
Abstract
Background
Bruxism is a sleep disorder characterized by grinding and clenching of the teeth that may be related to irreversible tooth injuries. It is a prevalent condition occurring in up to 31% of adults. However, there is no definitive answer as to which of the many currently available treatments (including drug therapy, intramuscular injections, physiotherapy, biofeedback, kinesiotherapy, use of intraoral devices, or psychological therapy) is the best for the clinical management of the different manifestations of bruxism. The aim of this systematic review and network meta-analysis is to answer the following question: what is the best treatment for adult bruxists?
Methods/design
Comprehensive searches of the Cochrane Library, MEDLINE (via PubMed), Scopus, and LILACS will be completed using the following keywords: bruxism and therapies and related entry terms. Studies will be included, according to the eligibility criteria (Controlled Clinical Trials and Randomized Clinical Trials, considering specific outcome measures for bruxism). The reference lists of included studies will be hand searched. Relevant data will be extracted from included studies using a specially designed data extraction sheet. Risk of bias of the included studies will be assessed, and the overall strength of the evidence will be summarized (i.e., GRADE). A random effects model will be used for all pairwise meta-analyses (with a 95% confidence interval). A Bayesian network meta-analysis will explore the relative benefits between the various treatments. The review will be reported using the Preferred Reporting Items for Systematic Reviews incorporating Network Meta-Analyses (PRISMA-NMA) statement.
Discussion
This systematic review aims at identifying and evaluating therapies to treat bruxism. This systematic review may lead to several recommendations, for both patients and researchers, as which is the best therapy for a specific patient case and how future studies need to be designed, considering what is available now and what is the reality of the patient.
Systematic review registration
PROSPERO CRD42015023308
Similar content being viewed by others

Background
Different definitions for bruxism have been proposed. The American Academy of Sleep Medicine, in 1990, defined sleep bruxism (SB) as a parasomnia because it is an undesirable physical phenomenon which occurs predominantly during sleep [1]. In 2010, another study defined sleep bruxism as the stereotyped oromandibular activity during sleep, characterized by teeth grinding and clenching [2]. In 2013, bruxism was also defined as the repetitive jaw-muscle activity characterized by clenching or grinding of the teeth and/or by bracing or thrusting of the mandible, in an international consensus [3]. The known manifestations of bruxism are sleep bruxism, which occurs during sleep, and awaking bruxism, which occurs during wakefulness [3]. Regardless of the definition, etiology or kind of manifestation, it is mainly characterized by teeth grinding and clenching, and patients diagnosed with this condition are commonly referred to as bruxists.
According to a recent review, both bruxism physiology and pathology have unknown causal associated factors. Nevertheless, some conditions like smoking, use of certain medications, and breathing problems can be considered as risk factors for bruxism [4]. Indeed, the main and widely accepted hypothesis is that the abnormal rhythmic mandibular movements detected during bruxism activity are caused by central and autonomic nervous system [5]. In the past, based on suspicion that occlusal imbalance was the main etiological factor for bruxism, dentists used to indicate occlusal adjustment [6], occlusal stabilization splints [7], or even oral rehabilitation, based on occlusal equilibration theories to deal with bruxists [8, 9]. These treatments, especially occlusal splints, still have no proven effectiveness for bruxism management based on RCTs and should be considered as a more limited treatment modality once the splints’ effect seem not to address the cause of bruxism and serves mainly for the management of patients’ signs and symptoms. [10, 11] Alternative therapies such as relaxation and biofeedback were proposed (and proved efficacious) for bruxism, especially in cases of awaking bruxism, which are more related to stress and anxiety [12–14].
Sleep hygiene techniques (e.g., relaxation before sleeping or avoiding caffeine) are also recommended to control sleep bruxism; however, recent data showed that these therapies were not efficacious for muscular activity control, once the autonomic muscular activity do not decrease using this sort of therapy [15]. The use of portable devices with contingent electrical stimulation (CES) is a promising strategy for bruxism therapy, especially because there are no side effects reported [16, 17]. The use of a night guard stabilization splint is also recommended after rehabilitation with dental implants, but no clinical trial confirmed this need [18–21]. There are also studies giving support to the use of clonidine and mandibular advancement appliances (MAA) and suggesting that occlusal splints should be used only as transient therapies while MMA can present side effects and maladaptation [7, 10, 18–21]. The MMA can actually be effective to reduce muscular activity in bruxists [22], but there is currently a lack of long-term evaluation. Both CES and MMA still need further investigation.
