
Abstract
Background and objectives
Prescribed exercise to treat medical conditions and to prepare for surgery is a promising intervention to prevent adverse health outcomes for older adults; however, adherence to exercise programs may be low. Our objective was to identify and grade the quality of predictors of adherence to prescribed exercise in older adults.
Methods
Prospective observational and experimental studies were identified using a peer-reviewed search strategy applied to MEDLINE, EMBASE, Cochrane, and CINAHL from inception until October 6, 2020. Following an independent and duplicate review of titles, abstracts, and full texts, we included prospective studies with an average population age >65 years, where exercise was formally prescribed for a medical or surgical condition. We excluded studies where exercise was prescribed for a chronic musculoskeletal condition. Risk of bias was assessed using the Quality in Prognostic studies tool or Cochrane risk of bias tool, as appropriate. Predictors of adherence were identified and graded for quality using an adaptation of the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework for predictor studies.
Results
We included 19 observational studies and 4 randomized controlled trials (n=5785) Indications for exercise included cardiac (n=6), pulmonary rehabilitation (n=7), or other (n=10; surgical, medical, and neurologic). Of the 10 studies that reported adherence as the percent of prescribed sessions completed, average adherence was 80% (range 60–98%; standard deviation (SD) 11%). Of the 10 studies that reported adherence as a categorical threshold demarking adherent vs not adherent, average adherence was 57.5% (range 21–83%; SD 21%). Moderate-quality evidence suggested that positive predictors of adherence were self-efficacy and good self-rated mental health; negative predictors were depression (high quality) and distance from the exercise facility. Moderate-quality evidence suggested that comorbidity and age were not predictive of adherence.
Conclusions
These findings can inform the design of future exercise programs as well as the identification of individuals who may require extra support to benefit from prescribed exercise.
Systematic review registration
PROSPERO CRD42018108242
Similar content being viewed by others

Background
Western populations are aging at a rapid rate; it is estimated that by 2050, adults over the age of 65 could account for up to 30% of our population [1]. The declining physical function that accompanies older age is associated with increased disability, institutionalization, and mortality [2]. Additionally, frailty, a multidimensional syndrome related to age- and disease-related deficits, increases in prevalence with age and results in vulnerability to stressors and adverse health outcomes [3, 4]. Therefore, a large proportion of older individuals facing physiologic stressors, such as surgery or chronic medical conditions, are at risk of suffering worse outcomes compared to those who are more physically fit.
Older individuals preparing for surgery or who have medical problems may benefit from interventions that target increasing their physical reserve to improve outcomes [5]. Exercise has been identified as a promising perioperative intervention to improve postoperative outcomes in vulnerable older adults having surgery [6], may reduce mortality after cardiac events [7], and is a key aspect in managing peripheral artery disease and pulmonary disease [8, 9]. While exercise shows encouraging results for the treatment and prevention of adverse health outcomes in older adults [6], participants must adhere to the prescribed program in order to benefit from the exercise intervention [10, 11]. However, it is well-documented that older adults’ adherence to prescribed exercise programs is low, especially in those with complex health conditions [12,13,14,15,16]. To support successful implementation of exercise programs for older adults, we must first identify what factors influence adherence to these programs to ensure that participants are willing and able to comply. To our knowledge, no studies have synthesized and graded the strength of evidence for patient- and program-level factors that predict exercise adherence.
To address this gap in the literature, our objective was to identify and grade the quality of predictors of adherence to prescribed exercise in older adults with either a medical or surgical indication (at any time point in their course of illness, i.e., as rehabilitation or prehabilitation). This systematic review will provide knowledge to inform current care and future research regarding the implementation and design of exercise programs for older adults with medical and surgical indications for exercise.
Methods
Design
This was a systematic review that followed best practice recommendations from the Cochrane Collaboration [17] and for systematic reviews of observational and prognostic studies [18, 19]. We pre-registered our protocol (PROSPERO 2018 CRD42018108242) and reported findings using the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (see Additional file 1) [20]. All stages of the review were conducted using Distiller SR (Evidence Partners, Ottawa, Canada), a cloud-based systematic review platform.
