
Abstract
Background
Lower respiratory tract infection (LRTI) caused by respiratory syncytial virus (RSV) has been associated with greater risk of recurrent wheezing and subsequent asthma. However, it is still unclear whether this association is causal or not. RSV-specific monoclonal antibodies have been shown to reduce RSV-related hospitalisations in high-risk infants, i.e. those born pre-term, but the longer term follow-up has given conflicting evidence for the prevention of recurrent wheeze or asthma.
Objective
We aim to perform a systematic review and meta-analysis to determine whether or not prophylaxis with a monoclonal antibody for prevention of RSV-bronchiolitis reduces the risk of subsequent recurrent wheeze or asthma. If so, this would support the hypothesis that the association between RSV and recurrent wheeze and/or asthma is causative.
Methods
To identify relevant studies, we will search a number of databases including Medline, Embase, PubMed and Web of Science and will also manually look for unpublished data by contacting the manufacturers of monoclonal antibodies. The intervention being investigated is RSV-specific monoclonal antibody prophylaxis, and the outcome being measured is recurrent wheeze and/or asthma. Studies will be screened according to inclusion/exclusion criteria, to include primary studies of any study design type. Eligible studies will then be evaluated for quality and assessed for bias independently by three reviewers using the ‘Grading of Recommendations Assessment, Development and Evaluation’ (GRADE) approach. The results of the studies will be extracted into 2 × 2 outcome tables, and a meta-analysis will be carried out to produce forest plots based on relative risk. Heterogeneity will be assessed using the I2 statistic. The statistical software we will use is StatsDirect.
Discussion
This review will aid in determining if the relationship between RSV and asthma development is a causal one, by showing the effect (if any) of RSV prophylaxis on subsequent recurrent wheeze/asthma. If this study shows RSV prophylaxis to have no effect on the outcome of recurrent wheeze/asthma, the question of causality remains.
Similar content being viewed by others


Background
Acute bronchiolitis is an extremely common acute lower respiratory tract infection in infants, with symptoms including coughing, shortness of breath, crackles, wheezing and poor nutrition [1]. The majority of young children will experience bronchiolitis, and approximately 3% will require hospital admission [1]. In many countries, bronchiolitis is the most common reason for hospitalisation of young children [1]. It has been shown that lower respiratory tract infections in early life, particularly in infancy, are associated with development of recurrent wheeze and asthma in later childhood [2]. Pre-term infants especially are at an increased risk of both severe bronchiolitis and recurrent wheeze or asthma development independently [3, 4].
The pathogenesis of asthma is multifactorial, but in simple terms, asthma causes hypersensitivity and inflammation of the airways, with common symptoms being wheeze and shortness of breath [5]. Recurrent wheeze in infancy has a significant effect on the quality of life of both the patients and their families [6]. An international study was carried out which surveyed random samples of the general population of infants. They found that 45.2% of infants in the study population had at least one wheezing episode, and 20.3% had recurrent wheeze, defined as three or more episodes of wheezing [7]. Asthma is the most prevalent chronic respiratory disease worldwide [8]. It has been estimated that the cost of asthma is approximately £1.1 billion in the UK, highlighting it as a key public health issue [9]. It creates a huge burden on both patients and health services in terms of quality of life and cost, with the most significant impact being amongst lower socioeconomic groups and ethnic minorities [10]. With the overall prevalence increasing globally, further research is needed into why this increase is happening, and whether or not there are any preventative measures that can be undertaken [10].
Acute bronchiolitis in early life is very strongly associated with an increased risk of asthma development [11]. It has been shown that infants hospitalised with acute bronchiolitis have a significantly increased risk of developing childhood wheeze and asthma, with one study from Finland finding the risk of recurrent wheeze or asthma development, after acute bronchiolitis at less than 6 months, to be twice that of the general population [12]. However, while this association is very well established, the mechanism by which this may occur is poorly understood; thus, this relationship is yet to be proven as being causal [13]. There is much debate over whether or not acute bronchiolitis is merely just the first manifestation of asthma, rather than being the cause of it. To assess causality, studies assessing the prevention of the proposed risk factor, i.e. bronchiolitis, on the outcome of asthma are needed [11].
