
Abstract
Background
Despite the enormous financial and humanistic burden of chronic low back pain (CLBP), there is little consensus on what constitutes the best treatment options from a multitude of competing interventions. The objective of this network meta-analysis (NMA) is to determine the relative efficacy and acceptability of primary care treatments for non-specific CLBP, with the overarching aim of providing a comprehensive evidence base for informing treatment decisions.
Methods
We will perform a systematic search to identify randomised controlled trials of interventions endorsed in primary care guidelines for the treatment of non-specific CLBP in adults. Information sources searched will include major bibliographic databases (MEDLINE, Embase, CENTRAL, CINAHL, PsycINFO and LILACS) and clinical trial registries. Our primary outcomes will be patient-reported pain ratings and treatment acceptability (all-cause discontinuation), and secondary outcomes will be functional ability, quality of life and patient/physician ratings of overall improvement. A hierarchical Bayesian class-based NMA will be performed to determine the relative effects of different classes of pharmacological (NSAIDs, opioids, paracetamol, anti-depressants, muscle relaxants) and non-pharmacological (exercise, patient education, manual therapies, psychological therapy, multidisciplinary approaches, massage, acupuncture, mindfulness) interventions and individual treatments within a class (e.g. NSAIDs: diclofenac, ibuprofen, naproxen). We will conduct risk of bias assessments and threshold analysis to assess the robustness of the findings to potential bias. We will compute the effect of different interventions relative to placebo/no treatment for both short- and long-term efficacy and acceptability.
Discussion
While many factors are important in selecting an appropriate intervention for an individual patient, evidence for the analgesic effects and acceptability of a treatment are key factors in guiding this selection. Thus, this NMA will provide an important source of evidence to inform treatment decisions and future clinical guidelines.
Systematic review registration
PROSPERO registry number: CRD42019138115
Similar content being viewed by others

Background
Low back pain is the leading cause of years lived with disability across the world [30]. It is also the second most common reason reported by patients for visiting their family doctor [24] and has an estimated lifetime prevalence of 80% [59]. The most common type of low back pain by far is the non-specific type [2], indicating the absence of an identifiable cause. While acute episodes of non-specific low back pain can improve markedly in the first 6 weeks, recent estimates suggest that pain can persist for over 12 weeks in 24–61% of cases [12]. This type of chronic low back pain (CLBP) carries an enormous economic burden both from direct (e.g. treatment) and indirect (e.g. lost work productivity) costs. In the UK, the cost to the NHS from low back pain exceeds £12 billion a year (NatCen Social [45]), with the chronic form representing the largest proportion of these costs [6]. CLBP is also associated with impaired quality of life, mobility and daily function as well as social isolation, disability and depression [46].
Because the underlying pathology of non-specific CLBP is by definition unidentified, treatment is largely focused on reducing pain symptoms, and a range of pharmacological and non-pharmacological intervention strategies are used in clinical practice [39]. A recent review of international practice guidelines [47] found that while NSAIDs and exercise were commonly recommended, the endorsement of many other treatments including opioids, antidepressants, paracetamol, muscle relaxants, spinal manipulation and acupuncture varied considerably across guidelines. The apparent uncertainty over which pool of interventions constitute the most effective options for treating non-specific CLBP suggests the need for a stronger evidence base.
Network meta-analysis (NMA) provides a powerful means of assessing multiple competing interventions by synthesising data across a network of different treatments [15]. By incorporating indirect evidence (where two treatments can be compared by assessing their performance relative to a common comparator such as placebo), the relative effects of two interventions can be evaluated even when no head-to-head trials are available. This cannot be achieved with standard pairwise meta-analysis and helps to establish a hierarchy of the best interventions for a particular condition. In addition, where there is both direct and indirect evidence, these can be combined using all the available evidence to compute the relative treatment effect.
The objective of this NMA is to assess the effectiveness and acceptability of interventions endorsed in primary care practice guidelines for the treatment of non-specific CLBP, with the aim of providing a comprehensive evidence base to inform treatment decisions. The project is called Study of Pain Interventions using Network meta-Analysis: Low-back pain (SPINAL).
Methods/design
This protocol conforms to PRISMA-P [42] recommendations (Additional file 1) and was developed based on guidelines for systematic reviews of back pain interventions from the Cochrane Back and Neck Group [26]. Eligibility criteria were developed using the PICOS framework and are reported in detail in the following sections and summarised briefly in Table 1.
Population
Inclusion criteria
We will include studies of adults (≥ 18 years) with non-specific CLBP. This is typically defined as pain without a specific known cause or pathology that persists for 12 or more weeks and that occurs below the costal margin and above the inferior gluteal folds.
Studies that simply describe low back pain as non-specific or chronic without providing detail of how this was determined will be included, provided this designation does not conflict with information elsewhere in the text (e.g. where a specific cause of LBP such as infection, cancer or fracture is listed, or where there is an obvious non-chronic symptom duration). Where it cannot be reliably determined whether LBP is specific or non-specific, we will assume non-specific as this represents the vast majority of LBP cases [47]. Where LBP duration cannot be reliably determined, we will assume LBP is acute and exclude the study as it seems likely that any chronicity would have been referred to in the text; but we will document such studies and include them as part of a sensitivity analysis if there are > 5 such studies.
Exclusion criteria
We will exclude studies of LBP patients with radicular pain, e.g. sciatica (or where > 10% of participants have radicular symptoms in mixed samples of patients with and without radicular pain). Radicular symptoms are typically a result of spinal nerve compromise and represent a population that may require different treatment options and who are commonly differentiated in treatment guidelines [47]. To help ensure a consistent patient population, we will exclude studies with a minimum baseline threshold for individual patient eligibility that is below 4 on a 0–10 rating, unless separate data are available for participants with baseline pain of 4 or above. We chose a threshold of 4 or above as this represents a common and established individual patient entry criterion and will ensure a homogenous sample of patients with pain of at least a moderate, clinically meaningful level [4] who are the most likely to seek treatment. If a trial does not specify individual baseline pain as an entry criterion, we will calculate z-scores from the sample mean baseline pain using the formula z = (mean baseline pain − 4.0)/SD and retain only trials where z > − 1, indicating approximately 85% of patients reporting a baseline pain of 4 or more.