Search strategy
A search strategy was developed in consultation with an information specialist (see Supplementary Table S2; Additional file 2) and peer-reviewed [21]. Citations were extracted from MEDLINE, Embase, Cochrane, and CINAHL from inception until October 2020. Only English or French studies were included, as reviewers were only English- and French-speaking. All reference lists were reviewed to identify relevant studies that could have been missed by our database searches.
Eligibility criteria
Studies were eligible for inclusion if the following criteria were met [1]: average age of participants ≥65 years [2]; participants had a medical or surgical condition as an indication for exercise [3]; participants were prescribed or recommended a formal exercise program, and [4] any predictors of exercise adherence were reported. Prior to beginning our review, we recognized that exercise programs for chronic musculoskeletal conditions (e.g., low back pain or chronic joint pain, or arthritis) versus other indications would be a primary source of heterogeneity. We also identified several syntheses of adherence in chronic musculoskeletal conditions that were already available [22,23,24,25,26]; therefore, we excluded studies where chronic musculoskeletal conditions were the indication for exercise. Study designs were limited to prospective observational or experimental studies to minimize the effects of misclassification bias and measurement error. Effect estimates predictive of adherence were limited to those that underwent multivariable adjustment to minimize confounding bias, as recommended by best practice guidelines [19]. This meant that we included [1]: adjusted associations between participant or program characteristics and adherence reported from prospective cohort studies or the experimental arm of randomized trials of prescribed exercise [2] or the effect estimate from a randomized trial if it estimated the effect of two different program features on adherence.
Study selection and data extraction
Title and abstract screening was performed in duplicate (JFS, MV, SP); any studies reviewed as “yes” or “unsure” by either reviewer were advanced to full-text review. Agreement between both reviewers was required to exclude a study. Full-text articles were also assessed in duplicate (JFS, MV, SP) and reasons for exclusion at this stage were recorded and categorized (wrong age group, no exercise program, no predictors of adherence, no medical or surgical condition, wrong study design, and other). Disagreements between reviewers during full-text review were resolved by consensus through discussion with the senior author (DIM).
A unique data extraction form was created for this study. The form was piloted in a sample of 8 studies by two extractors (MV, SP), which were then reviewed with the senior author. Following piloting, data was extracted by one reviewer and independently reviewed and checked for accuracy by a second reviewer. Extracted data included publication details (author, year), study design, sample size, average age, medical/surgical condition indicating exercise, and whether frailty status was assessed. We also extracted characteristics at the exercise program level, including inpatient/outpatient, supervised/unsupervised, type of program (i.e., cardiac rehabilitation, pulmonary rehabilitation, or other), and effect estimates or p-values of predictors of adherence. Our primary outcome, program adherence, was recorded, including the definition used to quantify adherence and the overall adherence rate reported.
Risk of bias assessment
Risk of bias was evaluated independently in duplicate (JFS, MV, SP), and disagreements were resolved through discussion with the senior author (DIM). Randomized controlled trials were assessed using the Cochrane risk of bias tool for randomized trials [17], while observational studies were assessed using the Quality in Prognostic Studies (QUIPS) tool [27].
Synthesis of results and analysis
Our primary analysis was structured to support the Grading of Recommendations Assessment, Development and Evaluation (GRADE) adaptation for the prognostic factor research framework [28].
First, we categorized studies based on the indication for exercise (cardiac rehabilitation, pulmonary rehabilitation, and others). Next, prognostic factors were identified and categorized within themes (based on a consensus meeting within the investigative team). Where a prognostic factor was reported by two or more studies, the strength and quality of the association of the predictive factor with adherence was assigned using the GRADE prognostic factor framework. This process applies 8 criteria that can upgrade or downgrade the quality of evidence supporting a prognostic factor and allows for evidence of a review of prognostic factors to be efficiently summarized for end-users [28].
We also calculated descriptive statistics for the overall collection of included studies, as well as by indication for exercise. Overall adherence rates were calculated and averaged across all studies, as well as by exercise indication category. Adherence measures were separated based on the measurement on a continuous scale (i.e., percent of prescribed exercise completed) or as a binary measurement (i.e., categorical threshold demarking adherent vs not adherent).
Due to the heterogeneity of the included studies, meta-analysis and subgroup analyses were not performed.