The most common cause of acute bronchiolitis is respiratory syncytial virus (RSV), most often in infants up to 12 months. Rhinovirus is also a cause of acute bronchiolitis, generally occurring in slightly older infants [12]. RSV is an RNA virus which uses surface glycoproteins G and F to infect cells [14]. RSV-specific monoclonal antibodies are drugs which have shown efficacy in reducing RSV hospitalisations in high-risk infants, such as those born prematurely [15]. They work by binding to this F glycoprotein, preventing viral invasion of the host cells. This provides passive immunity by blocking the fusion of infected cells and reducing cell-to-cell transmission and viral activity [14, 16]. These monoclonal antibodies have a half-life of approximately 3 weeks hence the need for once-monthly injections during RSV season, to maintain a prophylactic level [17].
The main example of RSV-specific monoclonal antibodies is palivizumab. Palivizumab is a humanised monoclonal antibody which has been found to be effective in reducing hospitalisations due to RSV bronchiolitis in high-risk infants. It is injected once monthly from November to March as this is the typical RSV season [15]. Palivizumab has been repeatedly proven to be safe and well tolerated with very low rates of minor adverse events such as injection site reaction, fever, diarrhoea and irritability [18].
Motavizumab is derived from palivizumab, therefore making it a second-generation humanised monoclonal antibody. It was originally thought to display better efficacy and therefore had a lower dose requirement when compared to palivizumab [18, 19]. However, it is important to note that motavizumab was discontinued in 2010 due to questions due to its side effect profile, particularly in regard to serious skin reactions, and questions over whether or not it was actually more efficacious than palivizumab [18, 20, 21].
Other RSV-specific monoclonal antibody biosimilars to palivizumab do exist. Suptavumab was developed recently; however, it failed to meet its primary endpoint in clinical trials and was withdrawn in 2017 [22]. Even more recently developed is nirsevimab, which has a longer half-life than palivizumab thus offers protection against RSV through one single intramuscular injection [23]. Lunamab is another RSV-specific monoclonal antibody which was developed as a cheaper biosimilar to palivizumab aimed at low-income countries [24]. However, given that these are only recently developed, it is unlikely we will come across any longer term follow-up studies with regard to recurrent wheeze.
Monoclonal antibodies are expensive drugs. It is estimated that the cost of palivizumab is around £3000–£5000 per child [25]. Despite its proven efficacy and the high prevalence of RSV infection in infancy, most children will not experience a severe illness; therefore, it is not cost-effective to give to all infants [13, 25]. A systematic review analysing the cost-effectiveness of RSV prophylaxis based on the outcome of bronchiolitis found that it is cost-effective within certain subgroups of infants who are considered to be at high risk. These subgroups include very early pre-term infants (< 32 weeks), children with congenital heart disease and aboriginal children [26]. It also found that in infants of 33–35 weeks gestational age, RSV prophylaxis could be cost-effective against bronchiolitis if also based on the presence of certain risk factors which include chronological age, number of siblings, history of atopy, absence of breast-feeding, cigarette smoke exposure and day care attendance [27].
While these cost-effectiveness analyses have concluded that passive immunoprophylaxis is not financially viable for all infants born late pre-term (33–35 weeks), they have mainly been based on the outcome of RSV bronchiolitis itself, and not recurrent wheeze [28]. Given that the lungs of infants born late pre-term are not as immunologically developed as those born over 35 weeks, and also given the fact that the RSV hospitalisation rate amongst these late pre-term infants ranges between 3.75 and 9.8%, it is clear that this is a population which cannot be ignored [29]. A sub-group analysis in this gestational age group of infants will highlight their relative risk of recurrent wheeze after receiving RSV-specific monoclonal antibody prophylaxis and potentially re-open the discussion on the cost-effectiveness of monoclonal antibodies in this sub-group of pre-term infants.
