
Abstract
Background
Vaccination, albeit a necessity in the prevention of infectious diseases, requires appropriate strategies for addressing vaccine hesitancy at an individual and community level. However, there remains a glaring scarcity of available literature in that regard. Therefore, this review aims to scrutinize globally tested interventions to increase the vaccination uptake by addressing vaccine hesitancy at various stages of these interventions across the globe and help policy makers in implementing appropriate strategies to address the issue.
Methods
A systematic review of descriptive and analytic studies was conducted using specific key word searches to identify literature containing information about interventions directed at vaccine hesitancy. The search was done using PubMed, Global Health, and Science Direct databases. Data extraction was based on study characteristics such as author details; study design; and type, duration, and outcome of an intervention.
Results
A total of 105 studies were identified of which 33 studies were included in the final review. Community-based interventions, monetary incentives, and technology-based health literacy demonstrated significant improvement in the utilization of immunization services. On the other hand, media-based intervention studies did not bring about a desired change in overcoming vaccine hesitancy.
Conclusion
This study indicates that the strategies should be based on the need and reasons for vaccine hesitancy for the targeted population. A multidimensional approach involving community members, families, and individuals is required to address this challenging issue.
Similar content being viewed by others

Background
Vaccines have always been one of the most innocuous and effective approaches for the prevention of many infectious diseases [1]. In spite of this, vaccine-preventable diseases are still widespread. In the preceding years, there have been outbreaks of infectious diseases in many parts of the world regardless of having effective vaccines against such diseases. The plausible reason for it could be “vaccine hesitancy” [2].
Vaccine hesitancy refers to a delay in acceptance or refusal of vaccination despite availability of vaccination services [3]. Against the backdrop of a large number of unimmunized children globally and frequent outbreaks of vaccine-preventable diseases [4], WHO has listed vaccine hesitancy as one of the top ten global health threats in 2019 [5] and has drawn major concerns across the world due to increase and resurgence of vaccine-preventable diseases. The reasons of reluctance or refusal are complex varying across time, place, specific type of vaccines [6, 7], and context-specific such as related to confidence, convenience, and complacency. Similarly, multiple factors such as religious beliefs, geographic barriers, parent-provider relationship, perceived risk of adverse events following immunization (AEFI), lack of knowledge about vaccination, and disease risk perception give rise to vaccine hesitancy [8]. A survey conducted by WHO and UNICEF showed that vaccine hesitancy emerged a decade ago [9]. However, it has gained attention due to the current changing scientific, cultural, medico-legal, and media environments, despite all the efforts made to increase the awareness and increase the vaccines uptake. The trend has been realized in several countries across the world including the UK, USA, and India [10]. This has triggered global researchers to understand the determinants of this emerging issue throughout the world. One of the reviews conducted by Jarrett et al. (2015) on similar background and methodology have conducted their review on the basis of three broad theme {dialogue-based, incentive-based (non-financial), reminder/recall-based} have some of the shortcomings. The study did not mention technology-based health literacy as well as incentive based on financial aspect in their review. The study also includes grey literature in their review which arises the potential literature bias in the review [11].
Various strategies such as community activity by community health workers and medical interns, monetary incentives, and educational videos as well as media-based approach have been piloted and evaluated in diverse settings to understand their impact on reducing the vaccine hesitancy. However, there is a paucity of critical synthesis of all these interventions across the globe and contextual summarization to guide program managers and policy makers in implementing appropriate strategies to address vaccine hesitancy. Therefore, this review aims to analyze globally tested interventions to increase the vaccination uptake by addressing the issues through globally tested interventions for people with different degrees of vaccine hesitancy.
Methods
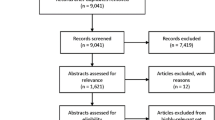
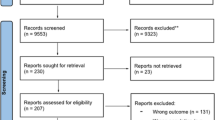
This systematic review was reported in line with the quality requirements of the PRISMA reporting guideline, from June to September 2019 and the flow chart has been mentioned as Fig. 1 for understanding the method followed [12]. The checklist of PRISMA reporting guideline has also been added as Additional Document.

