVID-19. Nature. 2022;609:801–7.
Wang Y, Chi H. Fasting as key tone for COVID immunity. Nat Metab. 2022;4:1229–31.
Dhatariya KK. Defining and characterising diabetic ketoacidosis in adults. Diabetes Res Clin Pract. 2019;155:107797.
Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32:1335–43.
Cooperman MT, Davidoff F, Spark R, Pallotta J. Clinical studies of alcoholic ketoacidosis. Am Diabetes Assoc. 1974;23:433–9.
Shah P, Isley WL. Ketoacidosis during a low-carbohydrate diet. New Engl J Med. 2006;354:97–8.
Funding
None declared.
Author information
Authors and Affiliations
Contributions
Su An Hui: study concept and design, search, acquisition of data, preparation of manuscript. Dr. Angela Lin Chiew: study concept and design, search, critical revision of manuscript for intellectual content. Dr. Barbara Depczynski: study concept and design, search, critical revision of manuscript for intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Patients or the public were not involved in the design, conduct, reporting, nor dissemination plans of our research.
Consent for publication
Patient consent for publication: Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search strategy. Table 3. Risk of bias using Newcastle-Ottawa Scale. Table 4. Certainty assessment based on outcomes.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hui, S.A., Chiew, A.L. & Depczynski, B. What is the utility of blood beta-hydroxybutyrate measurements in emergency department in patients without diabetes: a systematic review. Syst Rev 12, 71 (2023). https://doi.org/10.1186/s13643-023-02203-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-023-02203-7