Botulinum toxin injection in the masticatory muscles is another promising treatment alternative to reduce muscular activity in bruxists, but scarce strong data exists to support this therapy as a routine, while side effects may also be present [23–25]. In fact, some drugs can be used to decrease bruxism episodes, but some pharmacological treatments may be unsafe if used for long periods, considering the inherent side effects or risks of dependency [7].
Interventions in individuals diagnosed as bruxists used to be needed to control pain, temporomandibular disorders, or in an attempt to control the progression of tooth wear [7, 19, 26]. These signs and symptoms can be caused or even enhanced by bruxism, but the current support therapies for bruxism aim mainly to control the consequences rather than to address to the cause(s) of the(se) problem(s) [27]. The multifactorial etiology of orofacial pain and temporomandibular disorders makes these problems not always solvable by the dentist alone, even when bruxism is suspected to be involved in the etiology.
Review objectives
We plan to conduct a systematic review and network meta-analysis to try to answer the following question: which is the best treatment for adult bruxists, considering the reduction of muscular activity or reduction of grinding noises at night, sleep-related variables, comorbidities, and costs of the different therapies found. We will explore in this review as primary outcome parameters masseter muscle activity measurement using electromyography and slow wave sleep percentage during the polysomnographic recording.
Why it is important to do this review
Bruxism is a common condition with a prevalence ranging from 8 to 31% in adults [28]. As it was shown, an effective long-term therapy to treat bruxists still lacks and several remaining questions still need to be answered, as “what should be done to support patients that are confirmed bruxists” or “what should be done after an oral rehabilitation is conducted and the patient is still clenching.” Some reviews, systematic reviews, and meta-analysis still show no definitive answers for all these questions [11, 12, 29], and this may be due to the comparison of only two interventions at a time, not summarizing a more comprehensive set of comparisons addressing the multiple interventions available. Remarkably, few studies compare different treatment effects of diverse current available therapies [7]. It would be helpful for the clinician and patients to know the current available treatments for the different manifestations of bruxism, what are their advantages and disadvantages to better choose among the options based on evidence and not only on expert’s opinion.
Methods/design
The protocol of this systematic review and network meta-analysis will be written in accordance with the PRISMA-P (Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols) [30] guidance. The completed systematic review will be written using the PRISMA-NMA extension statement to structure the contents of the final report. [31] This protocol is registered in the PROSPERO database (international prospective register of systematic reviews) as CRD42015023308. The literature search was established to address the research question phrased as follows in the PICO framework: Population—adult patients diagnosed with bruxism; interventions and comparisons: adenotonsilectomy, medications (benzodiazepines, dopaminergics, sympatholytics, antihistamines, antiepileptics, antidepressants, serotonin precursors), compared among them or to placebo; botulinum toxin intramuscular injections compared to saline solution, muscular electric stimulation (contingent, microcurrent or transcutaneous current), biofeedback (audible noise/sound, adverse taste response to muscular activity), behavioral (relaxation exercises, sleep hygiene measures, cognitive instructions), and kinesiotherapy (facial massage, masticatory or facial muscles’ exercises). It is possible in some reports that the therapies’ results might be compared among them, compared to placebo groups or to controls; outcomes—decrease of muscular activity (records with different kinds of electromyography), relief in muscular symptoms (e.g., pain, soreness, discomfort, fatigue, either self-reported or through clinical examination), decrease or arrest of dental wear, or dental grinding noises; study design—RCT and CCT. We will consider any published trial from 1956 to present published in the English language.
Criteria for selecting studies for this review
The following criteria will be used to identify studies to be included in this review.
Types of participants
Studies that enrolled adults (from 18 years of age) diagnosed as bruxists will be considered for inclusion. Studies including patients with tooth wear, temporomandibular disorders, or orofacial pain will also be eligible for inclusion.
Interventions
According to the literature, interventions for bruxists are of wide variation and can be divided into the following groups: (1) intraoral: occlusal adjustment, occlusal splints, mandibular advancement appliances, NTI (nociceptive trigeminal inhibitory) splint; (2) physiotherapy for masticatory muscles’ with electrical stimulus: biofeedback, microcurrent transcutaneous stimulation, transcutaneous electrical nerve stimulation, contingent electrical stimulation; (3) drug therapy: antidepressants, l-dopa inhibitors, antiepileptic, sympatholytic, antihistamine, or dopaminergic drugs; (4) intramuscular injection: botulinum toxin A; (5) biofeedback: aversive taste, audible noise, or audible sound; (6) behavioral: relaxation techniques, “sleep hygiene” measures, cognitive treatment, psychological advice; (7) kinesiotherapy: masticatory muscles’ massage, facial exercise, or (8) others: alternative or support therapies. Any study evaluating any of the interventions listed above will be retained for inclusion in the review. Analysis will be conducted at therapy/group level.
