
Abstract
Background
Early diagnosis and treatment of tuberculosis (TB) have been shown to reduce the impact of TB illness particularly, among TB key populations such as people living with HIV/AIDS, prisoners, refugees, migrants, displaced populations, survivors of TB illness, and indigenous populations. We propose to conduct a systematic scoping review to map global evidence on active tuberculosis case finding policies, strategies, and interventions for TB key populations.
Method and analysis
This study will be guided by the scoping review framework, proposed by Arksey and O’Malley. A comprehensive literature search will be performed in the following electronic databases: PubMed, SCOPUS, Web of Science, Science Direct, and EBSCOhost (Academic search complete, PsycINFO, Health Sources, CINAHL, and MEDLINE with full text). Primary studies both published in peer-reviewed journals and grey literature such as unpublished studies, thesis, and studies in press addressing our research question will be included. To reduce selection bias, two independent reviewers will perform title, abstract, and full article screening in parallel. Also, data extraction from the included studies will be conducted by two independent reviewers. We will use NVivo version 11 software to extract the outcomes relevant to answering the research question from the included studies using a content thematic analysis. The results of this proposed study will be presented according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis: Extension for Scoping Review (PRISMA-ScR). The mixed methods assessment tool version 2018 will be employed for quality appraisal of the included studies.
Discussion
We anticipate that the mapped evidence will help reveal diverse active TB case finding policies, strategies, and interventions to help inform future adoption and implementation to reduce TB missing cases worldwide. We also anticipated that the results of the proposed scoping review will help reveal research gaps, which can be addressed to ensure early detection and treatment of TB among key populations. The proposed study will may as well contribute to healthcare systems strengthening and improve research in TB key populations.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Tuberculosis (TB) is a poverty-related disease and the world’s leading killer among infectious diseases [1, 2]. Worldwide, almost 1.5 million people die of TB illness each year making it one of the top ten causes of death [1, 3, 4] with over 94% of all TB deaths occurring in low- and middle-income countries yearly [1, 4]. Globally, close to a third of people have latent TB infection and places them at risk of developing TB illness [1]. However, people living with human immune-deficiency virus (HIV) infection or acquired immuno-deficiency syndrome (AIDS), prisoners, migrants, refugees, survivors of TB infection, and indigenous populations are highly vulnerable and at much higher risk of developing TB illness [3].
Of the 10 million people fell who ill with TB globally in 2017, nearly 30% of them were “missing” that is, people with TB who did not report, undiagnosed, or untreated [3, 5,6,7]. TB key populations such as prisoners, people living with TB/HIV coinfection, migrants, refugees, and indigenous populations may have poor health-seeking behaviour and experience significant marginalisation and human rights violations [3, 8]. They also experience far-reaching stigma and discrimination, state and non-state violence and harassment, restrictive laws and policies, and criminalization of behaviours or practices which put them at higher risks and also undermine their access to quality healthcare services [3, 8,9,10]. TB is spread from person to person through coughing and sneezing [11, 12]. It is estimated that one person with active or untreated TB can spread the infection to as many as 15 other people in a year. This makes the hunt for “missing cases” more urgent [3, 13].
To address the challenge of TB “missing cases”, policies, effective strategies, and implementation of active case interventions for TB key populations are highly essential globally [14, 15]. Active TB case finding approaches such as screening of TB contacts, workplace screening, screening prior to entry into a therapy or drug treatment, mandatory screening in the criminal justice system, and refugee programmes are essential to facilitate early detection of TB case and treatment. This study therefore aims to map global evidence on active tuberculosis case finding policies, strategies, and interventions for TB key populations. We anticipate that the results of this study will reveal research gaps for future meta-analysis or primary studies to inform policy towards ending TB epidemics as stipulated in end TB strategy [16].
Methods
Overview
A scoping review is useful in mapping a range of literature that exists around a topic of interest and aids to focus the research questions by charting existing research findings and identifying research gaps [17]. A scoping methodology is also considered a useful approach for determining the need and value of a future primary study or a full systematic review [17]. Based on this, the current scoping review will be guided by the enhanced Arksey and O’Malley scoping review framework [17, 18]. The framework involves the following: identifying the research question, identifying relevant studies, study selection, charting the data, and collating, summarising, and reporting results.