Whenever we encounter trials that include both eligible and ineligible patients, we will try to determine whether data on the eligible subset can be extracted separately (e.g. in trials including both children and adults, separate the adults; in trials including both patients with and without sciatica, separate those without sciatica; in trials with baseline pain both < 4 and ≥ 4, separate those with ≥ 4 pain; and in trials with LBP duration both below and above 12 weeks, separate those with LBP ≥ 12 weeks). If the data for the eligible subset are not available from the published papers and cannot be obtained from the authors, the entire trial will be included, if the percentage of eligible patients is expected to be more than 85% (as exemplified for the baseline pain criterion above).
Interventions
We will include interventions for the treatment of CLBP in primary care that are endorsed by any of the 15 clinical practice guidelines reviewed by Oliveira et al. [47], with the exception of herbal medicine as this is endorsed by only one guideline (and recommended against in one other guideline) and is often studied in trials of very low quality [29]. Our rationale for focusing on treatments only included in practice guidelines is that these represent the pool of intervention strategies more likely to be adopted in clinical practice and because their presence in guidelines usually indicates a higher quality evidence base [47]. Surgical and interventional pain management (e.g. spinal injections, radiofrequency denervation, deep brain and spinal cord stimulation [43]) will be excluded as these are invasive procedures that are recommended for low back only as next-line treatment in secondary or tertiary care for severe or refractory LBP where conservative primary care treatments have failed, and are not recommended in any guidelines when LBP is chronic and non-specific [47].
Both single and combined treatments are considered eligible, and medications may be fixed or flexibly dosed. For medications approved for pain, we will include only trials that use licenced dosing ranges based on European Medicines Agency guidelines. Where a drug is used off-label and no dosing guidelines exist for pain management, we will include all such trials but perform sensitivity analysis removing studies using dosages outside the approved dosing range for that drug’s approved indication.
Classification of interventions
Treatments will be grouped into intervention classes to allow us to compare the relative effects of intervention classes as well as individual treatments within a class, using a Bayesian hierarchical class-based NMA model [18, 19]. Grouping individual treatments into meaningful classes maximises statistical power and provides a simpler and more interpretable framework on which to ultimately inform treatment decisions (comparing each individual treatment with every other for 40 treatments, for example, would result in 780 potential comparisons). We will also perform separate analysis of pharmacological and non-pharmacological networks as described in the “Network meta-analysis” section.
Initial classifications were informed by key reviews of treatment guidelines for CLBP interventions [9, 25, 39, 46, 47, 56] and then circulated to seven members of the Lancet Low Back Pain Series Working Group (not previously known to the lead author) for evaluation and comment. We received responses from five members (see the “Acknowledgements” section), and subsequent refinements were made resulting in a final set of classifications (Table 2). Classifications are differentiated primarily by mechanisms of action, although when putative mechanisms were unclear (e.g. acupuncture) or there was uncertainty over the most appropriate classification, that treatment was listed in its own class.
A non-exhaustive list of examples of the most common interventions that comprise each class are given in Table 2. Pharmacological interventions returned by searches that are not listed in Table 2 will be classified based on MeSH and emtree headings, and non-pharmacological interventions will be classified after discussion with the review team prior to analysis with rationale for these classifications documented in the final report.
In the absence of any definitive criteria for differentiating ‘weak’ vs. ‘strong’ opioids, we followed the classifications used by Whittle et al. [57] where strong opioids are generally those with higher rates of conversion to morphine. For topical pharmacological agents, while the agents used (e.g. ibuprofen) are also often present in other classes, we nevertheless assessed this as a distinct class given the potential benefits of topical relative to systemic administration. We defined exercise therapy as ‘a series of specific movements with the aim of training or developing the body by a routine practice or as physical training to promote good physical health’ [1]. Although there are numerous meaningful ways to categorise exercise types, we decided on two basic classifications of non-specific and mind-body type approaches. However, if excessive heterogeneity is observed within each exercise type relative to other classes, we will explore sources of possible heterogeneity based on pre-defined exercise characteristics identified by Hayden et al. [33] as potentially important to efficacy (including dose/intensity, supervised vs. non-supervised, delivery type and design) and consider reclassification if necessary. Finally, as no consensus could be reached on the classification of McKenzie therapy, we provisionally classified this as education as the approach invokes components of several treatments, but we will explore the impact of this decision in a sensitivity analysis.
Comparator
A different eligible individual treatment or a control condition (placebo/sham or no-intervention).
Outcomes
Primary outcomes
-
(1)
Pain intensity, assessed with an established rating scale (e.g. 0–10 numerical rating scale or VAS) at specific time periods defined below
-
(2)
Acceptability, defined as (one minus) the proportion of patients who discontinued treatment during the trial for any reason
Assessment timing
The effects of different interventions on pain will be evaluated within the following distinct assessment windows: immediate (≤ 2 weeks post-randomisation), short term (> 2 weeks to ≤ 3 months), medium term (> 3 months to < 12 months) and long term (≥ 12 months). These time windows were selected based on a sample of 24 eligible articles from provisional searches. If these divisions fail to sensitively reflect the pattern of assessment timings used across studies, we may reclassify these windows prior to analysis to reflect trial practices.