The aim of this systematic review is to determine whether or not giving monoclonal antibody RSV prophylaxis in infancy reduces the risk of recurrent wheeze or asthma development in later childhood. This will then potentially provide some answers to the question of causality in the association of RSV infection and subsequent asthma.
Methods/design
This systematic review and meta-analysis will be investigating if intervention with RSV prophylaxis compared with no prophylaxis has any effect on the outcome of recurrent wheeze or asthma in a population of infants born early pre-term to term. A literature search will be carried out across a number of databases, including Medline, Embase, Web of Science and PubMed, using a comprehensive search strategy. We will also contact the manufacturers of the monoclonal antibodies for any unpublished data. Studies will then be screened according to title and abstract, and then text body using clear inclusion and exclusion criteria. This protocol follows the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) recommendations, and the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) standards will be adhered to in reporting the findings (Additional file 1: Appendix 1).
Inclusion and exclusion criteria
Table 1 summarises the inclusion/exclusion criteria which will be used in study screening.
Types of studies and participants
This review will include all types of primary study design including randomised control trials, prospective observational case-control studies and cohort studies. All participants will be infants born early pre-term up to term and followed up from infancy to childhood (1–10 years) in line with the inclusion criteria.
Intervention, comparison and outcome
The intervention being investigated is RSV-specific monoclonal antibodies for immunoprophylaxis. This is being compared against no RSV prophylaxis. The outcome being measured is development of subsequent recurrent wheeze and/or asthma.
Information sources and search strategy
The literature search will be carried out electronically using a strategy developed in collaboration with the Queen’s University Belfast Medical Librarian. To ensure all potential literature is included, we will search Embase, Medline, PubMed, Web of Science and the Cochrane Library. We will also contact the manufacturers of the RSV-specific monoclonal antibodies for any unpublished data and search trial registries such as ‘ClinicalTrials.gov’ and ‘BMC Trials’ for potentially suitable studies that may be imminently reported. An example of the planned electronic search strategy including limits applied can be seen in Table 2.
Data collection and analysis
Selection of studies
The studies will be independently screened according to the inclusion and exclusion criteria by two reviewers. The screening will be a two-step process, first by title and abstract, and then by full-text, with those excluded by full text listed and explained in the appendix of the final report. A third-party reviewer will be involved in the case of any disagreements. Using a reference software (Mendeley), any duplicate articles will be identified. Any relevant reviews found in the literature search will only be used to source additional primary studies for this review.
Data extraction and management
We will use the standard Population, Intervention, Comparison and Outcome (PICO) approach. The population is defined as infants born at less than 36 weeks. The intervention is monoclonal antibody prophylaxis, compared to a placebo/no monoclonal antibody prophylaxis, and the primary outcome is recurrent wheeze and asthma development. Data will be extracted using an adapted form of the ‘Data collection form for Intervention review – RCTs and non-RCTs’ of the Cochrane Collaboration [30]. An example of this is in Additional file 1: Appendix 2. Data will be presented in a summary of findings table including the types of studies, population number, number in intervention, comparison groups, 2 × 2 outcome results tables, relative risk and a column for evaluation of the quality of evidence and bias risk. This summary of findings table will be presented in the results section, as per the Cochrane handbook [31]. If any data is missing, we will contact the authors of the paper to obtain the complete set.
Risk of bias
The risk of bias and quality of evidence will be evaluated independently by three reviewers using the ‘Grading of Recommendations Assessment, Development and Evaluation’ (GRADE) approach. This grades the evidence as being of high, moderate, low or very low quality by using the study design as a starting point and upgrading or downgrading the evidence according to certain criteria. Five factors which lower the quality of the evidence include limitations of study design and execution leading to bias, inconsistency or heterogeneity, indirectness, imprecision and publication bias [32]. The most likely bias to occur is sponsorship bias as a lot of the studies are likely to be funded by the manufacturers of the monoclonal antibodies.