Literature review data synthesis flowchart
A search was conducted in the PubMed, Global Health, and Science Direct electronic databases to identify peer-reviewed literature. Search was not restricted to any time period and included literature search for title, abstract, and full-text in English language only.
Search strategy
The search strategy was set up using database-specific vocabularies. The literature search was conducted using the keywords “immunization,” “vaccine,” “vaccination,” “vaccine strategy,” “vaccine intervention,” “vaccine hesitant,” “vaccine hesitancy,” “vaccine refusal,,” “trust in vaccination,” “vaccine confidence,” “vaccine resistance,” “vaccine impact,” “vaccine concern,” “vaccine rejection,” and “vaccine side effects” using “AND” and “OR” operators.
Inclusion and exclusion criteria
While searching for vaccination strategies, we considered universally recommended vaccines for children, adolescents, and adults such as diphtheria, tetanus, pertussis, poliomyelitis, hepatitis B, tuberculosis (BCG vaccine) measles, mumps, rubella, hemophilus influenza B (Hib), varicella, pneumococcal vaccine, meningococcal vaccine, human papillomavirus (HPV), oral polio vaccine, and seasonal influenza vaccine. Based on the objective, we included interventions that were targeted towards addressing vaccine hesitancy among parents and caregivers. For review, descriptive and analytical studies that described the effect of strategies on addressing vaccine hesitancy were included.
Studies that were opinion-based or did not focus primarily on populations eligible to receive vaccine or their parents or that did not allow the authors to extract information on vaccination were excluded from our analysis.
Study selection process
Two researchers independently reviewed the identified studies for eligibility using a two-step process. In the first step, title, abstract, and keywords were screened to segregate the eligible studies followed by a full-text retrieval and screening. Similarly, data extraction was performed independently by two researchers and unmatched studies were included or excluded in consensus with a third researcher.
Data extraction and synthesis
Data extraction included study characteristics such as (1) author, year, journal, study design, study setting, study period, and study population; (2) the vaccines considered; (3) information about the intervention being studied such as type of intervention and duration of the intervention; and (4) information on follow-up time, analysis performed, and outcomes of interest.
We categorized the review under four broad themes, i.e., community health training, incentive-based approach; technology-based health literacy; and media engagement using participants, interventions, comparisons, outcomes, and study design (PICO) strategy (Fig. 2) [13].
-
1)
Community health trainings: It included community health information dissemination through health workers, mobilizers, medical officers; social mobilization through medical interns, prominent religious leaders; and knowledge- and experience-sharing by influential women from the community to accelerate vaccine uptake [13].
-
2)
Incentive-based approach: It involved incentives to encourage parents to immunize their children, including provision of food, other goods, and certificates of recognition or monetary support to encourage vaccination [13].
-
3)
Technology-based health literacy: It involved use of technology in informing beneficiaries through various modern age-technologies such as mobile phone. Activities in this category included mobile phone recall text messages in local languages, pictorial messages, and automated phone calls or interactive voice recording for spreading awareness [13].
-
4)
Media engagement: Mobilization through various campaigns and platforms such as radio, TV, and print media should feature concise, easily understood public service announcements by national public figures, well-known and authoritative local representatives, and representative members of the target population [13].

Strategies to remove a vaccine hesitancy
Critical appraisal
The Effective Public Health Practice Project (EPHPP) quality assessment tool for quantitative studies was applied to determine the risk of bias in all eligible studies [14]. Literature screening and data extraction piloting was done on five documents by all three reviewers to standardize the review and data extraction process. Furthermore, disagreements during review were resolved by consensus.
Results
The search identified 2495 peer-reviewed articles. After removing duplicates, 1141 articles were screened using title, abstract, and keywords, which excluded 1036 papers leaving 105 full-text papers for review. Of these, 33 were evaluated and described. Among the evaluated peer-reviewed literature, nine were related to community health training’s theme [15,16,17,18,19,20,21,22,23], five were related to incentive-based approach [24,25,26,27,28], eight were related to technology-based health literacy [18, 29,30,31,32,33,34,35], and eleven were related to media engagement [36,37,38,39,40,41,42,43,44,45,46] (Tables 1 and 2).