Types of studies
We will include randomized controlled trials (RCTs) and controlled clinical trials (CCTs). Review papers, expert opinions, case reports, and series of case reports will be excluded. The bibliographies of relevant systematic reviews will be studied to identify any studies missed by our literature search.
Information sources and literature search
Electronic searches
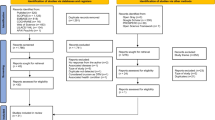
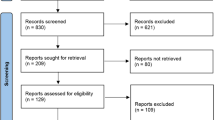
Comprehensive searches of the Cochrane Library, MEDLINE (via PubMed), Scopus, and LILACS will be completed using the strategy described on the Additional file 1. Two independent authors (MEM and JAS) will select the articles. The search will encompass all the indexed articles, computerized literature databases supplemented by manual searching of reference lists from each relevant paper identified.
Study selection procedure
All titles and abstracts found will be independently read. After the searches, when found, the duplicates will be removed and the papers evaluated. The abstracts found in multiple searches to identify potentially eligible articles for inclusion will be read. All potentially eligible studies will be retrieved and full-text articles reviewed to determine eligibility. Hand search in the references of the selected studies will be also done. Inconsistencies will be solved by discussion among independent investigators (RSO and TC). In case of missing data or information, authors will be contacted. The reviewers that will be enrolled in the searches are experienced in orofacial pain management, specialist clinicians, or methodologists in evidence-based medicine.
Data collection process
A standardized, electronic data collection form implemented in Microsoft Excel will be used to extract the following data: study design, diagnosis, number of participants, types of interventions compared, patient demographics, outcome measures, results, risk of bias assessment, and study authors’ main conclusions. Two researchers will perform data extraction independently.
Outcomes
Different outcomes will be considered in this review whenever available:
-
Primary effects: reduction of masticatory muscle activity (duration or intensity) detected by measurement of episodes per hour (day or nighttime) which can be assessed with polysomnography or in millivolts with electromyography;
-
Secondary effects (measured, self-reported or reported by bed partners): sleep quality improvement, mouth range improvement, patient discomfort, temporomandibular joint pain (orofacial pain), sounds, psychological discomfort, quality of life, stress degree/level, tooth grinding reduction, dental wear arrestment;
-
Comorbidity (side effects or adverse effects), costs, time span of the treatment (short-span and long-span outcomes can be evaluated separately) and;
-
Compliance (adherence to the treatment) with the different therapies.
Heterogeneity assessment
The different manifestations of bruxism (awake or sleep bruxism) may be treated separately in the outcome analysis, considering the subgroup analyses and/or meta-regression.
Assessment of effectiveness
The tools used to verify the effectiveness of bruxism therapy are mostly electromyography (portable devices or non-portable devices) or electrodes used in polysomnography. According to the literature, a therapy is effective for bruxism when the episodes of masticatory muscle activity (masseter and temporalis) are reduced and, depending on the methods of the studies number of episodes per hour, numbers of episodes per night are used to quantify muscular activity. Duration and intensity of muscular activity can also be used to assess the effect of certain bruxism therapies.
Other parameters may be used to monitor reduction of bruxism such as reduction of grinding sounds, tooth wear arresting, and masticatory muscle pain.
Risk of bias assessment
Studies will be assessed for bias using the Cochrane risk of bias tool considering the judgment of the random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias as “Low risk” of bias, “High risk” of bias, or “Unclear risk” of bias.
GRADE assessment
The evidence will be interpreted according to the GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. This approach is based on four steps considering direct and indirect treatment estimates for each comparison of the evidence network, rating the quality of each direct and indirect effect estimate, rating the NMA estimate for each comparison of the evidence network and quality of each NMA effect estimate [32].
Data synthesis
An overview of all selected studies will be narratively displayed. Once data are obtained, a sheet will be made to tabulate data for the different outcomes. Classification according to the population and study characteristics and nature of the therapy will be made. Both traditional pairwise meta-analyses and network meta-analyses will be conducted.