As many pharmacological interventions may be more likely to be trialled for immediate and short-term outcomes, and certain non-pharmacological treatment (e.g. exercise) trials may be more likely to include long-term outcomes, separate analyses in each time window ensure that the relative efficacies of competing interventions will be evaluated in time windows appropriate for how those interventions are used. When pain ratings have been collected by the study authors at multiple time points within a time window, we will use the time point closest to the median for the immediate and short-term windows and the longest follow-up for the long-term follow-up window. If data are not reported at these time points (but are reported for other time points), we will make every possible attempt to retrieve these data to reduce the possibility of exaggerated treatment effects from selective reporting of the largest effects [49]. If we are unable to retrieve the preferred data, we will use outcomes at the next closest time point but conduct sensitivity analysis excluding these studies.
Effect sizes
Odds ratios will be computed for acceptability. If sufficient data are available, odds ratios for pain will also be computed contrasting the number of treatment responders across two interventions (or an intervention and control). A responder will be defined as a patient who demonstrates ≥ 30% and ≥ 50% reduction from baseline pain rating (we will examine both thresholds separately) reflecting ‘moderate’ and ‘substantial’ clinically important improvement according to IMMPACT recommendations [22]. When a study does not report treatment response rate, we will impute these from continuous pain ratings with an established conversion formula [28, 53], unless an excessive number of imputations are required given that this imputation assumes a normal distribution which is usually untestable.
As odds ratios can be difficult to interpret for many people, we will also present additional statistics generally perceived as more intuitive. Specifically, we will calculate risk ratios, absolute risk differences and numbers needed to treat for primary outcomes, by back transformation of the odds ratios. The baseline risk value needed for this transformation will be estimated from random-effects meta-analysis of risk from the placebo arm of placebo-controlled trials. For this purpose, we will use a subset of trials [18] judged to be representative of the overall population of chronic low back pain patients based on expert clinical input of the review team.
For pain, we will also calculate effect size as the mean difference in pain ratings across treatments, as these are expected to be reported in nearly all studies. If pain ratings are not reported on the usual 0–10 scale, they will be normalised to this scale. We will use post-treatment scores to compute effect size, unless only change from baseline scores are reported in which case we will use these. Effect sizes using either method can be legitimately pooled [13], and both produce the same effect size when study pre-treatment scores are equal across groups (as would be expected here given only randomised designs are eligible). Where we do use change from baseline scores and standard deviation(s) needed for effect size computations are not reported, they will be computed in the following priority order: first, using standard formula [5] based on the change score variance and the study pre-post correlation (or if unavailable, the average pre-post correlation across studies that report it); and second, using the average standard deviation based on studies that report it.
Secondary outcomes
Based on recommendations for a core outcome set (COS) in non-specific low back pain [8], we also included the following outcomes and associated recommended assessment measures:
-
(1)
Physical functioning (PF), assessed with the Oswestry Disability Index 2.1a or Roland-Morris Disability Questionnaire (the two recommended COS measures and the most commonly used in trials). If a study does not employ either scale, we will include any of the following: Quebec Back Pain Disability Scale, BPI-PI, MPI-PI, SF-36-PF, PROMIS-PF, CLBPDQ, LBPRS-DI, and ODI 1.0 as there is evidence of their validity as assessments of PF [8]
-
(2)
Health-related quality of life, assessed with the Short-Form Health Survey (SF-12/ SF-36) or PROMIS-GH-10.
-
(3)
Patient or physician ratings of overall improvement.
As all secondary outcomes are assessed on a continuous measure, we will use the mean difference as the effect size. If an outcome is assessed by multiple different scales, we will use the most common scale and convert scores from any other scales to the same metric if an established mapping algorithm exists. If this results in a low number of available studies (e.g. < 60% of the total studies reporting that outcome), to maximise data inclusion, we will standardise all scales for that outcome and use the standardised mean difference, provided that an inspection of the domain of the scales suggests the scales can be meaningfully combined. We will conduct sensitivity analysis in all instances where scales have been combined.
Outcomes with missing data
Where missing participant data is present, studies may report analysis on only the subset of patients who adhered to the intervention (per-protocol) or on all participants who were assigned to the intervention at the start of the trial (intention-to-treat) after missing data has been imputed (e.g. using last observation carried forward). If both per-protocol and intention-to-treat analyses are reported, we will prioritise intention-to-treat data [54]. In all instances, we will report whether analysis was conducted on data that were complete, complete after imputation or incomplete, and we will examine and report any material differences in results across these types. When primary outcomes are missing, an effort will be made to contact authors to obtain data.
Study designs
Only randomised controlled trials comparing an active intervention with another eligible intervention or control will be included. Randomisation can be at the individual or group level, and both parallel group and crossover designs will be included. For crossover designs, only data from the first trial period will be extracted to eliminate any possibility of carryover effects.
Language
No language restrictions will be initially applied, although studies for which adequate translation cannot be obtained will be considered potentially eligible and described in the final report but will not be included in the meta-analysis.
Information sources
We will search for published RCTs indexed in the following databases by the final search date: MEDLINE (1946-), MEDLINE In-Process, EMBASE (1974-), CENTRAL, CINAHL (1937-), LILACS (1982-) and PsycINFO (1967-). We will also search for published, unpublished and ongoing trials in clinical trial registries ClinicalTrials.gov and WHO International Clinical Trials Registry Platform (ICTRP). We will complement published data with results reported in these trial registries. We will additionally search the websites of drug regulatory bodies of the FDA (USA), MHRA (UK) and EMA (Europe). It is important to include unpublished data, since the well-known bias towards publication of significant findings can, when relying on published literature alone, lead to an overestimation of treatment effects and an underestimation of adverse effects [21]. The search strategy will be augmented through hand searching of relevant reviews and of the reference lists of included articles for additional studies.
For unpublished clinical trials, if a study is listed as ongoing and ≥ 1 year has elapsed since registration, we will attempt to establish whether the listed trial status is current. If it emerges that such trials have in fact been completed or terminated, we will attempt to obtain data from: (a) the trial registry, (b) study authors, (c) drug regulatory agency websites and (d) OpenTrials (which while still in its preliminary stages can provide a wide range of unpublished evidence including regulatory documents, clinical study reports and protocols). Where possible, the same sources will be approached when a trial has been published but key primary outcomes are not reported or reported only partially in the journal publication.