Community health trainings
Out of the total 33 studies considered, there were nine studies that were based on community health training strategy. Majority of the studies revealed parents/caregivers of children as the study population except for one study that primarily addressed the issue of vaccine hesitancy in religious leaders of a community. The most targeted vaccines were diphtheria pertussis tetanus (DPT1, DPT2, DPT3) vaccine, Bacille Calmette-Guerin (BCG) vaccine, poliovirus 3, measles, influenza, and HPV vaccine. Lack of knowledge, negative parental attitude, and misconceptions were the foremost encountered causes for vaccine hesitancy that were addressed predominantly by health workers/medical interns [15,16,17,18,19]. Home visits and information campaigns were the most common types of community training modalities except for the two studies that had personally controlled health management systems (PCHMS) and community-level nutrition information system for action (COLNISA) as community health training strategies that led to an overall rise in vaccine coverage from 21 to 33% [20, 21, 43, 44]. Community activity for systematic engagement of parents and home visits by community health workers and medical interns significantly improved program acceptance and utilization of immunization services (Table 2).
Incentive-based approach
Five studies published between 2008 and 2013 were identified that focused on performance-based incentives for vaccination [24,25,26,27,28]. Incentive-based approach mostly involved general hospitals in the rural and lower socio-economic strata of the society. Most of these studies suggested monetary incentives only. Influenza, BCG, polio, DPT2, DPT3, measles, HBV, meningococcal 4 (MCV4), and tetanus diphtheria-acellular pertussis (Tdap) were the most sought-after targeted vaccines. A dearth of financial burden and negligence were the suggested reasons for vaccine hesitancy. Findings of these studies suggested that incentives had a high impact on the uptake of immunization services. The effect of non-financial incentives on vaccine uptake for parents and communities located in low-income settings (India) was moderate (RR: 2.16, [CI: 1.54, 2.78]) [25], except for one study that depicted no increase in vaccine acceptance using incentive-based search strategy [27] (Table 2).
Technology-based health literacy
Lately, leveraging on the health literacy using technology such as informative posters, leaflets and videotapes, social media, organizing lectures, etc., were used to bring behavioral change regarding vaccination. The studies depicted that this intervention strategy was mostly acted upon in urban primary care practices and large multispecialty medical organizations. Inadequate information /rumors, parental concerns about safety and lack of awareness, clinicians’ beliefs and practice concerns attributed to vaccine hesitancy [18, 29,30,31,32]. The eight studies available highlighted and dealt with vaccine hesitancy towards polio vaccine, varicella, pneumococcal influenza, DTPDTP, hepatitis B (HBV), hemophilus influenza B (HiB), inactivated polio vaccine (IPV), and measles mumps rubella (MMR). These studies suggested that educational intervention using videos, posters, and lectures demonstrated an improved vaccine acceptance (Table 2) [33,34,35].
Media engagement
Interventions such as reminder calls, SMS, and emails were adopted as media-based strategy in nine studies to address vaccine hesitancy. Most of the studies targeted general vaccines whereas only four out of eleven studies had interventions directed towards meningococcal (MCV4), tetanus diphtheria-acellular pertussis (Tdap), MMR, and influenza vaccines [37,38,39,40]. Low income, negative attitude towards immunization, and lack of knowledge were the most recorded reasons for vaccine hesitancy. The overall study outcome with this intervention strategy revealed that simple recall messages through SMS and email were preferred; however, these did not bring the desired change in overcoming vaccine hesitancy (Table 2) [41, 42, 44, 45].
Risk of bias
Out of the 33 studies reported, 29 studies noted a high risk of bias and one study reported no risk of bias. The risk of bias is calculated on the basis of study design, analysis, withdrawals and dropouts, data collection practices, selection bias, invention integrity, blinding as part of a controlled trial, and confounders (Table 1).
Discussion
The studies included interventions with diverse approaches that were implemented in different settings and targeted various populations, which helped us to get a holistic view of interventions globally to build confidence on vaccines, increase acceptance, and promote adequate immunization behaviors. In the review, we observed that the strategies suggested or evaluated were similar to traditional strategies such as IPC and social mobilization through education and empowerment, financial and non-financial incentives for motivation of beneficiaries and mobilizers, and technology assistance for communication to bring about a behavioral change. The studies used in this systematic review are equally from low, middle and higher-income countries focusing on involvement of political leaders, medical leaders, and mobile vaccination team for addressing the issues of vaccine hesitancy [30, 36].
