
Abstract
Background
Approximately 45% of all under-five child deaths are among newborn infants, babies in their first 28 days of life, or the neonatal period every year in the World Health Organization (WHO) Africa Region. To facilitate the achievement of Sustainable Development Goal (SDG) 3.2, innovative interventions are needed to address this challenge. Thus, this scoping review aims to map research evidence on perinatal asphyxia among neonates in the WHO Africa Region.
Methods
This scoping review will be guided by the Arksey and O’Malley framework, Levac et al. recommendations, and the Joanna Briggs Institute checklist for scoping reviews. Relevant published literature will be searched using a combination of keywords, Boolean terms, and Medical Subject Headings in the following databases: PubMed, SCOPUS, CINAHL, and Web of Science from January 2016 onwards. We will further search the World Health Organization and government websites, as well as the reference list of included studies for potentially eligible studies. This scoping review will include research evidence involving countries in the WHO Africa Region, with a focus on the burden of perinatal asphyxia, contributory/associated factors of perinatal asphyxia, clinical interventions for perinatal asphyxia, and interventions/strategies for the prevention of perinatal asphyxia in the SDGs era. Two reviewers will independently sort the studies to include and exclude, guided by the eligibility criteria. Also, the data from the included studies will be extracted and any discrepancies resolved using a third reviewer. Thematic analysis will be conducted, and the findings reported using both qualitative tables and figures. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Review (PRISMA-ScR) will be followed to report this study’s results. Quality appraisal of the included studies will be done utilising the mixed methods appraisal tool version 2018.
Conclusion
This scoping review results may reveal research evidence gaps to inform future primary studies, systematic reviews and meta-analyses; and possibly contribute towards the realisation of the SDG 3.2 by countries in the WHO Africa Region. The finding of this review will be disseminated using multiple channels such as workshops, peer review publications, conferences, and social media.
Similar content being viewed by others


Background
Perinatal asphyxia is a lack of blood flow or gas exchange to or from the foetus in the period immediately before, during, or after the birth process [1]. In other words, the World Health Organization [2] defined perinatal asphyxia as “the failure to initiate and sustain breathing at birth” [2]. A diagnosis of asphyxia is established, when a newborn has an APGAR (Appearance, Pulse, Grimace, Activity, and Respiration) score of less than seven at the first to the fifth minute after birth. Birth asphyxia results in impairment of tissue perfusion leading to hypoxemia and metabolic acidosis with multi-organ failure or death [3]. Globally, an estimated 4 million newborns die in the neonatal period; 3 million of them died within 7 days of life [3]. More than 99% of neonatal mortality occurs in lower-and-middle-income countries (LMICs) [4]. Neonatal mortality accounted for 46% of under-five mortality in 2014 and it is estimated to increase to 52% by 2030 if appropriate measures are not implemented to address it [5]. Moreover, perinatal asphyxia is said to be responsible for about 42 million disability-adjusted life years (DALYs) [6]. To this end, reducing preventable newborn deaths is part of the global health agenda captured in the Sustainable Development Goals (SDGs) [7].
The United Nations Sustainable Development Goal three (SDG 3) seeks among other targets to end preventable deaths of newborns and children under 5 years of age, with all countries aiming to reduce neonatal mortality to less than 12 per 1000 live births and under-5 mortality to less than 25 per 1000 live births by 2030 (SDG 3.2) [7]. In LMICs however, the proportion of birth asphyxia is estimated to be more than ten (10) times higher compared to high-income countries (HIC) (2 per 1000 births in HIC) [8]. To reduce neonatal mortality to less than 12 per 1000 live births, interventions such as improving skills of birth attendance, increasing the availability of emergency obstetric care, and training of this personnel with access to resuscitation equipment among others have been suggested [9, 10]. However, there is the need to understand the contributory factors to enable the scale-up or implementation of appropriate clinical and contextual preventive interventions. Thus, to reduce newborn deaths and DALYs attributable to perinatal asphyxia, research evidence on burden of perinatal asphyxia, contributory/associated factors of perinatal asphyxia, clinical interventions for perinatal asphyxia, and interventions/strategies for the prevention (primary, secondary and tertiary) [11] of perinatal asphyxia is crucial.
Although several primary studies and systematic reviews may have been conducted in the past relating to perinatal asphyxia, about 45% of all under-five child deaths are among newborn infants, babies in their first 28 days of life or the neonatal period every year in the WHO Africa Region [12]. To this end, it is essential to identify literature glut and gaps in order to guide subsequent research and health policy decisions and reforms. Therefore, this study aims to systematically map and describe the range of evidence relating to perinatal asphyxia in the SDGs era in the WHO Africa Region.
Methods
This scoping review will be conducted using the Arksey and O’Malley framework (identifying the research question; identifying relevant studies; study selection; charting the data; and collating, summarising and reporting results) [13] including the Levac et. al. recommendations [14]. Also, the recent Joanna Briggs Institute guidelines for scoping reviews will be consulted [15]. The Preferred Reporting Items for Systematic and Meta-Analyses Checklist was used as a guide to write this protocol (Supplementary file 1).