Search strategy
The search strategy was informed by PICOS criteria and will be comprised of three groups of terms relating to (1) randomised trials, (2) CLBP and (3) interventions. Search terms will be combined with a Boolean “AND” and consist of both controlled subject headings (where provided by the database) and free-text keywords in titles and abstracts.
Randomised trials will be identified using highly sensitive search filters validated for each database [23, 31, 41, 58] and CLBP studies identified using search terms suggested by Furlan et al. [26]. For identifying treatments, we will employ subject headings for intervention trials and an extensive list of keywords for specific interventions from clinical practice guidelines [25, 46, 47] and relevant Cochrane Reviews (https://back.cochrane.org/our-reviews).
Search strings were reviewed and approved by a healthcare information specialist at the University of Greenwich (see Additional file 2 for the draft MEDLINE example).
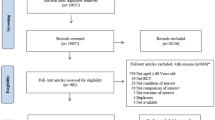
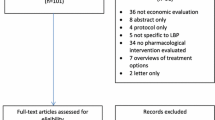
Study selection
Records returned by initial searches will be screened for relevancy in two stages. First, the titles and abstracts of each record will be independently screened by two members of the review team, who will exclude studies not meeting the eligibility criteria. The online software Rayyan [48] will be used to facilitate first stage screening by highlighting keywords relating to inclusion and exclusion criteria. Second, the full-text of the remaining articles will be screened by the same two reviewers, who will retain for inclusion in the NMA only those that meet the eligibility criteria. Disagreements at any stage will be resolved through discussion or, if not resolved, with a third member of the review team.
Data extraction
Data from each study will be extracted by one member of the review team and checked for accuracy by a senior member of the review team, with sets of studies distributed across a pool of reviewers. We will use a standardised excel coding form adapted from our previous work, with explanatory notes provided on how coding should be performed for each variable to ensure consistency across coders. If there are missing method data or missing outcome data, the corresponding author will be contacted via e-mail with one additional reminder email sent within 3 weeks if no response is received. Subsequently, other authors will be contacted. If no response is received before analysis is conducted, the study will be excluded from the NMA but the basic study findings will be described in a separate section of the final report. When data are identified as being published across multiple sources, we will prioritise extraction from the most complete data sources. Where these sources include both published and unpublished data, we will extract both but prioritise published data in the analysis as this has been subject to peer-review, but conduct sensitivity analysis including both published and unpublished data.
When available study data do not allow computation of effect sizes using standard formula (e.g. based on means and SDs) we will (a) extract other statistics (e.g. F, p, t) that allow effect sizes to be computed using alternative formula [11]; (b) contact study authors for data, and (c) for missing SDs, use the pooled SD from other studies [27] or external data. Finally, where a pain rating scale assesses not only average pain, but least and worst pain over the previous period (as in the Brief Pain Inventory), we will use only average pain ratings.
Data items
Study information extracted will include (1) study identifiers (e.g. title, authors, publication date); (2) study characteristics (e.g. trial design, source of financial support, trial size, study location); (3) participant characteristics (e.g. mean sample age, male/female ratio, SES, pain duration, severity and current or previous treatments); (4) intervention details (e.g. type and class of treatment, intervention details, duration, dosage, delivery method); and (5) outcome data (including assessment used, timing, missing data details).
Robustness of findings and risk of bias
Risk of bias will be assessed for all studies using the revised Cochrane Risk of Bias (RoB) tool (RoB 2.0 [54]). Assessments will be carried out independently by two reviewers, with any disagreement resolved by discussion or, if needed, consultation with a third reviewer. We will also collect additional measures of bias (see “Meta-regression and sensitivity analysis”) and examine their potential influence in meta-regression.
We will conduct threshold analysis [7, 50] to quantify the level of bias that would have to be present in the estimated treatment effect to have resulted in a major change in treatment ranking (such as a change in the order of the highest ranked interventions). If the magnitude of such potential bias is implausible, then conclusions on the ‘best’ treatments are more robust. If the level of bias needed to overturn treatment decisions is plausible, then we will closely examine RoB scores for that treatment as well as relevant external work to determine whether such bias is likely to be present to help evaluate our confidence in the findings.
An alternate method for assessing robustness is Salanti’s [51] GRADE for NMA extension, implemented using the CINeMA web application. This estimates overall RoB for a treatment comparison by aggregating individual study RoB scores after weighting each score based on a study’s contribution to the overall treatment effect size. For the proposed NMA, however, we chose threshold analysis as we will employ a Bayesian analysis (CINeMA currently applies frequentist weights), and threshold analysis is more suited to directly informing treatment decisions [50].
Data synthesis and analysis
We will provide a descriptive table summarising the key characteristics of each eligible study, including interventions, patient populations and trial characteristics. A network diagram will show which intervention classes were compared, with larger network nodes indicating a greater number of patients and thicker connecting lines between nodes indicating a greater number of trials.
Consistency assumption
A key assumption of NMA is that each participant should be equally likely to have received any of the treatments in the network. If this assumption holds, a key consequence is that there should be no systematic differences in effect modifiers (such as important patient characteristics) across different sets of treatment comparisons that might otherwise explain apparent intervention differences [10].
As described in the “Population” section, we will ensure similarity by restricting patient populations to those with non-specific LBP that is chronic only and who report a moderate or greater level of pain. We will also qualitatively assess the clinical similarity of populations across different treatment comparisons on potentially important factors, such as age, sex, baseline pain severity and CLBP duration [3, 32, 40], and present this in a summary table. Statistical tests of consistency we will employ are described in the “Assessment of consistency” and the “Assessment of within-comparison heterogeneity” sections. One common concern with comparing pharmacological and non-pharmacological interventions in general is that one class of intervention is administered as a first-line treatment and the other is given to treatment-resistant cases for whom previous interventions have failed. Because we are examining chronic LBP, however, treatment failure would have been likely for all patients during the acute phase of their LBP in order for chronic LBP to develop.