Standard pairwise meta-analysis
A random effects model will be used for all pairwise analyses when data are available. The heterogeneity will be evaluated through the estimation of the variance between studies (chi-square test and I 2 statistic). We will split the muscle activity into reduction or non-reduction, and the number of people who were in non-reduction group will be used to calculate the odds ratios (OR) and corresponding 95% confidence intervals (CIs). Mean differences between treatments may also be considered.
Network geometry
The network of treatments will be judged based on the available study data presented and evaluated graphically. We will evaluate if there is a sufficient number of comparisons in network with no available data, if there is a high number of comparisons based on single studies, if there are any “closed loops” which allow testing agreement between direct and indirect estimates for comparison on network, if any key treatments are missing, and if the possible lumping of treatments is minimizing the clinical relevance of the review. Next, the feasibility of a network meta-analysis will be assessed. Treatments will probably be lumped into eight groups a priori (cited earlier) considering the type of treatment: intraoral, physiotherapy, drug therapy, intramuscular injection, biofeedback, kinesiotherapy, and other alternative or support therapies.
Network meta-analysis (NMA)
NMA will be performed using a Bayesian framework through the Winbugs software considering the random effects models, which use vague (noninformative) prior distributions for all treatment effects as well as the between-study variance parameter. The results of all pairwise comparisons will be reported as OR and corresponding 95% credibility intervals (CrIs). The median treatments rankings and the surface under the cumulative ranking curve (SUCRA) will be presented as well. Analyses will be performed using Markov-Chain Monte-Carlo methods.
We will assess the convergence based on the Gelman Rubin diagnostics and inspection of Monte Carlo errors [33]. The consistency of results will be assessed examining through the comparison of results of pairwise and network meta-analyses. Also, we will evaluate the consistency by fitting the consistency and inconsistency models for network meta-analyses and through the comparison of deviance information criterion (DIC) between both models with smaller values indicative of a better fit and considering a difference of 5 or more as important [34]. Possible violation of transitivity could be associated with inclusion of patients with different health conditions and different habits. We will explore this through a subgroup and meta-regression analyses considering the following factors: inclusion of patients with obstructive sleep apnea syndrome, loud snorers, subjects with moderate daytime sleepiness, heavy alcohol drinkers, caffeine drinkers, smokers, subjects with a highly stressful life, and those with anxiety.
Discussion
This systematic review is planned as the current literature points toward the direction that the amount of wear is not always related to nocturnal bruxism activity [35]. If this is indeed correct, there is a void on what treating bruxism really means. Dentists and patients sometimes do not know if they are treating/being treated for muscular pain, tooth wear, or even if they are being protected against dental wear (anecdotal). Lastly, we feel that this systematic review may lead to several recommendations, for both patients and researchers, as which is the best therapy for a specific patient case and how future studies need to be designed [36], considering what is available now and what is the reality of the patient.
Although the comparison among treatments in a network meta-analysis is performed based on direct comparisons of interventions and indirect comparisons based on a common comparator, some factors may influence the estimates obtained from the analysis as number of trials included in the network; heterogeneity and inconsistency and several methods have been proposed to lead with those factors [37, 38]. In dentistry, this analytical approach has been used in different subjects such as restorative dentistry, periodontology, cariology and others [39–41].
Abbreviations
- CCT:
-
Controlled clinical trials
- CES:
-
Contingent electrical stimulation
- CI:
-
Confidence intervals
- CrIs:
-
Credibility intervals
- DIC:
-
Deviance information criterion
- GRADE:
-
DIC
- MAA:
-
Mandibular advancement appliances
- NMA:
-
Network meta-analysis
- NTI:
-
Nociceptive trigeminal inhibitory
- OR:
-
Odds Ratios
- PRISMA-NMA:
-
Preferred Reporting Items for Systematic Reviews incorporating Network Meta-Analyses
- PRISMA-P:
-
Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols
- RCT:
-
Randomized controlled trials
- SB:
-
Sleep bruxism
- SUCRA:
-
Surface under the cumulative ranking curve
References
Thorpy MJ. International classification of sleep disorders: diagnostic and coding manual. Rochester (NY): Minnesota: American Sleep Disorders Association; 1990.
Kato T, Lavigne GJ. Sleep bruxism: a sleep-related movement disorder. Sleep Med Clin. 2010;5:9–35.