Identifying the research question
Population, Concept and Context (PCC) mnemonic [19] was used to determine the eligibility of the scoping review question, as shown in Table 1. The main review question will be What evidence exist on active TB case finding policies, strategies, and interventions for TB key populations globally?
The sub-review questions will be as follows:
-
What evidence exist on polices for active TB case finding in key populations globally?
-
What evidence exist on strategies for active TB case finding in key populations globally?
-
What evidence exist on active TB case finding interventions for key populations globally?
Identify relevant studies
We will conduct a thorough keyword search to identify all relevant studies from multiple databases regardless of the date of publication, language, and publication status (published, unpublished, and in press). We will search the following electronic databases: PubMed, SCOPUS, Web of Science, Science Direct, and EBSCOhost (Academic Search Complete, PsycINFO, Health Sources, CINAHL, and MEDLINE with full text) for relevant studies. The reference list of all included studies will also be thoroughly for relevant articles. The combination of keywords that will be used to search for relevant studies from the electronic databases are “active tuberculosis”, “case finding”, “policy”, “intervention”, “strategies”, “key population” “HIV patients”, “prisoners”, “refugees”, “indigenous populations”, “migrants”, “survivor of tuberculosis illness”, and “hard-to-reach populations”. Boolean terms, AND/OR, and Medical Subject Heading (MeSH) terms will be used during the keywords search to identify relevant studies. Details of the search records such as the date of the search, database, keywords, number of studies, and number of eligible studies will be adequately documented for each search as demonstrated for the pilot search in PubMed (Table 2).
Eligibility criteria
To ensure the selection of relevant studies for this review, the study selection will be guided by the eligibility criteria as specified under the inclusion/exclusion criteria.
Inclusion criteria
We will include studies that meet the following criteria:
-
Studies presenting evidence on the study conducted among TB key populations globally
-
Studies reporting evidence on active case finding policies for TB key populations globally
-
Studies reporting evidence on active case finding strategies for TB key populations globally
-
Studies presenting evidence on active case finding intervention for TB key populations globally
-
Quantitative, qualitative, and mixed methods study designs
Exclusion criteria
This will include the following:
-
Studies targeting the general population
-
Studies focusing on health education on TB
-
Qualitative study designs
-
Other types of reviews
-
Studies reporting on diagnostic accuracy without yield
Study selection
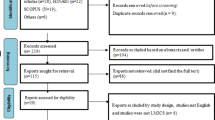
To reduce selection bias, two independent investigators will conduct a comprehensive title screening in the abovementioned electronic databases guided by the eligibility criteria. All eligible studies will be imported into endnote X9 software and duplicates removed. The final endnote library will then be shared among the reviewers. Two investigators will also independently sort the studies into the categories “excluded” and “included” at the abstract and full-text screening stages, based on the inclusion criteria listed above. In an event where an article could not be retrieved from the databases, we will request for assistance from the University of KwaZulu-Natal library services or we may request for the full text from the authors. Categorisation choices will be compared and, where there is disagreement, the researchers will discuss the title and content of the study until a consensus is reached on a categorisation during the title and abstract screening stages. A third investigator will be engaged to resolve disagreement at the full-text screening stage. We will also calculate the inter-rater agreement (Cohen’s kappa coefficient (κ) statistic) and between reviewers following full-text screening as well as, the McNemar’s chi-square statistic using Stata 14. For articles with no available abstract, categorisation based on the title alone will be used. We will follow an adapted PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to report the screening results [20].
Charting the data
We will extract information relevant to the aim of this study. A data extraction form will be developed electronically using google forms and piloted with ten percent of the included studies by two investigators in order to ensure accuracy and consistency extracted data. The data extraction form will then be updated based on feedback from the investigators if needed before its final use. Table 3 shows the data extraction form that will be used for this proposed review.
Collating, summarising, and reporting the results
Content thematic analysis approach will be employed to abstract data relevant to answer the proposed scoping review question [21]. All data regarding active TB case finding interventions and strategies for TB key populations published globally will be extracted from the included articles. NVivo version 11 will be used for content thematic analysis of the included studies. The emerging themes from the included studies will be reported by giving a narrative summary of the results to answer the review question. The implications of the study results for future research, policy, and practice will also be examined and reported. The results of this proposed study will be presented according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis: Extension for Scoping Review (PRISMA-ScR) [20].