Studies done by Fiks et al., Williams et al., Zhang et al., and Rahman et al. reported a lower risk of bias when compared to other studies, which could be due to variation in the study design and settings [17, 18, 31, 36].
Most of the interventions analyzed in the review were primarily either to inform or to educate the target population about the risks and benefits of vaccination using community health training strategy, as lack of knowledge or awareness about vaccines was observed to be the major cause of vaccine hesitancy. These studies reported effective improvement in vaccines uptake after the exercise. Two of these studies focused on the involvement of mothers for knowledge and experience sharing [15, 16]. A study conducted by Brugha et al. revealed a significant rise from 60 to 80% in vaccine coverage after 6 months of home-visit community health training program [16]. Involvement of mothers showed a significant improvement in vaccination coverage (33–85%) in another similar study done by Usman et al. [23]. Nine studies were based on parent-centered information or education about vaccination and social mobilization of parents by health workers/medical interns [15,16,17,18,19,20,21,22,23]. All these studies showed a significant impact in changing parents’ attitude towards their child’s vaccination. Messaging on vaccination from political and religious leaders also imparted a positive impact on vaccination uptake [17, 36]. A study conducted in Denver (USA) found significant difference in attitude and practices related to immunization among vaccine-hesitant and non-hesitant religious leaders [47]. Similarly, effective communication regarding polio vaccination with the community had shown positive impact in Nigeria [29]. However, variation in study sample with no consideration towards population dynamics was a potential limitation of all the nine studies from community health training theme, as some studies are conducted involving parents and caregivers [19, 23, 36]. In some studies, information is captured from children [21]. The sample sizes are also different for these studies as one of the studies involved more than thirteen thousand participants and while another study involved 117 participants [19, 22].
Findings of studies conducted by Mouzoon et al., Banerjee et al., and Stitzer et al. suggested that incentives had a high impact on the uptake of immunization services [24, 25, 27]. Conditional cash transfer program led to a huge increase in vaccination coverage resulting in 95% coverage along with incentive-based interventions were also found to be effective in rural Nicaragua. The study shows an increase of 10% in vaccination coverage rate among 12–23 months old children to 95% for DPT3 in treatment group as compared to 85% in the control group [26]. It was evident from the synthesis that the incentive-based strategies had a positive impact on bringing about vaccination acceptance. The benefit of incentive-based health promotions had always been significant but sustainability and adherence after intervention was debatable [28]. An increasingly popular strategy in health policy is the use of “incentive” to individuals to avoid health risks. In particular, we must ask whether incentive schemes are more effective than policies that aim to address directly the barriers to “healthy” behaviors, especially those existing among disadvantaged groups. Furthermore, the implementation of incentives in large populations remained a challenge. At the same time, integration of incentives with other mother and child health services such as the Janani Suraksha Yojana implemented by Govt. of India can bring a positive change in improving immunization uptake along with education on delivery and nutrition in low-income and low-education settings [25].
Gaps in awareness such as complete absence of knowledge, less knowledge, and misconceptions were known to be the principal factors for lack of adequate health-seeking behavior. Strategies focusing on behavior change through knowledge and awareness will be most suitable for complex behavioral dynamics as it targets multiple layers of decision-making—individual, family, and society [29]. Additionally, the benefits of health literacy using technology to bring about public awareness are not only multi-faceted but also have potential to change the whole health-seeking behavior paradigm and not just the behavior towards vaccines [18]. Using mobile technology and social media has also improves peoples’ awareness for managing health and service delivery [48].
Recently, educational videos, lectures in hospital settings, mobile vaccination team visits, social marketing, and web-based questionnaires have been used to bring about a behavioral change regarding vaccination. A study conducted in the rural areas North Carolina of (USA) using social marketing campaign raised the awareness among parents and reduced barriers in accessing the HPV vaccine successfully [34]. Similarly, HPV vaccination rates were 2% higher among 9–13-year-old girls within 6 months of campaign launch [34]. Evaluation of social media interventions by Muehleisen et al. (2007) and Lemstra et al. (2011) showed a positive effect on uptake of MMR vaccine [32, 40]. In Northern Nigeria, a relative increase of ~ 310% in the polio vaccination uptake was observed through an educational intervention with a video containing awareness message about polio vaccination [21].