Outcomes
To ensure comparability between studies, the primary outcome being investigated for this review is any recurrent wheeze or asthma, including parent-reported wheeze as well as formally doctor-diagnosed wheeze or asthma. Parent-reported wheeze is an important outcome to include as not all infants who wheeze will be assessed by a physician. It is possible that individual studies may measure other relevant outcomes such as RSV hospitalisation or allergy diagnosis; however, these are not a priority for this review.
Data synthesis and meta-analysis
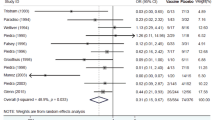
Using the main outcome of recurrent wheeze (dichotomous—yes/no) and the data from the 2 × 2 outcome tables produced, a meta-analysis will be performed using a random-effects model, with relative risk as the principal summary measure. Individual studies will be represented on a forest plot based on relative risk and 95% confidence intervals. Funnel plots will also be generated to portray publication bias or possible selective reporting within studies. The software which will be used for the meta-analysis is StatsDirect statistical software [33]. Sub-group analysis will be carried out in infants born 33–35 weeks gestational age to compare their relative risk of recurrent wheeze after receiving RSV-specific monoclonal antibodies with those born at an earlier gestational age. This will aim to provide insight as to whether it may be worth considering monoclonal antibody prophylaxis against RSV for infants in this age group.
Heterogeneity
To test for heterogeneity (inconsistency between studies), we will use the I2 test, taking an I2 of > 75% as being high heterogeneity. Sub-group analysis looking particularly at late pre-term infants may be carried out to explore the effectiveness of RSV prophylaxis on subsequent recurrent wheeze in this population.
Safety
Rates of adverse events such as injection site reactions/allergic reactions, fever, and rash in both intervention and control groups will be extracted and compared to evaluate the safety of the intervention.
Discussion
Asthma is the most prevalent chronic respiratory disease worldwide creating a huge burden on patients and services [7]. If this review demonstrates that RSV prophylaxis reduces asthma risk, this supports the hypothesis of a causal relationship between RSV infection and asthma development. This could have potentially huge clinical implications if there is the possibility of reducing rates of recurrent childhood wheeze with the use of RSV-specific monoclonal antibodies. This result and the subsequent sub-group analysis could also have significant implications in terms of which infants qualify as being ‘at-risk’ enough to receive the monoclonal antibodies and could thereafter open the discussion and allow for future studies on cost-effectiveness analysis of monoclonal antibodies with regard to reduction of recurrent wheeze. Also, if the review supports the hypothesis of a causal relationship between RSV bronchiolitis and subsequent recurrent wheeze, this will prompt further studies on the biological mechanism by which this may occur. On the contrary, if RSV prophylaxis is shown to have no effect on rates of asthma development, this will then open the debate further into whether the association between RSV infection in infancy and subsequent asthma development is actually causal or not.
Availability of data and materials
Not applicable
Abbreviations
- GRADE:
-
‘Grading of Recommendations Assessment, Development and Evaluation’
- RSV:
-
Respiratory syncytial virus
References
Øymar K, Skjerven HO, Mikalsen IB. Acute bronchiolitis in infants, a review. Scand J Trauma Resusc Emerg Med. 2014;22:23. Published 2014 Apr 3. https://doi.org/10.1186/1757-7241-22-23.
van Meel ER, den Dekker HT, Elbert NJ, Jansen PW, Moll HA, Reiss IK, de Jongste JC, Jaddoe VWV, Duijts L. A population-based prospective cohort study examining the influence of early-life respiratory tract infections on school-age lung function and asthma. Thorax. 2018;73(2):167–73.