Quality appraisal
To assess the quality of the included studies, the Mixed Method Quality Appraisal Tool (MMAT) Version 2018 [22] will be used to assess the methodological quality of all the included studies. We will use the MMAT to examine the included studies in the following categories: the appropriateness of the aim of the study, adequacy and methodology, study design, participant recruitment, data collection, data analysis, and findings presented. We will grade the quality of studies with a quality score ranging from ≤ 50% as low quality, 51–75% will be considered as an average quality, and 76–100% will be considered as high quality. This will ensure that the study designs of the included studies are appropriate for the research objectives. The quality assessment will also help us to report on the risk of bias of the included studies, and the quality of the evidence that will be reported.
Discussion
This systematic scoping review will map existing literature on active tuberculosis case finding policies, strategies, and interventions for TB key populations globally. The World Health Organization End TB Strategy aims to end the global TB epidemic, with targets to reduce TB deaths by 95% and to cut new cases by 90% between 2015 and 2035, and to ensure that no family is burdened with catastrophic expenses due to TB [23]. The WHO has also set interim milestones for 2020, 2025, and 2030 [23]. The End Strategy reinforces a focus on serving populations highly vulnerable to TB infection and poor healthcare access, such as hard-to-reach populations [23]. Populations such as people living with HIV/AIDS, prisoners, migrants, refugees, displaced persons, survivors of TB infection, and indigenous populations have been identified as key populations with a higher risk of developing TB illness [3].
We anticipate that the mapped evidence will help reveal diverse active TB case finding policies, strategies, and interventions to help inform future adoption and implementation to reduce TB missing cases worldwide. We also anticipated that the results of the proposed scoping review will help reveal research gaps, which can be addressed to ensure early detection and treatment of TB among key populations. The proposed study will may as well contribute to healthcare systems strengthening and improve research in TB key populations. The study further intends to build and contribute to a body of literature on TB research, particularly on the diagnosis of the most vulnerable populations. Moreover, the results of the proposed scoping review may contribute to eliminating TB by the year 2035.
Conclusion
The findings of this proposed systematic scoping review will provide evidence useful to influence the direction of future research such as meta-analysis and primary studies to influence policy, strategy, and implementation of active case finding interventions for TB key populations in countries most needed.
Availability of data and materials
We have duly cited all studies, and data is presented in a form of references.
Abbreviations
- TB:
-
Tuberculosis
References
World Health Organization. Global tuberculosis report 2017. 2017. Google Scholar. 2018.
Kuupiel D, Adu KM, Apiribu F, Bawontuo V, Adogboba DA, Ali KT, et al. Geographic accessibility to public health facilities providing tuberculosis testing services at point-of-care in the upper east region, Ghana. BMC public health. 2019;19(1):718.
The Global Fund. Tuberculosis 2018 [cited 2018 09/10/2018]. Available from: https://www.theglobalfund.org/en/tuberculosis/.
Gupta-Wright A, Corbett EL, van Oosterhout JJ, Wilson D, Grint D, Alufandika-Moyo M, et al. Rapid urine-based screening for tuberculosis in HIV-positive patients admitted to hospital in Africa (STAMP): a pragmatic, multicentre, parallel-group, double-blind, randomised controlled trial. Lancet. 2018;392(10144):292–301.
Dodd PJ, Yuen CM, Sismanidis C, Seddon JA, Jenkins HE. The global burden of tuberculosis mortality in children: a mathematical modelling study. Lancet Global Health. 2017;5(9):e898–906.
Dheda K, Gumbo T, Maartens G, Dooley KE, McNerney R, Murray M, et al. The epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant, extensively drug-resistant, and incurable tuberculosis. Lancet Respir Med. 2017;5(4):291–360.
Al-Darraji HA, Altice FL, Kamarulzaman A. Undiagnosed pulmonary tuberculosis among prisoners in Malaysia: an overlooked risk for tuberculosis in the community. Trop Med Int Health. 2016;21(8):1049–58.