Network meta-analysis
We will conduct a Bayesian NMA to estimate relative treatment effects based on a synthesis of direct (head-to-head trials) and indirect evidence (where two treatments are compared indirectly via a common comparator). We will use a class-based hierarchical model [18] to estimate the relative effects of different treatment classes (e.g. NSAIDs, opioids) and of individual treatments within a class (e.g. ibuprofen, aspirin, diclofenac). Pharmacological and non-pharmacological studies may differ in patient and study characteristics and type of biases that may exist. As such, we will conduct separate analyses of these two networks along with an analysis of the whole network (providing head-to-head comparisons of pharmacological and non-pharmacological interventions are available) to see if these two approaches yield similar results.
The relative effectiveness of different treatments will be modelled as a function of their performance relative to a placebo reference treatment. This will be presented as a forest plot for class effects and in table form for class and individual effects. Mean ranks with their 95% credible intervals and SUCRA (a simple transformation of the mean rank) will be used to provide a hierarchy of the best treatments.
Estimation details
Model parameters will be estimated in WinBUGS using Markov Chain Monte Carlo simulation. Posterior distributions will be derived from binomial (binary outcomes) and normal (continuous) likelihood functions using vague prior distributions. For within-treatment study variability, we will assume a common heterogeneity standard deviation and use a partially informative uniform prior with an upper bound limit based on the outcome scale used (e.g. U(0, 10) for pain ratings). For within-class variability (of treatments), we will use a uniform prior distribution estimated separately for each class. However, for classes with only a few elements, decisions will be made on whether the within-class variance estimates can be shared across similar classes (e.g. SNRI and SSRI classes). For other parameters, we will use wide non-informative normal priors. We will examine Gelman-Rubin trace plots to check that multiple chains achieve convergence during the burn-in period, and base our estimates on 50,000 or more subsequent iterations to ensure MC estimator error is less than 5% of the standard deviation for the treatment effect and heterogeneity parameters. With respect to multi-arm trials, the correlation between multiple treatment comparisons within these trials is naturally accounted for within the Bayesian framework.
The choice between a random-effects (RE) and fixed-effect (FE) model will be informed by a comparison of Deviance Information Criteria (DIC) model fit statistics. If the DIC for the RE model is at least 3 units lower (with lower values indicating better fit) [18], we will use a RE model. If the models are otherwise similar, we will choose the more parsimonious FE model provided there is no excessive study heterogeneity from separate pairwise analysis.
Assessment of consistency
We will assess whether there is consistency of direct and indirect evidence globally across the whole network (which is a natural consequence of the similarity assumption) using the unrelated mean effects model [17]. If evidence of inconsistency is found, we will use a node-splitting approach [16] to identify possible areas of local inconsistency and, if sufficient data exist, run network meta-regression to examine whether inconsistency (and study heterogeneity) is resolved by a consideration of differences in clinical variables (the “Consistency assumption” section).
In the event of minor unresolved inconsistency, we will proceed with NMA but advise caution in the interpretation of results for comparisons where there are material differences between direct and indirect estimates. If there is evidence of substantive inconsistency, we will consider excluding network nodes.
Assessment of within-comparison heterogeneity
Study heterogeneity within each treatment comparison will be examined with forest plots from pairwise meta-analysis for an initial visual assessment (and these will be used to alert us to potential outliers). We will also compute I2, which indicates the proportion of overall variance in effect sizes due to genuine heterogeneity. I2 > 60% can indicate a moderate or greater variation in study effect sizes [34] and will be explored with meta-regression. We will also compute Cochran’s Q with p < .10 used to indicate possible presence of heterogeneity and tau-squared to provide an estimate of effect size heterogeneity for different comparisons
Meta-regression and sensitivity analysis
Given sufficient data, we will use network meta-regression to explore whether inconsistency/heterogeneity and group differences in the two primary outcomes is influenced by potential biases such as industry sponsorship, performance in less (vs. more) developed countries [14], risk of bias scores, novel agent effects [52] and researcher allegiance to the study intervention [20]. Two members of the review team will independently assess researcher allegiance (with any disagreement resolved by consensus) using a checklist developed and piloted for the current study (Additional file 3) based on the modified reprint method [44]. We will also include effect size derivation method (post vs. change scores) as a dummy-coded covariate to check that effect sizes from both methods are similar.
We will produce treatment-control comparison-adjusted funnel plots to explore possible publication bias, and if bias is suspected explore this by including sample size as a covariate. We will also perform a test of excess significance [36] which is applied to data aggregated across the whole network of interventions (thus offering higher statistical power than pairwise tests) to assess whether there is an excess of statistically significant findings.
We will also assess the robustness of the findings to various decisions by performing sensitivity analyses including removing studies (a) with high risk of bias, (b) where imputations have been performed, (c) where we assumed LBP was non-specific when this could not be definitively determined (the “Population”section), and (d) where very high/low dosages were used for off label medications. In addition, we will rerun the analysis after reclassifying McKenzie therapy into mind-body awareness exercises based on feedback from the Lancet LBP working group.
Unit of analysis issues
For trials that use cluster randomisation without adjusting standard errors for the study’s design effect [35], we will apply this adjustment ourselves. As intra-class correlations needed to make this correction are seldom reported, we will use values obtained from external literature for the outcome examined (or if these are not available use a single plausible value and examine the impact of varying this value in sensitivity analysis).