Stranak Z, Saliba E, Kosma P, Posfay-Barbe K, Yunis K, Farstad T, et al. Predictors of RSV LRTI hospitalization in infants born at 33 to 35 weeks gestational age: a large multinational study (PONI). PLoS One. 2016;11(6):e0157446.
der Voort AMM S-v, Arends LR, de Jongste JC, Annesi-Maesano I, Arshad SH, Barros H, et al. Preterm birth, infant weight gain, and childhood asthma risk: a meta-analysis of 147,000 European children. J Allergy Clin Immunol. 2014;133(5):1317–29.
Krishnan JA, Lemanske RF, Canino GJ, Elward KS, Kattan M, Matsui EC, et al. Asthma Outcomes: Asthma Symptoms. J Allergy Clin Immunol. 2012;129(30):S124–35.
Oostenbrink R, Jansingh-Piepers EM, Raat H, Nuijsink M, Landgraf JM, Essink-Bot ML, et al. Health-related quality of life of pre-school children with wheezing illness. Pediatr Pulmonol. 2006;41(10):993–1000.
Mallol J, Garcia-Marcos L, Sole D, Brand P. International prevalence of recurrent wheezing during the first year of life: variability, treatment patterns and use of health resources. Thorax. 2010;65(11):1004–9.
Soriano JB, Abajobir AA, Abate KH, Abera SF, Agrawal A, Ahmed MB, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706.
Mukherjee M, Stoddart A, Gupta RP, Nwaru BI, Farr A, Heaven M, et al. The epidemiology, healthcare and societal burden and costs of asthma in the UK and its member nations: analyses of standalone and linked national databases. BMC Med. 2016;14(1):113. Available from. https://doi.org/10.1186/s12916-016-0657-8.
Loftus PA, Wise SK. Epidemiology of asthma. Curr Opin Otolaryngol Head Neck Surg. 2016;24(3):245–9.
Feldman AS, He Y, Moore ML, Hershenson MB, Hartert TV. Toward primary prevention of asthma. Reviewing the evidence for early-life respiratory viral infections as modifiable risk factors to prevent childhood asthma. Am J Respir Crit Care Med. 2015;191(1):34–44.
Törmänen S, Lauhkonen E, Riikonen R, Koponen P, Huhtala H, Helminen M. Risk factors for asthma after infant bronchiolitis. Allergy. 2018;73(4):916–22.
Piedimonte G, Perez MK. Role of early-life environmental influences in the development of asthma. How painful is it when you catch a bad cold too early? J Asthma. 2008;45(10):25–8.
Utrecht University. First consortium of local manufacturers to make affordable biosimilars available for low income countries. https://www.uu.nl/en/news/first-consortium-of-local-manufacturers-to-make-affordable-biosimilars-available-for-low-income Accessed 5 Mar 2019.
Olchanski N, Hansen RN, Pope E, D’Cruz B, Fergie J, Goldstein M, et al. Palivizumab Prophylaxis for Respiratory Syncytial Virus: Examining the Evidence Around Value. Open forum Infect Dis. 2018;5(3):ofy031.
Rogovik AL, Carleton B, Solimano A, Goldman RD. Palivizumab for the prevention of respiratory syncytial virus infection. Can Fam Physician. 2010;56(8):769–72.
McLellan JS, Chen M, Kim A, Yang Y, Graham BS, Kwong PD. Structural basis of respiratory syncytial virus neutralization by motavizumab. Nat Struct Mol Biol. 2010;17(2):248–50.
Bernhard R. Product review on the monoclonal antibody palivizumab for prevention of respiratory syncytial virus infection. Hum Vaccin Immunother. 2017;13(9):2138–49.
Cingoz O. Motavizumab. MAbs [Internet]. 2009;1(5):439–42.
Carbonell-Estrany X, Simoes EAF, Dagan R, Hall CB, Harris B, Hultquist M, et al. Motavizumab for prophylaxis of respiratory syncytial virus in high-risk children: a noninferiority trial. Pediatrics. 2010;125(1):e35–51.