Results
Study selection
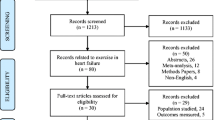
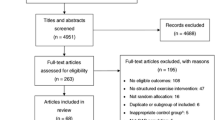
The search strategy identified 1133 records; 1121 remained after duplicates were removed. Following title and abstract screening, 284 full-text articles were assessed for eligibility and 23 were included. Study selection and reasons for exclusion are presented in Fig. 1, with reasons for exclusion at full-text review documented in see Supplementary Table S3 (Additional file 3).

PRISMA flow diagram for study selection and inclusion
Study characteristics
Study characteristics are presented in Table 1. Nineteen observational studies and 4 randomized controlled trials were included. Countries of origin of studies included Australia, Canada, USA, UK, Ireland, Denmark, and Netherlands. A total of 5651 individuals were prescribed exercise across all studies (sample sizes ranged from 30–1218 participants) and the average age ranged from 66–79 years. Indications for exercise included cardiac rehabilitation (n=6), pulmonary rehabilitation (n=7), and other (n=10; including surgical, medical, and neurologic indications). Most (20/23 (87%)) exercise programs were supervised.
Adherence to prescribed exercise rates
Exercise adherence was measured as a continuous percent of prescribed exercise sessions attended or completed in 10 studies, as a binary outcome with a specified cut-off (adherent vs not adherent) in 10 studies, as the number of sessions completed in 2 studies, and as a score of self-reported adherence in 1 study. Definitions for continuous measures of adherence included the percent of prescribed sessions completed (n=3) or attended (n=5), and of repetitions/minutes completed (n=2). Definitions for binary measures of adherence included entry into the program (n=1), a threshold number of weeks/sessions of program completed (n=3) or attended (n=3), sufficient completion by staff judgment (n=1), completion of any CR program (n=1), and continued self-reported adherence at 12 months (n=1). Of the 10 studies reporting adherence as a continuous percent, average overall adherence was 79% (range 60–95%; standard deviation (SD) 10%). Percent frequency value from Tooth et al. was used for combined measure. Of the 10 studies reporting adherence as a categorical threshold demarking adherent vs not adherent, average adherence was 58% (range 21–83%; SD 21%). Mean overall adherence for cardiac rehabilitation was 87% (continuous rate; n=1) and 44% (SD 30%; binary threshold; n=3). Mean overall adherence for pulmonary rehabilitation was 84% (SD 10%; continuous rate; n=3) and 67% (SD16%; binary threshold; n=4). Mean overall adherence for other indications was 75% (SD 9%; continuous rate; n=6) and 59% (SD14%; binary threshold; n=3). However, a lack of variance measures around adherence estimates limited our ability to perform formal comparative meta-analysis or meta-regression.
Predictors of exercise adherence
Predictors of exercise adherence were grouped into the following clusters: demographic, psychological, program-related, medical condition severity, comorbidities, and others. Demographic factors were evaluated by 13 studies [32, 35,36,37,38,39, 42, 43, 45, 48,49,50,51] (Table 2), psychological factors by 14 studies [29, 31, 32, 34,35,36,37,38, 41, 43, 45, 48,49,50,51] (Table 3), program-related factors by 7 studies [29, 33, 36, 40, 42, 44, 46], medical condition severity by 11 studies [31, 35,36,37,38, 45, 47,48,49,50,51], comorbidities by 8 studies [31, 32, 34, 39, 43, 48, 50, 51] and other predictors by 5 studies [29, 38, 42, 47, 48]. Similar factors were investigated between exercise indications (see Supplementary Tables S4, S5, S6; Additional files 4, 5, 6), however more functional measures to quantify lung function were used as potential predictors of adherence among pulmonary rehabilitation studies, while more disease characteristics and history measures were used among cardiac rehabilitation studies.
GRADE recommendations
Prognostic factors, categorized by themes, reported by at least 2 observational studies were assessed using the GRADE framework (Table 4). Overall, studies reported a small to negligible effect of most predictors. However, lower socioeconomic status (SES), the presence of depression, and farther distance from exercise facility predicted lower adherence, while higher self-efficacy and good mental health predicted higher adherence. Additionally, a dose-response effect was only observed for the predictors of depression and higher self-efficacy.