Identifying the research question
This scoping review study’s question will be: For children less than 28 days old, what research evidence on perinatal asphyxia exists in the WHO Africa Region within the SDGs era? The sub-review questions will be as follows:
-
What research evidence exists on the burden (incidence, prevalence, and mortality) of perinatal asphyxia in the WHO Africa Region?
-
What research evidence exists on the contributory/associated factors of perinatal asphyxia in the WHO Africa Region?
-
What research evidence exists on interventions/strategies for the prevention (primary, secondary, and tertiary) of perinatal asphyxia in the WHO Africa Region?
-
What research evidence exists on clinical interventions for perinatal asphyxia in the WHO Africa Region?
The eligibility criteria for this review are defined in Table 1 below.
Identify relevant studies
Relevant published literature that meets this review criteria will be sought in PubMed, SCOPUS and CINAHL, and Web of Science to answer the review question. The search engine Google Scholar and the World Health Organization and government websites, and the reference list of included studies will be searched to identify potentially eligible studies. The electronic search strategy will be developed in consultation with an expert librarian and guided by the Peer Review of Electronic Search Strategies (PRESS) statement. The search based on an expert librarian’s advice will comprise of keywords, Boolean terms, and Medical Subject Heading (MeSH) terms or Subject Headings where applicable (Table 2). Based on the database, the syntax will be modified. During the database search, language and study design restrictions will be removed, but the date (from 2016 onwards to the last search date) will be restricted. The Principal Investigator (MKM) will conduct the search with the help of the expert librarian. The search results will be documented and imported onto Mendeley Desktop Library.
Study selection
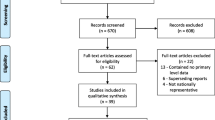
The selection of the studies will be conducted in two phases using pretested screening forms. At the first phase (titles and abstracts screening), duplicate articles will be removed, and two reviewers (MKM and FKT) will independently apply the review eligibility criteria to include articles that meet the criteria and exclude those not eligible. Any disagreement in this phase will be resolved through discussions. At the second phase, the full-text articles will be compiled and screened by two independent reviewers (MKM and FKT) using the eligibility criteria. Discrepancies between reviewers’ responses at this phase will be addressed using a third reviewer (DK). In the situation where a full-text article cannot be found from the databases, assistance would be sought from the Catholic University’s library and the Stellenbosch University Library or request the full text from the author(s) via their email address (es) for screening. The PRISMA 2020 flow diagram (Fig. 1) will be used to document the study selection process [16].

PRISMA 2020 flow diagram
Charting the data
A data charting form will be developed and piloted using at least 10% of the included studies by two independent reviewers. Differences of opinion will be resolved through discussion and the data extraction form modified accordingly. The author and date, study title, study objective/aim, study design, study location (country), study setting (facility-based, community-based), geographical location (rural and urban), study findings (incidence, prevalence, outcomes, contributory/associated factors, clinical interventions, and preventive interventions) will be extracted from the included studies independently by two reviewers (MKM and FKT). A third reviewer (DK) will resolve any discrepancies.
Quality appraisal
Mixed Method Quality Appraisal Tool (MMAT) Version 2018 [17] will be used to evaluate the methodological quality of all the studies included in this proposed scoping review. The relevance of the study, study design, adequacy and methodology, data collection, analysis of data, and study findings reported of all included will be examined using the MMAT tool. Quality assessment will be helpful in reporting the risk of bias of the studies included. The quality of the incorporated studies will be categorised by crafting the entire percentage quality score as specified by the 2018 MMAT. A percentage quality score ranging from ≤50% will be considered as low quality, 51–75% will be examined as average quality, and 76–100% will be considered as high quality.
Collating, summarising, and reporting the results
The analysis of the data collated will include descriptive analysis to describe the characteristics of the included studies and present using frequencies (percentage), tables, figures and maps. However, qualitative synthesis of the study findings through thematic analysis. Based on initial coding and categorisation, a thematic analysis will be utilised to define the themes linked with this study's research questions. A summary of the study findings will be reported qualitatively for each theme. All emerging sub-themes relating to perinatal asphyxia will be structured around the following: burden of perinatal asphyxia, contributory/associated factors of perinatal asphyxia, clinical interventions for perinatal asphyxia, interventions/strategies for the prevention of perinatal asphyxia in the WHO Africa Region. This study will not undertake a meta-analysis due to the exploratory nature of scoping review studies; however, a follow-up meta-analysis using the quantitative data from this study may be conducted. The PRISMA extension for scoping reviews will be followed to present the results.
Discussions
Approximately 45% of all under-five child deaths are among newborn infants, babies in their first 28 days of life or the neonatal period every year in the WHO Africa Region. Innovative interventions are needed to address this challenge. Hence, this scoping review aims to map research evidence on perinatal asphyxia among neonates in the WHO Africa Region focusing on the burden of perinatal asphyxia, contributory/associated factors of perinatal asphyxia, clinical interventions for perinatal asphyxia, interventions/strategies for the prevention of perinatal asphyxia. It is anticipated that the results of this study will lead to further research and provide evidence-based information to address perinatal asphyxia among neonates in the WHO Africa Region. This study will exclude studies conducted in the millennium development era (before 1st January 2016) in order to present recent research evidence. The finding of this review will be disseminated using multiple channels such as workshops, peer review publications, conferences, and social media.