Furthermore, the intervention focusing on the engagement of various kinds of media to reach the population has also proved to be efficient in creating awareness and promoting beneficial health-seeking behaviors [18]. Therefore, in conjunction with awareness-creating strategies, utilization of mass media in various forms such as print, audio, television, and social media can stimulate a positive perception among the population in different settings [21, 33]. However, improper documentation and socio-economic disparity in demographics was the major downside in the health literacy using technology-based intervention strategy.
Among all the strategies, recall strategies showed least improvement in mobilizing people from negative perception to acceptance. Furthermore, findings from a study in USA showed that parents aged 30 years and above preferred e-mail reminders as compared to other modes such as phone calls and text messages [43]. Few studies from USA and Nigeria have revealed a wide support and acceptability of text messages or SMS as a mode of immunization reminder or recall. A large proportion of parents had also shown willingness to be reminded about vaccinations by their health departments and via novel modalities such as email or text messaging [41, 45, 47]. Urban parents preferred reminders from their child’s doctor (46.7%) as compared to rural parents (33.7%) [37].
Although the recall strategies showed improvement in vaccine uptake by addressing the issues of vaccine hesitancy, they were inconsistent in all studies [40, 42, 43]. Therefore, it can be perceived that these kinds of passive reminders sent through modern communication channels may be only effective in case of technology-friendly populations. It is unlikely that mere recall messages through SMS or email, which were found to be preferred, will bring a desired change in the confidence on vaccines [38].
In light of the above knowledge, it is difficult to predict the superiority of any intervention over the other. Therefore, more studies with a better study design and targeting specific populations are required. Another reason for the lack of literature can be our limited access to indexing databases, which severely limits our capability to extract large amount of published literature.
Conclusions
Vaccine hesitancy not only increases an individual’s risk of contracting a disease but also increases the risk for the community. Vaccine hesitancy is a complex issue, and no standalone strategy can address it. Despite the complexity of vaccine hesitancy and the broad range of its determinants, increasing awareness about benefits of vaccination, social media engagement activities, and carefully tailored strategies addressing the determinants of the hesitancy can bring about the desired change.
Availability of data and materials
Presented in the manuscript; any additional data can be sent if requested, specifically.
Abbreviations
- AEFI:
-
Adverse events following immunization
- BCG:
-
Bacille Calmette-Guerin
- CI:
-
Confidence interval
- COLNISA:
-
Community-level nutrition information system for action
- DPT:
-
Diphtheria pertussis tetanus
- DTaP:
-
Diphtheria, tetanus and pertussis vaccines
- EPHPP:
-
Effective Public Health Practice Project
- HBV:
-
Hepatitis B virus
- Hib:
-
Hemophilus influenza B
- HPV:
-
Human papillomavirus
- IPV:
-
Inactivated polio vaccine
- MCV:
-
Meningococcal vaccine
- MMR:
-
Measles mumps rubella
- PCHMS:
-
Personally controlled health management systems
- PICO:
-
Participants, Interventions, Comparisons, Outcomes
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RR:
-
Relative risk
- SMS:
-
Short Message Service
- Tdap:
-
Tetanus diphtheria-acellular pertussis
- TV:
-
Television
- UNICEF:
-
United Nations International Children’s Emergency Fund
- USA:
-
The United States of America
- WHO:
-
World Health Organization
References
Orenstein WA, Ahmed R. Simply put: vaccination saves lives. Proc Natl Acad Sci U S A. 2017;114(16):4031–3. https://doi.org/10.1073/pnas.1704507114.
World Health Organization. Report of the sage working group on vaccine hesitancy. Geneva: WHO; 2014. https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf. Accessed 20 Jan 2020
Global immunization coverage sustained in the past five years. https://www.who.int/immunization/global_vaccine_action_plan/gvap_2017_secretariat_report_coverage.pdf; WHO (2016). Accessed 13 Dec 2019.
Dubé E, Gagnon D, Nickels E, Jeram S, Schuster M. Mapping vaccine hesitancy-Country-specific characteristics of a global phenomenon. Vaccine. 2014;32(49):6649–54. https://doi.org/10.1016/j.vaccine.2014.09.039.