Demographics
Demographic predictors included age, sex or gender, employment, education, living situation, and social status. Lower socioeconomic status was the only demographic predictor to have an effect on adherence. Low-quality evidence suggested that lower socioeconomic status predicted lower adherence. High-quality evidence suggested that sex did not predict adherence and moderate-quality evidence suggested that age did not predict adherence. Low, low, and very low-quality evidence, respectively, suggested that employment status, living status, and education were also not predictive of adherence.
Psychological factors
Psychological predictors included anxiety, depression, self-efficacy, perception of control, and self-rated mental health. High-quality evidence supported a negative association between the presence of depression and adherence. Moderate-quality evidence suggested that individuals who had good self-rated mental health and good self-efficacy had higher adherence. Low-quality evidence suggested that the presence of anxiety and perception of control did not predict adherence.
Comorbidities
Identified comorbidities reported as predictors of exercise adherence were Body Mass Index (BMI), smoking status, hypercholesterolemia, hypertension, and Charleston Comorbidity Index (CCI). None of these were predictive of exercise adherence, which was supported by moderate-quality evidence for BMI and CCI, low-quality evidence for smoking status and hypertension, and very low-quality evidence for hypercholesterolemia. Frailty was measured and reported in 1 study [40], but was not assessed as a predictor of exercise program adherence.
Medical condition severity
Measures of respiratory disease severity (better respiratory function and higher FEV1) were not found to be predictive of adherence, supported by low-quality evidence.
Program factors
Program-level predictors included farther distance from the exercise facility and continuous vs intermittent exercise. The type of exercise program (continuous vs intermittent) was evaluated by two randomized controlled trials, which suggested no association with adherence. Although randomized trials are considered to provide high-quality evidence, we downgraded the quality of evidence to moderate-quality, given that trial findings were contradictory (one trial reported better adherence to interval exercise, one reported better adherence with continuous exercise). Moderate-quality evidence suggested that living a farther distance from the exercise facility decreased adherence.
Other
Low-quality evidence suggests that a history of exercise participation is not predictive of exercise adherence.
Risk of bias within studies
Nine observational studies were deemed to be at low risk of bias and 10 were at moderate risk of bias; no studies were at high risk of bias (Supplementary Table S7). Importantly, prognostic factor measurement and study confounding components of the tool scored low risk of bias across all studies. All four randomized trials were assessed as high risk of bias due to lack of blinding, however, this is recognizably difficult in exercise interventions (Supplementary Table S8). One trial had a high risk of bias in the blinding of outcome assessment domain; all other domains were low or unclear risk of bias.
Discussion
In this systematic review of predictors of exercise adherence in older adults with medical or surgical indications for prescribed exercise, we found that positive predictors of adherence, supported by moderate-quality evidence, were higher self-efficacy and good self-rated mental health. Negative predictors included depression (high-quality) and distance from the exercise facility (moderate quality). Interestingly, comorbidity status, sex, and age did not appear to be predictive of adherence (supported by moderate- to high-quality evidence), as none suggested a directional association. We also found that having a history of exercise participation is not a predictor of exercise program adherence. This was a surprising finding because a common assumption is that people who have exercised previously will be more adherent to a program in the future. However, this finding was supported by low-quality evidence and therefore needs further investigation. As prescribed exercise programs are less likely to be effective without high levels of adherence, these findings provide important insights into current practice and future research. However, it should be noted that while most demographic, comorbidity, and psychological predictors were evaluated in all exercise indications with similar results, self-efficacy and self-rated mental health were not evaluated in any cardiac rehabilitation studies. Additionally, distance from the exercise facility was only evaluated in cardiac and pulmonary rehabilitation studies. The small number of identified predictors with at least moderate-quality evidence and the sparse data available for many predictors suggest that future research is needed in a variety of medical and surgical indications to better understand and predict exercise adherence in older adults.
Previous reviews have estimated exercise adherence rates in a variety of populations, typically reporting similar adherence rates as those identified in our study. For example, Bullard et al. [52] reported a pooled adherence rate of 77% (95% CI 68–84%) across 30 studies of adults with cancer, cardiovascular disease or diabetes. However, few studies have evaluated what patient- and program-factors predict adherence, and to our knowledge, none have evaluated the strength of this evidence using a standard framework such as GRADE. Similar to our findings, Morgan et al. [53] identified program location as a barrier to participation and adherence, while Sheill et al. [54] found that difficulties traveling to exercise locations were a substantial barrier for individuals with advanced cancer. We found no evidence that the type of exercise program (i.e., interval vs continuous exercise) was predictive of adherence, which is consistent with recommendations that the act of engaging in exercise is likely of greater importance than the specific type of exercise performed [52, 54].