Lobbezoo F, Ahlberg J, Glaros AG, Kato T, Koyano K, Lavigne GJ, et al. Bruxism defined and graded: an international consensus. J Oral Rehabil. 2013;40:2–4.
Lavigne GJ, Khoury S, Abe S, Yamaguchi T, Raphael K. Bruxism physiology and pathology: an overview for clinicians. J Oral Rehabil. 2008;5:476–94.
Klasser GD, Rei N, Lavigne GJ. Sleep bruxism etiology: the evolution of a changing paradigm. J Can Dent Assoc. 2015;81:f2.
Kardachi BJ, Bailey JO, Ash MM. A comparison of biofeedback and occlusal adjustment on bruxism. J Periodontol. 1978;49:367–72.
Huynh NT, Rompré PH, Montplaisir JY, Manzini C, Okura K, Lavigne GJ. Comparison of various treatments for sleep bruxism using determinants of number needed to treat and effect size. Int J Prosthodont. 2006;19:435–41.
Lobbezoo F, van der Zaag J, van Selms MK, Hamburger HL, Naeije M. Principles for the management of bruxism. J Oral Rehabil. 2008;35:509–23.
Behr M, Hahnel S, Faltermeier A, Bürgers R, Kolbeck C, Handel G, et al. The two main theories on dental bruxism. Ann Anat. 2012;194:216–9.
Dao TT, Lavigne GJ. Oral splints: the crutches for temporomandibular disorders and bruxism? Crit Rev Oral Biol Med. 1998;9:345–61.
Macedo CR, Silva AB, Machado MA, Saconato H, Prado GF. Occlusal splints for treating sleep bruxism (tooth grinding). Cochrane Database Syst Rev. 2007;4:CD005514.
Wang LF, Long H, Deng M, Xu H, Fang J, Fan Y, et al. Biofeedback treatment for sleep bruxism: a systematic review. Sleep Breath. 2014;18:235–42.
Ilovar S, Zolger D, Castrillon E, Car J, Huckvale K. Biofeedback for treatment of awake and sleep bruxism in adults: systematic review protocol. Syst Rev. 2014;3:42.
Klasser GD, Greene CS, Lavigne GJ. Oral appliances and the management of sleep bruxism in adults: a century of clinical applications and search for mechanisms. Int J Prosthodont. 2010;23:453–62.
Valiente López M, van Selms MK, van der Zaag J, Hamburger HL, Lobbezoo F. Do sleep hygiene measures and progressive muscle relaxation influence sleep bruxism? Report of a randomised controlled trial. J Oral Rehabil. 2015;42:259–65.
Jadidi F, Castrillon E, Svensson P. Effect of conditioning electrical stimuli on temporalis electromyographic activity during sleep. Oral Rehabil. 2008;35:171–83.
Conti PC, Stuginski-Barbosa J, Bonjardim LR, Soares S, Svensson P. Contingent electrical stimulation inhibits jaw muscle activity during sleep but not pain intensity or masticatory muscle pressure pain threshold in self-reported bruxers: a pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;117:45–52.
Mesko ME, Almeida RC, Porto JA, Koller CD, da Rosa WL, Boscato N. Should occlusal splints be a routine prescription for diagnosed bruxers undergoing implant therapy? Int J Prosthodont. 2014;27:201–3.
Grossi M. Should occlusal splints be a routine prescription for diagnosed Bruxers undergoing implant therapy. Int J Prosthodont. 2014;27:413–4.
Zhou Y, Gao J, Luo L, Wang Y. Does bruxism contribute to dental implant failure? A systematic review and meta-analysis. Clin Implant Dent Relat Res. 2015. doi:10.1111/cid.12300.
Sarmento HR, Dantas RV, Pereira-Cenci T, Faot F. Elements of implant-supported rehabilitation planning in patients with bruxism. J Craniofac Surg. 2012;23:1905–9.
Carra MC, Huynh NT, El-Khatib H, Remise C, Lavigne GJ. Sleep bruxism, snoring, and headaches in adolescents: short-term effects of a mandibular advancement appliance. Sleep Med. 2013;14:656–61.
Tinastepe N, Küçük BB, Oral K. Botulinum toxin for the treatment of bruxism. Cranio. 2014; http://www.tandfonline.com/doi/full/10.1179/2151090314Y.0000000022.