MacDonald NE. SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4.
Gowda C, Dempsey AF. The rise (and fall?) of parental vaccine hesitancy. Hum Vaccin Immunother. 2013;9(8):1755–62. https://doi.org/10.1016/j.vaccine.2015.04.036.
The Strategic Advisory Group of Experts (SAGE). Appendices to the report of the SAGE working group on vaccine hesitancy. 2014. https://www.who.int/immunization/sage/meetings/2014/october/2_SAGE_Appendicies_Background_final.pdf. Accessed 12 Feb 2020.
Marti M, De Cola M, MacDonald NE, Dumolard L, Duclos P. Assessments of global drivers of vaccine hesitancy in 2014 - looking beyond safety concerns. PLoS One. 2017;12(3):e0172310. https://doi.org/10.1371/journal.pone.0172310.
Larson HJ, Jarrett C, Schulz WS, Chaudhuri M, Zhou Y, Dube E, et al. Measuring vaccine hesitancy: the development of a survey tool. Vaccine. 2015;33(34):4165–75. https://doi.org/10.1016/j.vaccine.2015.04.037.
Streefland P, Chowdhury AM, Ramos-Jimenez P. Patterns of vaccination acceptance. Soc Sci Med. 1999;49(12):1705–16. https://doi.org/10.1016/s0277-9536(99)00239-7.
Jarrett C, Wilson R, O'Leary M, Eckersberger E, Larson HJ. SAGE Working Group on Vaccine Hesitancy. Strategies for addressing vaccine hesitancy - a systematic review. Vaccine. 2015;33(34):4180–90. https://doi.org/10.1016/j.vaccine.2015.04.040.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. https://doi.org/10.1136/bmj.b2700.
Eriksen M, Frandsen T. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Lib Assoc. 2018;106(4):420–31. https://doi.org/10.5195/jmla.2018.345.
Armijo-Olivo S, Stiles CR, Hagen NA, Biondo PD, Cummings GG. Assessment of study quality for systematic reviews: a comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: methodological research. J Eval Clin Pract. 2012;18(1):12–8. https://doi.org/10.1111/j.1365-2753.2010.01516.x.
Oche MO, Umar AS, Ibrahim MTO, Sabitu K. An assessment of the impact of health education on maternal knowledge and practice of childhood immunization in Kware, Sokoto State. J Public Heal Epidemiol. 2011;3(10):440–7.
Brugha RF, Kevany JP. Maximizing immunization coverage through home visits: a controlled trial in an urban area of Ghana. Bull World Health Organ. 1996;74(5):517–24.
Abdul Rahman MA, Al-Dabbagh SA, Al-Habeeb QS. Health education and peer leaders’role in improving low vaccination coverage in Akre district, Kurdistan region. East Mediterr Health J. 2013;19(2):125–9.
Williams SE, Rothman RL, Offit PA, Schaffner W, Sullivan M, Edwards KM. A randomized trial to increase acceptance of childhood vaccines by vaccine-hesitant parents: a pilot study. Acad Pediatr. 2013;13(5):475–80. https://doi.org/10.1016/j.acap.2013.03.011.
Spleen AM, Kluhsman BC, Clark AD, Dignan MB, Lengerich EJ. ACTION Health Cancer Task Force. J. An increase in HPV-related knowledge and vaccination intent among parental and non-parental caregivers of adolescent girls, age 9-17 years, in Appalachian Pennsylvania. J Cancer Educ. 2012;27(2):312–9. https://doi.org/10.1007/s13187-011-0294-z.
Lau AY, Sintchenko V, Crimmins J, Magrabi F, Gallego B, Coiera E. Impact of a web-based personally controlled health management system on influenza vaccination and health services utilization rates: a randomized controlled trial. J Am Med Inform Assoc. 2012;19(5):719–27. https://doi.org/10.1136/amiajnl-2011-000433.
Nasiru SG, Aliyu GG, Gasasira A, Aliyu MH, Zubair M, Mandawari SU, et al. Breaking community barriers to polio vaccination in Northern Nigeria: the impact of a grass roots mobilization campaign (Majigi). Pathog Glob Health. 2012;106(3):166–71. https://doi.org/10.1179/2047773212Y.0000000018.