Discussion
The results from this NMA will provide an important evidence base for clinicians to inform treatment decisions by providing a comparative assessment of a wide range of interventions [55]. This will help efforts to develop a precision medicine approach to the treatment for non-specific chronic low back pain, which can be used in everyday clinical settings. While there are numerous factors that must be considered in treatment decisions, such as cost-effectiveness, individual patient suitability and patient preferences [37], reliable information on the pain-relieving effects and acceptability of a treatment as well as an assessment of how bias-free these results might be are fundamental points in guiding these decisions.
Given the sheer scale of the burden of chronic low back pain, we expect the results of the NMA to be of considerable interest to clinicians, academics, guideline developers and policymakers [38] and we will disseminate the findings widely through academic publications, conference presentations and communication with healthcare providers.
Availability of data and materials
Not applicable
Abbreviations
- CINeMA:
-
Confidence in network meta-analysis
- COS:
-
Core outcome set
- CLBP:
-
Chronic low back pain
- FDA::
-
Food and Drug Administration
- GRADE:
-
Grading of Recommendations, Assessment, Development and Evaluation
- IMMPACT:
-
Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials
- LBP:
-
Low back pain
- NMA:
-
Network meta-analysis
- NSAIDs:
-
Non-steroidal anti-inflammatory drugs
- PF:
-
Physical functioning
- PICOS:
-
Population, intervention, comparator, outcomes, study design
- PRISMA-P:
-
Preferred Reporting Items for Systematic review and Meta-Analysis Protocols
- RoB:
-
Risk of bias
- SNRI:
-
Serotonin–norepinephrine reuptake inhibitor
- SSRI:
-
Selective serotonin reuptake inhibitor
- SUCRA:
-
Surface Under the Cumulative RAnking curve
- WHO:
-
World Health Organization
References
Abenhaim L, Rossignol M, Valat JP, Nordin M, Avouac B, Blotman F, Vautravers P. The role of activity in the therapeutic management of back pain. Report of the International Paris Task Force on Back Pain. Spine (Phila Pa 1976). 2000;25(4):1S-33S. https://doi.org/10.1097/00007632-200002151-00001.
Bardin LD, King P, Maher CG. Diagnostic triage for low back pain: a practical approach for primary care. Med J Aust. 2017;206(6):268–73. https://doi.org/10.5694/mja16.00828.
Beneciuk JM, Hill JC, Campbell P, Afolabi E, George SZ, Dunn KM, Foster NE. Identifying treatment effect modifiers in the STarT back trial: a secondary analysis. Journal of Pain. 2017;18(1):54–65. https://doi.org/10.1016/j.jpain.2016.10.002.
Boonstra AM, Stewart RE, Köke AJ, Oosterwijk RF, Swaan JL, Schreurs KM, Schiphorst Preuper HR. Cut-off points for mild, moderate, and severe pain on the numeric rating scale for pain in patients with chronic musculoskeletal pain: variability and influence of sex and catastrophizing. Frontiers in Psychology. 2016;7:1466. https://doi.org/10.3389/fpsyg.2016.01466.
Borenstein M, Hedges L, Higgins J, Rothstein HR. Introduction to meta-analysis. West Sussex: Wiley; 2009.
Buchbinder R, Underwood M. Prognosis in people with back pain. CMAJ. 2012;184(11):1229–30. https://doi.org/10.1503/cmaj.120627.
Caldwell DM, Ades AE, Dias S, Watkins S, Li T, Taske N, et al. A threshold analysis assessed the credibility of conclusions from network meta-analysis. Journal of Clinical Epidemiology. 2016;80:68–76. https://doi.org/10.1016/j.jclinepi.2016.07.003.
Chiarotto A, Boers M, Deyo RA, Buchbinder R, Corbin TP, Costa LOP, et al. Core outcome measurement instruments for clinical trials in nonspecific low back pain. Pain. 2018;159(3):481–95. https://doi.org/10.1097/j.pain.0000000000001117.
Chou R, Deyo R, Friedly J, Skelly A, Weimer M, Fu R, et al. Systemic pharmacologic therapies for low back pain: a systematic review for an American College of Physicians clinical practice guideline. Annals of Internal Medicine. 2017;166(7):480–92. https://doi.org/10.7326/M16-2458.
Cipriani A, Higgins JP, Geddes JR, Salanti G. Conceptual and technical challenges in network meta-analysis. Annals of Internal Medicine. 2013;159(2):130–7. https://doi.org/10.7326/0003-4819-159-2-201307160-00008.
Cooper H, Hedges L, Valentine J. Handbook of research synthesis and meta-analysis. NY: Russell Sage Foundation; 2009.
Costa L, Maher CG, Hancock MJ, McAuley JH, Herbert RD, Costa LO. The prognosis of acute and persistent low-back pain: a meta-analysis. CMAJ. 2012;184(11):E613–24. https://doi.org/10.1503/cmaj.111271.
da Costa BR, Nüesch E, Rutjes AW, Johnston BC, Reichenbach S, Trelle S, et al. Combining follow-up and change data is valid in meta-analyses of continuous outcomes: a meta-epidemiological study. Journal of Clinical Epidemiology. 2013;66(8):847–55. https://doi.org/10.1016/j.jclinepi.2013.03.009.
Desai K, Carroll I, Asch S, Hernandez-Boussard T, Ioannidis JPA. Extremely large outlier treatment effects may be a footprint of bias in trials from less developed countries: randomized trials of gabapentinoids. Journal of Clinical Epidemiology. 2019;106:80–7. https://doi.org/10.1016/j.jclinepi.2018.10.012.
Dias S, Caldwell DM. Network meta-analysis explained. Arch Dis Child Fetal Neonatal Ed. 2019;104(1):F8–F12. https://doi.org/10.1136/archdischild-2018-315224.
Dias S, Welton NJ, Caldwell DM, Ades AE. Checking consistency in mixed treatment comparison meta-analysis. Stat Med. 2010;29(7-8):932–44. https://doi.org/10.1002/sim.3767.