Some authors have advocated the identification of participant-level ‘red flags’ to adherence as a way to personalize exercise program design and support [52]. However, this approach requires a thorough understanding of what participant characteristics may act as red flags. At the participant level, consistent findings from our study and from others suggest that aspects of mental health are likely key predictors of adherence. The presence of depression was a strong negative predictor of adherence and the only predictor supported by high-quality evidence, while good self-rated mental health was a strong positive predictor of adherence, supported by moderate-quality evidence. In practice, identification of negative predictors, with a particular focus on mental health, could allow for increased personalization and targeting of support. For example, mental health aspects could be targeted by providing social support systems, as tangible and emotional support have been shown to be associated with lower depression among older adults [55,56,57]. The other negative predictor of exercise adherence in this study, distance from the exercise facility, could be targeted by developing and providing home-based exercise programs, which would eliminate this barrier altogether. Self-efficacy has previously been reported as a predictor of adherence in a systematic review of home-based physiotherapy [58], which is consistent with our findings and aligns with other systematic reviews that have found one’s intentions to engage in health-changing behaviors to be strongly predictive of adherence [59]. In practice, self-efficacy could be increased in patients by targeting sources of self-efficacy, such as verbal persuasion by providing positive feedback, or mastery experiences by telling patients to reflect on a time when they successfully acted upon an intention [60].
Moreover, obesity and multimorbidity were the only comorbidities with at least moderate-quality evidence as predictors. Many comorbidities were not assessed, and the impact of frailty was not reported in any studies, suggesting a need for future research to investigate the role of frailty as a potential predictor of exercise adherence. Finally, absent from the literature and related reviews is the consideration that program factors may interact with participant factors when predicting adherence. Although we were unable to identify any evidence of this phenomenon in our review, future evaluation is likely warranted to understand how participant-level red flags such as poor mental health may be modified by specifically targeted aspects of program design. Such efforts could lead to better personalization and potentially higher adherence in individuals at risk of poor participation.
Strengths and limitations
Our study’s findings should be considered in the context of its strengths and limitations. First, we conducted our review according to best-practice methodologies, which included protocol pre-registration, peer-review of our search strategy, review of multiple databases, a focus on adjusted estimates and contextualization of our findings within the GRADE strength of evidence framework. Furthermore, our results are based on identified studies that were generally at low or moderate risk of bias (apart from blinding issues in randomized trials, which is typical of exercise studies). However, despite pre-specifying a defined population of interest, included studies represented a somewhat heterogenous group of participants who engaged in exercise for cardiovascular, pulmonary, and other indications. We were also unable to adequately identify homogenous data to support quantitative meta-analyses. This may, in part, reflect the number of largely unvalidated measures used to define exercise adherence in clinical research [61]. Accordingly, we classified our studies based on whether adherence was measured using a continuous or binary definition; however, this may not have completely captured the heterogeneity in underlying adherence measures. Additionally, included studies were based in countries in Europe, North America, and Australia; therefore, findings might be limited in their generalisability to low- and middle-income countries. Finally, our search was restricted to English or French articles and we did not search unpublished data sources.
Conclusions
Design of prescribed exercise programs for older adults requires an understanding of how program and participant characteristics impact exercise adherence. Based on the GRADE Framework for prognostic research, mental health factors appear to be the most important patient-level predictors, while a farther distance from the exercise facility was the only clear program-related factor predicting adherence. These findings can help to inform the design of current programs and personalization of support for participants.
Availability of data and materials
Not applicable
Abbreviations
- QUIPS:
-
Quality in Prognostic Studies
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
- BMI:
-
Body mass index
- CCI:
-
Charleston Comorbidity Index
References
Statistics Canada. Population projections for Canada (2018 to 2068), provinces and territories (2018 to 2043); 2019.
Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332:556–62.
Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–M157.
Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. C Can Med Assoc J = J l’Association médicale Can. 2005;173:489–95.