Ofstead CL, Sherman BW, Wetzler HP, Langlay DAM, Mueller NJ, Ward JM, et al. Effectiveness of worksite interventions to increase influenza vaccination rates among employees and families. J Occup Environ Med. 2013;55(2):156–63. https://doi.org/10.1097/JOM.0b013e3182717d13.
Usman HR, Rahbar MH, Kristensen S, Vermund SH, Kirby RS, Habib F, et al. Randomized controlled trial to improve childhood immunization adherence in rural Pakistan: redesigned immunization card and maternal education. Trop Med Int Health. 2011;16(3):334–42. https://doi.org/10.1111/j.1365-3156.2010.02698.x.
Mouzoon ME, Munoz FM, Greisinger AJ, Brehm BJ, Wehmanen OA, Smith FA, et al. Improving influenza immunization in pregnant women and healthcare workers. Am J Manag Care. 2010;16(3):209–16.
Banerjee AV, Duflo E, Glennerster R, Kothari D. Improving immunisation coverage in rural India: clustered randomised controlled evaluation of immunisation campaigns with and without incentives. BMJ. 2010;340:1291. https://doi.org/10.1136/bmj.c2220.
Barham T, Maluccio JA. Eradicating diseases: The effect of conditional cash transfers on vaccination coverage in rural Nicaragua. J Health Econ. 2009;28(3):611–21. https://doi.org/10.1016/j.jhealeco.2008.12.010.
Stitzer ML, Polk T, Bowles S, Kosten T. Drug users’ adherence to a 6-month vaccination protocol: Effects of motivational incentives. Drug Alcohol Depend. 2011;107(1):76–9. https://doi.org/10.1016/j.drugalcdep.2009.09.006.
Robertson L, Mushati P, Eaton JW, Dumba L, Mavise G, Makoni J, et al. Effects of unconditional and conditional cash transfers on child health and development in Zimbabwe: a cluster-randomised trial. Lancet. 2013;381(9874):1283–92. https://doi.org/10.1016/S0140-6736(12)62168-0.
Ansari MA, Khan Z, Khan IM. Reducing resistance against polio drops. J R Soc Promot Health. 2007;127(6):276–9. https://doi.org/10.1177/1466424007083705.
Maltezou HC, Maragos A, Raftopoulos V, Karageorgou K, Halharapi T, Remoudaki H, et al. Strategies to increase influenza vaccine uptake among health care workers in Greece. Scand J Infect Dis. 2008;40(3):266–8. https://doi.org/10.1080/00365540701642658.
Fiks AG, Grundmeier RW, Mayne S, Song L, Feemster K, Karavite D, et al. Effectiveness of decision support for families, clinicians, or both on HPV vaccine receipt. Pediatrics. 2013;131(6):1114–24. https://doi.org/10.1542/peds.2012-3122.
Muehleisen B, Baer G, Schaad UB, Heininger U. Assessment of immunization status in hospitalized children followed by counseling of parents and primary care physicians improves vaccination coverage: an interventional study. J Pediatr. 2007;151(6):704–6. https://doi.org/10.1016/j.jpeds.2007.07.051.
Ahlers-Schmidt CR, Chesser A, Hart T, Paschal A, Nguyen T, Wittler RR. Text messaging immunization reminders: feasibility of implementation with low-income parents. Prev Med (Baltim). 2010;50(5-6):306–7. https://doi.org/10.1016/j.ypmed.2010.02.008.
Cates JR, Shafer A, Diehl SJ, Deal AM. Evaluating a county-sponsored social marketing campaign to increase mothers’ initiation of HPV vaccine for their preteen daughters in a primarily rural area. Soc Mar Q. 2011;17(1):4–26. https://doi.org/10.1080/15245004.2010.546943.
Pandey D, Vanya V, Bhagat S, Vs B, Shetty J. Awareness and attitude towards human papillomavirus (HPV) vaccine among medical students in a premier medical school in India. PLoS One. 2012;7(7):e40619. https://doi.org/10.1371/journal.pone.0040619.