Conclusion
This scoping review results may reveal research evidence gaps to inform future research such as primary studies, systematic reviews, and meta-analyses and possibly contribute towards the realisation of the SDG 3.2 by countries in the WHO Africa Region.
Availability of data and materials
We have duly cited all studies and data is presented in the form of references.
Abbreviations
- PCC:
-
Population, Concept and Context
- LMIC:
-
Lower- and middle-income countries
- ANC:
-
Antenatal care
- MMAT:
-
Mixed Method Quality Appraisal Tool
- SSA:
-
Sub-Sahara African
- WHO:
-
World Health Organization
- DALYs:
-
Disability-adjusted life years
- APGAR:
-
Appearance Pulse Grimace Activity and Respiration
- HIC:
-
High-income countries
- MeSH:
-
Medical Subject Heading
- SDG:
-
Sustainable Development Goal
References
Woday A, Muluneh A, St DC. Birth asphyxia and its associated factors among newborns in public hospital, northeast Amhara. Ethiopia. PLoS One. 2019;14(12):1–13.
W.H.O 2021. Guidelines on Basic New Born Resuscitation. WHO Guide Basic Newborn Resusc Infant. 2012;1(2012):65.
Lawn J, Shibuya K, Stein C. No cry at birth: Global estimates of intrapartum stillbirths and intrapartum-related neonatal deaths. Bull World Health Organ. 2005;83(6):409–17.
Cecilia O, Clement BMA. A Review of Neonatal Morbidity and Mortality in an Intensive Care Unit of a Paediatric Health Facility in Lagos, Nigeria. J Trop Dis. 2013;01(03):1–12.
Lawn J, Mongi P, Cousens S. Africa’s newborns – counting them and making them count. Oppor Africa’s Newborns. 2006;2(3):12.
Usman F, Imam A, Farouk ZL, Dayyabu AL. Newborn mortality in sub-saharan africa: Why is perinatal asphyxia still a major cause? Ann Glob Heal. 2019;85(1):5.
United Nations (UN). Sustainable Development Goal. Sustain Dev Goal. 2016;1(January):24.
Rule ARL, Maina E, Cheruiyot D, Mueri P, Simmons JM, Kamath-Rayne BD. Using quality improvement to decrease birth asphyxia rates after ‘Helping Babies Breathe’ training in Kenya. Acta Paediatr Int J Paediatr. 2017;106(10):1666–73.
Bakari A, Bell AJ, Oppong SA, Bockarie Y, Wobil P, Plange-Rhule G, et al. Neonatal near-misses in Ghana: A prospective, observational, multi-center study. BMC Pediatr. 2019;19(1):1–24.
Ameyaw E, Asafo Agyei SB, Plange RG. Spectrum of Diseases seen on Neonatal Ward at Komfo Anokye Teaching Hospital, Kumasi, Ghana. Pediatr Infect Dis Open Access. 2017;02(03):1–4.
Wildner M, Nennstiel-Ratzel U. Prevention, Secondary. In: Kirch W, editor. Encyclopedia of Public Health. Dordrecht: Springer; 2008. https://doi.org/10.1007/978-1-4020-5614-7_2760.
UNITAID. Development of Strategy 2017 - 2021: Strategic Option – Reproductive , Maternal , Newborn and Child Health (RMNCH ). WHO Reprod Matern Newborn, Child Adolesc Heal. 2021;(June 2016):12.
Malley O. Scoping studies: towards a methodological framework. Methodol Framew. 2005;4549:1–13.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):1–9.
Briggs J. The Joanna Briggs Institute Reviewers ’ Manual 2015 Methodology for JBI Scoping Reviews. Methiodology JBI scoping Rev. 2015;2015:24.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed methods appraisal tool (MMAT), version 2018. Registration of copyright. 2018;1148552(10).
Acknowledgements
We owe a debt of gratitude to the Almighty God for seeing us through with this scoping review protocol. We are also thankful to Catholic University College of Ghana – Fiapre for providing us with the necessary resources to write this manuscript.
Funding
No funding has been obtained yet for this study.
Author information
Authors and Affiliations
Contributions
MK-M and DK conceptualised the study. MK-M wrote the protocol. FK-TK, MA-M and contributed to the writing. DK and VB designed the study methodology and critically reviewed the protocol. MK-M wrote the final draft manuscript and all the authors approved it.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA-P 2015 Checklist
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mensah, M.K., Tano Kofi, F.K., Ansu-Mensah, M. et al. Mapping research evidence on perinatal asphyxia within the sustainable development era in sub-Saharan Africa: a scoping review protocol. Syst Rev 11, 182 (2022). https://doi.org/10.1186/s13643-022-02058-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-022-02058-4