Guideline for perioperative Care for People Living with frailty undergoing elective and emergency surgery. 1.0 ed. London: Centre for Perioperative Care; 2021.
McIsaac DI, Jen T, Mookerji N, Patel A, Lalu MM. Interventions to improve the outcomes of frail people having surgery: a systematic review. Quinn TJ, editor. PLoS One. 2017;12:e0190071.
Taylor RS, Brown A, Ebrahim S, et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med. 2004;116:682–92.
Parmenter BJ, Dieberg G, Smart NA. Exercise training for Management of Peripheral Arterial Disease: a systematic review and meta-analysis. Sports Med. 2015;45:231–44.
Puhan MA, Gimeno-Santos E, Cates CJ, Troosters T. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;12:CD005305.
Van Gool CH, Penninx BWJH, Kempen GIJM, et al. Effects of exercise adherence on physical function among overweight older adults with knee osteoarthritis. Arthritis Care Res. 2005;53:24–32.
Després J, Ewing CA. American College of Sports Medicine position stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc. 1998;30(6):975–91.
Picorelli AMA, Pereira LSM, Pereira DS, Felício D, Sherrington C. Adherence to exercise programs for older people is influenced by program characteristics and personal factors: a systematic review. J Physiother. 2014;60:151–6.
Wolinsky FD, Stump TE, Clark DO. Antecedents and consequences of physical activity and exercise among older adults. Gerontologist. 1995;35:451–62.
Jette AM, Rooks D, Lachman M, et al. Home-based resistance training: predictors of participation and adherence. Gerontologist. 1998;38:412–21.
Howze EH, Smith M, Digilio DA. Factors affecting the adoption of exercise behavior among sedentary older adults. Health Educ Res. 1989;4:173–80.
Rhodes RE, Martin AD, Taunton JE, Rhodes EC, Donnelly M, Elliot J. Factors associated with exercise An individual perspective. Sports Med. 1999;28:397–411.
Higgins J, Green S. Cochrane handbook for systematic reviews of interventions. 5.1.0The Cochrane Collaboration; 2011.
Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. 2000;283:2008–12.
Riley RD, Moons KGM, Snell KIE, et al. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ. 2019;364:k4597.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40–6.
Jordan JL, Holden MA, Mason EE, Foster NE. Interventions to improve adherence to exercise for chronic musculoskeletal pain in adults. Cochrane Database Syst Rev. 2010;1:CD005956.
Crandall S, Howlett S, Keysor JJ. Exercise adherence interventions for adults with chronic musculoskeletal pain. Phys Ther. 2013;93:17–21.
Jordan JL, Foster NE, Holden MA, Mason EE. Interventions to improve adherence to exercise for chronic musculoskeletal pain in adults. In: Jordan JL, editor. Cochrane database Syst rev. Chichester: Wiley; 2006.
Geneen LJ, Moore RA, Clarke C, Martin D, Colvin LA, Smith BH. Physical activity and exercise for chronic pain in adults: an overview of Cochrane reviews. Cochrane Database Syst Rev. 2017;4:CD011279.
Nicolson PJA, Bennell KL, Dobson FL, Van Ginckel A, Holden MA, Hinman RS. Interventions to increase adherence to therapeutic exercise in older adults with low back pain and/or hip/knee osteoarthritis: a systematic review and meta-analysis. Br J Sports Med. 2017;51:791–9.
Hayden JA, van der Windt DA, Cartwright JL, Co P. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;158:280–6.
Huguet A, Hayden JA, Stinson J, et al. Judging the quality of evidence in reviews of prognostic factor research: adapting the GRADE framework. Syst Rev. 2013;2:71.
Ades PA, Waldmann ML, Mccann WJ, Weaver SO. Predictors of cardiac rehabilitation participation in older coronary patients. Arch Intern Med. 1992;152:1033–5.
Aherne TM, Kheirelseid EAH, Boland M, et al. Supervised exercise therapy in the management of peripheral arterial disease – An assessment of compliance. Vasa - Eur J Vasc Med. 2017;46:219–22.
Brown AT, Hitchcock J, Schumann C, Wells JM, Dransfield MT, Bhatt SP. Determinants of successful completion of pulmonary rehabilitation in COPD. Int J COPD. 2016;11:391–7.