Guarda-Nardini L, Manfredini D, Salamone M, Salmaso L, Tonello S, Ferronato G. Efficacy of botulinum toxin in treating myofascial pain in bruxers: a controlled placebo pilot study. Cranio. 2008;26:126–35.
Long H, Liao Z, Wang Y, Liao L, Lai W. Efficacy of botulinum toxins on bruxism: an evidence-based review. Int Dent J. 2012;62:1–5.
Holbrook WP, Arnadóttir IB, Kay EJ. Prevention. Part 3: prevention of tooth wear. Br Dent J. 2003;195:75–81.
de la Hoz-Aizpurua JL, Díaz-Alonso E, LaTouche-Arbizu R, Mesa-Jiménez J. Sleep bruxism. Conceptual review and update. Med Oral Patol Oral Cir Bucal. 2011;16:e231–8.
Manfredini D, Winocur E, Guarda-Nardini L, Paesani D, Lobbezoo F. Epidemiology of bruxism in adults: a systematic review of the literature. J Orofac Pain. 2013;27:99–110.
Macedo CR, Macedo EC, Torloni MR, Silva AB, Prado GF. Pharmacotherapy for sleep bruxism. Cochrane Database Syst Rev. 2014;10:CD005578.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA, PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;349:g7647.
Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, Ioannidis JP, Straus S, Thorlund K, Jansen JP, Mulrow C, Catalá-López F, Gøtzsche PC, Dickersin K, Boutron I, Altman DG, Moher D. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162:777–84.
Puhan MA, Schünemann HJ, Murad MH, Li T, Brignardello-Petersen R, Singh JA, Kessels AG, Guyatt GH, GRADE Working Group. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349:g5630.
Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making. 2003;33:607–17.
Dias S, Welton N, Sutton A, Caldwell D, Lu G, Ades A. NICE DSU Technical Support Document 4: inconsistency in networks of evidence based on randomised controlled trials. 2011.
Baba K, Haketa T, Clark GT, Ohyama T. Does tooth wear status predict ongoing sleep bruxism in 30-year-old Japanese subjects? Int J Prosthodont. 2004;17:39–44.
Lee A, He LH, Lyons K, Swain MV. Tooth wear and wear investigations in dentistry. J Oral Rehabil. 2012;39:217–25.
Li T, Puhan MA, Vedula SS, Singh S, Dickersin K, Ad Hoc Network Meta-analysis Methods Meeting Working Group. Network meta-analysis-highly attractive but more methodological research is needed. BMC Med. 2011;9:79.
Mills EJ, Thorlund K, Ioannidis JP. Demystifying trial networks and network meta-analysis. BMJ. 2013;346:f2914.
Faggion Jr CM, Listl S, Frühauf N, Chang HJ, Tu YK. A systematic review and Bayesian network meta-analysis of randomized clinical trials on non-surgical treatments for peri-implantitis. J Clin Periodontol. 2014;41:1015–25.
Schwendicke F, Brouwer F, Schwendicke A, Paris S. Different materials for direct pulp capping: systematic review and meta-analysis and trial sequential analysis. Clin Oral Investig. 2016;20:1121–32.
Schwendicke F, Göstemeyer G, Blunck U, Paris S, Hsu LY, Tu YK. Directly placed restorative materials: review and network meta-analysis. J Dent Res. 2016;95:613–22.
Acknowledgements
We would like to thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, BRAZIL) for the scholarships for RSO and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) for the research grant for TPC.
Funding
This review has been funded by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, BRAZIL—award number: 88881.065005/2014-01). Dr. Brian Hutton is the recipient of a New Investigator Award from the Canadian Institutes of Health Research and the Drug Safety and Effectiveness Network. Dr. David Moher is funded by the University of Ottawa Research Chair.
Availability of data and materials
Not applicable.
Authors’ contributions
MEM conceived the study and drafted the protocol. JAS participated in the design of the study and drafted the protocol. RSO drafted the successful funding application to support the conduct of the review and will perform the statistical analysis. BH participated in its design and will plan and run the statistical analysis. DM participated in its design and helped to draft the protocol. TPC drafted the successful funding application to support the conduct of the review and participated in its design and coordination and helped to draft the protocol. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
Search terms. (DOCX 35 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Mesko, M.E., Hutton, B., Skupien, J.A. et al. Therapies for bruxism: a systematic review and network meta-analysis (protocol). Syst Rev 6, 4 (2017). https://doi.org/10.1186/s13643-016-0397-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-016-0397-z