Dias S, Welton NJ, Sutton AJ, Caldwell DM, Lu G, Ades AE. Evidence synthesis for decision making 4: inconsistency in networks of evidence based on randomized controlled trials. Med Decis Making. 2013;33(5):641–56. https://doi.org/10.1177/0272989X12455847.
Dias S, Ades AE, Welton NJ, Jansen JP, Sutton AJ. Network meta-analysis for decision-making (Statistics in Practice). Wiley; 2018.
Dominici F, Parmigiani G, Wolpert RL, Hasselblad V. Meta-analysis of migraine headache treatments: combining information from heterogeneous designs. Journal of the American Statistical Association. 1999;94(445):16. https://doi.org/10.2307/2669674.
Dragioti E, Dimoliatis I, Fountoulakis KN, Evangelou E. A systematic appraisal of allegiance effect in randomized controlled trials of psychotherapy. Ann Gen Psychiatry. 2015;14:25. https://doi.org/10.1186/s12991-015-0063-1.
Dwan K, Gamble C, Williamson PR, Kirkham JJ, Reporting BG. Systematic review of the empirical evidence of study publication bias and outcome reporting bias - an updated review. PLoS ONE. 2013;8(7):e66844. https://doi.org/10.1371/journal.pone.0066844.
Dworkin RH, Turk DC, McDermott MP, Peirce-Sandner S, Burke LB, Cowan P, et al. Interpreting the clinical importance of group differences in chronic pain clinical trials: IMMPACT recommendations. Pain. 2009;146(3):238–44. https://doi.org/10.1016/j.pain.2009.08.019.
Eady AM, Wilczynski NL, Haynes RB. PsycINFO search strategies identified methodologically sound therapy studies and review articles for use by clinicians and researchers. Journal of Clinical Epidemiology. 2008;61(1):34–40. https://doi.org/10.1016/j.jclinepi.2006.09.016.
Finley CR, Chan DS, Garrison S, Korownyk C, Kolber MR, Campbell S, et al. What are the most common conditions in primary care? Systematic review. Can Fam Physician. 2018;64(11):832–40.
Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–83. https://doi.org/10.1016/S0140-6736(18)30489-6.
Furlan AD, Malmivaara A, Chou R, Maher CG, Deyo RA, Schoene M, et al. 2015 updated method guideline for systematic reviews in the Cochrane Back and Neck Group. Spine (Phila Pa 1976). 2015;40(21):1660–73. https://doi.org/10.1097/BRS.0000000000001061.
Furukawa TA, Barbui C, Cipriani A, Brambilla P, Watanabe N. Imputing missing standard deviations in meta-analyses can provide accurate results. Journal of Clinical Epidemiology. 2006;59(1):7–10. https://doi.org/10.1016/j.jclinepi.2005.06.006.
Furukawa TA, Cipriani A, Barbui C, Brambilla P, Watanabe N. Imputing response rates from means and standard deviations in meta-analyses. Int Clin Psychopharmacol. 2005;20(1):49–52. https://doi.org/10.1097/00004850-200501000-00010.
Gagnier JJ, Oltean H, van Tulder MW, Berman BM, Bombardier C, Robbins CB. Herbal medicine for low back pain: a Cochrane review. Spine (Phila Pa 1976). 2016;41(2):116–33. https://doi.org/10.1097/BRS.0000000000001310.
GBD. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–59. https://doi.org/10.1016/S0140-6736(17)32154-2.
Glanville J, Dooley G, Wisniewski S, Foxlee R, Noel-Storr A. Development of a search filter to identify reports of controlled clinical trials within CINAHL Plus. Health Info Libr J. 2019;36(1):73–90. https://doi.org/10.1111/hir.12251.
Gurung T, Ellard DR, Mistry D, Patel S, Underwood M. Identifying potential moderators for response to treatment in low back pain: a systematic review. Physiotherapy. 2015;101(3):243–51. https://doi.org/10.1016/j.physio.2015.01.006.
Hayden JA, van Tulder MW, Tomlinson G. Systematic review: strategies for using exercise therapy to improve outcomes in chronic low back pain. Annals of Internal Medicine. 2005;142(9):776–85. https://doi.org/10.7326/0003-4819-142-9-200505030-00014.
Higgins JPT, Thomas J, Chandler J, Cumpston MLiT, Page MJ, Welch VA. Cochrane handbook for systematic reviews of interventions (2nd ed.). Chichester, UK: John Wiley & Sons; 2019.
Hox JJ, Moerbeek M, Van de Schoot R. Multilevel analysis: techniques and applications. London: Routledge; 2017.
Ioannidis JP, Trikalinos TA. An exploratory test for an excess of significant findings. Clin Trials. 2007;4(3):245–53. https://doi.org/10.1177/1740774507079441.
Kernot C, Tomlinson A, Chevance A, Cipriani A. One step closer to personalised prescribing of antidepressants: using real-world data together with patients and clinicians’ preferences. Evid Based Ment Health. 2019;22(3):91–2. https://doi.org/10.1136/ebmental-2019-300105.
Leucht S, Chaimani A, Cipriani AS, Davis JM, Furukawa TA, Salanti G. Network meta-analyses should be the highest level of evidence in treatment guidelines. Eur Arch Psychiatry Clin Neurosci. 2016;266(6):477–80. https://doi.org/10.1007/s00406-016-0715-4.
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–47. https://doi.org/10.1016/S0140-6736(16)30970-9.
Mallen CD, Peat G, Thomas E, Dunn KM, Croft PR. Prognostic factors for musculoskeletal pain in primary care: a systematic review. Br J Gen Pract. 2007;57(541):655–61.
Manríquez JJ. A highly sensitive search strategy for clinical trials in Literatura Latino Americana e do Caribe em Ciências da Saúde (LILACS) was developed. Journal of Clinical Epidemiology. 2008;61(4):407–11. https://doi.org/10.1016/j.jclinepi.2007.06.009.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews. 2015;4:1. https://doi.org/10.1186/2046-4053-4-1.