Casey E, Hughes JW, Waechter D, Josephson R, Rosneck J. Depression predicts failure to complete phase-II cardiac rehabilitation. J Behav Med. 2008;31:421–31.
Covey MK, Collins EG, Reynertson SI, Dilling DF. Resistance training as a preconditioning strategy for enhancing aerobic exercise training outcomes in COPD. Respir Med. 2014;108:1141–52.
Cox KL, Flicker L, Almeida OP, et al. The FABS trial: a randomised control trial of the effects of a 6-month physical activity intervention on adherence and long-term physical activity and self-efficacy in older adults with memory complaints. Prev Med (Baltim). 2013;57:824–30.
Craike M, Gaskin CJ, Courneya KS, et al. Predictors of adherence to a 12-week exercise program among men treated for prostate cancer: ENGAGE study. Cancer Med. 2016;5:787–94.
Fan VS, Giardino ND, Blough DK, et al. Costs of pulmonary rehabilitation and predictors of adherence in the National Emphysema Treatment Trial. COPD J Chronic Obstr Pulm Dis. 2008;5:105–16.
Gallagher R, McKinley S, Dracup K. Predictors of women’s attendance at cardiac rehabilitation programs. Prog Cardiovasc Nurs. 2003;18:121–6.
Hogg L, Garrod R, Thornton H, McDonnell L, Bellas H, White P. Effectiveness, attendance, and completion of an integrated, system-wide pulmonary rehabilitation service for COPD: prospective observational study. COPD J Chronic Obstr Pulm Dis. 2012;9:546–54.
Jensen BT, Laustsen S, Jensen JB, Borre M, Petersen AK. Exercise-based pre-habilitation is feasible and effective in radical cystectomy pathways—secondary results from a randomized controlled trial. Support Care Cancer. 2016;24:3325–31.
Karssemeijer EGA, Bossers WJR, Aaronson JA, Sanders LMJ, Kessels RPC, Olde Rikkert MGM. Exergaming as a physical exercise strategy reduces frailty in people with dementia: a randomized controlled trial. J Am Med Dir Assoc. 2019;20:1502 M.G.M. Olde Rikkert, Radboud University Medical Center, PO 9101 (hp 925), HB Nijmegen 6500, Netherlands. E-mail: Marcel.OldeRikkert@Radboudumc.nl.
Messer KL, Hines SH, Raghunathan TE, Seng JS, Diokno AC, Sampselle CM. Self-efficacy as a predictor to PFMT adherence in a prevention of urinary incontinence clinical trial. Health Educ Behav. 2007;34:942–52.
Mudge A, Adsett J. Factors predicting successful transition to community-based maintenance exercise programs following exercise rehabilitation. Cardiopulm Phys Ther J. 2013;24:18–24.
Pakzad S, Charette Y, Bourque P. Liens entre la perception de la maladie cardiovasculaire et la participation aux programmes de réadaptation cardiaque : Une étude exploratoire. Can J Cardiovasc Nurs. 2013;23:19–25.
Pandey A, Suskin N, Poirier P. The impact of burst exercise on Cardiometabolic status of patients newly diagnosed with type 2 diabetes. Can J Cardiol Canadian Cardiovasc Soc. 2017;33:1645–51.
Pickering RM, Fitton C, Ballinger C, Fazakarley L, Ashburn A. Self reported adherence to a home-based exercise programme among people with Parkinson’s disease. Park Relat Disord. 2013;19:66–71.
Rizk AK, Wardini R, Chan-Thim E, Bacon SL, Lavoie KL, Pepin V. Acute responses to exercise training and relationship with exercise adherence in moderate chronic obstructive pulmonary disease. Chron Respir Dis. 2015;12:329–39.
Tiedemann A, Sherrington C, Dean CM, et al. Predictors of adherence to a structured exercise program and physical activity participation in community dwellers after stroke. Stroke Res Treat. 2012;2012:136525.
Tooth L, McKenna K, Colquhoun D. Prediction of compliance with a post-myocardial infarction home-based walking program. Aust Occup Ther J. 1993;40:17–22.
van Montfort E, Denollet J, Widdershoven J, Kupper N. Interrelation and independence of positive and negative psychological constructs in predicting general treatment adherence in coronary artery patients — results from the THORESCI study. J Psychosom Res. 2016;88:1–7.