Zhang EJ, Chughtai AA, Heywood A, MacIntyre CR. Influence of political and medical leaders on parental perception of vaccination: a cross-sectional survey in Australia. BMJ Open. 2019;9(3):e025866. https://doi.org/10.1136/bmjopen-2018-025866.
Stockwell MS, Kharbanda EO, Martinez RA, Lara M, Vawdrey D, Natarajan K, et al. Text4health: Impact of text message reminder-recalls for pediatric and adolescent immunizations. Am J Public Health. 2012;102(2):15–21. https://doi.org/10.2105/AJPH.2011.300331.
Milkman KL, Beshears J, Choi JJ, Laibson D, Madrian BC. Using implementation intentions prompts to enhance influenza vaccination rates. Proc Natl Acad Sci U S A. 2011;108(26):10415–20. https://doi.org/10.1073/pnas.1103170108.
Moniz MH, Hasley S, Meyn LA, Beigi RH. Improving influenza vaccination rates in pregnancy through text messaging: a randomized controlled trial. Obstet Gynecol. 2013;121(4):734–40. https://doi.org/10.1097/AOG.0b013e31828642b1.
Lemstra M, Rajakumar D, Thompson A, Moraros J. The effectiveness of telephone reminders and home visits to improve measles, mumps and rubella immunization coverage rates in children. Paediatr Child Health. 2011;16(1):1–5. https://doi.org/10.1093/pch/16.1.e1.
Clark SJ, Butchart A, Kennedy A, Dombkowski KJ. Parents’ experiences with and preferences for immunization reminder/recall technologies. Pediatrics. 2011;128(5):1100–5. https://doi.org/10.1542/peds.2011-0270.
Kharbanda EO, Stockwell MS, Fox HW, Rickert VI. Text4health: a qualitative evaluation of parental readiness for text message immunization reminders. Am J Public Health. 2009;99(12):2176–8. https://doi.org/10.2105/AJPH.2009.161364.
Hofstetter AM, Vargas CY, Kennedy A, Kitayama K, Stockwell MS. Parental and provider preferences and concerns regarding text message reminder/recall for early childhood vaccinations. Prev Med (Baltim). 2013;57(2):75–80. https://doi.org/10.1016/j.ypmed.2013.04.007.
Brown VB, Oluwatosin OA. Feasibility of implementing a cellphone-based reminder/recall strategy to improve childhood routine immunization in a low-resource setting: a descriptive report. BMC Health Serv Res. 2017;17(Suppl 2):703. https://doi.org/10.1186/s12913-017-2639-8.
Saville AW, Beaty B, Dickinson LM, Lockhart S, Kempe A. Novel immunization reminder/recall approaches: rural and urban differences in parent perceptions. Acad Pediatr. 2014;14(3):249–55. https://doi.org/10.1016/j.acap.2014.02.003.
Garcia-Dia MJ, Fitzpatrick JJ, Madigan EA, Peabody JW. Using text reminder to improve childhood immunization adherence in the Philippines. Comput Inform Nurs. 2017;35(4):212–8. https://doi.org/10.1097/CIN.0000000000000307.
Williams JTB, O'Leary ST. Denver religious leaders’ vaccine attitudes, practices, and congregational experiences. J Relig Health. 2019;58(4):1356–67. https://doi.org/10.1007/s10943-019-00800-2.
Pai RR, Alathur S. Assessing awareness and use of mobile phone technology for health and wellness: insights from India. Health Policy Tech. 2019;8(3):221–7.
Acknowledgement
We are thankful to Ruma Bhargava and Kiran Agrahari for their support in initial phase of the work which helped in taking this work further in development of the manuscript.
Funding
The authors had received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
PS originated the idea of the study and helped in conceptualization and review. PD, SG, GKS, and PN reviewed and revised the draft. MKM, SK, and SG, AR conducted the literature search and data analysis and wrote the first draft. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that their is no following financial interests/personal relationships exists which may be considered as potential competing interests:

(Dr. Pritu Dhalaria)
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Singh, P., Dhalaria, P., Kashyap, S. et al. Strategies to overcome vaccine hesitancy: a systematic review. Syst Rev 11, 78 (2022). https://doi.org/10.1186/s13643-022-01941-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-022-01941-4