Walker EP. FDA Advisers Turn Down New RSV Drug. https://www.medpagetoday.com/publichealthpolicy/fdageneral/20456 Accessed 5 Mar 2019.
Herschler B. 2010. ‘AstraZeneca drops lung drug and takes $445 million charge.’ Reuters. https://uk.reuters.com/article/uk-astrazeneca-motavizumab/astrazeneca-drops-lung-drug-and-takes-445-million-charge-idUKTRE6BK17K20101221
Taylor P. Regeneron drops RSV drug. http://www.pmlive.com/pharma_news/regeneron_drops_rsv_drug_1202187 Accessed 5 Mar 2019.
Mazur NI, Higgins D, Nunes MC, Melero JA, Langedijk AC, Horsley N, et al. The respiratory syncytial virus vaccine landscape: lessons from the graveyard and promising candidates. Lancet Infect Dis. 2018;18(10):e295–311.
Teale A, Deshpande S, Burls A. Palivizumab and the importance of cost effectiveness. BMJ. 2009;11(338):b1935 Available from: http://www.bmj.com/content/338/bmj.b1935.abstract.
Smart KA, Lanctot KL, Paes BA. The cost effectiveness of palivizumab: a systematic review of the evidence. J Med Econ. 2010;13(3):453–63 Available from: https://www.ncbi.nlm.nih.gov/pubmed/20653398.
Figueras-Aloy J, Carbonell-Estrany X, Quero J, Group IS. Case-control study of the risk factors linked to respiratory syncytial virus infection requiring hospitalization in premature infants born at a gestational age of 33-35 weeks in Spain. Pediatr Infect Dis J. 2004;23(9):815–20 Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med5&NEWS=N&AN=15361718.
Simões EAF, Carbonell-Estrany X, Fullarton JR, Liese JG, Figueras-Aloy J, Doering G, et al. A predictive model for respiratory syncytial virus (RSV) hospitalisation of premature infants born at 33-35 weeks of gestational age, based on data from the Spanish FLIP Study. Respir Res. 2008;9(1):78 Available from: https://www.ncbi.nlm.nih.gov/pubmed/19063742.
Simoes EAF. Respiratory syncytial virus infection. Lancet. 1999;354(9181):847–52 Available from: http://www.sciencedirect.com/science/article/pii/S0140673699800403.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). Cochrane, 2019. Available from www.training.cochrane.org/handbook.
Deeks JJ, Higgins JPT, Altman DG. Chapter 11: Presenting results and ‘Summary of findings tables’ Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). In: The Cochrane Collaboration; 2011. Available from www.cochrane-handbook.org.
Deeks JJ, JPT H, Altman DG. Chapter 12: Interpreting results and drawing conclusions. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). In: The Cochrane Collaboration; 2011. Available from www.cochrane-handbook.org.
StatsDirect Ltd. StatsDirect statistical software. http://www.statsdirect.com. England: StatsDirect Ltd.; 2013.
Acknowledgements
Not applicable
Funding
Not applicable
Author information
Authors and Affiliations
Contributions
All authors contributed to the search strategy, eligibility criteria, research question design and data analysis strategy. LAQ (first author) was the primary author involved in the writing of the protocol. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
HE Groves has delivered a presentation on her research at a non-promotional educational meeting and received honoria from Abbvie. All other authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Appendix 1. PRISMA-P 2015 Checklist. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 checklist. Appendix 2: Data collection form for Intervention review – RCTs and non-RCTs. Adapted from the Cochrane Collaboration.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Quinn, L.A., Shields, M.D. & Groves, H.E. Respiratory syncytial virus prophylaxis for prevention of recurrent childhood wheeze and asthma: a protocol for a systematic review. Syst Rev 8, 333 (2019). https://doi.org/10.1186/s13643-019-1251-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-019-1251-x