Selzler AM, Simmonds L, Rodgers WM, Wong EYL, Stickland MK. Pulmonary rehabilitation in chronic obstructive pulmonary disease: predictors of program completion and success. COPD J Chronic Obstr Pulm Dis. 2012;9:538–45.
Selzler AM, Rodgers WM, Berry TR, Stickland MK. The importance of exercise self-efficacy for clinical outcomes in pulmonary rehabilitation. Rehabil Psychol. 2016;61:380–8.
Bullard T, Ji M, An R, Trinh L, MacKenzie M, Mullen SP. A systematic review and meta-analysis of adherence to physical activity interventions among three chronic conditions: cancer, cardiovascular disease, and diabetes. BMC Public Health. 2019;19:1–11.
Morgan F, Battersby A, Weightman AL, et al. Adherence to exercise referral schemes by participants – what do providers and commissioners need to know? A systematic review of barriers and facilitators. BMC Public Health. 2016;16:227.
Sheill G, Guinan E, Brady L, Hevey D, Hussey J. Exercise interventions for patients with advanced cancer: a systematic review of recruitment, attrition, and exercise adherence rates. Palliat Support Care. 2019;17:686–96.
Oxman TE, Berkman LF, Kasl S, Freeman DH, Barrett J. Social support and depressive symptoms in the elderly. Am J Epidemiol. 1992;135:356–68.
Chou KL, Chi I. Social support exchange among elderly Chinese people and their family members in Hong Kong: a longitudinal study. Int J Aging Hum Dev. 2001;53:329–46.
Grav S, Hellzèn O, Romild U, Stordal E. Association between social support and depression in the general population: the HUNT study, a cross-sectional survey. J Clin Nurs. 2012;21:111–20.
Essery R, Geraghty AWA, Kirby S, Yardley L. Predictors of adherence to home-based physical therapies: a systematic review. Disabil Rehabil. 2017;39:519–34.
Husebø AML, Dyrstad SM, Søreide JA, Bru E. Predicting exercise adherence in cancer patients and survivors: a systematic review and meta-analysis of motivational and behavioural factors. J Clin Nurs. 2013;22:4–21.
Wentzel KR, Wigfield A. Handbook of motivation at school. New York: Routledge; 2009.
McLean S, Holden MA, Potia T, et al. Quality and acceptability of measures of exercise adherence in musculoskeletal settings: a systematic review. Rheumatol (United Kingdom). 2017;56:426–38.
Acknowledgements
Not applicable.
Funding
This research was supported by the Canadian Frailty Catalyst Grant. DIM acknowledges salary support from The Ottawa Hospital Anesthesiology Alternate Funds Association and the Canadian Anesthesiologists’ Society Career Scientist Award. This research was conducted with financial support from the Canadian Frailty Network (CFN), which is supported by the Government of Canada through the Networks of Centres of Excellence (NCE) program. CFN had no role in the study design, data collection, analysis or interpretation of the results, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; drafting the manuscript or revising it critically for important intellectual content; and final approval of the version to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
Use of Distiller SR was supported by the Department of Anesthesiology & Pain Medicine at The Ottawa Hospital. All authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 2: Supplementary Table S2.
Search Strategy.
Additional file 3: Supplementary Table S3.
Full Text Review Reasons for Exclusion.
Additional file 4: Supplementary Table S4.
Predictors of Exercise Adherence for Cardiac Rehabilitation.
Additional file 5: Supplementary Table S5.
Predictors of Exercise Adherence for Pulmonary Rehabilitation.
Additional file 6: Supplementary Table S6.
Predictors of Exercise Adherence for Other Exercise Programs.
Additional file 7: Supplementary Table S7.
Risk of Bias Assessments for Observational Studies (QUIPS tool).
Additional file 8: Supplementary Table S8.
Risk of Bias Assessments for Randomized Controlled Trials (Cochrane Risk of Bias tool).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shaw, J.F., Pilon, S., Vierula, M. et al. Predictors of adherence to prescribed exercise programs for older adults with medical or surgical indications for exercise: a systematic review. Syst Rev 11, 80 (2022). https://doi.org/10.1186/s13643-022-01966-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-022-01966-9