Morlion B. Chronic low back pain: pharmacological, interventional and surgical strategies. Nat Rev Neurol. 2013;9(8):462–73. https://doi.org/10.1038/nrneurol.2013.130.
Munder T, Brütsch O, Leonhart R, Gerger H, Barth J. Researcher allegiance in psychotherapy outcome research: an overview of reviews. Clinical Psychology Review. 2013;33(4):501–11. https://doi.org/10.1016/j.cpr.2013.02.002.
NatCen Social Research. Health survey for England, 2012., University College London, Department of Epidemiology and Public Health; 2014. https://doi.org/10.5255/UKDA-SN-7480-1.
National Institute for Health and Care Excellence. Low back pain and sciatica in over 16 s: assessment and management. NICE Guideline, No. 59. London: National Guideline Centre (UK)., National Institute for Health and Care Excellence (UK); 2016.
Oliveira CB, Maher CG, Pinto RZ, Traeger AC, Lin CC, Chenot JF, et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. 2018;27(11):2791–803. https://doi.org/10.1007/s00586-018-5673-2.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Systematic Reviews. 2016;5(1):210. https://doi.org/10.1186/s13643-016-0384-4.
Page MJ, McKenzie JE, Kirkham J, Dwan K, Kramer S, Green S, Forbes A. Bias due to selective inclusion and reporting of outcomes and analyses in systematic reviews of randomised trials of healthcare interventions. The Cochrane database of systematic reviews, 10). 2014;MR000035. https://doi.org/10.1002/14651858.MR000035.pub2.
Phillippo DM, Dias S, Welton NJ, Caldwell DM, Taske N, Ades AE. Threshold analysis as an alternative to GRADE for assessing confidence in guideline recommendations based on network meta-analyses. Annals of Internal Medicine. 2019;170(8):538–48. https://doi.org/10.7326/M18-3542.
Salanti G, Del Giovane C, Chaimani A, Caldwell DM, Higgins JP. Evaluating the quality of evidence from a network meta-analysis. PLoS ONE. 2014;9(7):e99682. https://doi.org/10.1371/journal.pone.0099682.
Salanti G, Dias S, Welton NJ, Ades AE, Golfinopoulos V, Kyrgiou M, Ioannidis JP. Evaluating novel agent effects in multiple-treatments meta-regression. Stat Med. 2010;29(23):2369–83. https://doi.org/10.1002/sim.4001.
Samara MT, Spineli LM, Furukawa TA, Engel RR, Davis JM, Salanti G, Leucht S. Imputation of response rates from means and standard deviations in schizophrenia. Schizophr Res. 2013;151(1-3):209–14. https://doi.org/10.1016/j.schres.2013.10.029.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ Open. 2019;28:366.
Tomlinson A, Furukawa TA, Efthimiou O, Salanti G, De Crescenzo F, Singh I, Cipriani A. Personalise antidepressant treatment for unipolar depression combining individual choices, risks and big data (PETRUSHKA): rationale and protocol. Evid Based Ment Health. 2019. https://doi.org/10.1136/ebmental-2019-300118.
van Tulder M, Koes B. Low back pain. In S. McMahon, M. Koltzenburg, I. Tracey, & D. Turk (Eds.), Textbook of pain (6th ed.). London: Elsevier; 2013.
Whittle SL, Richards BL, Husni E, Buchbinder R. Opioid therapy for treating rheumatoid arthritis pain. The Cochrane database of systematic reviews, 11). 2011;CD003113. https://doi.org/10.1002/14651858.CD003113.pub3.
Wong SS, Wilczynski NL, Haynes RB. Developing optimal search strategies for detecting clinically sound treatment studies in EMBASE. J Med Libr Assoc. 2006;94(1):41–7.
World Health Organization. The burden of musculoskeletal conditions at the start of the new millennium. World Health Organ Tech Rep Ser. 2003;919:i-x, 1.
Acknowledgements
We are extremely grateful to several members of the Lancet Low Back Pain Series Working Group who provided vital commentaries on the most appropriate ways to classify the different CLBP interventions. Specifically, we would like to thank Prof. Judith Turner (University of Washington, USA), Prof. Peter Croft (Keele University, UK), Prof. Douglas Gross (University of Alberta, Canada), Prof. Julie Fritz (University of Utah, USA) and Professor Martin Underwood (University of Warwick, UK) for their invaluable comments. Many thanks also to Cathryn Peppard, a health librarian at the University of Greenwich, for assistance with the construction of search strings. Andrea Cipriani is supported by the National Institute for Health Research (NIHR) Oxford Cognitive Health Clinical Research Facility, by an NIHR Research Professorship (grant RP-2017-08-ST2-006), by the NIHR Oxford and Thames Valley Applied Research Collaboration and by the NIHR Oxford Health Biomedical Research Centre (grant BRC-1215-20005). The views expressed are those of the authors and not necessarily those of the UK National Health Service, the NIHR, or the UK Department of Health.
Funding
None
Author information
Authors and Affiliations
Contributions
TT was responsible for the conception and design of the study and for writing the initial protocol draft. JPAI contributed to the design of the study. TT and SD developed the statistical analysis plan and JPAI advised. SD, DP, SW, LM, CR, JS, JF, NV, ED, BS, MS, CM, AC and JPAI provided critical revisions of all aspects of the review. The final protocol has been approved by all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
PRISMA-P checklist.
Additional file 2.
MEDLINE search string.
Additional file 3.
Researcher allegiance.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Thompson, T., Dias, S., Poulter, D. et al. Efficacy and acceptability of pharmacological and non-pharmacological interventions for non-specific chronic low back pain: a protocol for a systematic review and network meta-analysis. Syst Rev 9, 130 (2020). https://doi.org/10.1186/s13643-020-01398-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-020-01398-3