Joshua IA, Dangata YY, Audu O, Nmadu AG, Omole NV. Human rights and Nigerian prisoners--are prisoners not humans? Med Law. 2014;33(4):11–20.
de Vries SG, Cremers AL, Heuvelings CC, Greve PF, Visser BJ, Belard S, et al. Barriers and facilitators to the uptake of tuberculosis diagnostic and treatment services by hard-to-reach populations in countries of low and medium tuberculosis incidence: a systematic review of qualitative literature. Lancet Infect Dis. 2017;17(5):e128–e43.
Fahy S. Rights-based TB programs for migrants and prisoners needed in North Korea. Health Hum Rights. 2016;18(1):109–14.
Cleveland JL, Robison VA, Panlilio AL. Tuberculosis epidemiology, diagnosis and infection control recommendations for dental settings: an update on the Centers for Disease Control and Prevention guidelines. J Am Dent Assoc. 2009;140(9):1092–9.
Yadav S, Mathur M, Dixit A. Knowledge and attitude towards tuberculosis among sandstone quarry workers in desert parts of Rajasthan. Indian J Tuberc. 2006;53(4):187.
Salaniponi FM, Gausi FK, Chimzizi RB, Harries AD. The missing cases of tuberculosis in Malawi: the contribution from cross-border registrations. Trans R Soc Trop Med Hyg. 2004;98(4):251–4.
Zenner D, Southern J, van Hest R, DeVries G, Stagg HR, Antoine D, et al. Active case finding for tuberculosis among high-risk groups in low-incidence countries. Int J Tuberc Lung Dis. 2013;17(5):573–82.
Story A, Aldridge RW, Abubakar I, Stagg HR, Lipman M, Watson JM, et al. Active case finding for pulmonary tuberculosis using mobile digital chest radiography: an observational study. Int J Tuberc Lung Dis. 2012;16(11):1461–7.
World Health Organization. Implementing the end TB strategy: the essentials. World Health Organization; 2015. Report No.: 9241509937.
Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):69.
Institute JB. Joanna Briggs Institute reviewers’ manual: 2015 edition/supplement. The Joanna Briggs Institute: Methodology for JBI Scoping Reviews Adelaide; 2015.
Tricco A, Straus S, Moher DJENhwe-now-cuE-sSD-p. Preferred Reporting Items for Systematic Reviews and Meta-Analysis: Extension for Scoping Reviews (PRISMA-ScR). 2018.
Braun V, Clarke V, Hayfield N. Terry GJHoRMiHSS. Thematic analysis. 2019:843–60.
Hong Qn, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed Methods Appraisal Tool (MMAT) Version 2018.
World Health Organization. WHO End TB Strategy: Global strategy and targets for tuberculosis prevention, care and control after 2015Geneva: World Health Organization; 2015 [cited 2019 07/05/2019]. Available from: https://www.who.int/tb/post2015_strategy/en/.
Acknowledgements
We are thankful to the University of KwaZulu-Natal, College of Health Sciences, for providing us with essential research resources to complete this study protocol. We would also like to thank the staff of the Department of Public Health Medicine, University of KwaZulu-Natal, for their diverse support.
Funding
This study is funded by the University of KwaZulu-Natal, College of Health Sciences Research Scholarship.
Author information
Authors and Affiliations
Contributions
DK conceptualised the study and wrote the protocol. VB and TPMT contributed to the writing and critically reviewed the draft protocol. DK wrote the final manuscript, and all authors approved the final draft.
Authors’ information
Desmond Kuupiel: He is a Postdoctoral Fellow in the Discipline of Public Health Medicine, School of Nursing and Public Health, University of Kwazulu-Natal, South Africa.
Dr. Vitalis Bawontuo: He is the Dean of the Faculty of Health and Allied Sciences, Catholic University College of Ghana, Fiapre, Sunyani.
Dr. Tivani Phosa Mashamba-Thompson: She is the Academic Leader Research for the School of Nursing and Public Health, University of KwaZulu-Natal, South Africa.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval is not applicable to this study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kuupiel, D., Bawontuo, V. & Mashamba-Thompson, T.P. Mapping evidence on tuberculosis active case finding policies, strategies, and interventions for tuberculosis key populations: a systematic scoping review protocol. Syst Rev 8, 162 (2019). https://doi.org/10.1186/s13643-019-1098-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-019-1098-1